

Abstract
Context:
Roller massagers are used as a recovery and rehabilitative tool to initiate muscle relaxation and improve range of motion (ROM) and muscular performance. However, research demonstrating such effects is lacking.
Objective:
To determine the effects of applying a roller massager for 20 and 60 seconds on knee-joint ROM and dynamic muscular performance.
Design:
Randomized controlled clinical trial.
Setting:
University laboratory.
Patients or Other Participants:
Ten recreationally active men (age = 26.6 ± 5.2 years, height = 175.3 ± 4.3 cm, mass = 84.4 ± 8.8 kg).
Intervention(s):
Participants performed 3 randomized experimental conditions separated by 24 to 48 hours. In condition 1 (5 repetitions of 20 seconds) and condition 2 (5 repetitions of 60 seconds), they applied a roller massager to the quadriceps muscles. Condition 3 served as a control condition in which participants sat quietly.
Main Outcome Measure(s):
Visual analog pain scale, electromyography (EMG) of the vastus lateralis (VL) and biceps femoris during roller massage and lunge, and knee-joint ROM.
Results:
We found no differences in pain between the 20-second and 60-second roller-massager conditions. During 60 seconds of roller massage, pain was 13.5% (5.7 ± 0.70) and 20.6% (6.2 ± 0.70) greater at 40 seconds and 60 seconds, respectively, than at 20 seconds (P < .05). During roller massage, VL and biceps femoris root mean square (RMS) EMG was 8% and 7%, respectively, of RMS EMG recorded during maximal voluntary isometric contraction. Knee-joint ROM was 10% and 16% greater in the 20-second and 60-second roller-massager conditions, respectively, than the control condition (P < .05). Finally, average lunge VL RMS EMG decreased as roller-massage time increased (P < .05).
Conclusions:
Roller massage was painful and induced muscle activity, but it increased knee-joint ROM and neuromuscular efficiency during a lunge.
Key Words: electromyography, pain, muscle activation, flexibility, stretch
Key Points
A roller massager applied to the quadriceps at a load equal to 25% of body mass was moderately painful and induced minor contractions.
The combination of active contractions and 20 to 60 seconds of roller massage improved knee-joint range of motion and reduced vastus lateralis electromyographic activity during a lunge.
Roller massage could be used to increase range of motion during a warm-up or as a complement to stretching during flexibility training sessions.
Many researchers have studied how stretching affects range of motion (ROM) and performance; in general, their results showed increased ROM and impairments in subsequent performance.1,2 Recently introduced alternative devices to stretching include the foam roller and roller massager. The use of these devices has produced increases in ROM.3,4 Authors of 2 studies examined how a foam roller affects flexibility.3,5 MacDonald et al3 reported 12.7% and 10.3% increases in knee-joint ROM at 2 minutes and 10 minutes, respectively, after two 1-minute bouts of foam rolling. MacDonald et al5 found that quadriceps ROM was 11% and 9% greater at 48 hours and 72 hours, respectively, and hamstrings ROM was 3% greater at 72 hours after treating exercise-induced muscle damage (EIMD) with a foam roller than with no rolling.5 In the only published study in which roller massagers were examined, Sullivan et al4 demonstrated an overall 4.3% increase in sit-and-reach ROM with 5 and 10 seconds of roller-massager application. They found a trend for 10 seconds of roller massager to increase ROM more than did 5 seconds (P = .07). Contrary to most static-stretching studies involving prolonged durations (>90 seconds per muscle group1,2), authors of all 3 studies reported either no subsequent reduction in voluntary force or activation or a lesser degree of impairment after EIMD.
Given that prolonged static stretching tends to produce subsequent deficits,1,2 researchers need to investigate whether prolonged applications of a roller massager negatively affect subsequent performance and increase ROM to a greater extent than did short durations. Furthermore, Sullivan et al4 studied the subsequent effects on isometric contractile properties. Therefore, it would be important to investigate the effects of roller massage on dynamic, functional movements. Whereas MacDonald et al5 demonstrated decreased EIMD discomfort with the use of a foam roller, no one has investigated the extent of discomfort or pain when using these rolling devices on a healthy muscle. Irrespective of its effectiveness, the extent of pain or discomfort associated with different durations of roller massaging may affect the use of the device by the general public. Therefore, the purpose of our study was to compare the effects of multiple repetitions of 20 and 60 seconds of roller-massager and control conditions on ROM, pain, and electromyography (EMG) of the quadriceps and hamstrings while rolling and when performing a dynamic movement (lunge action). Based on previous studies of foam rolling and roller massage, we hypothesized that a greater duration of roller massage would increase ROM and muscle discomfort without adversely affecting dynamic functional performance.
