

Abstract
Introduction
Severe cardiovascular collapse (CVC) is a life-threatening complication after emergency endotracheal intubation (ETI) in the ICU. Many factors may interact with hemodynamic conditions during ETI, but no study to date has focused on factors associated with severe CVC occurrence. This study assessed the incidence of severe CVC after ETI in the ICU and analyzed the factors predictive of severe CVC.
Methods
This was a secondary analysis of a prospective multicenter study of 1,400 consecutive intubations at 42 ICUs. The incidence of severe CVC was assessed in patients who were hemodynamically stable (mean arterial blood pressure >65 mmHg without vasoactive drugs) before intubation, and the factors predictive of severe CVC were determined by multivariate analysis based on patient and procedure characteristics.
Results
Severe CVC occurred following 264 of 885 (29.8 %) intubation procedures. A two-step multivariate analysis showed that independent risk factors for CVC included simple acute physiologic score II regardless of age (odds ratio (OR) 1.02, p < 0.001), age 60–75 years (OR 1.96, p < 0.002 versus <60 years) and >75 years (OR 2.81, p < 0.001 versus <60 years), acute respiratory failure as a reason for intubation (OR 1.51, p = 0.04), first intubation in the ICU (OR 1.61, p = 0.02), noninvasive ventilation as a preoxygenation method (OR 1.54, p = 0.03) and inspired oxygen concentration >70 % after intubation (OR 1.91, p = 0.001). Comatose patients who required ETI were less likely to develop CVC during intubation (OR 0.48, p = 0.004).
Conclusions
CVC is a frequent complication, especially in old and severely ill patients intubated for acute respiratory failure in the ICU. Specific bundles to prevent CVC may reduce morbidity and mortality related to intubation of these high-risk, critically ill patients.
Trial registration
clinicaltrials.gov NCT01532063; registered 8 February 2012.
Introduction
Severe cardiovascular collapse (CVC) is one of the most frequent, severe life-threatening complications after emergency endotracheal intubation (ETI) in critically ill patients. CVC after ETI is defined by hemodynamic instability (systolic blood pressure ≤65 mmHg recorded at least once and/or ≤90 mmHg for ≥30 minutes despite vascular loading with 500–1000 mL and/or introduction of vasoactive support) [1–4]. ETI in the ICU is most often an unscheduled procedure to treat severe respiratory failure and/or as part of cardiorespiratory resuscitation. Many factors may influence hemodynamic conditions during ETI, including patient medical history and medications, sepsis status, drugs used to induce anesthesia, reason for intubation, and intrathoracic positive pressure related to mechanical ventilation. Risk factors related to serious life-threatening complications include acute respiratory failure and shock as an indication for ETI [1, 5]. To date, however, no study has specifically analyzed factors associated with severe CVC following ETI in the ICU. Early identification of risk factors may enable the use of methods to reduce patient morbidity, including drug treatment, airway management, and additional assistance during intubation procedures [6].
This secondary analysis of a prospective, multiple center observational study performed in 42 ICUs in France (the FRIDAREA study) [7] assessed the incidence of severe CVC after ETI in the ICU as a primary endpoint, and analyzed risk factors predictive of severe CVC in these critically ill patients and evaluated mortality at 28 days as secondary endpoints.
Methods
Study design and population
This was a secondary analysis of patients in the FRIDAREA study database [7]. Briefly, FRIDAREA was a prospective, observational, multicenter study conducted in 42 ICUs to develop a model predictive of difficult intubation (original cohort), and in 18 ICUs to validate the model (validation cohort) [7]. All adult patients consecutively intubated in involved ICUs were included. Exclusion criteria were pregnancy, refusal to participate after information was provided or age <18 years. The primary endpoint was the incidence of severe CVC after ETI in the ICU and secondary endpoints were risk factors predictive of severe CVC in these critically ill patients and evaluated mortality at 28 days.
Ethics and consent
Because of the observational, noninvasive design of this study, the need for written consent was waived. The local ethics committee, the Comité de Protection des Personnes Sud-Mediterranée III, approved the study design (code UF 8819, register 2011-A001122-39).
Data collection
Clinical parameters were prospectively assessed before, during, and after intubation procedures, with an independent observer collecting variables during and after intubation. Data assessed before intubation included: age; body mass index; severity score (modified Simplified Acute Physiologic Score (SAPS) II at admission, with age eliminated to avoid colinearity with age in the multivariate analysis, as described previously [8, 9]); Sequential Organ Failure Assessment (SOFA) score on the day of the procedure; type of admission (medical versus surgical); co-morbidities such as alcoholism, smoking, cirrhosis, and chronic obstructive pulmonary disease (COPD); cause of admission; cause of intubation (coma was defined as a Glasgow score <8); date and hour of intubation (daytime procedures were those performed from 8 am to 7 pm, with all others defined as on-call procedures); intubation during the previous 2 weeks; nature and number of operators; fluid loading; vasopressor use; noninvasive ventilation (NIV); and emergency characteristics of the intubation (with a real emergency defined as the requirement for immediate ETI, relative emergency as ETI required within 1 hour, and deferred emergency as ETI required in >1 hour). Just before intubation preoxygenation and method of preoxygenation (standard versus NIV) were recorded.
