

Abstract
We hypothesized that during conditioning chemotherapy for allogeneic stem cell transplant (allo-SCT), disruption of stromal-leukemia interactions using granulocyte-colony stimulating factor (G-CSF) in combination with the CXCR4-specific inhibitor plerixafor, may promote release of leukemic cells from the niche and increase tumor elimination. In a phase 1/2 investigation, we treated 45 AML/MDS/CML patients (34 AML, 7 MDS, and 4 CML) with G-CSF (10 μg/kg daily for 6 days starting on day −9) plus plerixafor (doses of 0, 80, 160 or 240 μg/kg daily for 4 days starting on day −7) along with the busulfan-fludarabine (Bu-Flu) conditioning regimen. In the phase 1 part, we determined that G-CSF plus plerixafor is safe in this setting. We compared clinical effects and outcomes of AML/MDS study patients (n = 40) to 164 patients from a historical data set who received Bu-Flu alone prior to allo-SCT by stratifying on cytogenetics and disease status to correct for bias. Study patients had increased myeloid chimerism and lower rates of GvHD. There was no significant difference in relapse free survival or overall survival. The G-CSF plus plerixafor combination increased circulating white blood cells, CD34+ cells, and CXCR4+ cells, and preferentially mobilized FISH+ leukemic cells. ClinicalTrials.gov identifier is NCT00822770.
Keywords: myeloid leukemia, allogeneic stem cell transplant, plerixafor, granulocyte colony stimulating factor
Introduction
Allogeneic stem cell transplantation (allo-SCT) is frequently used as treatment for patients with acute myeloid leukemia (AML), myelodysplastic syndrome (MDS), and chronic myeloid leukemia (CML). Because relapse of the malignancy is the major cause of treatment failure,1 novel treatments that reduce relapse are needed to improve overall survival rates. One potential strategy is to interfere with the supportive interactions of leukemia cells with the bone marrow microenvironment.
The purpose of conditioning chemotherapy in allo-SCT is to eradicate leukemia cells and to provide sufficient immunosuppression to prevent rejection of the transplant. There is evidence that niche interactions between the bone marrow (BM) stroma and leukemic cells provide protection from chemotherapy.2, 3 A critical interaction between leukemia and the bone marrow microenvironment occurs when leukemia stem cells home and adhere to the protective niche using C-X-C chemokine receptor type 4 (CXCR4, also known as CD184) on the leukemic cell, and its ligand C-X-C chemokine receptor 12 (CXCL12, also known as stromal cell-derived factor-1α or SDF-1α) in the marrow niche.4-6 Increased CXCR4 on AML cells is associated with adverse outcomes, supporting the idea of a protective niche that is dependent on CXCR4 expression.7, 8
CXCR4-CXCL12 inhibition mobilizes marrow cells, and the CXCR4 inhibitor plerixafor is FDA approved for stem cell mobilization in non-Hodgkin's lymphoma and multiple myeloma prior to autologous SCT.9 In pre-clinical in vivo leukemia models, directed inhibition of CXCR4 resulted in mobilization of leukemic cells into circulation.10, 11 By interfering with CXCR4-CXCL12 interaction, plerixafor may also prevent internalization of CXCR4, thereby disrupting downstream signaling (for instance, in the PI3K/AKT pathway) and further sensitizing leukemic cells to therapy.10-12 A recent phase 1 study demonstrated sensitization was possible in humans, where AML patients who were treated with plerixafor prior to chemotherapy showed mobilization of leukemic cells and chemosensitivity to a standard ara-C plus anthracycline regimen.12
Granulocyte-colony stimulating factor (G-CSF), commonly used in stem cell mobilization, also disrupts leukocyte-stromal interactions and mobilizes leukocytes and leukocyte progenitors through alternative mechanisms.13 Two known pathways of cellular release include the generation of a proteolytic microenvironment14-16 and suppression of anchor cells in the stem cell niche.17-19 Additionally, G-CSF also disrupts the CXCR4/CXCL12 interaction via mechanisms independent from plerixafor.20, 21 When given in combination, G-CSF plus plerixafor are synergistic in mobilization effects.22
We hypothesized that disruption of stromal-leukemia interactions using G-CSF in combination with plerixafor during conditioning chemotherapy prior to allo-SCT would promote release of leukemic cells from the niche, sensitize them to the chemotherapy preparative regimen, and thereby reduce the risk of relapse post allogeneic hematopoietic transplantation. In this phase 1/2 study, we evaluated the administration of G-CSF and the CXCR4 specific inhibitor plerixafor in conjunction with the busulfan-fludarabine preparative regimen.
Patients, materials, and methods
Study group eligibility
Eligible patients were between the ages of 18 and 65, had a diagnosis of AML (in remission, relapse, or primary induction failure), MDS with an intermediate or high risk International Prognostic Scoring System (IPSS) score having failed to respond or recurred after chemotherapy, AML arising from MDS, or CML failing to respond to tyrosine kinase inhibitor and > 5% blasts in blood or bone marrow. Additional eligibility details may be found in Supplementary information. This trial is registered at ClinicalTrials.gov with identifier NCT00822770.
Drug administration and study design
The dosing schedule for plerixafor, busulfan, fludarabine and rabbit antithymocyte globulin is shown in Figure 1. G-CSF was administered at a dose of 10 μg/kg subcutaneous injection daily for 6 days starting on day −9. Plerixafor was administered at doses of 0, 80, 160 or 240 μg/kg daily for 4 days starting on day −7, 8 hours (+/− 4 hours) prior to fludarabine administration and 9 hours (+/− 4 hours) prior to busulfan administration on day −6. The phase 2 portion of the study used the maximum tolerated dose from the phase 1 portion, with the primary outcome of time to treatment failure, defined as either disease recurrence or death; study patients were compared to historical data using these outcomes. Timing of plerixafor administration prior to chemotherapy was based on maximal mobilization of 9-10 hours in humans observed in previous pharmacodynamic studies.23, 24 The busulfan-fludarabine conditioning regimen was administered as fludarabine 40 mg/m2 IV followed by fixed-dose busulfan 130 mg/m2 IV, each given daily for 4 days on days −6 to −3. Additional details of drug administration can be found in Supplementary information.