METHODS
Experimental Design
We used a repeated-measures pretest-posttest study design. All participants performed 3 randomized experimental conditions that were separated by 24 to 48 hours. In condition 1, participants applied a roller massager (Thera-Band; The Hygenic Corporation, Akron, OH) to the quadriceps muscles for 5 repetitions of 20 seconds; in condition 2, the roller massager was applied for 5 repetitions of 60 seconds. Condition 3 served as a control in which participants sat quietly for the average time that it took to complete conditions 1 and 2. Each condition was preceded by a warm-up on a Monark cycle ergometer (Monark Exercise AB, Vansbro, Sweden) at an intensity of 70 revolutions per minute and 1 kp for 3 minutes. Participants then performed knee-extension and knee-flexion maximal voluntary isometric contractions (MVICs) for EMG measurement before each condition. The dependent variables measured after the MVICs were quadriceps ROM and dynamic lunge EMG. During the roller-massager conditions, quadriceps and hamstrings EMG and visual analogue scale (VAS-10) pain scores were measured.
Participants
Ten recreationally active men (age = 26.6 ± 5.2 years, height = 175.3 ± 4.3 cm, mass = 84.4 ± 8.8 kg) participated. Recreationally active was defined as exercising approximately 3 times each week. No participant had sustained a neurologic or skeletal muscle injury for at least 1 year. Participants were instructed to refrain from smoking, drinking alcohol, or exercising for at least 6 hours before testing and to refrain from consuming food or caffeinated beverages for at least 2 hours before testing. All participants provided written informed consent, and the Memorial University of Newfoundland's Health Research Ethics Authority approved this study.
Roller-Massager Procedure
Participants were given a brief introduction to the roller-massager procedure. The roller massager consists of a hard rubber material that is 24 cm long and 14 cm in circumference and has low-amplitude, longitudinal grooves surrounding a plastic cylinder (Figure 1A). Its ridged design allows for both superficial and deep-tissue massage when it is rolled over the muscle. A constant-pressure rolling apparatus (Technical Services, Memorial University of Newfoundland, St John's, Newfoundland and Labrador, Canada) was constructed to ensure consistent pressure and frequency of rolling,4 eliminating the variations that would be typical if each participant applied the roller action to the limb. Weight plates were added to the vertical poles until the load on the apparatus reached 25% of body mass. We used this percentage because it would place a pressure on the quadriceps muscles that would not be too uncomfortable and painful for the participants. Participants sat upright and placed the entire dominant limb in the apparatus (Figure 1B). They initiated each roll from the distal portion of the quadriceps, starting from just superior to the patella, and ended each roll at the proximal portion of the quadriceps, approximately 3 to 5 cm below the anterior-superior iliac spine, and returned to the distal portion. Participants were instructed to roll back and forth over the length of the muscle in a continuous motion at a cadence of 30 beats per minute on a metronome (Franz Manufacturing Company, Inc, East Haven, CT). This pace allowed 1 full cycle to be completed in 4 seconds (2 seconds from distal to proximal and 2 seconds from proximal to distal). A 60-second rest period was given after each repetition in each condition. The roller massager was applied to the quadriceps for 5 repetitions of 20 seconds (100 seconds total) in condition 1 and 5 repetitions of 60 seconds (300 seconds total) in condition 2. During the control condition, the roller massager was not applied.
Figure 1.

A, Roller massager. B, Constant-pressure rolling apparatus.
Electromyography
Skin preparation for all electrodes included hair removal with reusable razors, dead epithelial cell removal with abrasive sandpaper, and cleansing with an isopropyl alcohol swab. Indelible ink outlines were traced around the surface electrodes to ensure accurate repeated electrode placement in trials. Bipolar surface EMG electrodes were used to measure all EMG signals. Two disc-shaped surface EMG recording electrodes that were 10 mm in diameter (Meditrace Pellet Ag/AgCl electrodes; Graphic Controls Ltd, Buffalo, NY) were placed 2 cm apart on the vastus lateralis (VL) and biceps femoris (BF) muscle bellies of the dominant limb, with a ground electrode placed on the fibular head. We applied tape and leads to the electrodes to ensure optimal surface contact throughout testing. All electromyographic activity was sampled at 2000 Hz with a Blackman 61-dB bandpass filter (Biopac Systems Inc, Holliston, MA) between 10 and 500 Hz; amplified with a bipolar differential amplifier that had an input impedance of 2 MΩ, common mode rejection ratio of 110 dB/min (50–60 Hz), and gain of 1000; converted using a 12-bit analog-to-digital converter; and stored on a personal computer (Inspiron 6000; Dell Computer, Round Rock, TX) for further analysis. A commercially available software program (AcqKnowledge 4.1; Biopac Systems Inc) was used to analyze the digitally converted analog data.
