

Abstract
Background
Little is known about heterogeneity in men's drinking behaviors and their related consequences across midadulthood, and moreover, whether individual or social factors may predict such differences. The present study examined 3 indicators of alcohol use; namely, alcohol volume, heavy episodic drinking (HED), and drinking-related problems for men in their 30s.
Methods
Participants were 197 at-risk men from the Oregon Youth Study assessed 5 times across ages 29–38 years. Growth mixture modeling with count outcomes was used to examine unobserved heterogeneity in alcohol trajectories. Associations of latent classes of alcohol users with (i) classes for the other alcohol indicators, (ii) alcohol use by peers and romantic partners, (iii) alcohol classes previously extracted from ages 18–29 years, and (iv) past year alcohol use disorder (AUD) diagnostic status at ages 35–36 years was examined.
Results
A 3-class solution afforded the best fit for each alcohol indicator. Alcohol problems were relatively established in the 30s, with an ascending use class found only for volume. Although relatively few men were in higher classes for all 3 indicators, 45% of the sample was in the highest class on at least 2 indicators of use. Peer drunkenness was a robust predictor of the alcohol classes. Concordance among classes of alcohol users was seen from the 20s to the 30s, with prior desistance likely to be maintained for alcohol volume and HED. AUD diagnoses at ages 35–36 years were more common in the higher classes obtained for alcohol volume and alcohol problems.
Conclusions
Many men in their 30s engaged in high volume of alcohol without frequent engagement in HED, likely relating to continuing alcohol problems. The convergence of men's alcohol use with that of their peers found at younger ages was maintained into early midadulthood.
Keywords: Alcohol Problems, Midadulthood, Heavy Drinking, Heterogeneity in Alcohol Use, Life-Course Alcohol Use
Introduction
Given the well-documented consequences of high levels of alcohol use – including medical, legal, marital, and occupational problems (Zucker et al., 1995) – there is now a large body of literature on the etiology of problematic drinking in adolescence and young adulthood (Hawkins et al., 1992; Stone et al., 2012). Alcohol problems that are manifested in early adulthood may desist, persist, or increase in later years (Capaldi et al., 2013). Given the high levels of alcohol consumption by young adults, an understanding of the determinants of subsequent use is critical for prevention and treatment of alcohol use disorders (AUDs).
Several prospective studies have examined developmental patterns of alcohol use, often called alcohol trajectories (e.g., Capaldi et al., 2013; Muthén and Muthén, 2000; Sher et al., 2011). Studies using growth mixture modeling (GMM; Muthén and Shedden, 1999) have examined unobserved heterogeneity in alcohol trajectories during the adolescent years, or from adolescence into emerging adulthood (e.g., Sher et al., 2011; Toumbourou et al., 2003; Tucker et al., 2003; Wiesner et al., 2007). Although GMM studies are relatively rare for noncollegiate young adults, such studies of older individuals are practically nonexistent.
Surprisingly little is known about changes in alcohol use during midlife (Helson and Soto, 2005), a period often characterized by high levels of alcohol use and alcohol problems (Grant et al., 2004). Although developmental approaches may be useful in understanding alcohol behavior in older adults (e.g., Oslin et al., 2005), we could only locate one GMM study conducted with participants in midadulthood, which was limited by the use of a clinical sample and retrospective reports (Jacob et al., 2005).
Patterns of Alcohol Volume, Heavy Episodic Drinking (HED), and Alcohol Problems in the 20S
A prior GMM study of alcohol use by the Oregon Youth Study (OYS) across the 20s that had separately examined trajectories of alcohol volume, HED, and alcohol problems found that unobserved heterogeneity in changes in alcohol use varied by indicator (Capaldi et al., 2013). For volume, 67% of the men fell into a high sustained use class. For HED, by contrast, most men followed a low and decreasing pattern. For volume and HED, there were similar numbers of men (16%–18%) who showed high levels at ages 19–20 years but later desisted. For alcohol problems, there was a downward trend across the period, although a relatively large proportion of the men (63%) showed a moderate level of sustained problems. For HED only, a latent class was found showing a pattern of increase across the 20s.
The possible associations of the classes obtained from the 20s with classes to be modeled for the same men in the 30s raise a number of key questions. First, do the men who showed relatively stable patterns of alcohol volume in the 20s (e.g., high sustained volume or low moderate volume of alcohol use) maintain that stability over the next decade? Next, do the men who showed high then sharply desisting patterns of volume and HED remain at very low levels in the 30s, or show patterns indicating relapse? Finally, does the latent HED class that showed an increasing trajectory across the 20s remain at high, or even increasing, HED levels in the 30s?
Social influence is related to substance use in adolescence and young adulthood, with alcohol use by peers being associated with an individual's alcohol use (Andrews et al., 2002; D'Amico et al., 2005). Influences of partners' alcohol use have been less studied, but associations between partners in their alcohol use have been found (Fleming et al., 2010; Leonard and Mudar, 2003; Mushquash et al., 2013), including in the OYS (Washburn et al., 2014). It was expected that both peer and partner alcohol use would discriminate among classes of alcohol use for the men, but due to some differences in measurement of alcohol use for peers and partners, no hypotheses were made regarding possible differential prediction.
The present study examined unobserved heterogeneity in alcohol trajectories for the three different indicators of alcohol use (volume, HED, and problems) used in the prior paper with the same sample (Capaldi et al., 2013), but now examining the men's alcohol use from the early to late 30s. Unconditional GMM with count data was conducted for the alcohol measures, and one of the classes was predefined to include abstainers, no HED, or men with no reported alcohol problems at all assessments in their 30s (Kreuter and Muthen, 2008). Next, GMM analyses were conducted that included alcohol behavior of the men's peers and romantic partners as covariates in the models to examine predictions of trajectory classes by social influences. Associations of membership across classes obtained with the different indicators were also examined. Finally, associations of 30s class memberships with (i) the men's alcohol classes previously modeled from ages 18–29 years and (ii) past year alcohol use disorders (AUD) diagnoses at ages 35–36 years were examined.
In summary, predictions were that (i) classes in the 30s would also show flatter levels over time than in the 20s (i.e., patterns would be more established, neither increasing nor decreasing over the 30s); (ii) both partner and peer alcohol use would be associated with the men's alcohol class membership; (iii) associations among the classes for the three alcohol indicators in the 30s would be statistically significant; (iv) significant associations would be found overall for the classes in the 20s and 30s, and men who showed relatively high then desisting patterns of alcohol volume, HED, and problems in the 20s would be likely to maintain desistance by being in a low group in the 30s; and (v) the classes would significantly discriminate between men who did versus did not meet criteria for an AUD diagnosis in the past year at ages 35–36 years.