Minimal and maximal heart rate, arterial pressure and saturation were measured before intubation, during intubation (between induction of anesthesia and tube insertion) and within 30 minutes after intubation. Drugs used for intubation were recorded. The MACOCHA score, a seven-item (Mallampati score III or IV, obstructive sleep apnea syndrome, reduced mobility of cervical spine, limited mouth opening, severe hypoxia, coma, nonanesthesiologist as operator) predictor of difficult intubation with a cut-off of 3 points [7], was assessed.
Finally, the percentages of patients undergoing capnography (end-tidal CO2 curve) and esophageal intubation; the rates of agitation, aspiration, cardiac arrest, and arrhythmias; ventilation parameters; and 28-day mortality rate were evaluated.
Definition of severe CVC
Arterial blood pressure was monitored continuously in patients carrying an intra-arterial catheter for 5 of 30 minutes after intubation in patients with cuff measurements. Severe CVC was defined as systolic blood pressure ≤65 mmHg recorded at least once and/or ≤90 mmHg lasting ≥30 minutes despite vascular loading with 500–1000 mL crystalloid and/or colloid solutions and/or a requirement for vasoactive support [1–4]. To avoid confounding factors of hemodynamic variability, only patients who were hemodynamically stable before intubation (defined as mean arterial blood pressure >65 mmHg without vasoactive drugs [10, 11]) were included. Therefore, patients intubated for cardiac arrest and shock were secondarily excluded.
Statistical analysis
All statistical analyses were performed using Stata software, version 12 (StataCorp, College Station, Tx, USA). The tests were two-sided, with a type I error set at α = 0.05. Mean and standard deviation (SD) or median and interquartile range were calculated for continuous variables, and number of patients and associated percentages were calculated for categorical parameters. Categorical variables were compared between independent groups using the Chi-squared test or Fisher’s exact test, and continuous variables were compared using Student's t-test or the Mann-Whitney test, with normality verified by the Shapiro-Wilk test and homoscedasticity by the Fisher-Snedecor test. Factors significant in the univariate analysis (p < 0.1 [12, 13]) and parameters deemed clinically relevant [6, 14, 15], such as use of ketamine or etomidate, COPD and fluid challenge >500 mL (adjustment factors), were included in backward and forward stepwise multivariate logistic regression analyses to determine risk factors independently associated with CVC. The interactions between possible predictive factors were also tested. Results were expressed as odds ratios (ORs) and 95 % confidence intervals (CIs). Multivariate analysis consisted of three steps: 1) patient characteristics (first model), 2) intubation procedures in the ICU (second model), and 3) parameters statistically significant in these two models (model). Univariate analyses identified a cut-off of inspired oxygen concentration (FiO2) of 70 % and age in three stages (<60, 60–75 and >75 years) for testing in the multivariate models. The Hosmer-Lemeshow test was used to assess the goodness of fit of the logistic model. A cross-validation process was considered to assess the goodness of fit of the final models obtained. Following these multivariate analyses, a receiver-operating characteristic (ROC) curve associated with the occurrence of CVC (model) was plotted for each proposed model. The statistical power of the final was tested according to works proposed by Tosteson and Demidenko [16, 17].
Results
During the study period, 1,400 intubation procedures were performed in 1,360 patients. After excluding 41 patients who underwent intubation for cardiac arrest, 212 who underwent intubation for shock and 262 who received vasoactive drugs before intubation, 885 intubation procedures were included (Fig. 1).
Fig. 1.

Study flow chart
Severe CVC was observed following 264 of 885 (29.8 %) intubation procedures. The relationships between patient characteristics and the incidence of severe CVC are shown in Table 1. Data on the intubation procedures are detailed in Table 2. Of the 885 intubations, 597 (67 %) were performed due to acute respiratory failure, 241 (27 %) due to coma and 148 (17 %) due to failure of planned extubation. Reasons for the 94 (11 %) other intubations included need for surgical procedures (n = 12, 1.4 %), self-extubation (n = 12, 1.4 %), endoscopy for digestive hemorrhage (n = 29, 3.3 %), uncontrolled agitation (n = 12, 1.4 %), air leak in the balloon probe (n = 4, 0.5 %) and others (n = 25, 2.8 %).