Participants performed one 4-second MVIC for the knee extensors and knee flexors to determine maximal EMG levels for the VL and BF muscles. We measured VL and BF EMG during each MVIC so that EMG activity during the lunge and roller-massager application could be normalized to MVIC EMG for each respective muscle. For both the knee-extension and knee-flexion MVICs, participants were instructed to contract as hard and as fast as possible and were given strong oral encouragement.
Knee-Extension MVIC
Participants were seated in a specially designed chair (Technical Services, Memorial University of Newfoundland) with the hips secured at 90°. Bilateral shoulder straps linked with waist and groin straps ensured minimal body translation. A foam-padded strap was placed around the right leg at the ankle. The participants performed the contraction by contracting the limb against the strap. A high-tension wire secured the strap, and isometric force was measured with a Wheatstone bridge configuration strain gauge (Omega Engineering Inc, Stamford, CT). Differential voltage from the strain gauge was amplified, converted using an analog-to-digital converter (model DA 100 MP100WSW; Biopac Systems Inc), and monitored on a computer. We calculated peak isometric force from the knee-extension MVIC and analyzed the root mean square (RMS) EMG of the VL over 1 second after the peak MVIC.
Knee-Flexion MVIC
Participants stood with their back toward an immovable object. They performed the contraction by pushing their right heel against the immovable object. We measured RMS EMG of the BF from 2 to 3 seconds during the 4-second MVIC.
Criterion Variables
The VAS-10 for Pain
We used the VAS-10 scale to measure pain at the end of condition 1 (at 20 seconds) and at 20, 40, and 60 seconds during condition 2.
Roller-Massager EMG
To measure the amount of muscle activation during roller-massager application, mean RMS EMG of the VL and BF was analyzed over a burst of electromyographic activity, which lasted approximately 1 second, near the beginning, middle, and end of each 20-second or 60-second roll. The EMG was bandpass filtered between 10 and 500 Hz.
Knee-Joint ROM
The details of the knee-joint ROM procedure used in our study have been reported elsewhere.3,5 Briefly, participants were placed in a kneeling lunge position with the tibia of the nondominant limb perpendicular to the floor. Participants maintained an upright position and increased their lunge-stride length until they experienced discomfort in the contralateral hip. The angle at which the hip was positioned was recorded, and this angle was used for all subsequent ROM measurements during each experimental condition. This process was repeated in all experimental conditions. After measuring the hip angle, we measured and recorded the initial knee angle with a goniometer (ProHealthcare Products, Lehi, UT), using the lateral malleolus, the lateral epicondyle, and the center of the VL as landmarks. We restrained participants across the chest to avoid changes in hip flexion. They were instructed to brace their abdominal muscles to ensure maintenance of trunk posture. We passively flexed the dominant knee until either the point of discomfort or the heel made contact with the gluteal region. The change in the angle at the knee was recorded as a measurement of quadriceps ROM.
Lunge EMG
Before the first session, participants performed a lunge with their dominant limb stepping forward. They were instructed to attempt to flex their dominant knee to approximately 90° on landing. The lunge length was recorded and used for each subsequent testing day. The mean RMS EMG signals of the VL and BF were analyzed via visual inspection of EMG for 4 phases during the lunge: (1) initiation, (2) toe-off and heel strike, (3) isometric hold, and (4) push-off. The mean RMS EMG was measured for each phase and normalized to the RMS EMG during MVIC. Each phase lasted approximately 1 second except the isometric phase, which was held for 2 seconds, and a metronome facilitated all lunge timing. Two lunge trials were completed each day: 1 immediately precondition and 1 immediately postcondition. The VL neuromuscular efficiency, which was defined as a decrease in muscle EMG for the same given task, was also determined during the lunge.