Methods
Participants
The OYS recruited fourth-grade classes of boys in schools in higher-delinquency neighborhoods in a medium-sized metropolitan area in the Pacific Northwest (74% recruitment; Capaldi and Patterson, 1987; N = 206), who were studied almost annually. Five assessments waves – at ages 29–30, 30–31, 31–32, 35–36, and 37–38 years – were used in the current analysis (participation 85% or higher, N = 197). Using the Hollingshead Index (1975), participants were primarily White (90%) and from lower-class and working-class families (75%). The study had continuous IRB approval, and consent was obtained at each assessment.
Procedures
In-person interviews were conducted with the OYS men and their romantic partners, and questionnaires were administered. Partners were interviewed biennially during couples' assessments. Data from one to four assessments of partner drinking were included in the analysis, depending on the number of times each man participated with a partner.
Measures
Three adult alcohol indicators
The men provided self-reports for beer, wine, and hard liquor of (i) any use in the past year; (ii) for users, the number of times used (capped at 365); and (iii) amount drunk on a typical occasion (i.e., in units of less than 1, 1, 2, 3, 4 to 5, 6 or more), units were equilibrated for alcohol content. Volume of alcohol use was calculated from frequency of use multiplied by the usual amount consumed for beer, wine, and hard liquor, separately; the three values were summed to create the total yearly alcohol volume score. Scores were converted to average number of drinks per week in the last year by dividing by 52.1775 and rounding to the highest integer value.
HED was defined as the number of times of having drunk 5 or more drinks in a row in the past 2 weeks. At each wave, the variable was coded 0 = never, 1 = once, 2 = twice, and 3 = 3 or more times. Although this count variable was capped at 3 or more, only 5.3% (n = 11) to 6.8% (n = 14) of the men endorsed this category across their 30s.
The alcohol problems scale consisted of seven items regarding past year symptoms. One item (When drinking, how high/drunk do you usually get) was rescaled from 0 = not at all, 1 = a little bit, 2 = quite, and 3 = very to binary (coded as 0 = not at all, 1 = little bit/quite/very) to match the six other dichotomous items (coded as no = 0, yes = 1): being unable to stop drinking, being drunk, being drunk in a public place, passing out from drinking, throwing up from drinking, losing or breaking things when drinking, and usually getting drunk when drinking. Unstandardized alphas for the binary indicators ranged from .73 to .78 across time points. Composite scores were created by summing across items, yielding a count of the number of alcohol-related problems endorsed in the last year (range: 0 - 7).
Peer frequency of drunkenness
Men were asked ‘During the past year, how many of your friends got drunk once in a while?’, coded 1 = none of them, 2 = very few of them, 3 = some of them, 4 = most of them, and 5 = all of them. Correlations across time points ranged from .41 to .68 (p < .001 for all correlations), and the mean across time was calculated.
Partner heavy drinking
The men's partners reported on the number of alcoholic drinks consumed on a typical occasion during the past year. Correlations over time points ranged from .22 to .76 (p = .013 to < .001), and the mean was calculated.
Classes of alcohol use in early adulthood
Capaldi et al. (2013) examined the heterogeneity in alcohol use for the men across ages 20 through 30 years for the three alcohol measures described above, using GMM with continuous outcomes, and identified three classes for each: for alcohol volume: Low/Moderate (16.5%), High Desisting (16.5%), and High Chronic (67%); for HED: Moderate Desisting (18%), Moderate Increasing (13%), and Low Desisting (69%); for alcohol problems: Low Desisting (23%), High Desisting (14%), and Moderate Chronic (63%). Associations of these class memberships with class solutions found in the present study for the 30s were examined.
Alcohol use disorders
Past year AUD diagnoses were obtained from The Composite International Diagnostic Interview (World Health Organization, 1997) administered to the men at ages 35–36 years (N = 184). If the past year, DSM-IV criteria were met for either alcohol dependence or alcohol abuse; AUD was coded equal to 1 (vs. 0).
Analytic Design
Men's Alcohol Behaviors in the 30s
Trends for each of the alcohol indicators across the men's 30s and the statistical properties of the count outcomes were initially examined by fitting unconditional latent growth curve (LGC) models. First, the degree of over dispersion for the indicators was evaluated, denoting the extent to which the variance of the scores in the sample exceeded the average (e.g., for alcohol volume this might indicate small number of heavy drinkers relative to a large number of moderate-to-non-drinkers). The HED and alcohol problems indicators ranged from 0–3 and 0–7, respectively, neither of these indicators was significantly over dispersed at any of the assessments, and Poisson distributions were utilized. In contrast, the volume indicators were calculated as drinks per week in the last year (i.e., not capped) and significantly over dispersed at all assessments in the 30s (ν̂ =.31 to .58, p = .01 to < .001); thus, negative binomial distributions were utilized (Agresti, 2013). Second, zero-inflation in the alcohol indicators was considered to result from two distinct processes: zero values at each assessment versus both zero and non-zero values over time. LGC models revealed that, on average, significant zero-inflation existed in each of the alcohol indicators at men's ages 31–32 years (b = -9.79, p < .001 for volume; b = 1.27, p < .001 for HED; b = -1.74, p < .001 for problems), but linear rates of change in zero-inflation across the 30s were not significant (b = 0.04, p = .69 for volume; b = -0.01, p = .89 for HED; b = 0.04, p = .47 for problems). Next, heterogeneity in men's drinking behaviors across the 30s was examined using GMM with count outcomes. Zero-inflation was accounted for by defining one of the classes for each of the indicators to have only zero counts and no variance across time (Kreuter and Muthen, 2008; Muthen and Muthen, 1998-2012). This yielded classes of long-term alcohol abstainers, long-term no HED, and long-term no alcohol-related problems; whereas in all other classes, average levels and rates of change were freely estimated. Zero-inflation was specified as a separate class because it “has the advantage of allowing the estimation of the probability of being in each class and the posterior probabilities of being in each class for each individual (p. 196, Muthen and Muthen, 1998–2012).” Furthermore, the zero classes could also be defined to include long-term (rather than sporadic) non-use or no-alcohol-related problems across the men's 30s. These individual posterior probabilities of latent class assignments were then related to the covariates and distal outcomes (detailed below).