Table 1.
Characteristics of patients
| Total | No collapse | Collapse | p-value | |
|---|---|---|---|---|
| (n = 885) | (n = 621) | (n = 264) | ||
| Age in years, mean ± SD | 58.4 ± 0.6 | 56.0 ± 0.7 | 64.0 ± 0.9 | <0.0001 |
| Male gender, n (%) | 563 (64.6) | 387 (63.4) | 176 (67.4) | 0.28 |
| SAPS II score regardless of age, mean ± SD | 36.8 (16.7) | 35.8 (16.5) | 39.3 (17.1) | 0.006 |
| Surgical admission, n (%) | 271 (30.6) | 195 (31.4) | 76 (28.8) | 0.47 |
| SOFA score, mean ± SD | 5.0 ± 0.1 | 4.8 ± 0.1 | 5.3 ± 0.2 | 0.02 |
| Reason for ICU admission: | ||||
| Acute respiratory failure, n (%) | 422 (48.7) | 260 (41.9) | 162 (61.4) | <0.0001 |
| Postoperative complications, n (%) | 92 (10.4) | 60 (9.7) | 32 (12.1) | 0.28 |
| Brain injury, n (%) | 263 (29.7) | 216 (34.8) | 47 (17.8) | <0.0001 |
| Acute kidney injury, n (%) | 54 (6.1) | 40 (6.4) | 14 (5.3) | 0.65 |
| Trauma, n (%) | 62 (7.0) | 51 (8.2) | 11 (4.2) | 0.03 |
| Past medical history | ||||
| Tobacco, n (%) | 297 (33.6) | 205 (33.0) | 92 (34.9) | 0.64 |
| Cirrhosis, n (%) | 83 (9.4) | 64 (10.3) | 19 (7.2) | 0.17 |
| COPD, n (%) | 153 (17.3) | 95 (15.3) | 58 (22.0) | 0.02 |
| Obesity, n (%) | 163 (18.4) | 114 (18.4) | 49 (18.6) | 0.94 |
| Diabetes, n (%) | 131 (14.8) | 89 (14.3) | 42 (15.9) | 0.55 |
| Reasons for intubation | ||||
| Coma, n (%) | 241 (27.2) | 194 (31.2) | 47 (17.8) | <0.0001 |
| Acute respiratory failure, n (%) | 597 (67.5) | 375 (60.4) | 222 (84.1) | <0.0001 |
| Extubation failure, n (%) | 148 (16.7) | 111 (17.9) | 37 (14.0) | 0.17 |
| Other, n (%) | 94 (10.6) | 83 (13.4) | 11 (4.2) | 0.88 |
COPD chronic obstructive pulmonary disease, SAPS Simplified Acute Physiologic Score, SD standard deviation, SOFA Sequential Organ Failure Assessment
Table 2.
Characteristics of intubation procedures
| Total | No collapse | Collapse | p-value | |
|---|---|---|---|---|
| (n = 885) | (n = 621) | (n = 264) | ||
| First intubation, n (%) | 543 (61.4) | 364 (58.6) | 179 (67.8) | 0.01 |
| Anesthesiologist, n (%) | 580 (65.5) | 415 (66.8) | 165 (62.5) | 0.22 |
| Fluid challenge, n (%) | 336 (38.0) | 229 (36.9) | 107 (40.5) | 0.33 |
| SpO2 before ETI, mean ± SD | 87.72 ± 0.5 | 88.4 ± 0.6 | 86.13 ± 0.8 | 0.03 |
| NIV (out of preoxygenation), n (%) | 324 (36.6) | 185 (29.8) | 139 (52.7) | <0.0001 |
| Drug for induction, n (%) | 863 (97.5) | 605 (97.4) | 258 (97.7) | 0.79 |
| Nesdonal, n (%) | 25 (2.8) | 17 (2.7) | 8 (3.0) | 0.81 |
| Propofol, n (%) | 139 (15.7) | 111 (17.9) | 28 (10.6) | 0.01 |
| Dose mg/kg, mean ± SD | 2.13 ± 1.23 | 2.10 ± 1.23 | 2.27 ± 1.27 | 0.54 |
| Etomidate, n (%) | 421 (47.6) | 286 (46.1) | 135 (51.1) | 0.17 |
| Dose mg/kg, mean ± SD | 0.45 ± .44 | 0.47 ± 0.46 | 0.42 ± 0.41 | 0.37 |
| Ketamine, n (%) | 188 (21.2) | 124 (20.0) | 64 (24.2) | 0.16 |
| Dose mg/kg, mean ± SD | 2.77 ± 1.06 | 2.82 ± 1.10 | 2.66 ± 0.98 | 0.31 |
