

Editor
Mediastinal bronchial artery aneurysms are uncommon, with fewer than 40 published case reports (1,2). Presentation is varied, ranging from an incidental imaging finding to hemomediastinum and shock resulting from aneurysm rupture. Rupture can occur with a bronchial artery aneurysm of any size, so prompt treatment is indicated upon diagnosis. Current treatment options include surgical resection, transarterial embolization, and stent-grafting with subsequent percutaneous embolization of feeding vessels. We report a case of an asymptomatic 53-year-old man in whom a mediastinal bronchial artery aneurysm was incidentally discovered on computed tomography (CT) of the chest. The aneurysm and its branches were successfully coil-embolized via a transarterial approach. The case description is as follows.
A 53-year-old man underwent a screening CT examination of the chest in the context of a testicular mass that was ultimately deemed benign. The CT scan revealed a 12-mm-diameter aneurysm arising from a 1–2-mm neck from the aorta (Figure, a–c). A short bronchial artery trunk emanated from the superior aspect of the aneurysm sac before bifurcating into left and right bronchial arteries. The patient was asymptomatic with no history of pulmonary infection or trauma or CT evidence of atherosclerosis. Of note, the patient’s medical history was significant for non-Hodgkin lymphoma, which had been successfully treated with stem cell transplantation 10 years earlier. He received no radiation therapy.
Figure.
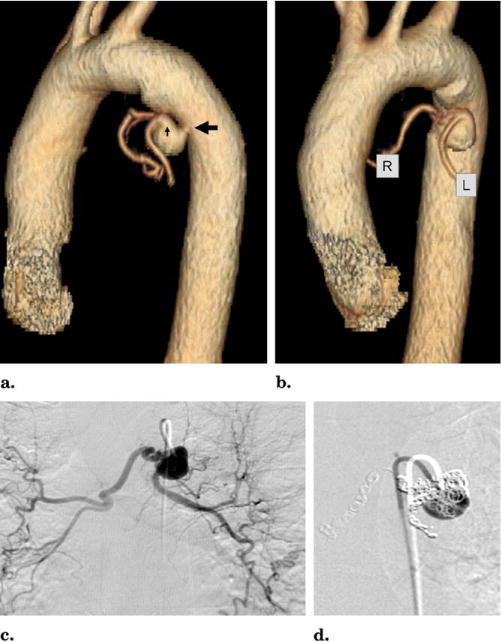
(a)Three-dimensionally reformatted CT image shows short aneurysm neck (large black arrow) and short bronchial artery trunk (small black arrow). (b) Three-dimensionally reformatted CT image shows right (R) and left (L) bronchial artery branches arising from the aneurysm sac. (c) Anteroposterior projection angiogram with catheter in bronchial artery aneurysm. (d) Coil embolization of both bronchial artery branches and aneurysm sac. (Available in color online at www.jvir.org.)
After written informed consent was obtained, the patient underwent treatment of the bronchial artery aneurysm by coil embolization. A bronchial artery angiogram was obtained from a right common femoral artery punctured with an 18-gauge, 7-cm needle (Cook, Bloomington, Indiana). A 6-F vascular sheath (Terumo, Tokyo, Japan) was inserted into the artery over a Bentsen guide wire (Cook). A 5-F Sos catheter (Angiodynamics, Queensbury, New York) was used to select the bronchial artery and an angiogram was obtained with use of Omnipaque contrast medium (Amer-sham, Princeton, New Jersey; Figure). A bronchial artery aneurysm arising from the trunk was identified. The spinal artery did not arise from the bronchial artery or its branches. A 2.6-F Turbo Tracker microcatheter (Boston Scientific, Natick, Massachusetts) was advanced through the Sos catheter into the left bronchial artery. Coil embolization was carefully performed with a combination of 3- and 4-mm Nester and Tornado coils (Cook) until the artery distal to the coils was occluded (Figure). Next, the right bronchial artery was selected and coil embolization was performed in a similar fashion. Branches were coil-embolized in a similar fashion. Finally, coils were placed across into the aneurysm sac itself. After the last coil was placed, repeat angiography demonstrated cessation of flow within the bronchial arterial branches with only a minimal amount of contrast medium opacification of the aneurysm sac. The sheath was removed and hemostasis was obtained. The patient was admitted overnight for observation and discharged the next day.
The patient returned 3 months after the embolization for a follow-up evaluation. A CT angiogram of the thorax was obtained, which demonstrated that the aneurysm remained thrombosed.
Three months after the embolization, the patient returned for a follow-up evaluation. Transesophageal echocardiography was performed, demonstrating complete thrombosis of the aneurysm sac. The thrombosed aneurysm was unchanged in size.
Bronchial artery aneurysms are divided based on their anatomic location as mediastinal or intrapulmonary (3). In general, bronchial artery aneurysms are uncommon, with a reported incidence of less than 1% based on selective bronchial angiograms (1). The subset of bronchial artery aneurysms occurring within the mediastinum are even more uncommon, as there are fewer than 40 published case reports (1,2).
