

Abstract
Prostatic urethral lift (PUL) is a minimally invasive procedure for the treatment of lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia. The procedure may be performed under local, spinal, or general anesthesia. The PUL procedure involves the delivery of implants that retract obstructing prostate lobes. Unlike other benign prostatic hyperplasia treatment options including pharmacological therapy, and the current invasive gold-standard transurethral resection of the prostate, the PUL procedure achieves quantifiable improvements in functional outcomes and quality of life, in the absence of major adverse events. Furthermore, improvement in LUTS may be attained while preserving erectile and ejaculatory function. Adverse effects associated with the PUL procedure are mild to moderate, and are transient in nature. The PUL procedure provides an alternative for men seeking treatment for bothersome LUTS, with fewer side-effects.
Keywords: Benign prostatic hyperplasia, Minimally invasive surgery, Prostatic urethral lift, Urolift
1. Introduction
Benign prostatic hyperplasia (BPH) is a common, age-related condition that can manifest clinically as lower-urinary tract symptoms (LUTS). LUTS associated with BPH increase with age, as does the need for intervention.
Treatment options include watchful waiting, pharmacotherapy, and surgery. The primary pharmacotherapy options commonly include α-blockers and 5α-reductase inhibitors (5ARIs). More recently, there has been an increasing use of phosphodiesterase type 5 inhibitors, antimuscarinic agents, and β-3 agonists. The gold standard for surgical intervention has been transurethral resection of the prostate (TURP), although laser technologies are increasing in popularity as an alternative to TURP. Minimally invasive surgical treatments such as transurethral needle ablation of the prostate and transurethral microwave thermotherapy were, for a time, popular alternatives to TURP but their use is declining. This has created a void in the therapeutic landscape and in recent years, the prostatic urethral lift (PUL) procedure has emerged as a promising alternative for men seeking treatment for bothersome LUTS, with fewer side-effects.
This review will summarize what is known about PUL as a minimally invasive treatment for LUTS due to BPH.
2. The Urolift device
PUL is performed using the Urolift device (NeoTract Inc., Pleasanton, CA, USA; Fig. 1). The procedure is performed endoscopically utilizing a 19F or 20F cystoscope sheath. The Urolift device is a custom designed disposable cartridge that accepts a 2.9-mm 0° 36-cm telescope lens. The cartridge is configured to deliver a single prosthesis that is constructed of a Capsular nitinol tab and a urethral stainless steel tab bridged by a nonabsorbable suture. The suture is under tension and draws the prostatic urethra to the prostate capsule.
Fig. 1.
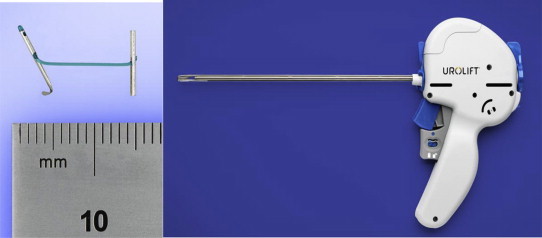
The Urolift system comprising customizable nylon sutures and the suture delivery device which is introduced under cystoscopic guidance. Images copyright NeoTract, Inc., Pleasanton, CA, USA.
3. Technique
The PUL procedure aims to create an anterolateral channel from the bladder neck to the verumontanum. The procedure may be performed under local, spinal, or general anesthesia, with or without additional sedation. The ability to perform the procedure under local anesthesia may be advantageous for patients with significant multiple comorbidities.
Patients are placed in the lithotomy position and a cystoscopy is performed to inspect the bladder neck and prostate, particularly the configuration of the middle and lateral lobes.
The first deployment should be performed at least 1.5 cm distal to the bladder neck with the device angled 20–30° from the 12 o'clock midline to ensure that the needle path is parallel to the bladder neck. The handle of the device is rotated in the axial plane to align with the proposed site of prosthesis deployment in the anterolateral part of the prostatic urethra. The needle, when released, travels in an arc and therefore correct positioning is essential to ensure that the needle does not travel through the bladder neck and proximally into the bladder base.