| Other, n (%) | 39 (4.4) | 24 (3.9) | 15 (5.7) | 0.23 |
| Opioids, n (%) | 74 (8.4) | 53 (8.5) | 21 (8.0) | 0.78 |
| Fentanyl, n (%) | 8 (0.9) | 5 (0.8) | 3 (1.1) | 0.63 |
| Sufentanil, n (%) | 53 (6.0) | 42 (6.8) | 11 (4.2) | 0.14 |
| Remifentanil, n (%) | 9 (1.0) | 6 (1.0) | 3 (1.1) | 0.82 |
| Other, n (%) | 3 (0.3) | 3 (0.48) | 0 (0) | 0.26 |
| NMBA, n (%) | 770 (87.0) | 543 (87.4) | 227 (86.0) | 0.56 |
| Suxamethonium, n (%) | 646 (73.0) | 446 (71.8) | 200 (75.8) | 0.23 |
| Rocuronium, n (%) | 92 (10.4) | 69 (11.1) | 23 (8.7) | 0.29 |
| Other, n (%) | 45 (5.1) | 32 (5.2) | 13 (4.9) | 0.89 |
| MACOCHA score, n (%) | 0.37 | |||
| <3 | 544 (83.9) | 385 (84.8) | 159 (82.0) | |
| ≥3 | 104 (16.1) | 69 (15.2) | 35 (18.0) | |
| Preoxygenation, n (%) | 841 (95.0) | 585 (94.2) | 256 (97.0) | 0.08 |
| Duration of preoxygenation, mean ± SD | 1.23 (0.7) | 1.21 (0.7) | 1.29 (0.7) | 0.11 |
| NIV for preoxygenation, n (%) | 371 (41.9) | 233 (37.5) | 138 (52.3) | < 0.0001 |
| Incident during ETI, n (%) | ||||
| Inhalation, n (%) | 102 (11.5) | 66 (10.6) | 36 (13.6) | 0.20 |
| Cardiac rhythm abnormalities, n (%) | 15 (1.7) | 8 (1.3) | 7 (2.7) | 0.15 |
| Desaturation, n (%) | 177 (20.0) | 101 (16.3) | 76 (28.8) | < 0.0001 |
| Implementation of sedation, n (%) | 802 (90.6) | 554 (89.2) | 248 (93.9) | 0.03 |
| FIO2, mean ± SD | 68.52 ± 0.9 | 65.57 ± 1.1 | 75.11 ± 1.5 | < 0.0001 |
| Tidal volume, mean ± SD | 458.5 ± 2.9 | 459.01 ± 3.4 | 457.35 ± 5.1 | 0.79 |
| PEEP, mean ± SD | 5.76 ± 0.1 | 5.65 ± 0.1 | 6.01 ± 0.1 | 0.02 |
| RM, n (%) | 108 (12.2) | 68 (11.0) | 40 (15.2) | 0.08 |
FiO 2 inspired oxygen concentration, MACOCHA score a seven-item (Mallampati score III or IV, obstructive sleep apnea syndrome, reduced mobility of cervical spine, limited mouth opening, coma, severe hypoxia, nonanesthesiologist as operator) simplified score, NMBA neuromuscular blocking agents, PEEP positive end-expiratory pressure, RM recruitment maneuver, SD standard deviation, SpO 2 oxygen saturation, NIV noninvasive ventilation
Univariate analysis showed that risk factors for CVC included patient age, SAPS II score regardless of age, SOFA score, COPD, acute respiratory failure as a reason for ICU admission and intubation, initial intubation in the ICU, hypoxemia before intubation, NIV before intubation (for ventilator support and/or only for preoxygenation), desaturation during the intubation procedure, FiO2 >70 % after intubation, administration of sedation immediately after intubation and ventilation with positive end-expiratory pressure (PEEP) of 6 cmH2O. Brain injury as a reason for ICU admission, coma as a reason for intubation and propofol (whatever the dosage per kg) to induce anesthesia were identified as protective factors of CVC. The 28-day mortality rate was significantly higher in patients who did than did not experience CVC (30.4 % versus 19.3 %, p = 0.001).