Figure 1.

Dosing schedule. Rabbit antithymocyte globulin (ATG) was given only to patients with unrelated donors, at a dose of 0.5 mg/kg on day −3, 1.5 mg/kg on day −2 and 2mg/kg on day −1.
Study group
A total of 45 patients (34 AML, 7 MDS, and 4 CML) were enrolled in the study. One patient, who had de novo AML, received G-CSF without plerixafor (Cohort 1, dose = 0 μg/kg plerixafor). Characteristics of patients who did receive plerixafor (n = 44) are shown in Table 1. Among AML/MDS patients, a total of 19 (47.5%) had primary refractory disease, 4 (10%) were in first or second relapse, 13 (32.5%) were in first complete remission, 2 (5%) were in second complete remission, and 2 (5%) were relapsed after allogeneic stem cell transplant, underwent subsequent treatment and were in CR at the time of second transplant.
Table 1.
Characteristics of all patients receiving G-CSF plus plerixafor (n = 44).
| Characteristic | N |
|---|---|
| Diagnosis (%) | |
| AML/MDS | 40 (90.9) |
| AML total | 33 (75) |
| De novo AML | 22 (50) |
| Treatment related AML | 4 (9.1) |
| AML from MDS | 6 (13.6) |
| Therapy related AML from MDS | 4 (9.1) |
| AML from MPD | 1 (2.3) |
| MDS total | 7 (15.9) |
| Treatment related MDS | 3 (6.8) |
| CML | 4 (9.1) |
| Response prior to transplant (%) | |
| AML/MDS (n = 40) | |
| Primary refractory | 19 (47.5) |
| 1st relapse refractory | 3 (7.5) |
| 2nd relapse refractory | 1 (2.5) |
| 1st complete remission | 13 (32.5) |
| 2nd complete remission | 2 (5) |
| Relapse post-allogeneic transplant | 2 (5) |
| CML (n = 4) | |
| Second chronic phase | 3 (75) |
| Blast phase | 1 (25) |
| Cytogenetics (%) | |
| AML/MDS (n = 40) | |
| Favorable | 2 (5) |
| Intermediate | 22 (53.7) |
| Unfavorable | 16 (40) |
| CML (n = 4) | |
| Ph+ | 4 (100) |
| Complex karyotype | 1 (25) |
| FLT3 status AML/MDS, n = 40 (%) | |
| FLT3-ITD positive | 11 (28) |
| FLT3-ITD negative | 25 (63) |
| FLT3-D835 positive | 1 (3) |
| FLT3 status not determined | 3 (8) |
| Age | |
| Median age, y (range) | 54 (25-65) |
| Prior therapies | |
| Median prior regimens (range) | 2 (0-6) |
| Donor (%) | |
| Sibling | 22 (50) |
| Unrelated | 22 (50) |
| Plerixafor dose (%) | |
| Cohort 2: 80 μg/kg | 3 (6.8) |
| Cohort 3: 160 μg/kg | 8 (18.2) |
| Cohort 4: 240 μg/kg | 33 (75) |
Disease evaluation, chimerism assessment and toxicity assessment
Prior response for AML patients and response to transplant was determined based on the revised International Working Group criteria for AML response.25 At day +30, and +100 post transplant, peripheral blood and bone marrow MNCs were tested by flow cytometry for chimerism and immune reconstitution by evaluating myeloid cells and T-cells using institutional standards. Maximum Tolerated Dose (MTD) of plerixafor used for the phase 2 portion of the study was determined using the continual reassessment method (CRM).26 Additional details can be found in Supplementary information.
Mobilization and biomarker analysis
Human mononuclear cells (MNCs) were isolated from peripheral blood (PB) samples and BM aspirates for flow cytometry and fluorescent in situ hybridization. Blood samples were drawn in the morning daily on day −9, −8, −7, −6, and −3, and bone marrow biopsies were performed at day +30 and +100 (+/− 15 days). All flow cytometry was performed on a Becton-Dickinson LSR II flow cytometer. MNCs isolated pre-transplant were analyzed by immunophenotyping using antibodies against CD34, CXCR4 (CD184), and VLA-4 (CD49D) (BD Pharmingen). For analysis of CXCR4 expression, we used 1D9 antibody that binds to the N-terminus of CXCR4 and is not inhibited by plerixafor.12, 27 Longitudinal changes in WBCs were evaluated using a random effect model.28 Mean fluorescence intensity (MFI) for CXCR4 was evaluated for days −9, −8, −7, −6, −5 (when available, n = 6), and day −3 for each patient using the ratio (MFI CXCR4 / MFI isotype control). Changes in CXCR4 MFI between two days were analyzed using paired t-tests. Fluorescent in situ hybridization techniques, fold changes for biomarker analysis and additional statistical details are described in Supplementary information.
Statistical methods for comparison to historical data
The primary endpoint for the study was time to treatment failure (relapse or death), compared to a historical dataset. The historical cohort consisted of 337 patients with AML or MDS who underwent allo-SCT after the same busulfan-fludarabine conditioning regimen, but without G-CSF/plerixafor. The initial busulfan-fludarabine treatment was described by de Lima, et. al., Blood, 2004.29 Our initial historical data set included all patients that received this regimen at our center. We included in our analysis similar aged patients transplanted after 2005. To correct for trial-versus-historical bias, patients in the combined trial and historical samples were stratified by cytogenetics (good/intermediate vs. bad) and disease status at time of transplant (CR vs. non-CR/relapse post-transplant), producing 4 strata.30 Comparison of characteristics between trial and historical patients used for analysis are found in Table 2. Additional statistical analysis is described in Supplementary information.
Table 2.
