

Abstract
Blunt chest traumas mostly occur due to car accidents and can cause many cardiac complications such as septal rupture, free-wall rupture, coronary artery dissection or thrombosis, heart failure, arrhythmias, and chordae and papillary muscle rupture. One of the most serious complication is tricuspid regurgitation (TR), which can be simply diagnosed by physical examination and confirmed by echocardiography. We describe a 48-year-old female patient, diagnosed with severe TR 13 years after a blunt chest trauma due to a car accident. TR was diagnosed with transthoracic echocardiography and three dimensional transthoracic echocardiography had defined the exact pathology of the tricuspid valve. The patient underwent successful surgery with bioprosthetic valve implantation and was discharged at 6th postoperative day without any complication. The patient had no problem according to the follow-up one month and six months after operation.
Keywords: Tricuspid valve insufficiency; Thoracic injuries; Echocardiography, three-dimensional; Tricuspid valve; Heart rupture
Introduction
Severe cardiac injuries after blunt chest traumas are life-threatening complications that are not rare.1 These traumas can lead to septal rupture, free-wall rupture, coronary artery thrombosis, heart failure, arrhythmias, chordae or papillary muscle rupture, and valvular injuries.1 Among the complications of valvular injuries, tricuspid regurgitation (TR)is the most common.2 In the acute phase of the trauma, the diagnosis of TR may be missed in the emergency department because of its well-tolerable nature as well as the presence of other more major concerns. Consequently, the patient may be diagnosed with TR several months or years after the index event. Two-dimensional transthoracic echocardiography (2-D TTE) is mostly sufficient for diagnosis when conducted by an experienced physician. Three-dimensional transthoracic echocardiography (3-D TTE) and three-dimensional transesophageal echocardiography (3-D TEE) may provide beneficial information on the anatomy of the valve thanks to their better anatomic and spatial resolutions.3
Case Report
A 48-year-old female patient was admitted to our hospital with shortness of breath and extreme fatigue during daily activities, previously diagnosed as hypertension and controlled with medication. She had a history of a blunt trauma to her chest in a car accident 13 years earlier. There was a holosystolic murmur (grade 3) in the fourth intercostal space at the left sternal border, which increased with inspiration, as well as pretibial edema and jugular venous distention during physical examination. Electrocardiography showed atrial fibrillation and right bundle branch block. Flail tricuspid valve, right ventricular volume overload, and reduced right ventricular function were determined by 2-D TTE (Figure 1), and severe TR was established by Doppler echocardiography (Figure 2). Further examinations were performed via 3-D TTE to define the exact pathology of the valve (Figures 3 and 4). Both posterior and anterior leaflets were flail, and there was a coaptation defect. In addition, severely dilated right atrium and right ventricle were detected. All of the tricuspid leaflets were affected. Because of the chronicity of the lesion, the leaflets were thickened and their movements were restricted, probably owing to the chronic inflammation and fibrosis of the leaflets and the subvalvular apparatus. Based on these echocardiographic findings and the patient’s complaints, tricuspid valve replacement was planned. The valve was not suitable for repair, and bioprosthetic valve implantation was performed successfully. The patient was discharged without postoperative complications.
Figure 1.
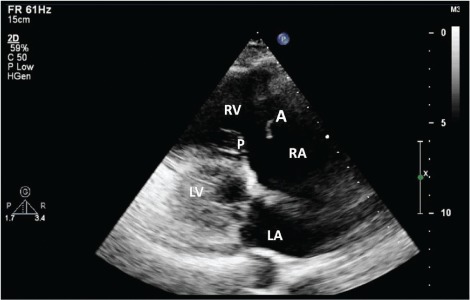
Transthoracic two-dimensional echocardiography, showing dilated right ventricle and right atrium, flail anterior leaflet of the tricuspid valve, and thickened and partly mobile posterior leaflet of the tricuspid valve from the parasternal long-axis view of the right ventricular inflow tract at mid-systole
LA, Left atrium; LV, Left ventricle; RA, Right atrium; RV, Right ventricle; A, Anterior leaflet of the tricuspid valve; P, Posterior leaflet of the tricuspid valve
Figure 2.

Doppler echocardiography, showing severe tricuspid insufficiency due to coaptation defect of tricuspid valve (asterisk) from the apical view tract at systole
LA, Left atrium; LV, Left ventricle; RA, Right atrium; RV, Right ventricle
Figure 3.

Transthoracic three-dimensional echocardiography, revealing severely dilated right ventricle and right atrium, flail and thickened anterior leaflet of the tricuspid valve, affected septal leaflet, and coaptation defect of the tricuspid valve in the apical four-chamber view at mid-systole
LA, Left atrium; LV, Left ventricle; RA, Right atrium; RV, Right ventricle; S, Septal leaflet of the tricuspid valve; A, Anterior leaflet of the tricuspid valve
Figure 4.

