

Abstract
We report a case of juvenile allergic urethritis secondary to double concentrate orange squash of a famous brand in a 3-year-old boy who developed bilateral urethro-ejaculatory reflux (UER) and severe urethral, perineal and scrotal pain referred to both lower limbs intermittently predominantly during and after micturition-simulating features of bilateral intermittent testicular torsion. Accurate history, urinalysis, ultrasound, colour Doppler and food challenge were helpful in diagnosis. Topical steroids, antihistaminic, analgesic and anti-inflammatory medications together with withdrawal of the allergen produced complete recovery. Allergic urethritis in association with bilateral UER causing secondary seminal vesiculitis and epididymitis is rare. It presented as acute scrotum and responded to innovative treatment. Allergic disease can have a dramatic effect on a child’s quality of life. This is the first documented case of allergic urethritis and associated UER presenting as juvenile acute scrotum. Steroids, antihistamines and anti-inflammatory agents together with avoidance of the allergen helped achieve recovery.
Background
Recently, there has been a dramatic increase in the number of children suffering from allergic diseases such as asthma, hay fever, eczema and food allergies. Food additive allergic reactions are intolerance to artificial and natural chemicals found in processed, packaged and ‘take-away’ fast foods. Usually, allergies affect the skin, and respiratory and gastrointestinal systems; primary involvement of the genitourinary tract in a severe allergic reaction in a dramatic presentation of an acute scrotum is exceptional. We report an unusual case that we encountered recently and managed successfully.
Case presentation
A 3-year-old boy was referred to the paediatric surgeons by his general practitioner, who was concerned about recurrent bilateral testicular torsion. The patient presented with a 5-day history of recurrent severe penile, bilateral scrotal pain and radiation of pain to both lower limbs, with limping and crawling. He had 4–5 daily episodes of intermittent severe pain in the urethra, scrotum, groin and both lower limbs. The episodes were characterised by the boy screaming in pain, holding his penis and scrotum, associated with leg pains and a limp more on the right than the left side. At each episode of severe pain, typically triggered by the act of micturition, he would typically hold his voiding, stop his activities, start crawling around, and be very reluctant to stand up and walk. This would last during micturition and for a few minutes thereafter, and occur a few times in quick succession, with pain-free episodes of several hours. His mother had not identified any obvious trigger. He was completely well in between episodes of pain, and these never occurred at night when he was fast asleep. When seen in the emergency department, he denied any pain.
He was a term baby and had no significant medical problems. He had mild eczema and was recently diagnosed with asthma. On further questioning, it appeared that the pain was associated with urination, and that the boy had started drinking double concentrate orange squash from a famous brand about 1 week prior and these episodes followed within a day or two of starting this new concentrate.
On examination, he was well and playful. Inspection of abdomen and legs was unremarkable. There was redness and tenderness centred around the external urinary meatus with oedema and redness reaching half way on the glans penis. The scrotal skin appeared normal in colour, thickness and texture, with presence on normal creases, but there was fullness on both the sides over the epididymis area of the scrotum. There was no testicular or abdominal tenderness. Both testes were palpated in the scrotum, the right more large and retractile than the left, and were of grossly similar size. The right epididymis was more tender, and slightly bigger and thicker than the left.
During the allergen challenge, there was anterior urethral tenderness down into the bulb of the urethra in the perineum and in the groin over the spermatic cord area, and both scrotal areas were tender, especially over the epididymis region.
Investigations
Urine dipstick detected traces of protein and white cell counts but no red blood cells or nitrites. Urine culture showed no organisms.
Ultrasound scan of the upper urinary tract was normal. The bladder showed no abnormality. Both seminal vesicles within the prostate gland were enlarged on ultrasound scan and vascular on colour Doppler study, with the right being very prominent and more vascular than the left (figure 1A, B). Both the epididymides were enlarged, tender and vascular, with the right being larger and more vascular than the left (figure 2A, B). The right testis was bigger than the left, but both were non-tender and had good vascularity (figure 3A, B).
Figure 1.
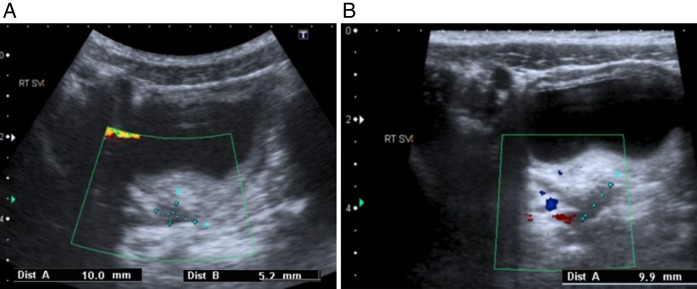
Ultrasound scan and colour Doppler of the pelvis showing enlarged and vascular seminal vesicles, the right (A) being more enlarged than the left (B).