Characteristics of G-CSF plus plerixafor AML/MDS study patients vs. historical patients.
| Parameter | Category | GCSF+plerixafor (N = 40) | Historical (N = 164) | p-value* |
|---|---|---|---|---|
| Age, mean (range) | 53.5 (31, 65) | 51.6 (31, 65) | 0.16 | |
| Gender, N (%) | Female | 23 (57.5) | 77 (47) | 0.29 |
| Male | 17 (42.5) | 87 (53) | ||
| Diagnosis, N (%) | AML | 26 (65) | 101 (61.6) | 0.89 |
| sAML | 7 (17.5) | 27 (16.5) | ||
| MDS | 7 (17.5) | 36 (21.9) | ||
| Donor source, N (%) | Unrelated | 21 (52.5) | 85 (51.8) | 1.0 |
| Sibling | 19 (47.5) | 77 (47) | ||
| Related other | 0 (0) | 2 (1.2) | ||
| Allotype, N (%) | 10/10 matched related | 19 (47.5) | 75 (45.7) | 0.06 |
| 10/10 matched unrelated | 21 (52.5) | 71 (43.3) | ||
| 9/10 matched | 0 (0) | 18 (11) | ||
| Cell source, N (%) | Peripheral blood | 27 (67.5) | 108 (65.9) | 1.0 |
| Bone marrow | 13 (32.5) | 56 (34.1) | ||
| FLT3-ITD, N (%) | Positive | 11 (27.5) | 15 (9.2) | <0.01 |
| Negative | 26 (65) | 120 (73.1) | ||
| Undetermined | 3 (7.5) | 29 (17.7) |
p-values calculated using Wilcoxon rank sum test for age, and generalized Fisher exact test for all other parameters.
Results
Plerixafor dose escalation and toxicities
Phase 1 plerixafor dose escalation was performed in 16 patients. There were no toxicities ascribed to the G-CSF plus plerixafor component of the regimen and 29 patients were enrolled in the phase 2 part of the trial using 240 μg/kg of plerixafor. The total number of adverse events by system and grade in patients who received G-CSF plus plerixafor is shown in Supplementary Table 1. Three patients (7%) had early death, and no early deaths were attributable to the study drugs. CR status did not correlate with maximum toxicity grade (Supplementary Table 2). There was no evidence of significant delays in neutrophil recovery (median 12 days, range 10-22) or platelet recovery (median 12.5 days, range 0-74) compared to historical data with busulfan-fludarabine conditioning alone.29
Clinical activity
Responses for all patients receiving G-CSF/plerixafor, categorized by disease (AML/MDS and CML) are shown in Table 3. Among all 40 AML/MDS patients who received G-CSF plus plerixafor prior to transplant, 37 (92.5%) had a complete or continued remission (CR or CCR), 1 (2.5%) had no response, and 2 (5%) had early death. Of the 25 (62.5%) patients with active disease (relapse/refractory) at study entry, 23 (92%) achieved a CR, 1 (4%) patient had NR, and 1 (4%) patient had early death. Overall survival for patients in CR at the time of transplant versus those not in CR is shown in Figure 2A. Median follow-up for all study patients was 11.6 months (range, 0.5-36.4 months).
Table 3.
Outcomes for AML/MDS/CML patients receiving G-CSF plus plerixafor (n = 44).
| Outcome | N |
|---|---|
| Responses total (%) | |
| Complete remission total | 39 (88.6) |
| No response / Early death total | 5 (11.4) |
| Relapse (%) | 25 (56.8) |
| Median follow-up, d (range) | 324 (16-1018) |
| Response by disease (%) | |
| AML/MDS (n = 40) | |
| Complete remission (CR) | 21 (52.5) |
| Continuous complete remission (CCR) | 16 (40) |
| No response (NR) | 1 (2.5) |
| Early death (ED) | 2 (5) |
| CML (n = 4) | |
| Complete molecular remission | 1 (25) |
| Major molecular remission | 1 (25) |
| NR | 1 (25) |
| ED | 1 (25) |
Figure 2.

Overall survival and relapse free survival among AML/MDS patients. A) OS of patients by disease status at time of transplant, CR vs. non-CR/relapsed post-transplant. B) Kaplan-Meier estimates for historical data vs. study data. B) Overall survival (left panel) and Relapse free survival (right panel). C) Overall survival estimates and D) Relapse free survival estimates are shown for each of the four strata in each panel. For both C) and D) the four strata are: (1) (upper left) Non-CR, unfavorable cytogenetics; (2) (upper right) Non-CR, intermediate/favorable cytogenetics; (3) (lower left) CR, unfavorable cytogenetics; and (4) (lower right) CR intermediate/favorable cytogenetics. Supplementary Table 7 reports analyses of the difference between survival probabilities for overall and progression free survival between the groups.
Four patients transplanted on protocol had CML and were analyzed separately. All four patients (100%) carried the Philadelphia chromosome (Ph+), and one patient (25%) also had other complex karyotypic abnormalities. The patient with karyotypic evolution was in blast phase at transplant. After transplant, one patient (25%) achieved a complete molecular response (durable >2 years post-transplant), one patient (25%) achieved a major molecular response (subsequently relapsed and died during course 1 of salvage chemotherapy >1 year post-transplant), and one patient each (25%) had NR (patient in blast phase at time of transplant) and early death.
Comparison to historical patients
We compared clinical outcomes of AML/MDS patients receiving G-CSF plus plerixafor with fixed dose busulfan-fludarabine and allogeneic hematopoietic transplantation (n = 40) to a historical data set of stratified, analogous AML/MDS patients from our institution transplanted with the same conditioning regimen in the absence of G-CSF/plerixafor (n = 164, stratification and sub-sample sizes shown in Supplementary Table 3).