Data Analysis
To determine the effects of roller-massager application on dependent variables, we performed a 1-way analysis of variance (ANOVA) with repeated measures for all dependent variables recorded in the precondition and postcondition tests. The factor was condition (roller-massager application for 20 seconds, 60 seconds, and control). To determine the effects of roller-massager application on pain, a 3-way ANOVA was calculated for the VAS-10 pain scale (2 × 5 × 3). Factors were condition (roller-massager application for 20 seconds or 60 seconds), repetition number (1, 2, 3, 4, and 5), and time (20, 40, and 60 seconds). To determine the activation level for each muscle during roller-massager application, we performed a 3-way ANOVA (2 × 5 × 3). Factors were condition (roller-massager application for 20 seconds or 60 seconds), repetition (1, 2, 3, 4, and 5), and time (20, 40, and 60 seconds). To determine the effects of roller-massager application on knee-joint ROM, we performed a 1-way ANOVA with repeated measures. To determine the effects of roller-massager application on lunge EMG, a 2-way ANOVA (3 × 4) with repeated measures was performed on the RMS EMG for each muscle during the lunge. Factors were condition (roller-massager application for 20 seconds, 60 seconds, and control) and lunge phase (initiation, toe-off and heel strike, isometric hold, and push-off). We considered F ratios to be different at an α level of .05. If we found main effects, we used a 2-way Bonferroni (Dunn) procedure to identify the interactions. Descriptive statistics in the text include percentages and means ± standard deviations. In the Figures, descriptive statistics are presented as means ± standard errors. We used SPSS (version 17.0; SPSS Inc, Chicago, IL) to analyze the data.
RESULTS
Pain
Roller massage caused moderate pain in both the 20-second (3.6 ± 0.70) and 60-second (4.28 ± 0.55) conditions. We found no main effects for pain with the 20-second (P = .70) and 60-second (P = .80) roller-massager conditions. However, we found an interaction, as pain was 13.5% (5.7 ± 0.70; P < .05) and 20.6% (6.2 ± 0.70; P < .05) greater at 40 and 60 seconds, respectively, than at 20 seconds (5.0 ± 0.80). We observed no difference in pain for each of the 5 repetitions of rolls during the 20-second (P = .80) or 60-second (P = .90) roller-massager conditions.
Muscle Activation
During roller massage, average VL and BF RMS EMG was 8% and 7%, respectively, of RMS EMG recorded during knee-extension and knee-flexion MVICs (Figure 2). We found no main effects for condition on VL RMS EMG (P = .60).
Figure 2.

A, Raw data illustrate electromyographic activity of the vastus lateralis and biceps femoris during roller-massager application. B, Normalized root mean square electromyography of the vastus lateralis and biceps femoris during each roll.
A main effect for condition demonstrated that BF RMS EMG was approximately 110% higher in the 60-second condition than in the 20-second condition (P < .05).
Knee-Joint ROM
A 1-way ANOVA with repeated measures showed an effect for condition on knee-joint ROM (P < .05). Post hoc tests showed that knee-joint ROM was 10% (P < .05) and 16% (P < .05) higher in the 20-second and 60-second conditions, respectively, than in the control condition. We noted a trend for the 60-second roller-massager application to increase ROM to a greater extent than the 20-second roller-massager application (P = .08).
Electromyographic Activity During a Lunge
A 2-way ANOVA with repeated measures showed an effect for condition on VL RMS EMG (P < .05). Post hoc tests showed that VL RMS EMG was 3% (P < .05) and 7% (P < .05) less in the 20-second and 60-second conditions, respectively, than in the control condition. Furthermore, VL RMS EMG was approximately 4% less in the 60-second condition than in the 20-second condition (P < .05). The 2-way ANOVA also showed differences between VL RMS EMG and BF RMS EMG in the control and 20-second conditions of approximately 6% (P < .01) and 2.5% (P < .01), respectively (Figure 3).
Figure 3.

A, Raw data illustrate electromyographic activity of the vastus lateralis and biceps femoris during the lunge. The lunge was divided into 4 phases as outlined. B, Total normalized root mean square electromyography of the vastus lateralis and biceps femoris during the lunge. a Indicates different from control (P < .05). b Indicates difference between muscles (P < .05). Data are presented as means ± standard errors.
A 3-way ANOVA for the quadriceps showed a main effect for group, time, and phase (P < .05). During the push-off phase, VL RMS EMG was approximately 24% (P < .05) and 30% (P < .05) less in the 20-second and 60-second conditions, respectively, than in the control condition (Figure 4).
Figure 4.