Figure 2.
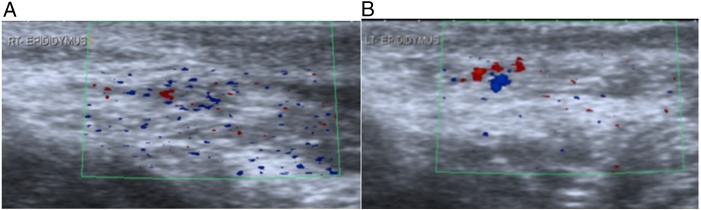
Ultrasound scan and colour Doppler of both epididymides showing enlarged and vascular epididymis, the right (A) being more enlarged than the left (B).
Figure 3.
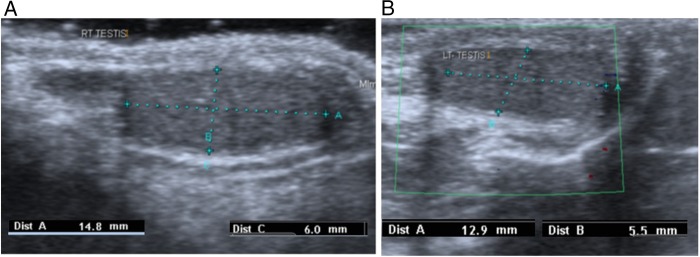
Ultrasound scan and colour Doppler of both testis, the right (A) being larger than the left (B).
The ingredients of the double concentrate orange squash were checked; they included water, sugar, orange fruit from concentrate (20%), citric acid, natural flavouring, sweeteners (aspartame, saccharin), acidity regulator (sodium citrate), preservatives (potassium sorbate, sodium metabisulfite), stabiliser (cellulose gum) and natural colour (carotenes), and contained a source of phenylalanine.
Pure fresh orange juice was given for 2 days, without producing any symptoms, and was well tolerated. A food challenge was carried out on the third day, with a standby arrangement for dealing with acute severe hypersensitivity reaction with adrenaline, chlorpheniramine and hydrocortisone sodium succinate, in view of the patient's pre-existing asthma and eczema placing him at higher risk of such reaction including anaphylaxis.
The challenge began by giving the patient the double concentrate orange squash in increasing quantities, while watching very closely for pain in the penile shaft, urethral pain and leg pains during micturition. Morning micturition was normal, but on subsequent micturition, the boy began having increasing pains and all his earlier symptoms returned. These symptoms were treated immediately with topical steroid cream, paracetamol, ibuprofen and antihistaminic chlorpheniramine medications. This proved to be the best test to show that the boy was allergic to the double concentrate orange squash, and its persistent avoidance resulted in a lasting cure.
Differential diagnosis
Initial referral being intermittent bilateral testicular torsion could neither be confirmed nor excluded. Bilateral epididymo-orchitis was considered likely, but the urine dipstick was not suggestive of urinary tract infection. A torsion of hydatid cyst was unlikely to be intermittent and bilateral. There were no features suggestive of idiopathic scrotal oedema. On detailed enquiry and clinicopathological correlation with imaging findings, juvenile allergic urethritis in association with bilateral urethro-ejaculatory reflux, seminal vesiculitis and epididymitis secondary to double concentrate orange squash of a famous brand, was contemplated.
Treatment
The patient was treated with topical steroid cream, paracetamol, ibuprofen and chlorpheniramine together with avoidance of the allergen, which provided lasting relief. At the food challenge, all the symptoms reappeared and the same treatment quickly resolved this. We reassured the parents and advised them to give the boy plenty of fluids and keep up good hygiene so as to avoid any allergic reaction and inflammation that might lead to recurrence of the severe pain and symptoms.
It was explained to the patient and his parents that the boy had an allergy and inflammation secondary to the contents of the concentrated orange juice, which led to inflammation of his urethra. This had further led to a temporary bilateral urethro-ejaculatory reflux secondary to oedema and swelling within the urethra, raising intraurethral pressure and leading to the painful epididymis more on the right side, and abnormal gait due to inflammatory pain in both seminal vesicles. All symptoms settled after the intervention and the boy reverted to normal.
Outcome and follow-up
Once the boy consistently avoided the concentrated orange squash and applied topical steroid cream, symptoms promptly reversed. He is eating and drinking normally, and playing and running around without any genital, urinary, pelvic or limb discomfort. He has progressed very well, and is currently completely asymptomatic and thriving well at follow-up.