Angulation of the device may be done by either moving the tip of the device away from the midline in the direction of the needle path, or by moving the handle of the device away from the midline in the opposite direction of the needle. The latter maneuver is preferable as it causes less mucosal trauma, does not move the prostate laterally, and ensures that the prostate and device is not displaced laterally so that the needle is in danger of reaching the pelvic side-wall.
Once the tip of the device is in the desired position it is deployed using the following sequence (Fig. 2):
-
(1)
Unlock the trigger.
-
(2)
Pull the top half (blue) of the trigger. This will fire a hollow Nitinol curved needle through the prostate and its capsule, bringing with it the capsular anchor and the nylon suture.
-
(3)
Pull the whole trigger (blue and gray parts) back. This will retract the hollow needle and tension the suture.
-
(4)
Advance the whole instrument towards the bladder neck ensuring that the blue suture fits into the notch (keyhole), until a glistening white line (Fig. 3) appears on the suture (it appears to run along the suture).
-
(5)
Depress the button on the back of the instrument to deploy the urethral anchor and cut the suture (occurs automatically).
-
(6)
Move the tip of the instrument directly to the midline to ensure that the urethral anchor falls away from the instrument. This maneuver ensures that the Urolift staple has been fully deployed and is not attached anymore, before advancing the instrument back into the bladder.
-
(7)
Leave the sheath in the bladder and decide if further devices or an assessment cystoscopy is needed.
Fig. 2.
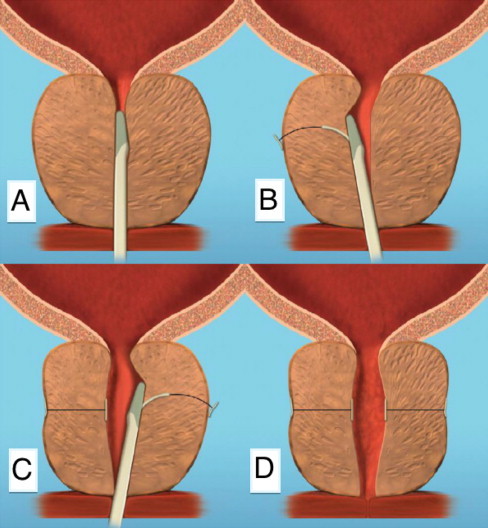
The delivery sequence of the Urolift device. (A) The device in introduced under cystosopic guidance; (B) the lateral lobes of the prostate are compressed by the device and the needle is deployed; and (C) additional sutures are delivered if needed to maintain (D) a patent urethral lumen.
Fig. 3.

The glistening white line.
Assessment cystoscopy should follow every two deployments to assess the effect of the Urolift on the configuration of the prostate. From the verumontanum, it should be possible to see an open anterior channel through to the bladder neck with no irrigation flow. Placement of additional devices may be necessary; the exact number, however, will vary depending on the response of the prostate to retraction. The number of devices required can range from two to 10 depending on the size and shape of the adenoma.
4. Patient selection
The ideal prostatic anatomy for a successful Urolift procedure is where the lateral lobe enlargement is responsible for bladder outlet obstruction. The bladder neck should be normal with minimal middle lobe enlargement. The size of the prostate in selected patients should not exceed 100 mL. The procedure may be performed using light general or local anesthesia, with or without additional sedation.
The Urolift procedure should be an option when considering management of BPH in patients seeking treatment for bothersome LUTS. As there is no de-novo sexual or ejaculatory dysfunction associated the Urolift procedure,1 the Urolift may be ideal for younger, sexually active men who request management of bothersome LUTS. Men who may not want to take lifelong medication, have failed medical management, or are averse to cavitating surgery would also be suitable for the Urolift procedure. The Urolift provides a minimally invasive and effective addition to the current management options for bothersome LUTS due to BPH.