In the first multivariate model, which included patient characteristics, SAPS II regardless of age (OR 1.02, 95 % CI 1.01–1.03, p = 0.005), age 60–75 years (OR 2.07, 95 % CI 1.39–3.10, p < 0.001 versus <60 years) and >75 years (OR 2.77, 95 % CI 1.73–4.43, p < 0.001 versus <60 years), acute respiratory failure as a reason for intubation (OR 1.56, 95 % CI 1.05–2.30, p = 0.03) and initial intubation in the ICU (OR 1.64, 95 % CI 1.12–2.40, p = 0.01) were independent risk factors for CVC, whereas coma as a reason for intubation was a protective factor (OR 0.51, 95 % CI 0.31–0.86, p = 0.01). A history of COPD was not significantly associated with CVC occurrence (OR 1.26, 95 % CI 0.80–1.97, p = 0.31). Brain injury as a reason for ICU admission was not an independent protective factor (OR 0.72, 95 % CI 0.43–1.19, p = 0.20).
In the second model, which included parameters associated with intubation procedures, independent risk factors for severe CVC occurrence were NIV as a preoxygenation method (OR 1.80, 95 % CI 1.24–2.59, p = 0.002) and FiO2 >70 % after intubation (OR 1.84, 95 % CI 1.29–2.61, p = 0.002). Use of ketamine (OR 1.61, 95 % CI 0.86–2.99, p = 0.14), use of etomidate (OR 1.35, 95 % CI 0.78–2.32, p = 0.29), use of propofol (OR 0.69, 95 % CI 0.35–1.37, p = 0.29), administration of sedation immediately after intubation (OR 1.27, 95 % CI 0.67–2.41, p = 0.47), and fluid challenge >500 mL (OR 1.20, 95 % CI 0.78–1.85, p = 0.42) were not significantly associated with CVC occurrence.
The third multivariate analysis showed that independent risk factors for CVC included SAPS II score regardless of age (OR 1.02, 95 % CI 1.01–1.03, p < 0.001), age 60–75 years (OR 1.96, 95 % CI 1.28–2.99, p < 0.002 versus <60 years) and >75 years (OR 2.81, 95 % CI 1.72–4.59, p < 0.001 versus <60 years), acute respiratory failure as a reason for intubation (OR 1.51, 95 % CI 1.01–2.26, p = 0.04), initial intubation in the ICU (OR 1.61, 95 % CI 1.08–2.41, p = 0.02), NIV as preoxygenation method (OR 1.54, 95 % CI 1.04–2.29, p = 0.03) and FiO2 >70 % after intubation (OR 1.91, 95 % CI 1.30–2.80, p = 0.001). Coma as a reason for intubation was independently associated with protection against CVC (OR 0.48, 95 % CI 0.30–0.79, p = 0.004) (Fig. 2).
Fig. 2.
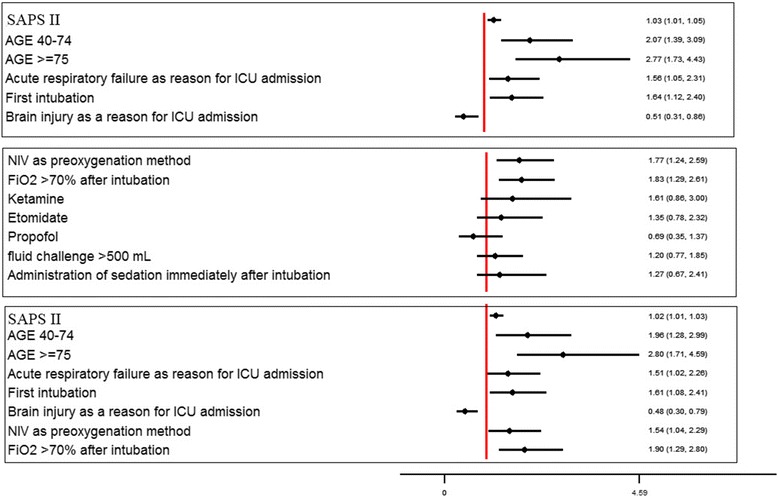
Forrest plot. FiO2 inspired oxygen concentration, NIV noninvasive ventilation, SAPS Simplified Acute Physiologic Score
ROC curves and statistical power
Analysis of ROC curves associated with CVC for each model showed that the area under the curve was more important for the third model (0.71) than for the first (0.68) and second (0.64) models. The statistical power of the final model was greater than 85 %. Except for the parameter “first intubation”, the statistical power was greater than 90 % for each predictive factor presented in the final model.
Discussion
This large cohort analysis showed that CVC was a frequent complication of intubation in the ICU. Patient age, SAPS II score regardless of age, intubation for acute respiratory failure, initial intubation in the ICU and FiO2 >70 % after intubation, but not COPD, were found to be independent risk factors for CVC. Moreover, CVC was associated with a significantly higher 28-day mortality rate.