Transthoracic three-dimensional echocardiography view of tricuspid valve from the atrial aspect at ventricular systole showing destructed anterior and posterior leaflets of the tricuspid valve (arrows) and coaptation defect.
Ao, Aorta; MV, Mitral valve; TV, Tricuspid valve; A, Anterior leaflet of the tricuspid valve; P, Posterior leaflet of the tricuspid valve
Discussion
The most common cause of TR is the dilatation of the right ventricle and functional causes. The literature contains an increasing number of the reported cases of TR due to traumas because of echocardiography availability in the emergency services and increased frequency of car accidents.4 The most frequently reported injury with TR is chordal rupture, followed by the anterior papillary muscle and leaflet tear. These injuries are thought to occur due to a sudden increased right ventricular pressure against a closed tricuspid valve, with the pressure causing the traction of the valvular and subvalvular apparatus.5 Although TR remains usually asymptomatic because of its nature, it can be diagnosed years after a blunt chest trauma, as was the case in our patient, and the prognosis is poor in these patients.6, 7 Eventually, severe TR can lead to severe right ventricular dilatation and right ventricular failure.
Sometimes 2-D images are not adequate for planning surgery and 3-D TTE may prove helpful. Indeed, 3D images can guide the surgery and help select the most appropriate approach. As was seen in our patient, a blunt chest trauma can cause damage to more than one leaflet and more than one valve, so echocardiographic examination is critical when a blunt chest trauma occurs. All clinicians should be aware of such complications because the early diagnosis of acute severe regurgitation is important inasmuch as it may require urgent surgery. General consensus has it that valve repair, if possible, is preferable to valve replacement. The timing of surgery mostly depends on pulmonary hypertension and symptomatic right ventricular failure,4 and the type of surgery depends on the patient’s pathology of the valve.8
In an emergency setting, it may not be possible to perform echocardiography due to the patient’s chest injury. TEE may be required when the physician suspects cardiac damage.9 Indeed, TEE is reliable, yields high quality images of the valves, and can be used to assess myocardial or valve injury in cases where TTE is inadequate. Recent advances in 3-D TEE confer better assessment of valvular heart disease, guidance of interventional procedures such as the closure of paraprosthetic leaks and atrial septal defects, accurate identification of the mitral valve prolapse, and measurement of the aortic valve area in aortic stenosis.10
Conclusion
Blunt chest truma can lead to various cardiovascular complications such as rupture of heart valve leaflets and serious aortic injuries. In some circumstances the damage was detected years after the accident. TTE and TEE are important modalities that can be used in emergeny departments. 3-D TTE and TEE are also helpful for the patients that TTE can not be performed because of the chest trauma; for to guide the surgery
References
- 1. Wall MJ, Tsai PI, Mattox KL. Traumatic heart disease. In: Braunwald E, Bonow RO, Mann DL, Zipes DP, Libby P. eds. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 9th edition Philadelphia: Elsevier Saunders; 2012; p. 1675–1676. [Google Scholar]
- 2. Schuster I, Graf S, Klaar U, Seitelberger R, Mundigler G, Binder T. Heterogenity of traumatic injury of the tricuspid valve. A report of four cases. Wien Klin Wochenschr 2008; 120: 499–503. [DOI] [PubMed] [Google Scholar]
- 3. Fukuda S, Saracino G, Matsumura Y, Daimon M, Tran H, Greenberg NL, Hozumi T, Yoshikawa J, Thomas JD, Shiota T. Three-dimensional geometry of the tricuspid annulus in healthy subjects and in patients with functional tricuspid regurgitation: a real-time, 3-dimensional echocardiographic study. Circulation 2006; 114: I492–498. [DOI] [PubMed] [Google Scholar]
- 4. Lin SJ, Chen CW, Chou CJ, Liu KT, Su HM, Lin TH, Voon WC, Lai WT, Sheu SH. Traumatic tricuspid insufficiency with chordae tendinae rupture: a case report and literature review. Kaohsiung J Med Sci 2006; 22: 626–629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Dounis G, Matsakas E, Poularas J, Papakonstantinou K, Kalogeromitros A, Karabinis A. Traumatic tricuspid insufficiency: a case report with a review of the literature. Eur J Emerg Med 2002; 9: 258–261. [DOI] [PubMed] [Google Scholar]
- 6. Gayet C, Pierre B, Delahaye JP, Champsaur G, Andre-Fouet X, Rueff P. Traumatic tricuspid insufficiency. An underdiagnosed disease. Chest 1987; 92: 429–432. [DOI] [PubMed] [Google Scholar]
- 7. Messika-Zeitoun D, Thomson H, Bellamy M, Scott C, Tribouilloy C, Dearani J, Tajik AJ, Schaff H, Enriquez-Sarano M. Medical and surgical outcome of tricuspid regurgitation caused by flail leaflets. J Thorac Cardiovasc Surg 2004; 128: 296–302. [DOI] [PubMed] [Google Scholar]
- 8. Jin HY, Jang JS, Seo JS, Yang TH, Kim DK, Kim DK, Kim U, Seol SH, Kim DI, Kim DS. A case of traumatic tricuspid regurgitation caused by multiple papillary muscle rupture. J Cardiovasc Ultrasound 2011; 19: 41–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Looi JL, Lee AP, Wong RH, Yu CM. 3D echocardiography for traumatic tricuspid regurgitation. JACC Cardiovasc Imaging 2012; 5: 1285–1287. [DOI] [PubMed] [Google Scholar]
- 10. Sugeng L, Shernan SK, Salgo IS, Weinert L, Shook D, Raman J, Jeevanandam V, Dupont F, Settlemier S, Savord B, Fox J, Mor-Avi V, Lang RM. Live 3-dimensional transesophageal echocardiography initial experience using the fully-sampled matrix array probe. J Am Coll Cardiol 2008; 52: 446–449. [DOI] [PubMed] [Google Scholar]