The parents have been given the option of referring to a paediatric allergy clinic for further tests, but the complete reversal of symptoms on avoiding the allergen and repeat symptoms on re-introduction, have suggested allergic urethritis as the possible diagnosis. In addition, the child is hospital and needle phobic and does not cooperate; so skin and blood tests will only be carried out if he runs into problems of recurrence.
Discussion
Non-specific urethritis in children is seen in adolescent boys and is a benign, rare, self-limiting and mild disease. In a recent case, a juvenile form of allergic urethritis clinically simulated cauda equina syndrome in a dramatic presentation requiring MRI of the spine. Although it is called idiopathic, there are three primary underlying mechanisms thought to cause this non-specific urethritis, namely allergy, inflammation and infection.
Our case, for the first time in the literature, has suggested an allergic aetiology and occurrence in a younger age group, as most idiopathic non-specific urethritis is seen in adolescents.1–3 Patel et al, for the first time, demonstrated urethrovasal reflux in a case of idiopathic adolescent posterior urethritis leading to recurrent acute scrotum requiring unnecessary scrotal explorations.
Various food additives used, including preservatives, flavour enhancers to improve food palatability, colourings to make food visually more attractive, sweeteners, emulsifiers, stabilisers and naturally occurring substances in food, especially vasoactive amines, can cause adverse reactions.4 Histaminuria from histamine-rich food may be responsible for allergic urethritis, and histamine content of oriental food may be high.
Many of the additives are harmless but, recently, preservative sensitivity has been a concern for allergic reactions. Preservatives give food longer shelf-life, and in our case, sodium metabisulfite was used in the double concentrate orange squash, which may have been the culprit. Sulfites found in fruit juice concentrate can cause urticarial, airway and mucosal irritation.
Relatively few adverse reactions are actually reported when additives are compared to nuts, eggs and other foodstuff. However, not only physical reactions but adverse hyperactive behavioural changes in children have also been documented when excess amounts of artificial food colouring and sodium benzoate preservatives are part of the diet.5
Usually, acute epididymitis in infants presenting as acute scrotum may have congenital anomalies of ectopic ureteric insertion in seminal vesicles or persistent utricle, but our case throws light on the fact that there may be reasons to believe that primary epididymal inflammation occurs more often than supposed through other mechanisms.6
Urethro-ejaculatory reflux is the primary mechanism, and it is often associated with urogenital anomalies among infants and dysfunctional voiding among young boys.7 The increasing incidence of epididymitis should raise questions on the policy of routine exploration of acute scrotum in children.8
Allergy is a hypersensitivity reaction to allergens that are normally tolerated. In an allergic reaction, the interaction between the IgE and the allergen causes the release of inflammatory chemicals such as histamines and leukotrienes, which are responsible for the symptoms leading to difficulty in voiding due to oedema and swelling in the urethra. This causes a temporary rise in intraurethral pressure leading to secondary urethro-ejaculatory reflux. There is transitional epithelium in the upper and middle urinary tract, which is water and chemical proof, while the urethral, meatal, inner and junctional foreskin and genital epithelium are not, thus leading to severe reaction and symptoms.
The diagnosis of food or drink allergy requires a thorough history from the patient and family as well as empirical testing. Genitourinary allergy manifests as reflux into the ejaculatory duct, pain/dysuria and frequency of micturition. Two main types of allergy testing are available: skin patch and blood. Blood testing for allergen specific IgE-antibodies (s-IgEa) has the advantage of being more sensitive and specific, but is not easily available. However, skin testing is easy to use, widely available and quick, and allows for concomitant evaluation of multiple allergens, but it cannot be performed if the patient has a skin disease.9
In the absence of any evidence of infection in most cases of juvenile recurrent balanitis, non-specific adolescent urethritis and balanitis xerotica obliterans (BXO), we believe that the underlying mechanism could be low-grade allergy or autoimmunity to the various additives in packed or processed food, or to artificial or natural biodegradation products, leading to severe ongoing inflammation, as they are very susceptible to steroid treatment.1–3 10 It appears that these are part of a spectrum of diseases, with acute juvenile allergic urethritis being the smallest and most easily reversible lesion at the beginning of the spectrum, followed by balanitis, recurrent balanitis and BXO, in order of severity; further work is required to explore this hypothesis.
Allergy caused by specific food, drink or a preservative should be managed by strict avoidance. In case of anaphylaxis, an adrenaline autoinjector may be needed for prompt treatment, but in most acute phase genitourinary allergies, antihistamines would suffice; also, sodium chromoglycate may be a helpful adjuvant to dietary avoidance. Hydrocortisone is of secondary and preventive value in severely affected patients, to prevent further deterioration, as it takes several hours to be effective clinically. The patient must not be re-exposed and expert advice should be sought.