The CVC rate observed in our study cohort was similar to those reported previously [1], especially in patients without preexisting hypotension before intubation (29 % of 84 patients) [3], or if 15 % were receiving vasopressor before intubation (33 % of 794 patients) [18]. The CVC rate may be dependent on the definition of CVC, particularly the level and duration of hypotension. Based on previous studies, we arbitrarily defined CVC as an arterial systolic blood pressure ≤65 mmHg recorded at least once and/or ≤90 mmHg lasting ≥30 minutes despite vascular loading with 500–1000 mL of crystalloid and/or colloid solutions and/or necessitating introduction of vasoactive drugs [1, 18, 19]. Mortality in the ICU was not related to hypotension after intubation, regardless of its definition and severity [18].
The three models used in our multivariate analyses were built to propose an approach to risk factors for CVC [12]. The first model included patient characteristics, the second model included details of intubation procedures, and the third model included both sets of factors.
Elevated SAPS II score, a good surrogate for illness severity and well correlated with patient mortality, was found to be a risk factor for CVC [20]. Early intubation within the first 24 hours of ICU admission was associated with a high SAPS II score. We did not include age as a component of the SAPS II score to avoid colinearity in the multivariate analyses [8, 9]. A first intubation in ICU was another risk factor. It could follow an uncontrolled evolution of the reason of ICU admission (acute respiratory failure, for example), possibly after NIV failure. In contrast, subsequent intubations may follow extubation failure following the correct treatment of initial shock and multiorgan failure [21].
Acute respiratory failure has been identified as a risk factor for CVC and for complications related to intubation [1, 3, 22, 23]. Desaturation time during apnea associated with intubation may be reduced in ICU patients, especially in hypoxemic patients [24, 25]. Patients with acute respiratory failure have limitations in oxygen transport, alveolar volume and enhanced shunt fraction. Hemoglobin desaturation has been found to increase mortality rates in this population [26, 27]. Preoxygenation with NIV and elevated postintubation FiO2 (>70 %) reflect the severity of respiratory failure.
Although fluid challenge before intubation was not significantly associated with CVC in univariate analysis, it was included in multivariate analysis. Its inclusion was justified by the results of a before/after study comparing the implementation of different treatments and procedures during the intubation procedure [6]. Fluid challenge may be a marker of preload dependence or hemodynamic status and may correspond to a prior severe hemodynamic condition characterized by a potential hypovolemic status before induction. These results are complicated by differences in fluid challenge among the ICUs surveyed. Fluid challenge before intubation is systematic in some ICUs, according to the aforementioned bundle, but is administered only to patients with hypovolemia in other ICUs.
Etomidate and ketamine are anesthetic drugs that have a rapid onset and short half-life, are well tolerated hemodynamically and improve intubation conditions [28, 29]. Increased induction with etomidate or ketamine in the ICU from 35 % to 76 % was associated with a significant reduction in the incidence of severe hypotension [6]. In this observational study, etomidate and ketamine were associated with CVC in univariate analysis but not in multivariate analysis. The lack of correlation between the incidence of CVC and administration of these drugs suggests that etomidate and ketamine were chosen for the most severely ill patients because of their hemodynamic safety profiles [6, 30–32].
A previous study showed that implementation of an intubation management protocol reduced the incidence of intubation-related ICU complications, in particular CVC (15 % versus 27 %) [6]. This protocol included fluid challenge before intubation, preoxygenation with NIV, rapid sequence induction (with ketamine or etomidate, and suxamethonium) and early administration of sedation and vasopressors if needed. Our univariate analysis showed that early administration of sedation was significantly associated with CVC. Its nonsignificance on multivariate analysis suggests that it was probably a confounding factor due to patient severity.
Comatose patients who required ETI were less likely to develop CVC during intubation. Indeed, most comatose patients experience failure of only one organ [33]. Furthermore, laryngoscopy and intubation after rapid sequence induction in these patients often results in hypertension, as most patients intubated after rapid sequence induction show a sympathetic response to laryngeal stimulation, characterized by tachycardia and increases in mean arterial pressure and intracranial pressure [33, 34].
The study had several limitations. First, it was not designed to identify factors protective against CVC. Indeed, patients with hemodynamic instability before ETI were not included in this analysis. The addition of such patients may modify the interpretation of these analyses; however, the rate of life-threatening complications after ETI in patients with septic shock before ETI (about 36 %) was similar to the rate reported in nonselected critically ill patients [35]. These patients must be evaluated in future studies. Several of the factors found to be significant in univariate analysis were not included in the multivariate models, for statistical or clinical reasons. For example, PEEP level was not clinically relevant (5.7 versus 6.0 cmH2O). Another limitation was our inability to evaluate the correlation between the doses of drugs used for ETI (ketamine, etomidate, thiopental and/or propofol) with the degree of hypotension. The specific association between drugs used to facilitate intubation and severe CVC requires further study. COPD and hypercarbic status have been regarded as independently associated with life-threatening hypotension after intubation, with elevated CO2 levels causing generalized vasodilatation [3, 36]. Another limitation is that the presence of an arterial catheter for invasive blood pressure measurement was not fulfilled. It could be a prerequisite and a very important safety measure [6]. Hypercarbia causes sympathetic stimulation, increasing cardiac output secondary to tachycardia [36]. Unfortunately, this study was not designed to record levels of CO2 before and after intubation; only the presence of end-tidal CO2 curve was noted. Thus, we could not determine the role of CO2 variations on CVC occurrence.
