

Description
A previously well 3-year-old child presented with retrosternal pain and dysphagia. She reported swallowing a round metal object, which was presumed to be a coin. Physical examination and vital signs were unremarkable.
This was further investigated with an anteroposterior (AP) chest X-ray, which demonstrated a circular radiopaque foreign body in the distal oesophagus (figure 1). As she was stable, a conservative approach was adopted to see if the foreign body would spontaneously pass through the gastrointestinal tract.
Figure 1.
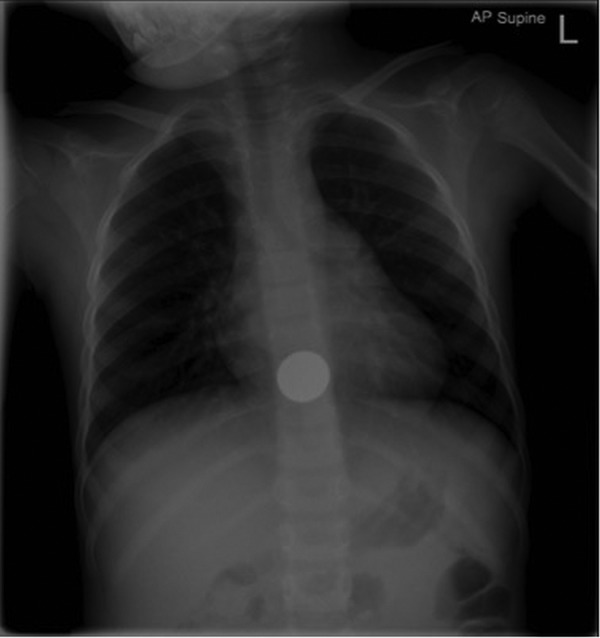
Anteroposterior chest X-ray demonstrating a circular foreign body in the distal oesophagus with presumed ‘halo’ sign.
The next morning, she had a repeat AP chest X-ray, which showed the foreign body still located in the distal oesophagus. It was noted that the circular opacity on the radiograph had a ‘halo’ sign (normally seen in presence of a button battery), therefore prompt endoscopic retrieval was performed (figure 2). Unexpectedly, the foreign body revealed to be two overlapping one pence coins which simulated a ‘halo’ sign on X-ray (figure 3).
Figure 2.

Endoscopic view of two coins in the oesophagus.
Figure 3.

Two overlapping coins retrieved from the oesophagus.
Ingestion of foreign body is a common problem in children and it is important to differentiate between button battery and coin ingestion. This is because of the difference in terms of treatment required. Oesophageal button batteries necessitate urgent removal whether the patient is symptomatic or not as they can cause major corrosive injury within 2 h of ingestion.1 Coin ingestion can initially be managed conservatively if the patient is asymptomatic although it may require removal should it become impacted. Ingestion of more than one coin is a reported contraindication to bougienage.2
In this case, a lateral view plain film may have helped to determine the number of coins and differentiated them from a button battery, which sometimes shows a ‘step-off’ sign on the lateral view in contrast to coins.1
Taking into account the potential harmful complications of button battery ingestion, it is our practice to always err on the side of caution when diagnosis is in question and expedite endoscopic retrieval.
Learning points.
Coins and button batteries are the most commonly ingested foreign bodies in children.3
A button battery in the oesophagus has to be urgently removed as major corrosive injury can occur within 2 h of ingestion.1
In case of multiple coin ingestion or unclear history from parent/patient, anteroposterior (AP) and lateral radiographs may both help in differentiating coins from button batteries.
Button batteries are identifiable by a ‘halo’ sign on AP and sometimes a ‘step-off’ sign on lateral X-rays.1
Footnotes
Contributors: RWCG wrote the case and performed the literature review. ON, PBJ and SS revised and provided additions to the drafts and highlighted the learning messages.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Jatana KR, Litovitz T, Reilly JS et al. Pediatric button battery injuries: 2013 task force update. Int J Pediatr Otorhinolaryngol 2013;77:1392–9. doi:10.1016/j.ijporl.2013.06.006 [DOI] [PubMed] [Google Scholar]
- 2.Jona JZ, Glicklich M, Cohen RD. The contraindications for blind esophageal bouginage for coin ingestion in children. J Pediatr Surg 1988;23:328–30. [DOI] [PubMed] [Google Scholar]
- 3.Ludemann JP, Dehghani N. Ingested foreign bodies in children—BC Children's Hospital Emergency Room Protocol. BCMJ 2008;50:257–61. [Google Scholar]