Allergic reactions associated with additives, preservatives, excipients, colour, flavours, etc, are potentially avoidable and largely preventable. It is always wise to read all processed or packaged food labels and check the full ingredient list or formula of the preparations; legislation now ensures that additives must be clearly labelled. We recommend reading food labels carefully and keeping a food diary to identify offending additives and preservatives. The best practice is to provide fresh fruits and juice, and avoid all processed and packed food at all times in children and adolescents, if at all possible, and encourage a healthy lifestyle to avoid such severe allergic reactions.
Learning points.
Allergic urethritis can have a dramatic effect on a child’s quality of life and can mimic serious conditions such as intermittent bilateral testicular torsion.
Allergies generally affect respiratory, cutaneous and gastrointestinal tracts, and involvement of the genitourinary tract is exceptional; this is the first documented case of double concentrate orange squash-induced juvenile allergic urethritis and associated urethro-ejaculatory reflux leading to bilateral seminal vesiculitis and epididymo-orchitis simulating intermittent bilateral testicular torsion.
Using a food challenge was a good way to diagnose this condition under controlled conditions.
Steroids, antihistamines and anti-inflammatory agents together with allergen avoidance were useful in the treatment.
The increasing incidence of epididymitis and more evidence of other mechanisms responsible for epididymitis should question the policy of routine exploration of acute scrotum in children.
Acknowledgments
The authors are grateful to Catherine Newby, General Practitioner at Southmead and Henbury Family Practice, for prompt referral; and Anne Frampton, Consultant Paediatric Accident and Emergency, for her help and support on the weekend.
Footnotes
Contributors: RVP, MB, DG and TY have made substantial contributions to the conception and design of this paper, search of the literature, acquisition, analysis and interpretation of the data, drafting the article or revising it critically for important intellectual content and to the final approval of the version to be published.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Goring J, Patel R, Asharaf J et al. Experience with instillation triamcinolone into the urethra for idiopathic urethritis. Absracts for 23th Congress of the European Society for Paediatric Urology; Genova, Italy: ESPU, 2013:225. [Google Scholar]
- 2.Ninan GK, Pringle K, Patel RV. Upper urinary tract inflammation and dilatation secondary to idiopathic urethritis—a plea for steroid treatment. Int J Urol 2014;21:348–9. 10.1111/iju.12241 [DOI] [PubMed] [Google Scholar]
- 3.Ninan GK, Bhishma P, Patel R. Steroid treatment for recurrent epididymitis secondary to idiopathic urethritis and urethrovasal reflux. Eur J Pediatr Surg Rep 2013;1:56–9. 10.1055/s-0033-1343076 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ortolani C, Bruinjzeel Koomen C, Bengtsonn U et al. Controversial aspects of adverse reactions to food. Allergy 1999;54:27–45. 10.1034/j.1398-9995.1999.00913.x [DOI] [PubMed] [Google Scholar]
- 5.Bateman B, Warner JO, Hutchinson E et al. The effects of a double blind, placebo controlled artificial food colourings and benzoate preservative challenge on hyperactivity in a general population sample of preschool children. Arch Dis Child 2004;89:506–11. 10.1136/adc.2003.031435 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sakellaris GS, Charissis GC. Acute epididymitis in Greek children: a 3-year retrospective study. Eur J Pediatr 2008;167:765–9. 10.1007/s00431-007-0584-y [DOI] [PubMed] [Google Scholar]
- 7.Kajbafzadeh AM, Taleb S, Montaser-Kouhsari L et al. Urethral triplication and urethrovasal reflux in 5-day-old male infant. Urology 2011;78:186–8. 10.1016/j.urology.2010.09.019 [DOI] [PubMed] [Google Scholar]
- 8.Wiersma R. Urethro-ejaculatory duct reflux in children: an updated review. Eur J Pediatr Surg 2009;19:374–6. 10.1055/s-0029-1234115 [DOI] [PubMed] [Google Scholar]
- 9.Cox L, Williams B, Sicherer S et al. Pearls and pitfalls from the American College of Allergy, Asthma and Immunology/American Academy of Allergy, Asthma and Immunology Specific IgE Test Task Force. Ann Allergy Asthma Immunol 2008;101:580–92. 10.1016/S1081-1206(10)60220-7 [DOI] [PubMed] [Google Scholar]
- 10.Wilkinson DJ, Lansdale N, Everitt LH et al. Foreskin preputioplasty and intralesional triamcinolone: a valid alternative to circumcision for balanitis xerotica obliterans. J Pediatr Surg 2012;47:756–9. 10.1016/j.jpedsurg.2011.10.059 [DOI] [PubMed] [Google Scholar]