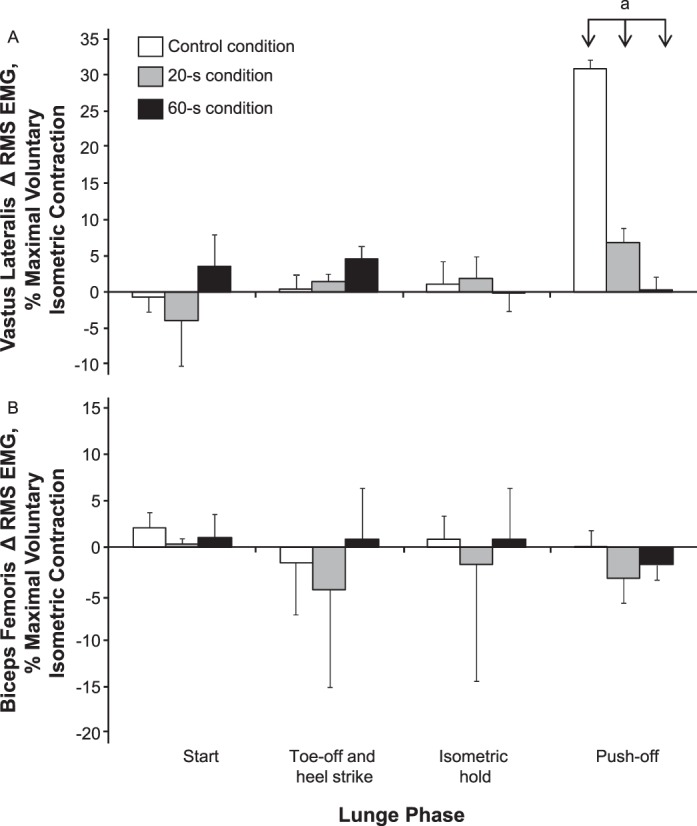
A, Vastus lateralis and B, biceps femoris root mean square (RMS) electromyography (EMG) during each phase of the lunge. a Indicates different from control (P < .05). Data are presented as means ± standard errors.
DISCUSSION
Our most important findings were that the latter stages (40 and 60 seconds) of roller massaging involved higher perceptions of pain than did 20 seconds of roller massaging. Roller massaging was an active muscle process, as the extent of BF and VL activation was 7% to 8% of MVIC, which did not increase as the perception of pain increased. In agreement with our hypothesis, using a roller massage on the quadriceps increased knee-joint ROM 10% and 16% more with the 20-second and 60-second roller-massager conditions, respectively, than in the control condition. Finally, both durations of roller-massager application increased neuromuscular efficiency during the lunge (ie, reduced VL EMG) compared with control, and 60 seconds of roller massaging enhanced muscle efficiency more than 20 seconds of roller massaging did.
The roller massage caused moderate pain during both rolling durations, with 13.5% and 20.6% greater perceived pain at 40 seconds and 60 seconds, respectively, than at 20 seconds. Whereas no other authors have reported pain perception with roller-massager application, MacDonald et al5 observed a similar range of pain perception with a foam roller. Using visual analog scales ranging from 0 to 10, both we (VAS-10 pain) and MacDonald et al5 (BS-11 Numerical Rating Scale) reported similar ranges of perceived pain of approximately 3 to 6 and 2.5 to 7.5, respectively. We are also the first to use either a roller massager or a foam roller to monitor EMG activity during the rolling. On average, participants activated their muscles to 7% to 8% of an MVIC, probably because of the moderate pain perception. The low-intensity contraction may have provided 3 benefits. First, cocontractions were elicited to help protect the muscle from the roller pressure. Cocontracting the muscles in anticipation of or during a potentially discomforting event is a natural response.6,7 Second, the contractions would generate heat from the metabolic reactions. Muscle contractions are inefficient; 60% of the energy is converted to heat.8 Increased heat could contribute to reduced muscle and connective tissue viscoelasticity, thereby enhancing ROM. Third, the low-intensity contractions may have increased ROM through similar mechanisms as contract-relax proprioceptive neuromuscular facilitation (CRPNF) stretching.
The increase in ROM in our study is similar to that reported in a number of studies using static stretching9–12 as well as musculotendinous junction massage13 (11.3% in hip flexion) and deep-stripping massage strokes14 (10.7% in hamstrings). Authors4 of the only published roller-massager study showed an average 4.3% increase in sit-and-reach ROM with 5 and 10 seconds of roller-massager application. The substantially greater increases in ROM with our study (10% to 16%) might be related to the increased roller-application duration (5 and 10 seconds versus 20 and 60 seconds). The acute improvement in ROM in our study is similar to the relative quadriceps ROM increases reported with two 1-minute bouts of foam-roller application (10.3% to 12.7%).3 In our study, the increased duration of roller-massager application (60 seconds) led to a trend toward a greater increase in ROM than did the shorter duration (20 seconds) (P = .08) (Figure 4).