The number of classes necessary to summarize adequately the unobserved heterogeneity in the indicators was primarily assessed using the Lo-Mendell-Rubin Likelihood Ratio Test (LRT; Lo et al., 2001), which tests for improvement in overall model fit for a k versus (k + 1) model. Secondary criteria included maximizing entropy – which is a measure of the class assignment certainty – and minimizing information criteria (i.e., the Akaike Information Criterion [Akaike, 1987], Bayesian Information Criterion [BIC], and sample size adjusted BIC [Nylund et al., 2007]). Convergence, comparative fit, parsimony, class size, and the average class probabilities were also considered in model selection (Feldman et al., 2009).
Finally, stability in levels of men's drinking behaviors and related problems across the 30s was assessed by fitting and subsequently comparing change in overall model fit for two nested models: intercept-only GMMs, which assumed stability over time, and linear GMMs, which did not assume stability by allowing for change in the average levels of the alcohol indicators across the 30s. Stability was assessed using the Satorra-Bentler Scaled Chi-Square likelihood ratio difference test (SB χ2; Satorra and Bentler, 2011).
Relating men's alcohol classes in the 30s to contextual factors, AUDs, and prior use in the 20s
The best fitting GMMs were then used in a manual 3-step procedure that corrects for uncertainty in class assignments (Asparouhov and Muthén, 2013) to (i) predict 30s alcohol classes from peer and partner alcohol use (both in univariate and multivariate models) and (ii) predict men's AUD diagnoses in their late 30s from their 30s alcohol classes. For each of the three alcohol indicators, χ2 analyses were used to assess congruence between men's most likely class memberships in their 20s and their most likely class memberships in their 30s. Given prior publication of the 20s classes, this was considered the most appropriate approach. To test hypotheses regarding whether the subset of men who showed desisting trends in alcohol volume, HED, and problems across their 20s had showed continued desistance, as indexed by membership in no or lower use classes in the 30s, one sample binomial tests of proportions were conducted for men in each of the following 20s alcohol classes – High Desisting volume, Moderate Desisting HED, High Desisting problems. In each case, the null hypothesis was that the probability of being in the no or lower use/problems class versus the higher class in the 30s would be equal to chance (i.e., .50).
Results
Alcohol Use Classes in the 30s
Both intercept-only and linear GMMs of varying class sizes were fit to the data and class enumeration criteria were evaluated (see Table 1, not all model results shown). For each of the three alcohol indicators, the Lo-Mendell-Rubin LRTs indicated that 3-class GMM solutions most adequately summarized the variance in men's drinking behaviors. Regarding estimated class sizes, in each of the 4-class solutions for alcohol volume and alcohol problems, a class comprised less than 7% of the sample and the 4‐class solution for HED showed a problematic fit, assigning no men to one of the classes. Although entropy was maximized in the 2-class solutions for alcohol volume and alcohol problems, this was to be expected and not substantively interesting – considering that each solution included a long-term alcohol no use/problems class – thus indicating, for example, that there is near certainty in discriminating among men who never used alcohol in their 30s from those who did. Interestingly, however, much less certainty was observed for HED class assignments, even when considering only a long-term No HED class and an HED user class. In sum, 3-class GMM solutions were chosen for all three alcohol indicators.
Table 1. Fit Comparisons for all Models.
| Outcome Measure: (Model Type) | Number of Classes† | AIC | BIC | Sample-Size Adjusted BIC | Entropy | N | Lo-Mendell-Rubin Adjusted LRT Test, p-value |
|---|---|---|---|---|---|---|---|
| Volume: (linear negative binomial model) | |||||||
| 1 | 5162.21 | 5201.61 | 5163.59 | na | 197 | na | |
| 2 | 5112.58 | 5148.69 | 5113.85 | .97 | 13/184 | -0.18, p= .0001 | |
| 3 | 5106.02 | 5151.98 | 5107.63 | .78 | 90/13/94 | 3.301, p= .040 | |
| 4 | 5098.80 | 5154.61 | 5100.75 | .88 | 160/13/12/12 | 0.270, p= .073 | |
| Heavy Episodic Drinking: (linear Poisson model) | |||||||
| 1 | 1450.19 | 1473.17 | 1451.00 | na | 197 | na | |
| 2 | 1439.47 | 1459.17 | 1440.16 | .65 | 97/100 | 1.35, p= .001 | |
| 3 | 1435.48 | 1465.03 | 1436.51 | .66 | 67/97/33 | 1.20, p= .002 | |
| 4 | 1438.63 | 1478.02 | 1440.01 | .51 | 48/0/121/28 | 2.58, p= .335 | |
| Problems: (intercept Poisson model) | |||||||
| 1 | 2852.87 | 2869.29 | 2853.45 | na | 197 | na | |
| 2 | 2949.90 | 2959.75 | 2950.25 | .94 | 26/171 | 0.17, p< .001 | |
| 3 | 2914.61 | 2931.02 | 2915.18 | .82 | 42/26/129 | 1.36, p< .001 | |
| 4 | 2917.79 | 2940.78 | 2918.60 | .83 | 49/26/119/3 | 1.38, p= .529 |
Note:
All GMMs fit with two or more classes were estimated such that one of the classes was defined as a long-term alcohol abstainer/No HED class or a long-term no-alcohol-related-problems class. Single-class solutions were estimated using zero-inflated negative binominal distributions for alcohol volume and zero-inflated Poisson distributions for HED and problems. AIC: Akaike Information Criterion, BIC: Bayesian Information Criterion, Lo-Mendell-Rubin (Lo et al., 2001) Adjusted Likelihood Ratio Test denotes change in overall model fit for a (k) versus (k+1) class model (e.g., 1- vs. 2-class model).