5. Clinical outcomes
The PUL procedure has been shown to be efficacious in improving symptom scores and quality of life (QoL) in men with LUTS.2,3 Not only are the clinical outcomes following PUL immediate, but they have also demonstrated durability for up to 2 years. Durable clinical outcomes are obtained without coincident serious adverse events or sexual dysfunction associated with other BPH/LUTS treatments.
The results of a multicenter prospective cross-over trial demonstrated the ability of PUL to provide clinically and statistically significant improvements in LUTS and QoL. International Prostate Symptom Score (IPSS), Health Related Quality of Life (HRQL), BPH Impact Index (BPHII), and Maximum urinary flow rate (Qmax) were improved when compared to the sham control. Mean IPSS improvement was 122% greater than the sham control (11.1 points vs. 5.0 points). Of note, the IPSS score for both the sham and crossover PUL groups at 2 weeks demonstrated a change from baseline. The authors of this study hypothesize that the change in IPSS in sham patients may be due to a combination of psychological effects of sham treatment, in addition to temporary urethral dilation following rigid cystoscopy. This sham effect was shown to diminish over time.4
Improvements in BPHII, HRQL, and Qmax were also evident when compared to the sham controls. Qmax increased from 7.9 mL/s at baseline to 10.3 mL/s 3 months postsham, and 12.0 mL/s 3 months post-PUL; the improvement in Qmax following PUL was sustained to 12 months (12.5 mL/s).4 The improvements in clinical outcomes demonstrated in this study are also reflected in previous randomized blinded studies of PUL.1,5 Improved clinical outcomes were prompt with reductions in American Urological Association Symptom Index (AUASI) by four points from baseline at 2 weeks, and 11 points at 3 months post-PUL. The reduction in AUASI was 88% greater than that of the sham control and the improvement in this parameter was improvement that was sustained to 12 months. Additional clinical outcomes including Qmax, QoL, and BPHII were also significantly improved compared to the sham control.4 These improvements have also demonstrated durability in a recent 2-year follow-up study, with sustained improvements in QoL, improved Qmax between 12 months and 24 months, and a slight decrease in symptom relief by 24 months.6
The rate of retreatment in patients was 5% at 1 year, with 1.4% of patients requiring TURP and laser vaporization, in addition to 3.6% of patients requiring PUL revisions.4 Retreatment rate at 2 years increased to 7.1%.6 Rates of retreatment are similar to other published studies including a previously published Australian multicenter study.2 This study similarly demonstrated a rapid and sustained improvement in functional and clinical outcomes. The decrease in IPSS was immediate, as demonstrated in other published studies [7,8], with a 42% decrease at 2 weeks, and 49% at 6 months. The improvement showed durability with a 42% decrease at 2 years; this improvement in IPSS was statistically significant at all follow-up intervals. BPHII decreased by 39% by 2 weeks, and evidenced a 60% reduction at 2 years. QoL also demonstrated a durable improvement from an average 4.9 at baseline to 2.5 at 1 year and 2 years. Similarly, Qmax also demonstrated statistically significant improvement with an average increase of 30% at all intervals. Improvements to IPSS, BPHII, QoL, and Qmax were statistically significant at all intervals; similar results have been demonstrated in other studies.1,7,8 Retreatment rates were 20% with 13 of 64 patients requiring TURP, repeat PUL, or vaporization of the prostate. Of the patients who required retreatment, 77% were among the first patients treated in this study. The cumulative retreatment rates for the last 39 patients in this study were 8%.2
6. Adverse events
Unlike other available treatments for BPH associated LUTS, PUL has demonstrated a unique ability to mitigate the symptoms of LUTS while avoiding the adverse events associated with both pharmacological and more invasive treatment modalities. Early safety and feasibility studies have shown that adverse events associated with the PUL procedure are mild, transient, and have rapid resolution.3 The favorable safety profile of PUL makes it an appealing option for the treatment of BPH-associated LUTS for both patients and urologists.