Another possible variable to explain the increased ROM could be the force of the roller massager. Sullivan et al4 applied a constant 13 kg to the hamstrings, whereas we applied an average 21 kg (25% of body mass with an average body mass of 84 kg) to the quadriceps. Furthermore, Sullivan et al4 rolled the hamstrings, whereas we rolled the quadriceps. However, given that MacDonald et al3 reported similar increases in knee-joint ROM after foam rolling the quadriceps, the difference in muscles probably does not play the most important role.
The 2 factors of prolonged rolling duration and greater force may have altered the viscoelasticity and thixotropic properties of the fascia,15 promoting a more gel-like state16 without any impairment to the neuromuscular properties measured in our study. Twomey and Taylor17 indicated that long-term mechanical stress was required to induce a gel-like state, which would permit a greater ROM.18 In addition, greater friction-related heat could have accumulated from the prolonged roller-massage duration and greater applied force. Heat helps to soften and reduce the viscosity of tissue.16 Furthermore, the roller massager may mechanically break apart scar tissue, remobilizing the fascia back to its gel-like state.19
In addition to fascia and muscle changes, neural influences could also be associated with the increase in knee-joint ROM that the roller-massager application induced. The low-intensity contractions during roller massage, as illustrated by VL and BF EMG reaching 7% to 8% of that recorded during MVIC, may have induced increased ROM in a fashion similar to CRPNF stretching. Intensities of CRPNF contraction as low as 20% of MVIC held for 6 seconds were just as effective as maximal contractions for increasing ROM, possibly because of alterations in muscle-spindle length or stretch perception.20 Whereas the contraction intensity was lower during roller-massager application, the amount of time during which the muscles were active was much longer than 6 seconds. The 8% contraction intensity, in addition to the overall duration during which the muscles were active during rolling, may have been enough to induce increased ROM similar to that seen after CRPNF stretching. However, the lowest contraction intensity during CRPNF required to induce increased ROM remains unknown. Vigorous pressure placed on the soft tissue may overload the cutaneous receptors, possibly diminishing the sensation of the stretch endpoint and increasing stretch tolerance.21 The roller massager has been suggested to act as a self-myofascial–release technique similar to massage.4 Massage has been reported to suppress H-reflexes,22–24 thereby decreasing the afferent excitation of the target motor neurons.25 Further research is necessary to determine the precise mechanisms underlying the increased ROM associated with roller massage and foam rolling.
Rather than having no effect on dynamic performance as we hypothesized, the roller massager improved movement efficiency; less VL electromyographic activity was needed to perform the same lunge action after application. The suppression of H-reflexes afferent excitation by massage may be partly responsible for the decreased EMG during a lunge after roller-massager application, but a revealing finding regarding the mechanism underlying this increased efficiency may be related to the overall versus specific changes in VL EMG. Whereas total VL EMG was 3% and 7% less in the 20-second and 60-second conditions, respectively, than in the control condition, during the push-off phase, it was 24% and 30% less in these conditions, respectively, than in the control condition. Given that the statistical interactions did not show any other phase-specific differences (initiation, toe-off and heel strike, isometric hold), we presume that the increased efficiency arose from a more efficient stretch-shortening cycle (SSC). The SSC exercises use accumulated elastic energy during the eccentric phase of the contraction to help augment the concentric phase.26 Behm and Chaouachi1 indicated that increased muscle compliance (less muscle stiffness) can enhance the ability of the musculotendinous unit to store elastic energy over a longer period.27–29 Although the increased compliance associated with static stretching is implicated in the impairment of rapid SSC actions, such as sprinting and hurdle jumps, more prolonged SSC actions can benefit from a more compliant musculotendinous unit.1 For example, Wilson et al30 reported a 5% increase in rebound bench press after 8 weeks of flexibility training. Godges et al31 found that more flexible people had lower energy costs with distance running (longer contact or amortization time than sprinting). Walshe and Wilson32 indicated that participants with stiff tissue were more disadvantaged at higher drop heights than were participants with more compliant tissue. They postulated that the stiffer musculotendinous unit would have a decreased ability to handle the high loads. Because the transition from the eccentric to concentric phases of the lunge involved a 2-second isometric pause, an improved ability to store elastic energy for a longer period with the roller massager would increase the efficiency of the subsequent concentric push-off, resulting in less muscle activation needed to accomplish the task. In accord with this evidence, the 4% greater efficiency with 60 seconds than 20 seconds of roller-massager application would be associated with the 60-second–duration trend toward a greater increase in ROM (greater muscle compliance; 6.4%).