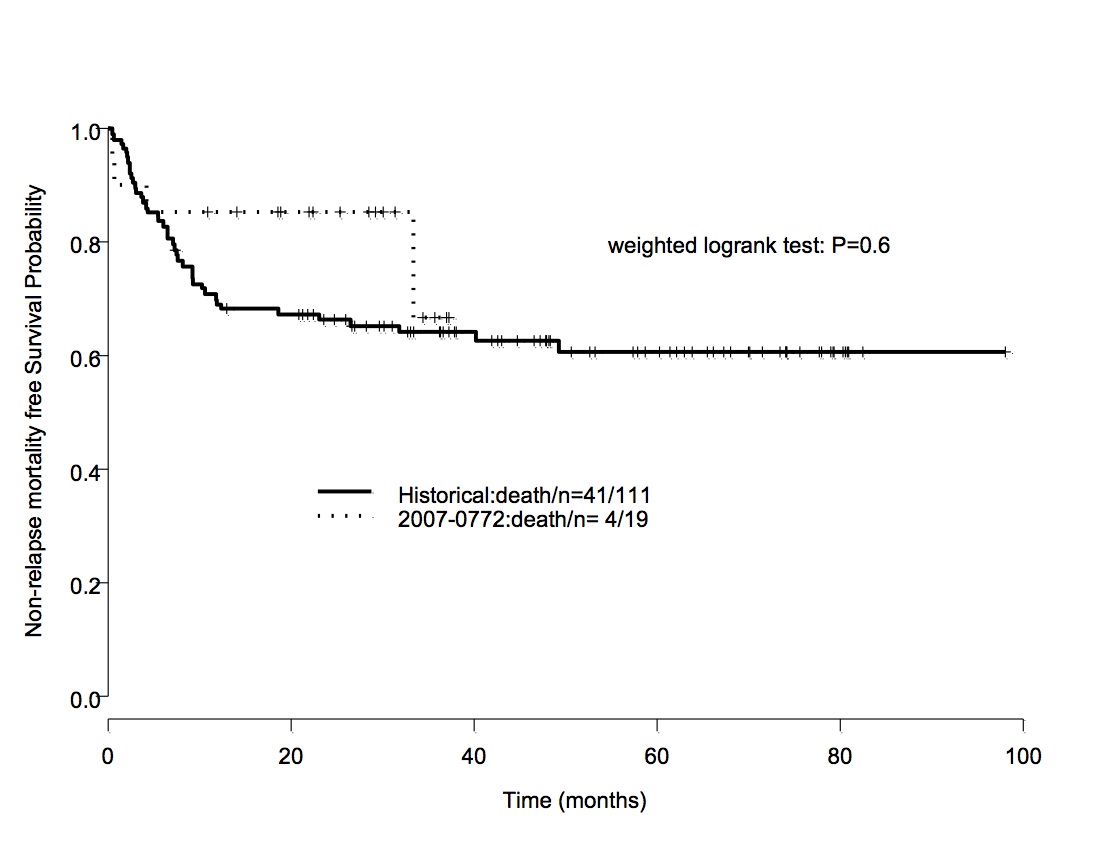
In the stratum-weighted event time comparisons, OS was not significantly different between the study and historical patients (weighted logrank p-value = 0.79. There was a trend towards inferior RFS which was not statistically significant p = 0.10; Figure 2B-D, Supplementary Table 4). In the stratum-weighted comparison of donor immune reconstitution, there was a significantly larger fraction of patients in the study group with complete myeloid chimerism at day +30 and day +100 (p-values < 0.01 and = 0.02, respectively, Table 4, Supplementary Table 5). Fewer study patients had ≥80% lymphoid chimerism at day +30 and day +100, but these differences were not significant (Table 4). Among patients who received G-CSF plus plerixafor, there was a lower incidence of grade 1 acute GvHD (p-value = 0.01), and a non-significant lower incidence of grade 2 acute GvHD (p-value = 0.08, Table 4, Supplementary Table 5). No study patient (0%) experienced grade 3 or 4 acute GvHD, while the incidence of grade 3 and 4 GvHD was 5.5% (9/164) in the historical population (Table 4). There was also a lower incidence of chronic GvHD in evaluable study vs. historical patients (p-value < 0.01, Table 4). Lower rates of GvHD among study patients were also observed when patients were categorized by donor type (Supplementary Table 6). Among patients who died, there was greater relapse related death among study patients (84% study vs. 56% historical), whereas there was greater non-relapse related mortality among historical patients (16% study vs. 44% historical, Supplementary Table 7). Kaplan Meier estimates of survival based on non-relapse mortality show no significant difference between the groups using a stratified weighted comparison (weighted log-rank p-value = 0.6, Supplementary Figure 1).
Table 4.
Incidence of GvHD and chimerism among evaluable study vs. historical patients.
| Parameter | G-CSF+plerixafor No./N (%) | Historical No./N (%) | p-value* |
|---|---|---|---|
| Grade 1 acute GvHD | 10/40 (25) | 74/164 (45.1) | 0.01 |
| Grade 2 acute GvHD | 9/40 (22.5) | 52/164 (31.7) | 0.08 |
| Grade 3/4 acute GvHD | 0/40 (0) | 9/164 (5.5) | NA |
| Chronic GvHD | 8/38 (21) | 65/138 (47.1) | <0.01 |
| Myeloid 100% chimerism at day +30 | 34/37 (91.9) | 99/144 (68.8) | <0.01 |
| Myeloid 100% chimerism at day +100 | 23/30 (76.7) | 67/107 (62.6) | 0.02 |
| T-cell 100% chimerism at day +30 | 12/36 (33.3) | 49/141 (34.8) | 0.42 |
| T-cell 100% chimerism at day +100 | 11/29 (37.9) | 42/107 (39.3) | 0.35 |
| T-cell ≥80% chimerism at day +30 | 18/36 (50) | 85/141 (60.3) | 0.10 |
| T-cell ≥80% chimerism at day +100 | 18/29 (62.1) | 77/107 (72) | 0.11 |
p-values are based on stratified comparisons.
Cell mobilization
We analyzed PB samples by complete blood count with differential and flow cytometry from 5 separate days: day −9 (baseline prior to treatment with G-CSF/plerixafor), days −8 and −7 (after treatment with G-CSF), day −6 (after treatment with G-CSF/plerixafor and prior to Bu-Flu), and day −3 (after Bu-Flu). All 44 patients receiving plerixafor had cell counts analyzed for white blood cells, blasts, and cells positive for CD34, CXCR4, and VLA-4. Mean fold changes for these populations show mobilization from baseline of day −9 and are plotted in Figure 3A-B. Maximum mean fold changes were 5 for PB blasts, >22 for CD34+ cells, and >38 for CXCR4+ cells by day −3 compared to baseline. Complete fold change data are presented in Supplementary Table 8.