In a randomized blinded trial of 206 men, only two serious adverse events were related to the PUL procedure. These serious adverse events involve an instance of clot retention in association with reinitiation of warfarin therapy, and the second serious event involved a patient who required removal of a bladder stone at 12 months; stone formation in this instance was not associated with the implants.5 The more common adverse events in this randomized study included postoperative dysuria, discomfort, urgency, and hematuria. As emphasized in other studies [7], these adverse events were mild to moderate and resolved within a 2-week period. Following the PUL procedure, 94% of patients agreed to undergo follow-up cystoscopy at 12 months. Of the 127 cystoscopy recordings available for review, none demonstrated any abnormal pathology or strictures. Furthermore, there was no evidence of encrustation in implants that had been delivered within the prostate.5
Following unblinding of the sham group patients, eligible patients were given the opportunity to receive treatment with PUL, and enrolled into a subsequent cross-over study published this year.4 The sham patients essentially became their own control for this study. The most common adverse events experienced post-PUL included dysuria, hematuria, and pelvic pain, with 36%, 26%, and 21% of patients affected, respectively. These adverse events were also experienced in sham patients. The severity of adverse events in this study was classified according the Clavien–Dindo classification system. Two Class III events occurred in relation to urinary retention, with one patient requiring readmission to hospital for 2 days. None of the adverse events reported in this study were Class IV or V. Again, such adverse events were demonstrated to be mild and transitory.4
Similar results were also published by Shore et al8 in a prospective multicenter study of 51 patients. Adverse events were, again, mild to moderate Clavien–Dindo Grade I events and resolved within one month. Hematuria was the most common adverse event with 80% of patients experiencing transient hematuria that lasted for a median 4 days, followed by dysuria (74%), incontinence (25%), and pelvic pain (20%).8 Symptoms of transient dysuria (25%), hematuria (16%), and urgency (10%) were also reported by McNicholas et al7 in 102 patients treated with PUL. Additionally, there were three cases each of urinary retention, urinary tract infection, and orchitis, all of which were treated routinely.7 No serious adverse events were reported in either of these studies.
The results of these recent studies have also been demonstrated in the earlier publications. Again, Clavien Grade I symptoms including hematuria and dysuria were common among treated patients, with these symptoms typically resolving within the 1st week following PUL (2). Urge incontinence was also reported in 8% of patients and generally resolved by 8 days on average. Infective complications including rigors, urinary tract infection, epididymo-orchitis, and prostatitis occurred in 10 patients (16%). A single patient with a history of cardiovascular disease, requiring anticoagulant washout prior to PUL, suffered an Non-ST elevation myocardial infarction (NSETMI). These adverse events were treated appropriately without any long-term complications. There were no Calvien Class III, IV, or V events. Additionally, no long-term complications related to the presence of implants were noted on 6-month cystoscopy follow-up in 22 patients examined.2
7. Sexual function
The absence of ejaculatory or erectile adverse effects is a clear advantage of the PUL procedure. To date, there has been no reported deterioration in erectile or ejaculatory function post-PUL. The tissue-sparing nature of the PUL procedure underlies its ability to preserve sexual function in patients. Since the procedure does not affect the integrity of the bladder neck, antegrade ejaculation is maintained and in the absence of thermal tissue damage, the risk of erectile dysfunction (ED) is minimized.9
An early Australian study of PUL and sexual function demonstrated no degradation in sexual function following PUL. Improvements in Sexual Health Inventory for Men (SHIM) scores at all follow-up intervals were evident, with statistically significant improvements at 3 months and 12 months. The preservation in erectile function was sustained to 12 months in all patients with no ED, mild, moderate, or severe ED. Additionally, no ejaculatory compromise was demonstrated, as measured by the Male Sexual Health Questionnaire for Ejaculatory Dysfunction (MSHQ-EjD) function scores. Slight increases in MSHQ-EjD scores at all intervals were recorded, with a significant increase from baseline at 6 weeks follow-up (10.6 at baseline vs. 12.3 at 6 weeks). Furthermore, ejaculatory bother did not increase following PUL.