Conclusion
This is the first study designed to specifically analyze independent risk factors for severe CVC after ETI in the ICU. Physicians must be aware that tracheal intubation of an old and severe patient for acute respiratory failure leaves them at high risk for severe CVC. Use of specific bundles to prevent CVC may decrease morbidity and mortality related to intubation of these critically ill patients.
Key messages
This study is the first to specifically report independent risk factors for severe cardiovascular collapse (CVC) after endotracheal intubation (ETI) in the intensive care unit. ETI of old and critically ill patients for acute respiratory failure carries a high risk of severe CVC. Use of specific bundles to prevent CVC may decrease morbidity and mortality related to intubation of these critically ill patients.
Acknowledgements
We thank members of the AzuRea Network and members of the FRIDAREA study group.
Abbreviations
- CI
Confidence interval
- COPD
Chronic obstructive pulmonary disease
- CVC
Cardiovascular collapse
- ETI
Endotracheal intubation
- FiO2
Inspired oxygen concentration
- NIV
Noninvasive ventilation
- OR
Odds ratio
- PEEP
Positive end-expiratory pressure
- ROC
Receiver operating characteristic
- SAPS
Simplified Acute Physiologic Score
- SD
Standard deviation
- SOFA
Sequential Organ Failure Assessment
Footnotes
Competing interests
EF reports having consulting fees from General Electric Medical Systems (Helsinki, Finland), Baxter (Deerfield, IL, USA), and Dräger (Lübeck, Germany); lecture fees from Fresenius Kabi (Bad-Hamburg, Germany); and accommodation and travel reimbursement for meetings from Fisher & Paykel Healthcare Ltd (Auckland, New Zealand). SJ reports receiving consulting fees from Dräger, General Electric Medical Systems, and Maquet France (MAQUET Gmbh & Co KG, Rastatt, Germany); lecture fees from Fisher and Paykel Healthcare Ltd, Abbott (North Chicago, IL, USA), and Philips (Amsterdam, The Netherlands); and reimbursement of travel expenses from Pfizer (New York, NY, USA). JMC reports receiving consulting fees from Baxter, Fresenius Kabi, Dräger, and General Electric Medical Systems; payment for expert testimony from Baxter, Fresenius Kabi, and Dräger; lecture fees from General Electric Medical Systems, Baxter, Fresenius Kabi, Dräger, Hospal (Meyzieu, France), Merck Sharp & Dohme (Whitehouse Station, NJ, USA), and LFB Biomedicaments (Les Ulis, France); payment for the development of educational presentations from Dräger, General Electric Medical Systems, Baxter, and Fresenius Kabi; and reimbursement of travel expenses from Bird (Palm Springs, CA, USA), Astute Medical (San Diego, CA, USA), Astellas Pharma (Northbrook, IL, USA), Fresenius Kabi, Baxter, Fisher & Paykel Healthcare Ltd, and Hospal. The other authors declare that they have no competing interests.
Authors’ contributions
SP, ADJ and JD conceived of and designed the study, interpreted the data, and helped to draft the manuscript. SJ and JMC were involved with data acquisition and provided critical revisions to the manuscript. BP designed and performed the statistical analysis and provided critical revisions to the manuscript. EF contributed to interpretation of the data and provided critical revisions to the manuscript. All authors read and approved the final manuscript and agree to be accountable for all aspects of the work.
Contributor Information
Sebastien Perbet, Email: sperbet@chu-clermontferrand.fr.
Audrey De Jong, Email: audreydejong@hotmail.fr.
Julie Delmas, Email: j_delmas@chu-clermontferrand.fr.
Emmanuel Futier, Email: efutier@chu-clermontferrand.fr.
Bruno Pereira, Email: bpereira@chu-clermontferrand.fr.
Samir Jaber, Email: s-jaber@chu-montpellier.fr.
Jean-Michel Constantin, Phone: +33473750476, Email: jmconstantin@chu-clermontferrand.fr.