Figure 3.

Biomarker analysis over time using different methods for evaluation and comparison. A-C) Fold change (calculated for each patient as ratio of measured value over value at baseline) analysis plotted for various cell populations and cell surface markers. Mean fold changes for all patients from baseline of day −9 with standard error are shown. At base of panel C), administration days for doses of G-CSF (G), plerixafor (P), busulfan-fludarabine (BuFlu) are shown (see Figure 1 for complete details). Fold changes for A: white blood cells (WBCs) and blasts; B: CXCR4+, CD34+, and VLA-4+ cells; C: FISH+ and FISH- cells for patients with informative cytogenetics; D) Longitudinal analysis using a random effect model (see Supplementary Table 7) of estimated mean WBC as a function of time, with 95% confidence bands, for the 4 strata based on disease status at time of transplant and cytogenetics, using mean age and mean log (BM blasts): (1) (upper left) Non-CR with unfavorable cytogenetics, (2) (upper right) Non-CR with intermediate/favorable cytogenetics, (3) (lower left) CR with unfavorable cytogenetics, and (4) (lower right) CR with intermediate/favorable cytogenetics; E-F) Change in mean fluorescence intensity (MFI) of CXCR4 (level of CXCR4 surface expression) during conditioning. E) Mean MFI with standard error over time (* denotes p-value < 0.05, ** denotes p-value < 0.01). F) Scatter plot showing each patient's CXCR4 MFI. Values shown for all p-values < 0.1. At base of panels E) and F), administration days for doses of G-CSF (G), plerixafor (P), busulfun-fludarabine (BuFlu) are shown (see Figure 1 for complete details).
To determine the relative proportion of mobilization of leukemic and non-leukemic cells, we performed FISH analysis on MNCs from peripheral blood of patients with informative cytogenetics (n = 22). FISH probes used, counted events, and calculated absolute leukemic cells × 109/L for each patient tested are shown in Supplementary Table 9. Over the first three days, the increase in FISH+ (leukemic) cells was higher than FISH- (non-leukemic) cells (Figure 3C), indicating that cytogenetically abnormal leukemic cells were mobilized more frequently than normal cells. To verify that mobilization of WBCs was independent of baseline characteristics, we performed a longitudinal analysis using a random effects model with covariates of possible influence (disease status, cytogenetics, age and % BM blasts, Supplementary Table 10). WBCs were effectively mobilized for patients in each stratum (Figure 3D). Patients in CR with unfavorable cytogenetics generally appeared to have inferior mobilization, and those not in CR with intermediate/favorable cytogenetics appeared to have superior mobilization (Figure 3D). Finally, no correlation was found between plerixafor dose escalation and mobilization effects on WBCs, blasts, CD34+ cells, or FISH+ cells (Supplementary Table 11). We did find that increased baseline WBC counts or blasts (BM, PB absolute, or PB percentage) strongly correlated with increased peak mobilization of WBCs, blasts, and CD34+ cells, and was significantly correlated with an increase in percentage CXCR4+ cells in the first three days of administration of G-CSF and plerixafor (Supplementary Table 12 and Supplementary Figure 2).
We determined the mean fluorescence intensity (MFI, which corresponds to level of surface expression) of CXCR4 for each day of analysis for each patient. We noted an initial decrease in mean MFI from day −8 to day −7 with a subsequent increase from day −7 to day −3 (Figure 3E-F). There was an overall increase in CXCR4 surface expression over the entire course of the pre-transplant treatment.
Discussion
Our phase 1 study results indicate that G-CSF plus plerixafor up to 240 μg/kg is safe when given to patients with AML undergoing allogeneic transplant with an established IV busulfan-fludarabine regimen. While mobilization of blasts occurred, there were no instances of adverse events secondary to leukostasis. Significant mobilization of WBCs, blasts, CD34+, CXCR4+, and VLA-4+ cells was observed. The intended biological effect of our approach, to mobilize leukemic clones, was apparent by detecting FISH+ (leukemic) cells in patients with informative cytogenetics. For many cell populations, continued mobilization from baseline was observed even after chemotherapy was administered. This may represent continued effect of G-CSF plus plerixafor, mobilization effects of chemotherapy, or slow kinetics of busulfan-induced myelosuppression, which occurs in a time-dependent fashion, and possibly in an apoptosis-independent fashion.31, 32 However, there was a decrease in FISH+ MNCs after administration of chemotherapy, suggesting that chemotherapy was effective in eliminating leukemic cells.