CONCLUSIONS
We demonstrated that applying roller-massage pressure (ie, load) to the quadriceps that was equal to 25% of body mass resulted in a moderately painful roller-massager application, which induced minor contractions (<10% MVIC) of the target muscle. However, the combination of active contractions and 20 to 60 seconds of roller massage improved ROM and muscular efficiency (reduced VL EMG) during a lunge. Given that authors1,2 of 2 recent meta-analyses have demonstrated that static stretching generally causes impairments in subsequent performance, we recommend using a roller massager to increase ROM during a warm-up or as a complement to stretching during flexibility training sessions.
REFERENCES
- 1.Behm DG, Chaouachi A. A review of the acute effects of static and dynamic stretching on performance. Eur J Appl Physiol. 2011;111(11):2633–2651. doi: 10.1007/s00421-011-1879-2. [DOI] [PubMed] [Google Scholar]
- 2.Kay AD, Blazevich AJ. Effect of acute static stretch on maximal muscle performance: a systematic review. Med Sci Sports Exerc. 2012;44(1):154–164. doi: 10.1249/MSS.0b013e318225cb27. [DOI] [PubMed] [Google Scholar]
- 3.MacDonald GZ, Penney MD, Mullaley ME, et al. An acute bout of self-myofascial release increases range of motion without a subsequent decrease in muscle activation or force. J Strength Cond Res. 2013;27(3):812–821. doi: 10.1519/JSC.0b013e31825c2bc1. [DOI] [PubMed] [Google Scholar]
- 4.Sullivan KM, Silvey DB, Button DC, Behm DG. Roller-massager application to the hamstrings increases sit-and-reach range of motion within five to ten seconds without performance impairments. Int J Sports Phys Ther. 2013;8(3):228–236. [PMC free article] [PubMed] [Google Scholar]
- 5.MacDonald GZ, Button DC, Drinkwater EJ, Behm DG. Foam rolling as a recovery tool after an intense bout of physical activity. Med Sci Sports Exerc. 2014;46(1):131–142. doi: 10.1249/MSS.0b013e3182a123db. [DOI] [PubMed] [Google Scholar]
- 6.Chambers AJ, Cham R. Slip-related muscle activation patterns in the stance leg during walking. Gait Posture. 2007;25(4):565–572. doi: 10.1016/j.gaitpost.2006.06.007. [DOI] [PubMed] [Google Scholar]
- 7.Pijnappels M, Bobbert MF, van Dieen JH. EMG modulation in anticipation of a possible trip during walking in young and older adults. J Electromyogr Kinesiol. 2006;16(2):137–143. doi: 10.1016/j.jelekin.2005.06.011. [DOI] [PubMed] [Google Scholar]
- 8.Martini FH, Nath JL. Fundamentals of Anatomy and Physiology. 8th ed. San Francisco, CA: Pearson/Benjamin Cummings; 2009. [Google Scholar]
- 9.Behm DG, Kibele A. Effects of differing intensities of static stretching on jump performance. Eur J Appl Physiol. 2007;101(5):587–594. doi: 10.1007/s00421-007-0533-5. [DOI] [PubMed] [Google Scholar]
- 10.Behm DG, Plewe S, Grage P, et al. Relative static stretch-induced impairments and dynamic stretch-induced enhancements are similar in young and middle-aged men. Appl Physiol Nutr Metab. 2011;36(6):790–797. doi: 10.1139/h11-107. [DOI] [PubMed] [Google Scholar]
- 11.Murphy JR, Di Santo MC, Alkanani T, Behm DG. Aerobic activity before and following short-duration static stretching improves range of motion and performance vs. a traditional warm-up. Appl Physiol Nutr Metab. 2010;35(5):679–690. doi: 10.1139/H10-062. [DOI] [PubMed] [Google Scholar]
- 12.Power K, Behm D, Cahill F, Carroll M, Young W. An acute bout of static stretching: effects on force and jumping performance. Med Sci Sports Exerc. 2004;36(8):1389–1396. doi: 10.1249/01.mss.0000135775.51937.53. [DOI] [PubMed] [Google Scholar]
- 13.Huang SY, Di Santo M, Wadden KP, Cappa DF, Alkanani T, Behm DG. Short-duration massage at the hamstrings musculotendinous junction induces greater range of motion. J Strength Cond Res. 2010;24(7):1917–1924. doi: 10.1519/JSC.0b013e3181e06e0c. [DOI] [PubMed] [Google Scholar]