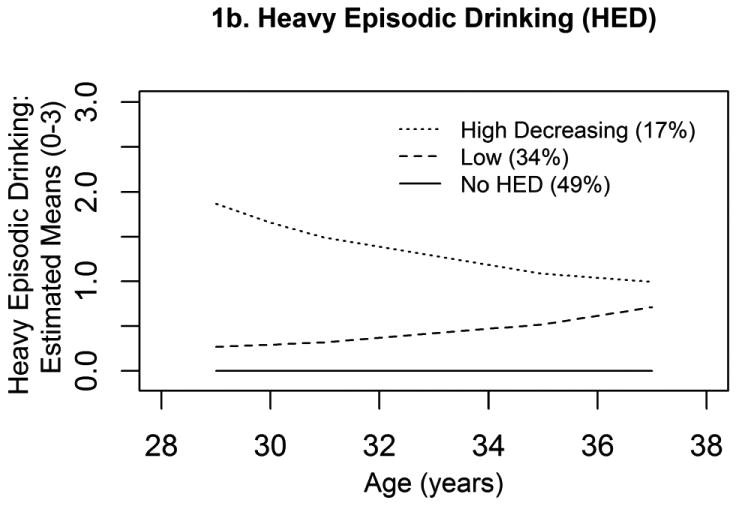
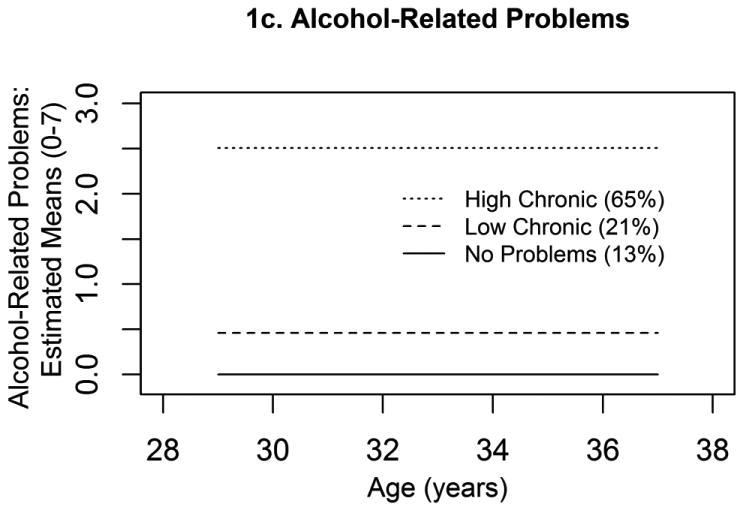
The extent to which men's alcohol use behaviors and alcohol-related problems were established across the 30s was examined by comparing 3-class intercept-only GMMs to 3-class linear GMMs. On average, men's alcohol-related problems were found to be established across their 30s, as indexed by nonsignificant improvement in overall model fit for the linear model over the intercept-only model (SB χ2(4) = 5.13, p = .274), whereas the addition of linear slope terms improved overall model fit for alcohol volume (SB χ2(4) = 79.90, p < .001) and HED (SB χ2(4) = 34.90, p < .001), indicating significant change across the 30s. These 3-class solutions are depicted in Figure 1: (i) for alcohol volume (1a), Abstainers (7%), High Increasing volume (48%; β̂ slope = 0.09, p = .001) and Low Decreasing volume (45%; β̂ slope = -0.09, p = .001); (ii) for HED (1b), No HED (49%), High Decreasing HED (17%; β̂ slope = -0.14, p = .001), and Low HED (34%; β̂ slope = 0.06, p = .101); and (iii) for alcohol problems (1c), No Problems (13%), High Chronic problems (65%), and Low Chronic problems (21%). Class sizes indicated that few men abstained from alcohol use or had no alcohol-related problems across their 30s; whereas, nearly one-half of the men showed no HED. For alcohol volume and problems, almost one-half of the men and over two-thirds of the men were assigned to the higher of the two user classes, respectively. In contrast, more men were assigned to the low HED versus High Decreasing HED class.
Figure 1. GMM 3-Class Solutions in 30s.
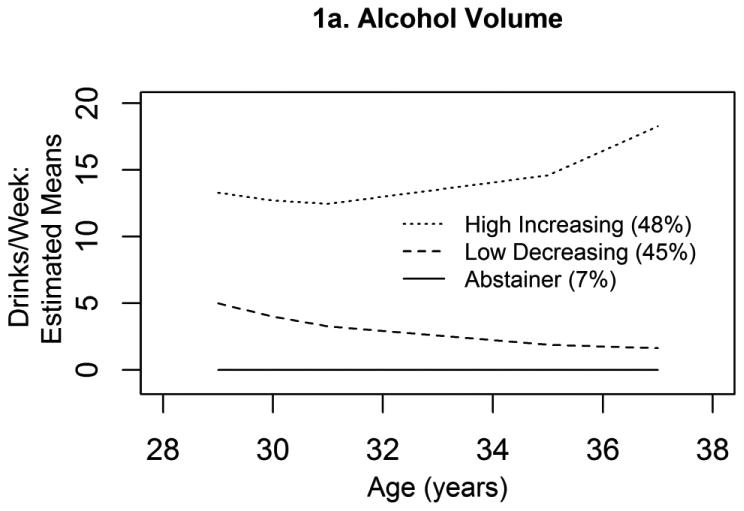
1a. Alcohol Volume
1b. Heavy Episodic Drinking (HED)
1c. Alcohol-Related Problems
Overall, findings were consistent with the hypothesis that men's patterns of alcohol use behaviors in the 30s would be more established than at earlier ages, with relatively flat persisting patterns (e.g., no class trajectories crossed over); however, significant changes in men's alcohol volume and HED patterns across the 30s were observed. Regarding HED, as predicted, there was no significantly increasing HED class in the 30s. The high class showed a significant decrease in HED across the period. In contrast, mixture analyses for alcohol volume yielded both an increasing and decreasing use class.
Prediction of Differential Alcohol Use from Peer and Partner Use
For each of the three indicators, prediction from peer and partner alcohol use – which were significantly associated (r = .28, p < .001) – was first examined in separate univariate prediction models and subsequently in multivariate models that included both predictors (Table 2). Univariate results revealed that both peer and partner use discriminated among men in the highest versus no alcohol use or HED and problems classes for all three indicators. However, only peer use was able to distinguish between men with relatively low alcohol use from those who had not used, but this was only true for HED (not for alcohol volume or alcohol-related problems). Likewise, only peer use discerned among men in the higher versus lower alcohol volume and alcohol-related problems classes; in contrast, neither predictor was related to men's assignments to the higher versus lower HED classes. Last and most importantly, multivariate results revealed that all of the effects on men's alcohol class assignments attributable to partner use were attenuated by peer use; whereas the patterns of significance for peer use remained unchanged across the univariate and multivariate models.