We found that FISH+ cells were mobilized more readily than non-leukemic cells, and this difference increased significantly over time. No differential mobilization of leukemic cells was seen when plerixafor was used as a single agent,12 indicating the likely role of G-CSF in the observed phenomenon. A number of reasons could explain preferential mobilization of leukemic clones. Our treatment might induce mobilization of abnormal leukemic cells more readily than non-leukemic cells, especially if there is higher dependence of leukemic cells on CXCR4/CXCL12 interactions. Alternatively, more leukemic clones might occupy the bone marrow leading to greater numbers of leukemic cells being mobilized over time. Treatment with G-CSF plus plerixafor might induce a proliferation or differentiation effect with mobilization that results in preferential expansion of leukemic cells in peripheral blood. G-CSF is responsible for activating normal hematopoietic stem cells into proliferation, and there is limited data on its proliferative and differentiation effect in AML.33 G-CSF has also been shown to negatively modulate neutrophil apoptosis, another potential mechanism for increase in cell number.34, 35
G-CSF plus plerixafor led to accumulation of increased numbers of circulating CXCR4+ cells and cells with increased surface expression of CXCR4 over time. The substantial increase in CXCR4+ cells suggests that the addition of G-CSF to plerixafor in the context of treating leukemia patients better mobilizes CXCR4+ cells. Mean fluorescence intensity of CXCR4 expression showed that after an initial decrease, our population had increased leukocyte CXCR4 expression over time. A similar effect has been observed previously when plerixafor was used alone in patients with AML undergoing induction chemotherapy and was shown to be due to plerixafor-mediated inhibition of CXCR4 internalization by CXCL12.12 Pre-clinical data suggest that G-CSF downregulates surface CXCR4 expression on AML blasts in an in vivo xenograft model,12 and this may explain the initial decrease in CXCR4 MFI between day −8 and −7 after G-CSF is used alone. CXCR4 levels as measured by MFI were elevated upon addition of plerixafor and chemotherapy, however the contribution of each cannot be determined given the concomitant administration of both. There is evidence that chemotherapy can induce CXCR4 expression, which may be a contributing factor in resistance to apoptosis.36
The comparison analysis suggested that G-CSF/plerixafor with busulfan-fludarabine conditioning prior to allo-SCT does not improve RFS in AML/MDS patients versus similar historical patients receiving the same conditioning without G-CSF/plerixafor. In fact, study patients had non-significantly worse RFS. While preclinical data suggested that disruptions of stroma-leukemia interactions would enhance chemosensitivity and improve outcomes of patients undergoing allo-SCT for hematological malignancies, our practical experience in this study suggests patient outcomes were not superior. OS also was not significantly different between the study and historical patients. Study patients had a lower incidence and severity of acute GvHD, and a lower incidence of chronic GvHD, and may have had a concomitant decreased graft versus leukemia (GvL) effect. There was non-significantly decreased lymphoid chimerism for study patients at day +30 and +100, supporting the observed decrease in GvHD. The non-significant difference in lymphoid chimerism may help explain the non-significant trend towards earlier relapse among study patients. There were some differences between the stratified study and historical patients, such as FLT3 status and level of matching (non-significant). These differences do not necessarily explain the strongly significant differences seen for GvHD and increased myeloid chimerism in study patients. When we evaluated rates of GvHD, we found higher fractions of historical patients had acute and chronic GvHD for patients receiving matched related or matched unrelated transplants, further suggesting treatment effect.
Interestingly, and in distinction to lymphoid engraftment, study patients had significantly increased complete myeloid chimerism compared to historical patients. The reason for the reciprocal myeloid and lymphoid engraftment effects between study and historical patients is not understood, but suggests that G-CSF/plerixafor given to recipients prior to transplant has unanticipated effects on engraftment of transplanted cells. Inhibition of the CXCR4-CXCL12 axis alters the activity of T-regulatory cells (T-regs) and mobilizes them out of the protective bone marrow into circulation.37, 38 Additional recent evidence suggests that G-CSF also modulates both the microenvironment and T-cells in a way that promotes the expansion of T-regs leading to attenuation of GvHD.39 An alternative explanation could be deleterious effects of G-CSF on the bone marrow hematopoietic niche making it less hospitable for normal HSC engraftment, as has been suggested in a preclinical in vivo model.21 Finally, although plerixafor inhibits CXCR4, we show evidence it contributes to increased surface expression of CXCR4. Increases in surface CXCR4 also may have the effect of protecting surviving leukemic stem cells in the marrow niche. The mechanism by which our patients had relapse, if different from historical patients, may be elucidated by further study using mouse modeling of hematopoietic transplant. Finally, while not the intent of this study, the incidental finding of decreased GvHD and increased myeloid engraftment may be especially important for non-malignant reduced intensity conditioning and cord blood transplants, where GvL is not necessary, and decreased GvHD with increased myeloid engraftment may be particularly useful.
Our study demonstrated the safety of G-CSF plus plerixafor with busulfan-fludarabine conditioning, and its superior ability to mobilize leukemic cells. Comparison to historical data suggests that OS was not superior for patients in the study group, and RFS was non-significantly inferior. While the use of these agents in the setting of multimodal therapy and/or allogenic stem cell transplantation remains to be defined, these findings are intriguing. Current work is underway to capitalize on knowledge of mobilization from this study using timed sequential conditioning prior to allo-SCT.
Supplementary Material
{kind=link}
{kind=link}
Acknowledgements
This work was supported by the National Institutes of Health/National Cancer Institute grants P01 CA55164-19, P01 CA049639-21, R21 CA137637 (to MK), CCSG P30 CA016672, and the Paul and Mary Haas Chair in Genetics (to M.A.). The authors thank Professor Axel Zander (University Medical Center Hamburg-Eppendorf Clinic for Stem Cell Transplantation, Hamburg, Germany) for scientific input on the manuscript.
Footnotes
Conflict-of-interest disclosure: MK, RC received research funding from Genzyme. RC served as a consultant for Genzyme.
Authorship
M.K. designed research, contributed essential tools, performed research, analyzed data, wrote the manuscript, funded the studies. C.B.B. performed research, analyzed data, wrote the manuscript. P.F.T., Z.Z. performed research, analyzed data. E.S., S.C., P.K., A.A., U.P., P.A., Y.N., S.P. contributed essential tools. W.Q., J.C., G.R., B.M, R.W., H.L., W.S., G.W., A.G., R. Cool, performed research, analyzed data. M.A., R. Champlin. designed research, contributed essential tools, analyzed data.
Supplementary information
Supplementary information is available at BMT's website.