Despite some of the limitations in this early study, including small sample size and lack of inclusion criteria for sexual function, the results correlate with a more recent randomized study.1 As shown by McVary et al1, no de-novo, sustained ejaculatory dysfunction or ED has resulted following treatment with PUL. Although SHIM and MSHQ-EjD scores did not vary from sham baseline controls at 3 months, there was an improvement in MSHQ-EjD function scores by 14% at 12 months, in addition to improvements in ability to ejaculate (4%), intensity of ejaculation (23%) and amount of ejaculate (22%). Stratification of patients according to erectile function demonstrated a significant improvement in SHIM scores for patients with severe ED, and continued stability of erectile function in other patients.1
8. Discussion
One of the major benefits of the PUL uncovered from clinical trials is its lack of negative effect on both ejaculatory and erectile function. This is something that has not been observed with any other treatment for LUTS due to BPH to this point in time.
When we consider management by watchful waiting, the relationship between LUTS due to BPH and ED should be considered. This relationship is well established where ED is shown to be more prevalent with increasing levels of LUTS independent of age.10 This perhaps provides some rationale as to why improvement of sexual dysfunction has been observed in a number of men undergoing treatment for their LUTS. It could also be argued that the nontreatment of LUTS, without specific treatment of ED, could be associated with prolongation and deterioration of ED.
The two principal forms of drug treatment, α-blockers and 5ARIs, are associated with ejaculatory dysfunction and ED, respectively, and these pose material risks for men concerned about maintaining sexual function. 5ARIs are also associated with a reduction in libido. Minimally invasive ablative treatments such as transurethral needle ablation of the prostate and transurethral microwave thermotherapy are also associated sexual dysfunction adverse events. Cavitating surgery such as TURP and laser prostatectomy are well known to be associated with ejaculatory dysfunction in particular, although their association with ED is currently subject to conjecture.
Given the possibility of measurable sexual dysfunction with essentially all treatment options for BPH-associated LUTS, men who are especially concerned about this risk may be considered candidates for PUL.
The principle concern about PUL is the lack of data to support its long-term benefit. It cannot be realistically anticipated that long-term efficacy of a mechanically based treatment will match that of cavitating surgery. It is well known that men with a larger baseline prostate volume will be more likely to experience clinical BPH progression and this may well be observed over time. It could be argued that men with smaller prostates will be less likely to have subsequent prostate growth and may well represent the cases where long-term efficacy can be recorded. There are currently few data on effect of retreatment with further PUL or conventional cavitating surgical treatment. Data are also awaited on comparison between the current PUL and TURP trials.
Despite the lack of available data on the long-term efficacy of PUL, there appears to be a place for bladder outlet treatment in men who do not want long-term medical therapy, with the associated side-effect profile. Equally, some men may feel that their symptoms are not severe enough to warrant formal endoscopic cavitation type (TURP, laser) surgery, again with the associated side effects. There might be a place for men who desire treatment for symptoms but opt out of the two mentioned above. Urolift with its day surgery appeal, may be an attractive option for men who could limit their time off work, and not be troubled with the side effects of current conventional surgery. Documented side-effects of Urolift seem even less bothersome than medical therapy and may well appeal to men who will decide what they want to achieve, and what they want to preserve (i.e., sexual function). Being able to have treatment with local anesthetic avoids the added cost and inconvenience associated with the current conventional endoscopic therapies.