Table 2. Odds Ratios for Alcohol Class Predictions from Peer and Partner Alcohol Use.
| Model | Predictor Variable | N | Odds Ratio (High vs. Zero Class) |
Odds Ratio (Low vs. Zero Class) |
Odds Ratio (High vs. Low Class) |
|---|---|---|---|---|---|
| Alcohol Volume | |||||
| Univariate | Partner heavy drinking | 184 | 11.99* | 1.71 | 7.03M |
| Peer drunkenness | 197 | 7.33** | 1.41 | 5.21*** | |
| Multivariate | |||||
| Partner heavy drinking | 184 | 4.64M | 4.92M | 0.94 | |
| Peer drunkenness | 4.78* | 1.04 | 4.58*** | ||
| Heavy Episodic Drinking | |||||
| Univariate | Partner heavy drinking | 184 | 2.47* | 2.14M | 1.15 |
| Peer drunkenness | 197 | 5.22*** | 3.62*** | 1.44 | |
| Multivariate | |||||
| Partner heavy drinking | 184 | 1.57M | 1.26 | 1.25 | |
| Peer drunkenness | 5.10*** | 3.13*** | 1.63 | ||
| Alcohol Problems | |||||
| Univariate | Partner heavy drinking | 184 | 3.75* | 2.52 | 1.49 |
| Peer drunkenness | 197 | 15.15** | 2.85 | 5.31*** | |
| Multivariate | |||||
| Partner heavy drinking | 184 | 1.81 | 1.53 | 1.19 | |
| Peer drunkenness | 15.34** | 3.23 | 4.74*** |
Note: “High/Low/Zero” Class labels denote “High increasing volume/Low decreasing volume/Alcohol abstainer” for Alcohol Volume; “High decreasing HED/Low HED/No HED” for Heavy Episodic Drinking; and “High chronic/Low chronic/No problems” for Alcohol Problems.
p <.001.
p <.01.
p <.05.
p <.10.
Comparison of Class Memberships across Alcohol Indicators
Table 3 shows the cell sizes by classes cross-tabulated over the three alcohol indicators. The most frequent combination was of men with High Increasing volume and High Chronic problems but in the Low HED class (n = 44, 22.3%); whereas fewer men (n = 26, 13.2%) were likely to be in the highest classes for all three indicators. The other two most frequent combinations were of men with Low Decreasing volume, No HED, and either High Chronic problems (n = 27, 13.7%) or Low Chronic problems (n = 28, 14.2%). Whereas relatively few men were in the highest classes for all three alcohol indicators, 45% of men were in the highest classes on at least two indicators. Overall, the comparisons across GMM class memberships for the three indicators of alcohol use indicated moderate concordance.
Table 3. Associations among 30s Alcohol Class Assignments.
| 30s Problems Class | |||||
|---|---|---|---|---|---|
|
|
|||||
| 30s Volume Class | 30s HED Class | No Problems | Low Chronic Problems | High Chronic Problems | Subtotal |
| Abstainer | No HED | 13 | 0 | 0 | 13 |
| Low HED | 0 | 0 | 0 | 0 | |
| High Decreasing HED | 0 | 0 | 0 | 0 | |
|
| |||||
| Subtotal | 13 | 0 | 0 | 13 | |
|
| |||||
| Low Decreasing Volume | No HED | 10 | 28 | 27 | 65 |
| Low HED | 0 | 5 | 13 | 18 | |
| High Decreasing HED | 0 | 0 | 7 | 7 | |
|
| |||||
| Subtotal | 10 | 33 | 47 | 90 | |
|
| |||||
| High Increasing Volume | No HED | 1 | 6 | 12 | 19 |
| Low HED | 2 | 3 | 44 | 49 | |
| High Decreasing HED | 0 | 0 | 26 | 26 | |
|
| |||||
| Subtotal | 3 | 9 | 82 | 94 | |
Note: Tabled numbers denote count (n).
Comparison of class memberships in the 20s and the 30s
Omnibus χ2 tests indicated that each of the 2-way comparisons for alcohol class memberships in the 20s versus 30s was significant (Table 4, Panels I, II, and III): volume by volume, χ2 (4) = 40.93, p < .001; HED by HED, χ2 (4) = 53.39, p < .001; and problems by problems, χ2 (4) = 88.07, p < .001. No men who were in the High Chronic volume class in their 20s abstained from alcohol use in their 30s. Of the men in the Low Moderate and High Desisting volume classes in their 20s, over two-thirds from each class were in the abstaining or Low Decreasing classes in their 30s. Thus, most of the men in the High Desisting class in their 20s maintained low or no volume of use in their 30s.
Table 4. Class Membership Comparisons 20s and 30s.
| 20s Volume Class | ||||
|---|---|---|---|---|
|
|
||||
| 30s Volume Class | Low Moderate | High Desisting | High Chronic | Total |
| Abstainer | 9 | 4 | 0 | 13 |
| % within 30s Abstainer class | 69.2% | 30.8% | 0% | 100% |
| % within 20s Volume class | 27.3% | 12.9% | 0% | 6.6% |
| Low Decreasing | 15 | 18 | 57 | 90 |
| % within 30s Low Decreasing class | 16.7% | 20.0% | 63.3% | 100% |
| % within 20s Volume class | 45.5% | 58.1% | 42.9% | 45.7% |
| High Increasing | 9 | 9 | 76 | 94 |
| % within 30s High Increasing class | 9.6% | 9.6% | 80.9% | 100% |
| % within 20s Volume class | 27.3% | 29.0% | 57.1% | 47.7% |
|
| ||||
| Total | 33 | 31 | 133 | 197 |
| % within 30s Volume class | 16.8% | 15.7% | 67.5% | 100% |
| % within 20s Volume class | 100% | 100% | 100% | 100% |
| 20s HED Class | ||||
|
|
||||
| 30s HED Class | Low Desisting | Moderate Desisting | Moderate Increasing | Total |
|
| ||||
| No HED | 83 | 12 | 2 | 97 |
| % within 30s No HED class | 85.6% | 12.4% | 2.1% | 100% |
| % within 20s HED class | 61.5% | 32.4% | 8.0% | 49.2% |
| Low | 43 | 16 | 8 | 67 |
| % within 30s Low HED class | 64.2% | 23.9% | 11.9% | 100% |
| % within 20s HED class | 31.9% | 43.2% | 32.0% | 34.0% |
| High Decreasing | 9 | 9 | 15 | 33 |
| % within 30s High Decreasing HED class | 27.3% | 27.3% | 45.5% | 100% |
| % within 20s HED class | 6.7% | 24.3% | 60.0% | 16.8% |
|
| ||||
| Total | 135 | 37 | 25 | 197 |
| % within 30s HED class | 68.5% | 18.8% | 12.7% | 100% |
| % within 20s HED class | 100% | 100% | 100% | 100% |
| 20s Problems Class | ||||
|
|
||||
| 30s Problems Class | Low Desisting | High Desisting | Moderate Chronic | Total |
|
| ||||
| No Problems | 18 | 6 | 2 | 26 |
| % within 30s No Problems class | 69.2% | 23.1% | 7.7% | 100% |
| % within 20s Problems class | 38.3% | 21.4% | 1.6% | 13.2% |
| Low Chronic | 22 | 8 | 12 | 42 |
| % within 30s Low Chronic Problems class | 52.4% | 19.0% | 28.6% | 100% |
| % within 20s Problems class | 46.8% | 28.6% | 9.8% | 21.3% |
| High Chronic | 7 | 14 | 108 | 129 |
| % within 30s High Chronic Problems class | 5.4% | 10.9% | 83.7% | 100% |
| % within 20s Problems class | 14.9% | 50.0% | 88.5% | 65.5% |
|
| ||||
| Total | 47 | 28 | 122 | 197 |
| % within 30s Problems class | 23.9% | 14.2% | 61.9% | 100% |
| % within 20s Problems class | 100% | 100% | 100% | 100% |
Note: Tabled numbers denote count (n) unless noted otherwise.