References
- 1.van den Brink MRM, Porter DL, Giralt S, Lu SX, Jenq RR, Hanash A, et al. Relapse after allogeneic hematopoietic cell therapy. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation. 2010;16(1 Suppl):S138–145. doi: 10.1016/j.bbmt.2009.10.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ninomiya M, Abe A, Katsumi A, Xu J, Ito M, Arai F, et al. Homing, proliferation and survival sites of human leukemia cells in vivo in immunodeficient mice. Leukemia : official journal of the Leukemia Society of America, Leukemia Research Fund, U.K. 2007;21(1):136–142. doi: 10.1038/sj.leu.2404432. [DOI] [PubMed] [Google Scholar]
- 3.Meads MB, Gatenby RA, Dalton WS. Environment-mediated drug resistance: a major contributor to minimal residual disease. Nature Reviews Cancer. 2009;9(9):665–674. doi: 10.1038/nrc2714. [DOI] [PubMed] [Google Scholar]
- 4.Möhle R, Bautz F, Rafii S, Moore MA, Brugger W, Kanz L. The chemokine receptor CXCR-4 is expressed on CD34+ hematopoietic progenitors and leukemic cells and mediates transendothelial migration induced by stromal cell-derived factor-1. Blood. 1998;91(12):4523–4530. [PubMed] [Google Scholar]
- 5.Möhle R, Schittenhelm M, Failenschmid C, Bautz F, Kratz-Albers K, Serve H, et al. Functional response of leukaemic blasts to stromal cell-derived factor-1 correlates with preferential expression of the chemokine receptor CXCR4 in acute myelomonocytic and lymphoblastic leukaemia. British journal of haematology. 2000;110(3):563–572. doi: 10.1046/j.1365-2141.2000.02157.x. [DOI] [PubMed] [Google Scholar]
- 6.Voermans C, van Heese WPM, de Jong I, Gerritsen WR, van Der Schoot CE. Migratory behavior of leukemic cells from acute myeloid leukemia patients. Leukemia : official journal of the Leukemia Society of America, Leukemia Research Fund, U.K. 2002;16(4):650–657. doi: 10.1038/sj.leu.2402431. [DOI] [PubMed] [Google Scholar]
- 7.Rombouts EJC, Pavic B, Löwenberg B, Ploemacher RE. Relation between CXCR-4 expression, Flt3 mutations, and unfavorable prognosis of adult acute myeloid leukemia. Blood. 2004;104(2):550–557. doi: 10.1182/blood-2004-02-0566. [DOI] [PubMed] [Google Scholar]
- 8.Konoplev S, Rassidakis GZ, Estey E, Kantarjian H, Liakou CI, Huang X, et al. Overexpression of CXCR4 predicts adverse overall and event-free survival in patients with unmutated FLT3 acute myeloid leukemia with normal karyotype. Cancer. 2007;109(6):1152–1156. doi: 10.1002/cncr.22510. [DOI] [PubMed] [Google Scholar]
- 9.Brave M, Farrell A, Ching Lin S, Ocheltree T, Pope Miksinski S, Lee S-L, et al. FDA review summary: Mozobil in combination with granulocyte colony-stimulating factor to mobilize hematopoietic stem cells to the peripheral blood for collection and subsequent autologous transplantation. Oncology. 2010;78(3-4):282–288. doi: 10.1159/000315736. [DOI] [PubMed] [Google Scholar]
- 10.Zeng Z, Xi Shi Y, Samudio IJ, Wang RY, Ling X, Frolova O, et al. Targeting the leukemia microenvironment by CXCR4 inhibition overcomes resistance to kinase inhibitors and chemotherapy in AML. Blood. 2009;113(24):6215–6224. doi: 10.1182/blood-2008-05-158311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Nervi B, Ramirez P, Rettig MP, Uy GL, Holt MS, Ritchey JK, et al. Chemosensitization of acute myeloid leukemia (AML) following mobilization by the CXCR4 antagonist AMD3100. Blood. 2009;113(24):6206–6214. doi: 10.1182/blood-2008-06-162123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Uy GL, Rettig MP, Motabi IH, McFarland K, Trinkaus KM, Hladnik LM, et al. A phase 1/2 study of chemosensitization with the CXCR4 antagonist plerixafor in relapsed or refractory acute myeloid leukemia. Blood. 2012;119(17):3917–3924. doi: 10.1182/blood-2011-10-383406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Motabi IH, DiPersio JF. Advances in stem cell mobilization. Blood reviews. 2012 doi: 10.1016/j.blre.2012.09.003. [DOI] [PubMed] [Google Scholar]
- 14.Lévesque JP, Takamatsu Y, Nilsson SK, Haylock DN, Simmons PJ. Vascular cell adhesion molecule-1 (CD106) is cleaved by neutrophil proteases in the bone marrow following hematopoietic progenitor cell mobilization by granulocyte colony-stimulating factor. Blood. 2001;98(5):1289–1297. doi: 10.1182/blood.v98.5.1289. [DOI] [PubMed] [Google Scholar]
- 15.Lévesque J-P, Hendy J, Takamatsu Y, Williams B, Winkler IG, Simmons PJ. Mobilization by either cyclophosphamide or granulocyte colony-stimulating factor transforms the bone marrow into a highly proteolytic environment. Experimental Hematology. 2002;30(5):440–449. doi: 10.1016/s0301-472x(02)00788-9. [DOI] [PubMed] [Google Scholar]
- 16.Lévesque J-P, Hendy J, Winkler IG, Takamatsu Y, Simmons PJ. Granulocyte colony-stimulating factor induces the release in the bone marrow of proteases that cleave c-KIT receptor (CD117) from the surface of hematopoietic progenitor cells. Experimental Hematology. 2003;31(2):109–117. doi: 10.1016/s0301-472x(02)01028-7. [DOI] [PubMed] [Google Scholar]
- 17.Winkler IG, Sims NA, Pettit AR, Barbier V, Nowlan B, Helwani F, et al. Bone marrow macrophages maintain hematopoietic stem cell (HSC) niches and their depletion mobilizes HSCs. Blood. 2010;116(23):4815–4828. doi: 10.1182/blood-2009-11-253534. [DOI] [PubMed] [Google Scholar]