The analogy of the smartphone versus the tablet versus the personal computer, is one often used to make the point that there could be an in-between option. Most people were not aware of how the iPad-style tablets would fit into daily computing until it became clear with experience. Before then, the smartphone and personal computer/notebook seemed adequate. Perhaps, the Urolift too, fits somewhere between medical and current endoscopic surgery, creating an option, because of the paucity of potential side effects. It would ideally suit a sexually active man with bothersome bladder outlet obstruction, who did not want to take daily medication but was not ready for TURP, or laser surgery. It has a role as an intermediate-term therapy.
9. Conclusion
The prostatic urethral lift procedure represents a promising avenue for the treatment of BPH-associated LUTS. In the current therapeutic milieu of existing BPH treatments, PUL exists as an effective and minimally invasive alternative to pharmacological treatment and invasive surgical treatment, creating balance between provision of symptomatic relief of LUTS and minimization of adverse events.
Conflicts of interest
P.C. and H.W. have a financial interest in Neotract. P.C., P.R., and H.W. have been clinical trial investigators for Neotract. C.G. has no conflicts to report.
References
- 1.McVary K.T., Gange S.N., Shore N.D. Treatment of LUTS secondary to BPH while preserving sexual function: randomized controlled study of prostatic urethral lift. J Sex Med. 2014;11:279–287. doi: 10.1111/jsm.12333. [DOI] [PubMed] [Google Scholar]
- 2.Chin P.T., Bolton D.M., Jack G. Prostatic urethral lift: two-year results after treatment for lower urinary tract symptoms secondary to benign prostatic hyperplasia. Urology. 2012;79:5–11. doi: 10.1016/j.urology.2011.10.021. [DOI] [PubMed] [Google Scholar]
- 3.Woo H.H., Chin P.T., McNicholas T.A. Safety and feasibility of the prostatic urethral lift: a novel, minimally invasive treatment for lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH) BJU Int. 2011;108:82–88. doi: 10.1111/j.1464-410X.2011.10342.x. [DOI] [PubMed] [Google Scholar]
- 4.Cantwell A.L., Bogache W.K., Richardson S.F. Multicentre prospective crossover study of the “prostatic urethral lift” for the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia. BJU Int. 2014;113:615–622. doi: 10.1111/bju.12540. [DOI] [PubMed] [Google Scholar]
- 5.Roehrborn C.G., Gange S.N., Shore N.D. The prostatic urethral lift for the treatment of lower urinary tract symptoms associated with prostate enlargement due to benign prostatic hyperplasia: The L.I.F.T. Study. J Urol. 2013;190:2161–2167. doi: 10.1016/j.juro.2013.05.116. [DOI] [PubMed] [Google Scholar]
- 6.Roehrborn C.G., Rukstalis D.B., Winston-Salem N.C. Two year durability of the prostatic urethral lift: multi-center prospective study. J Urol. 2014;191:e792. 20. [Google Scholar]
- 7.McNicholas T.A., Woo H.H., Chin P.T. Minimally invasive prostatic urethral lift: surgical technique and multinational experience. Eur Urol. 2013;64:292–299. doi: 10.1016/j.eururo.2013.01.008. [DOI] [PubMed] [Google Scholar]
- 8.Shore N., Freedman S., Gange S. Prospective multi-center study elucidating patient experience after prostatic urethral lift. Can J Urol. 2014;21:7094–7101. [PubMed] [Google Scholar]
- 9.Woo H.H., Bolton D.M., Laborde E. Preservation of sexual function with the prostatic urethral lift: a novel treatment for lower urinary tract symptoms secondary to benign prostatic hyperplasia. J Sex Med. 2012;9:568–575. doi: 10.1111/j.1743-6109.2011.02568.x. [DOI] [PubMed] [Google Scholar]
- 10.Rosen R.C., Wei J.T., Althof S.E., Seftel A.D., Miner M., Perelman M.A. Association of sexual dysfunction with lower urinary tract symptoms of BPH and BPH medical therapies: results from the BPH Registry. Urology. 2009;73:562–566. doi: 10.1016/j.urology.2008.05.034. [DOI] [PubMed] [Google Scholar]