- 14.McKechnie GJ, Young WB, Behm DG. Acute effects of two massage techniques on ankle joint flexibility and power of the plantar flexors. J Sports Sci Med. 2007;6(4):498–504. [PMC free article] [PubMed] [Google Scholar]
- 15.Paolini J. Review of myofascial release as an effective massage therapy technique. Athl Ther Today. 2009;14(5):30–34. [Google Scholar]
- 16.Schleip R. Facial plasticity: a new neurobiological explanation. Part 1. J Bodyw Mov Ther. 2003;7(1):11–19. [Google Scholar]
- 17.Twomey L, Taylor J. Flexion creep deformation and hysteresis in the lumbar vertebral column. Spine (Phila Pa 1976) 1982;7(2):116–122. doi: 10.1097/00007632-198203000-00005. [DOI] [PubMed] [Google Scholar]
- 18.Barnes MF. The basic science of myofascial release: morphologic change in connective tissue. J Bodyw Mov Ther. 1997;1(4):231–238. [Google Scholar]
- 19.Stone JA. Myofascial release. Athl Ther Today. 2000;5(4):34–35. [Google Scholar]
- 20.Feland JB, Marin HN. Effect of submaximal contraction intensity in contract-relax proprioceptive neuromuscular facilitation stretching. Br J Sports Med. 2004;38(4):E18. doi: 10.1136/bjsm.2003.010967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sayenko DG, Vette AH, Obata H, Alekhina MI, Akai M, Nakazawa K. Differential effects of plantar cutaneous afferent excitation on soleous stretch and H-reflex. Muscle Nerve. 2009;39(6):761–769. doi: 10.1002/mus.21254. [DOI] [PubMed] [Google Scholar]
- 22.Behm DG, Peach A, Maddigan M, et al. Massage and stretching reduce spinal reflex excitability without affecting twitch contractile properties. J Electromyogr Kinesiol. 2013;23(5):1215–1221. doi: 10.1016/j.jelekin.2013.05.002. [DOI] [PubMed] [Google Scholar]
- 23.Goldberg J, Sullivan SJ, Seaborne DE. The effect of two intensities of massage on H-reflex amplitude. Phys Ther. 1992;72(6):449–457. doi: 10.1093/ptj/72.6.449. [DOI] [PubMed] [Google Scholar]
- 24.Sullivan SJ, Williams LR, Seaborne DE, Morelli M. Effects of massage on alpha motoneuron excitability. Phys Ther. 1991;71(8):555–560. doi: 10.1093/ptj/71.8.555. [DOI] [PubMed] [Google Scholar]
- 25.Trimble MH, Enoka RM. Mechanisms underlying the training effects associated with neuromuscular electrical stimulation. Phys Ther. 1991;71(4):273–280. doi: 10.1093/ptj/71.4.273. [DOI] [PubMed] [Google Scholar]
- 26.Komi PV, Bosco C. Utilization of stored elastic energy in leg extensor muscles by men and women. Med Sci Sports. 1978;10(4):261–265. [PubMed] [Google Scholar]
- 27.Bosco C, Tihanyi J, Komi PV, Fekete G, Apor P. Store and recoil of elastic energy in slow and fast types of human skeletal muscles. Acta Physiol Scand. 1982;116(4):343–349. doi: 10.1111/j.1748-1716.1982.tb07152.x. [DOI] [PubMed] [Google Scholar]
- 28.Cavagna GA, Dusman B, Margaria R. Positive work done by a previously stretched muscle. J Appl Physiol. 1968;24(1):21–32. doi: 10.1152/jappl.1968.24.1.21. [DOI] [PubMed] [Google Scholar]
- 29.Edman KA, Elzinga G, Noble MI. Enhancement of mechanical performance by stretch during tetanic contractions of vertebrate skeletal muscle fibres. J Physiol. 1978;281:139–155. doi: 10.1113/jphysiol.1978.sp012413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wilson GJ, Elliot BC, Wood GA. Stretch shorten cycle performance enhancement through flexibility training. Med Sci Sports Exerc. 1992;24(1):116–123. [PubMed] [Google Scholar]
- 31.Godges JJ, Macrae H, Longdon C, Tinberg C, Macrae PG. The effects of two stretching procedures on hip range of motion and gait economy. J Orthop Sports Phys Ther. 1989;10(9):350–357. doi: 10.2519/jospt.1989.10.9.350. [DOI] [PubMed] [Google Scholar]
- 32.Walshe AD, Wilson GJ. The influence of musculotendinous stiffness on drop jump performance. Can J Appl Physiol. 1997;22(2):117–132. doi: 10.1139/h97-010. [DOI] [PubMed] [Google Scholar]