For HED, the majority of men who had shown increases in HED across their 20s continued to engage in HED in their 30s – although showing a downward trend across that latter period. Most men in the Moderate Desisting HED class in their 20s continued this trend in their 30s. Of the men who were in the Low Desisting HED class in their 20s, most showed no HED in their 30s.
Finally, regarding alcohol problems, most men in the Moderate Chronic class in their 20s were in the High Chronic Problems class in their 30s. Of the men in the High Desisting Class in their 20s, one-half were in the high problems class in the 30s. Overall for the three indicators, most men in the higher classes in their 30s had also been in the higher classes in their 20s, with relatively few men moving from a lower class in their 20s into a high class in their 30s.
To test hypotheses regarding whether men in classes that had shown strong desisting patterns during their 20s for alcohol volume, HED, and alcohol-related problems (Capaldi et al., 2013) showed continued desistance, as indexed by membership in no or low use or problems classes in the 30s, one sample binomial tests of proportions were conducted for men in each of the following 20s alcohol classes – High Desisting volume, Moderate Desisting HED, and High Desisting problems. In each case, the null hypothesis was that the probability of being in the no or low use or problems class in the 30s would be .50. For alcohol volume, 71% (22 of 31) of the men in the High Desisting class were classified in the Abstainer or Low Decreasing volume class in their 30s; thus showing significant sustained desistance (p = .029). For HED, 76% (28 of 37) of the men in the Moderate Desisting class in the 20s were classified in the No HED or Low HED class in their 30s (p = .003); thus significantly maintaining their HED desistance. Finally, for alcohol problems, 50% (14 of 28) of the men in the High Desisting problems class in the 20s were classified in the No or Low Chronic problems class in their 30s (p = 1.00); thus not maintaining problem desistance.
Association of 30s Class Membership to AUD Diagnoses
At ages 35–36 years, only n = 17 of 184 men (9.2%) reported past year alcohol use symptoms that met criteria for a positive AUD diagnosis (050% of men met criteria for a positive lifetime AUD diagnosis). Cross-tabulations of men's most likely estimated class memberships and AUD diagnoses are given in Table 5. Significantly greater odds for AUD diagnoses were associated with the higher 30s alcohol volume and problems class memberships, but not the 30s HED class memberships. All 17 men who were diagnosed with an AUD were assigned to the High Decreasing Alcohol volume class (n = 17 of 94, 18.1%), thus resulting in infinitely large ORs when comparing the High Decreasing Volume Class to the Abstainer and Low Volume classes. Likewise, of the 120 men in the High Chronic Problems class, n = 16 (13.3%) were diagnosed with an AUD versus no men in the No Problems class and 1 man in the Low Chronic Problems class. However, men were not significantly more likely to be diagnosed with an AUD if they were in the High Decreasing HED class (5 of 29, 17.2%) versus the Low HED class (9 of 63, 14.3%; OR = 1.33, p = .197), nor versus the No HED class (3 or 92, 3.2%; OR = 28.57, p = .775). Similarly, men in the Low HED class were no more likely than men in the No HED class to be diagnosed with an AUD (OR = 21.37, p = .788). Thus, even though relatively few men were diagnosed with a past year AUD at ages 35–36 years, the probability of being diagnosed significantly increased if men were in the Higher (vs. No or Lower) Alcohol Volume and Alcohol Problems classes in their 30s.
Table 5.
Associations of Men's Past Year AUD Diagnosis at Ages 35–36 years with 30s Class Memberships
| AUD Diagnosis | |||
|---|---|---|---|
|
|
|||
| 30s Volume Class | No | Yes | Total |
| Abstainer | 13 | 0 | 13 |
| Low Decreasing | 85 | 0 | 85 |
| High Increasing | 69 | 17 | 86 |
|
| |||
| Total | 167 | 17 | 184 |
| AUD Diagnosis | |||
|
|
|||
| 30s HED Class | No | Yes | Total |
|
| |||
| No HED | 89 | 3 | 92 |
| Low | 54 | 9 | 63 |
| High Decreasing | 24 | 5 | 29 |
|
| |||
| Total | 167 | 17 | 184 |
| AUD Diagnosis | |||
|
|
|||
| 30s Problems Class | No | Yes | Total |
|
| |||
| No Problems | 23 | 0 | 23 |
| Low Chronic | 40 | 1 | 41 |
| High Chronic | 104 | 16 | 120 |
|
| |||
| Total | 167 | 17 | 184 |
Note: Tabled numbers denote count (n).
Discussion
Predictors of heterogeneity in alcohol use trajectories extracted from data on volume, HED, and alcohol problems were examined from ages 29–30 through 37–38 years in a predominantly working-class sample of men. Although relatively few of the men met criteria for an AUD in the past year at ages 35–36 years, such a diagnosis was significantly associated with being in both the High Increasing Alcohol Volume and High Chronic Alcohol Problems classes. The prediction that patterns in men's alcohol problems would be more entrenched in the 30s than in the 20s was supported because no significant growth was found for the alcohol problems classes. Furthermore, a substantial number of men showed relatively high alcohol problems, with the High Chronic Problems class comprising 65% of the sample and reporting an average of 2.5 alcohol problems.