Myriad predisposing conditions have been described in the setting of bronchial artery aneurysm, including bronchiectasis, atherosclerosis trauma, radiation therapy, mycotic infection, and Osler–Weber–Rendu syndrome. Interestingly, in approximately one quarter of described cases, no predisposing etiology could be identified (1,3). One author (3) has hypothesized that these etiologies result in a common pathway of increased blood flow through the bronchial arteries and/or focal weakening of the arterial wall, which leads to aneurysm formation.
Most cases present with hemoptysis or pain resulting from mass effect or hemorrhage. Hemodynamic compromise can occur in the setting of rupture (1,3). CT imaging is the diagnostic modality of choice. Because of increased use of cross-sectional imaging, mediastinal bronchial artery aneurysms are now being diagnosed not only in symptomatic patients, but also as incidental findings in the asymptomatic populace (2,4–7).
Treatment is generally indicated on diagnosis because the first presenting symptom(s) may be a result of rupture. In addition, reported cases do not show a size threshold below which mediastinal bronchial artery aneurysms can be safely observed (8,9). Initial treatment efforts relied on surgical resection from midline or lateral thoracotomy. Increasingly, transarterial embolization has been employed as a treatment method, often with similar efficacy as surgery, but with decreased morbidity. One of the limitations of transarterial embolization is spontaneous recanalization of previously occluded vessels. In this scenario, repeat embolization or surgical resection should be performed (1). It may be difficult to safely perform transarterial embolization of bronchial artery aneurysms that arise directly from the aorta with little or no neck. This anatomic challenge may be overcome by the use of detachable coils, which can be optimally positioned before deployment or by anchoring “pushable” coils in smaller branch arteries emanating from the aneurysm sac. Recently, thoracic stent-grafting in conjunction with percutaneous embolization has been used to treat mediastinal bronchial artery aneurysms not anatomically suitable for embolization alone (9,10).
Footnotes
None of the authors have identified a conflict of interest.
References
- 1.Tanaka K, Ihaya A, Horiuci T, et al. Giant mediastinal bronchial artery aneurysm mimicking benign esophageal tumor: a case report and review of 26 cases from literature. J Vasc Surg. 2003;38:1125–1129. doi: 10.1016/s0741-5214(03)00707-9. [DOI] [PubMed] [Google Scholar]
- 2.Zhang LJ, Yang GF, Lu GM. Noninvasive diagnosis of bronchial artery aneurysm using dual-source computed tomography angiography. Acta Radiol. 2008;49:291–294. doi: 10.1080/02841850701753714. [DOI] [PubMed] [Google Scholar]
- 3.Hoffmann V, Ysebaert D, De Schepper A, Colpaert C, Jorens P. Acute superior vena cava obstruction after rupture of a bronchial artery aneurysm. Chest. 1996;110:1356–1358. doi: 10.1378/chest.110.5.1356. [DOI] [PubMed] [Google Scholar]
- 4.Wilson SR, Winger DI, Katz DS. CT visualization of mediastinal bronchial artery aneurysm. AJR Am J Roentgenol. 2006;187:W544–W545. doi: 10.2214/AJR.06.0291. [DOI] [PubMed] [Google Scholar]
- 5.Lin J, Wood DE. Bronchial artery aneurysm refractory to transcatheter embolization. Ann Thorac Surg. 2008;86:306–308. doi: 10.1016/j.athoracsur.2008.01.033. [DOI] [PubMed] [Google Scholar]
- 6.Kasashima F, Endo M, Kosugi I, et al. Mediastinal bronchial artery aneurysm treated with a stent-graft. J Endovasc Ther. 2003;10:381–385. doi: 10.1177/152660280301000235. [DOI] [PubMed] [Google Scholar]
- 7.Kalva SP, Wicky S. Mediastinal bronchial artery aneurysms: endovascular therapy in two patients. Catheter Cardiovasc Interv. 2006;68:858–861. doi: 10.1002/ccd.20902. [DOI] [PubMed] [Google Scholar]
- 8.Fukunaga A, Okushiba S, Ohno K, et al. Mediastinal bronchial artery aneurysm with hematemesis. Dis Esophagus. 2003;16:328–331. doi: 10.1111/j.1442-2050.2003.00360.x. [DOI] [PubMed] [Google Scholar]
- 9.Sanchez E, Alados P, Zurera L, et al. Bronchial artery aneurysm treated with aortic stent graft and fibrin sealant. Ann Thorac Surg. 2007;83:693–695. doi: 10.1016/j.athoracsur.2006.06.082. [DOI] [PubMed] [Google Scholar]
- 10.Sakai T, Razavi MK, Semba CP, Kee ST, Sze DY, Dake MD. Percutaneous treatment of bronchial artery aneurysm with use of transcatheter coil embolization and thoracic aortic stent-graft placement. J Vasc Interv Radiol. 1998;9:1025–1028. doi: 10.1016/s1051-0443(98)70445-2. [DOI] [PubMed] [Google Scholar]