- 18.Chow A, Lucas D, Hidalgo A, Méndez-Ferrer S, Hashimoto D, Scheiermann C, et al. Bone marrow CD169+ macrophages promote the retention of hematopoietic stem and progenitor cells in the mesenchymal stem cell niche. The Journal of experimental medicine. 2011;208(2):261–271. doi: 10.1084/jem.20101688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Christopher MJ, Rao M, Liu F, Woloszynek JR, Link DC. Expression of the G CSF receptor in monocytic cells is sufficient to mediate hematopoietic progenitor mobilization by G-CSF in mice. The Journal of experimental medicine. 2011;208(2):251–260. doi: 10.1084/jem.20101700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lévesque J-P, Hendy J, Takamatsu Y, Simmons PJ, Bendall LJ. Disruption of the CXCR4/CXCL12 chemotactic interaction during hematopoietic stem cell mobilization induced by GCSF or cyclophosphamide. Journal of Clinical Investigation. 2003;111(2):187–196. doi: 10.1172/JCI15994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Winkler IG, Pettit AR, Raggatt LJ, Jacobsen RN, Forristal CE, Barbier V, et al. Hematopoietic stem cell mobilizing agents G-CSF, cyclophosphamide or AMD3100 have distinct mechanisms of action on bone marrow HSC niches and bone formation. Leukemia : official journal of the Leukemia Society of America. Leukemia Research Fund, U.K. 2012;26(7):1594–1601. doi: 10.1038/leu.2012.17. [DOI] [PubMed] [Google Scholar]
- 22.Broxmeyer HE, Orschell CM, Clapp DW, Hangoc G, Cooper S, Plett PA, et al. Rapid mobilization of murine and human hematopoietic stem and progenitor cells with AMD3100, a CXCR4 antagonist. The Journal of experimental medicine. 2005;201(8):1307–1318. doi: 10.1084/jem.20041385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Liles WC, Broxmeyer HE, Rodger E, Wood B, Hübel K, Cooper S, et al. Mobilization of hematopoietic progenitor cells in healthy volunteers by AMD3100, a CXCR4 antagonist. Blood. 2003;102(8):2728–2730. doi: 10.1182/blood-2003-02-0663. [DOI] [PubMed] [Google Scholar]
- 24.Stewart DA, Smith C, MacFarland R, Calandra G. Pharmacokinetics and pharmacodynamics of plerixafor in patients with non-Hodgkin lymphoma and multiple myeloma. Biology of blood and marrow transplantation : journal of the American Society for Blood and Marrow Transplantation. 2009;15(1):39–46. doi: 10.1016/j.bbmt.2008.10.018. [DOI] [PubMed] [Google Scholar]
- 25.Cheson BD, Bennett JM, Kopecky KJ, Büchner T, Willman CL, Estey EH, et al. Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. 2003:4642–4649. doi: 10.1200/JCO.2003.04.036. [DOI] [PubMed] [Google Scholar]
- 26.O'Quigley J, Pepe M, Fisher L. Continual reassessment method: a practical design for phase 1 clinical trials in cancer. Biometrics. 1990;46(1):33–48. [PubMed] [Google Scholar]
- 27.Förster R, Kremmer E, Schubel A, Breitfeld D, Kleinschmidt A, Nerl C, et al. Intracellular and surface expression of the HIV-1 coreceptor CXCR4/fusin on various leukocyte subsets: rapid internalization and recycling upon activation. Journal of immunology (Baltimore, Md. : 1950) 1998;160(3):1522–1531. [PubMed] [Google Scholar]
- 28.Diggle PJ, Heagerty P, Liang K-Y, Zeger S. Analysis of Longitudinal Data. First edition Oxford University Press; 2002. [Google Scholar]
- 29.de Lima M, Couriel D, Thall PF, Wang X, Madden T, Jones R, et al. Once-daily intravenous busulfan and fludarabine: clinical and pharmacokinetic results of a myeloablative, reduced-toxicity conditioning regimen for allogeneic stem cell transplantation in AML and MDS. Blood. 2004;104(3):857–864. doi: 10.1182/blood-2004-02-0414. [DOI] [PubMed] [Google Scholar]
- 30.Morgan SL. Matching Estimators of Causal Effects: Prospects and Pitfalls in Theory and Practice. Sociological Methods & Research. 2006;35(1):3–60. [Google Scholar]
- 31.Bishop JB, Wassom JS. Toxicological review of busulfan (Myleran). Mutation research. 1986;168(1):15–45. doi: 10.1016/0165-1110(86)90020-5. [DOI] [PubMed] [Google Scholar]
- 32.Meng A, Wang Y, Van Zant G, Zhou D. Ionizing radiation and busulfan induce premature senescence in murine bone marrow hematopoietic cells. Cancer Research. 2003;63(17):5414–5419. [PubMed] [Google Scholar]
- 33.Morrison SJ, Wright DE, Weissman IL. Cyclophosphamide/granulocyte colony- stimulating factor induces hematopoietic stem cells to proliferate prior to mobilization. Proceedings of the National Academy of Sciences of the United States of America. 1997;94(5):1908–1913. doi: 10.1073/pnas.94.5.1908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Colotta F, Re F, Polentarutti N, Sozzani S, Mantovani A. Modulation of granulocyte survival and programmed cell death by cytokines and bacterial products. Blood. 1992;80(8):2012–2020. [PubMed] [Google Scholar]
- 35.Adachi S, Kubota M, Lin YW, Okuda A, Matsubara K, Wakazono Y, et al. In vivo administration of granulocyte colony-stimulating factor promotes neutrophil survival in vitro. European journal of haematology. 1994;53(3):129–134. doi: 10.1111/j.1600-0609.1994.tb00660.x. [DOI] [PubMed] [Google Scholar]
- 36.Sison EAR, McIntyre E, Magoon D, Brown P. Dynamic chemotherapy-induced upregulation of surface CXCR4 expression as a mechanism of chemotherapy resistance in pediatric acute myeloid leukemia. Molecular cancer research : MCR. 2013 doi: 10.1158/1541-7786.MCR-13-0114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kean LS, Sen S, Onabajo O, Singh K, Robertson J, Stempora L, et al. Significant mobilization of both conventional and regulatory T cells with AMD3100. Blood. 2011;118(25):6580–6590. doi: 10.1182/blood-2011-06-359331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Zou L, Barnett B, Safah H, Larussa VF, Evdemon-Hogan M, Mottram P, et al. Bone marrow is a reservoir for CD4+CD25+ regulatory T cells that traffic through CXCL12/CXCR4 signals. Cancer Research. 2004;64(22):8451–8455. doi: 10.1158/0008-5472.CAN-04-1987. [DOI] [PubMed] [Google Scholar]
- 39.MacDonald KPA, Le Texier L, Zhang P, Morris H, Kuns RD, Lineburg KE, et al. Modification of T cell responses by stem cell mobilization requires direct signaling of the T cell by G-CSF and IL-10. Journal of immunology (Baltimore, Md. : 1950) 2014;192(7):3180–3189. doi: 10.4049/jimmunol.1302315. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.