On the other hand, patterns in men's alcohol volume and HED across the 30s were not found to be established. Interestingly, although the highest volume and alcohol problems classes did not show any significant desistance across this period (in fact the highest volume class showed a significant increase), the high HED class (a relatively small proportion of the men) did show decreasing HED across the period. Many men in their 30s consumed large quantities of alcohol without frequent engagement in HED, and the high increasing volume likely related to problem symptoms (as the latter did not decrease). This hypothesis was supported by the comparisons of class memberships of alcohol trajectories in the 30s among the three alcohol indicators.
Further, interesting issues emerged in comparing class memberships for the 30s with classes for the same three indicators that had been modeled from ages 18–19 through 28–29 years in a prior study (Capaldi et al., 2013). Significant associations for each of the three indicators indicated considerable continuity in men's relative levels of alcohol use from the 20s to the 30s; in particular, few men who were in a lower use class in their 20s moved to a high class in their 30s. Thus, few men were moving in a problematic direction in their 30s relative to other men in the sample. This suggests that preventive efforts need to be introduced at young ages, including during late childhood and in early adolescence. It should be cautioned that differences in the modeling involving continuous (20s) versus count (30s) data preclude drawing conclusions regarding absolute levels of use rather than use relative to other men.
A key issue regarding treatment or secondary prevention is whether men showing desistance in alcohol use in their 20s sustained their lower use in their 30s. Findings indicated this was the case for alcohol volume and for HED but not for alcohol problems. The longer-term maintenance of desistance trends for alcohol volume and HED are encouraging, and programs influential in encouraging such desistance in the 20s may have long-term benefits.
Regarding direct social influence from peer and partner drinking, peer drunkenness was predictive of membership in the higher classes for all three alcohol indicators, controlling for partner heavy drinking. Thus, even when most of the men have substantial family responsibilities, peer heavy use was strongly related to the men's alcohol use. The men may be drinking with friends after work or in other social situations. Interestingly, partner heavy drinking was only significantly predictive of a higher volume of alcohol use, HED, and alcohol-related problems (compared with abstention or no HED or no problems) when peer use was not considered in the models. Thus outcome-specific (i.e., alcohol use) social influences, especially from peers, remain important factors affecting men's alcohol use in the 30s. The findings for peer and partner influence should be viewed in light of the fact that the measures of alcohol use differed for peers and for partners. Perhaps if partner drunkenness rather than heavy drinking had been assessed, the partner variable might have shown a stronger association. Further, partner drinking was assessed by partner report and peer drunkenness by the OYS men's reports. However, issues of peer and partner influence also differ naturally since men usually only have one partner (at a time) but a number of friends or peers. The findings do indicate that the closeness of men's alcohol use to that of their peers, which begins in late childhood or early adolescence (Dishion et al., 1996) and continues through adolescence (Hawkins et al., 1992) and the 20s (Andrews et al., 2002), also extends through the 30s. Thus, interventions that influence the social contexts of drinking, particularly drinking with friends, may be expected to be beneficial across developmental stages.
This study had some limitations. The size of the sample was relatively small, reducing power to detect associations of risk factors with class membership. There were differences in the GMM modeling approaches taken in the prior study of heterogeneity of alcohol use in the 20s (Capaldi et al., 2013) and the current study of the 30s, notably due to use of continuous measures modeled in the 20s versus count data with a predefined zero class in the 30s. This change was due both to lower levels of use in the 30s than the 20s and to advances in understanding of the most appropriate applications of GMM (Feldman et al., 2009; Masyn et al., 2014). Note also that the use of GMM comes with recognition that class solutions are not ‘found’ subpopulations but appropriate explanations of heterogeneity given the OYS data and sample. In addition, because the sample was composed of predominantly lower socioeconomic status White men, generalizability of our findings to women, other ethnic groups, and men of higher socioeconomic status warrants further study.
Findings from the present study addressed the unobserved heterogeneity in alcohol trajectories in early midadulthood and on predictors of classes extracted from the different forms of alcohol use. They provide some encouragement regarding maintenance of desistence for some men, but cautionary notes regarding the relatively large proportions of men who showed relatively high levels of alcohol volume and chronic alcohol problems. Men in such classes may have higher mental and physical health problems or impaired functioning in later adulthood.
Acknowledgments
The project described was supported by awards from National Institutes of Health (NIH), U.S. PHS to Dr. Capaldi: Award Number 1R01AA018669 (Understanding Alcohol Use over Time in Early Mid-Adulthood for At-Risk Men) from the National Institute on Alcohol Abuse and Alcoholism (NIAAA); HD 46364 (Risk for Dysfunctional Relationships in Young Adults) from the National Institute of Child Health and Development (NICHD); and R01 DA 015485 (Adjustment Problems and Substance Use in Three Generations) from the National Institute of Drug Abuse (NIDA). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH, NIAAA, NICHD, or NIDA. We thank Jane Wilson and the Oregon Youth Study team for high-quality data collection, and Sally Schwader for editorial assistance with this manuscript.
References
- Agresti A. Categorical Data Analysis. 3rd ed. Wiley; Hoboken, NJ: 2013. [Google Scholar]
- Akaike H. Factor analysis and AIC. Psychometrika. 1987;52:317–332. [Google Scholar]
- Andrews JA, Tildesley E, Hops H, Li F. The influence of peers on young adult substance use. Health Psychol. 2002;21:349–357. doi: 10.1037//0278-6133.21.4.349. [DOI] [PubMed] [Google Scholar]
- Asparouhov T, Muthen BO. Auxiliary variables in mixture modeling: A 3-step approach using Mplus. 2013 (Mplus Web Notes: No. 15, Version 6). Retrieved from http://statmodel.com/examples/webnotes/AuxMixture_submitted_corrected_webnote.
- Capaldi DM, Feingold A, Kim HK, Yoerger K, Washburn IJ. Heterogeneity in growth and desistance of alcohol use for men in their 20s: Prediction from early risk factors and association with treatment. Alcohol Clin Exp Res. 2013;37(Suppl s1):E347–E355. doi: 10.1111/j.1530-0277.2012.01876.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Capaldi DM, Patterson GR. An approach to the problem of recruitment and retention rates for longitudinal research. Behav Assess. 1987;9:169–177. [Google Scholar]
- D'Amico E, Ellickson PL, Collins RL, Martino S, Klein DJ. Processes linking adolescent problems to substance-use problems in late young adulthood. J Stud Alcohol. 2005;66:766–775. doi: 10.15288/jsa.2005.66.766. [DOI] [PubMed] [Google Scholar]
- Dishion TJ, Spracklen KM, Andrews DW, Patterson GR. Deviancy training in male adolescent friendships. Behav Ther. 1996;27:373–390. [Google Scholar]
- Feldman BJ, Masyn KE, Conger RD. New approaches to studying problem behaviors: A comparison of methods for modeling longitudinal, categorical adolescent drinking data. Dev Psychol. 2009;45:652–676. doi: 10.1037/a0014851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fleming CB, White HR, Catalano RF. Romantic relationships and substance use in early adulthood: An examination of the influences of relationship type, partner substance use, and relationship quality. J Health Soc Behav. 2010;51:153–167. doi: 10.1177/0022146510368930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grant BF, Dawson DA, Stinson FS, Chou P, Dufour MC, Pickering RP. The 12-month prevalence and trends in DSM–IV alcohol abuse and dependence: United States, 1991–1992 and 2001–2002. Drug Alcohol Depend. 2004;74:223–234. doi: 10.1016/j.drugalcdep.2004.02.004. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychol Bull. 1992;112:64–105. doi: 10.1037/0033-2909.112.1.64. [DOI] [PubMed] [Google Scholar]
- Helson R, Soto CJ. Up and down in middle age: Monotonic and nonmonotonic changes in roles, status, and personality. J Pers Soc Psychol. 2005;89:194–204. doi: 10.1037/0022-3514.89.2.194. [DOI] [PubMed] [Google Scholar]
- Jacob T, Bucholz KK, Sartor CE, Howell DN, Wood PK. Drinking trajectories from adolescence to the mid-forties among alcohol dependent males. J Stud Alcohol. 2005;66:745–755. doi: 10.15288/jsa.2005.66.745. [DOI] [PubMed] [Google Scholar]
- Kreuter F, Muthén BO. Analyzing criminal trajectory profiles: Bridging multilevel and group-based approaches using growth mixture modeling. J Quant Criminol. 2008;24:1–31. [Google Scholar]
- Leonard KE, Mudar P. Peer and partner drinking and the transition to marriage: A longitudinal examination of selection and influence processes. Psychol Add Behav. 2003;17:115–125. doi: 10.1037/0893-164x.17.2.115. [DOI] [PubMed] [Google Scholar]
- Lo Y, Mendell NR, Rubin DB. Testing the number of components in a normal mixture. Biometrika. 2001;88:767–778. [Google Scholar]
- Masyn KE, Petras H, Liu W. Growth curve models with categorical outcomes. In: Bruinsma G, Weisburd D, editors. Encyclopedia of Criminology and Criminal Justice. Springer; New York, NY: 2014. pp. 2013–2025. [Google Scholar]
- Mushquash AR, Stewart SH, Sherry SB, Mackinnon SP, Antony MM, Sherry DL. Heavy episodic drinking among dating partners: A longitudinal actor–partner interdependence model. Psychol Add Behav. 2013;27:178–183. doi: 10.1037/a0026653. [DOI] [PubMed] [Google Scholar]
- Muthén BO, Muthén LK. The development of heavy drinking and alcohol-related problems from ages 18 to 37 in a U. S. national sample. J Stud Alcohol. 2000;61:290–300. doi: 10.15288/jsa.2000.61.290. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus User's Guide. 7th ed. Muthén & Muthén; Los Angeles, CA: 1998–2012. [Google Scholar]
- Muthén BO, Shedden K. Finite mixture modeling with mixture outcomes using the EM algorithm. Biometrics. 1999;55:463–469. doi: 10.1111/j.0006-341x.1999.00463.x. [DOI] [PubMed] [Google Scholar]
- Nylund KL, Asparouhov T, Muthén BO. Deciding on the number of classes in latent class analysis and growth mixture modeling. A Monte Carlo simulation study. Struct Equ Modeling. 2007;14:535–569. [Google Scholar]
- Oslin DW, Slaymaker VJ, Blow FC, Owen PL, Colleran C. Treatment outcomes for alcohol dependence among middle-aged and older adults. Addict Behav. 2005:1431–1436. doi: 10.1016/j.addbeh.2005.01.007. [DOI] [PubMed] [Google Scholar]
- Satorra A, Bentler P. University of California Los Angeles: Department of Statistics; 2011. Scaling corrections for statistics in covariance structure analysis. Retrieved from: http://escholarship.org/uc/item/8dv7p2hr. [Google Scholar]
- Sher KJ, Jackson KM, Steinley D. Alcohol use trajectories and the ubiquitous cat's cradle: Cause for concern? J Abnorm Psychol. 2011;120:322–335. doi: 10.1037/a0021813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stone AL, Becker LG, Huber AM, Catalano RF. Review of risk and protective factors of substance use and problem use in emerging adulthood. Addict Behav. 2012;37:747–775. doi: 10.1016/j.addbeh.2012.02.014. [DOI] [PubMed] [Google Scholar]
- Toumbourou JW, Williams IR, Snow PC, White VM. Adolescent alcohol trajectories in the transition from high school. Drug Alcohol Rev. 2003;22:111–116. doi: 10.1080/09595230100100534. [DOI] [PubMed] [Google Scholar]
- Tucker JS, Orlando M, Ellickson PL. Patterns and correlates of binge drinking trajectories from adolescence to young adulthood. Health Psychol. 2003;22:79–87. doi: 10.1037//0278-6133.22.1.79. [DOI] [PubMed] [Google Scholar]
- Washburn IJ, Capaldi DM, Kim HK, Feingold A. Alcohol and marijuana use in early adulthood for at-risk men: Time-varying associations with peer and partner substance use. Drug Alcohol Depend. 2014 doi: 10.1016/j.drugalcdep.2014.04.001. on line first. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiesner M, Capaldi DM, Kim HK. Arrest trajectories across a 17-year span for young men: Relation to dual taxonomies and self-reported offense trajectories. Criminology. 2007;45:835–863. doi: 10.1111/j.1745-9125.2007.00099.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. Composite International Diagnostic Interview (CIDI). Core Version 2.1. World Health Organization; Geneva, Switzerland: 1997. [Google Scholar]
- Zucker RA, Fitzgerald HE, Moses HD. Emergence of alcohol problems and the several alcoholisms: A developmental perspective on etiologic theory and life course trajectory. In: Cicchetti D, Cohen DJ, editors. Developmental Psychopathology: Risk, Disorder, and Adaptation. Vol. 2. Wiley; New York, NY: 1995. pp. 677–711. [Google Scholar]