References
- 1.Jaber S, Amraoui J, Lefrant JY, Arich C, Cohendy R, Landreau L, et al. Clinical practice and risk factors for immediate complications of endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Crit Care Med. 2006;34:2355–2361. doi: 10.1097/01.CCM.0000233879.58720.87. [DOI] [PubMed] [Google Scholar]
- 2.Griesdale DE, Bosma TL, Kurth T, Isac G, Chittock DR. Complications of endotracheal intubation in the critically ill. Intensive Care Med. 2008;34:1835–1842. doi: 10.1007/s00134-008-1205-6. [DOI] [PubMed] [Google Scholar]
- 3.Franklin C, Samuel J, Hu TC. Life-threatening hypotension associated with emergency intubation and the initiation of mechanical ventilation. Am J Emerg Med. 1994;12:425–428. doi: 10.1016/0735-6757(94)90053-1. [DOI] [PubMed] [Google Scholar]
- 4.Schwartz DE, Matthay MA, Cohen NH. Death and other complications of emergency airway management in critically ill adults. A prospective investigation of 297 tracheal intubations. Anesthesiology. 1995;82:367–376. doi: 10.1097/00000542-199502000-00007. [DOI] [PubMed] [Google Scholar]
- 5.De Jong A, Jung B, Jaber S. Intubation in the ICU: we could improve our practice. Crit Care. 2014;18:209. doi: 10.1186/cc13776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jaber S, Jung B, Corne P, Sebbane M, Muller L, Chanques G, et al. An intervention to decrease complications related to endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Intensive Care Med. 2010;36:248–255. doi: 10.1007/s00134-009-1717-8. [DOI] [PubMed] [Google Scholar]
- 7.De Jong A, Molinari N, Terzi N, Mongardon N, Arnal JM, Guitton C, et al. Early identification of patients at risk for difficult intubation in the intensive care unit: development and validation of the MACOCHA score in a multicenter cohort study. Am J Respir Crit Care Med. 2013;187:832–839. doi: 10.1164/rccm.201210-1851OC. [DOI] [PubMed] [Google Scholar]
- 8.Krinsley J, Schultz MJ, Spronk PE, van Braam HF, van der Sluijs JP, Melot C, et al. Mild hypoglycemia is strongly associated with increased intensive care unit length of stay. Ann Intensive Care. 2011;1:49. doi: 10.1186/2110-5820-1-49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Poukkanen M, Koskenkari J, Vaara ST, Pettila V, Karlsson S, Korhonen AM, et al. Variation in the use of renal replacement therapy in patients with septic shock: a substudy of the prospective multicenter observational FINNAKI study. Crit Care. 2014;18:R26. doi: 10.1186/cc13716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Patel BM, Chittock DR, Russell JA, Walley KR. Beneficial effects of short-term vasopressin infusion during severe septic shock. Anesthesiology. 2002;96:576–582. doi: 10.1097/00000542-200203000-00011. [DOI] [PubMed] [Google Scholar]
- 11.Nicolas-Robin A, Barouk JD, Amour J, Coriat P, Riou B, Langeron O. Hydrocortisone supplementation enhances hemodynamic stability in brain-dead patients. Anesthesiology. 2010;112:1204–1210. doi: 10.1097/ALN.0b013e3181d4f34d. [DOI] [PubMed] [Google Scholar]
- 12.Lee K, Koval JJ. Determination of the best significance level in forward logistic regression. Commun Statist Simula. 1997;26:559–575. doi: 10.1080/03610919708813397. [DOI] [Google Scholar]
- 13.Shtatland ES, Cain E, Barton MB. The perils of stepwise logistic regression and how to escape them using information criteria and the Output Delivery System. SUGI’26 Proceedings. Cary, NC: SAS Institute Inc; 2001. p. 222–6.
- 14.Hosmer DW, Lemeshow S. Applied Logistic Regression. New-York: John Wiley & Sons, Inc.; 1989. [Google Scholar]
- 15.Steyerberg EW, Eijkemans MJ, Harrell FE, Jr, Habbema JD. Prognostic modelling with logistic regression analysis: a comparison of selection and estimation methods in small data sets. Stat Med. 2000;19:1059–1079. doi: 10.1002/(SICI)1097-0258(20000430)19:8<1059::AID-SIM412>3.0.CO;2-0. [DOI] [PubMed] [Google Scholar]
- 16.Tosteson TD, Buzas JS, Demidenko E, Karagas M. Power and sample size calculations for generalized regression models with covariate measurement error. Stat Med. 2003;22:1069–1082. doi: 10.1002/sim.1388. [DOI] [PubMed] [Google Scholar]
- 17.Demidenko E. Sample size and optimal design for logistic regression with binary interaction. Stat Med. 2008;27:36–46. doi: 10.1002/sim.2980. [DOI] [PubMed] [Google Scholar]
- 18.Simpson GD, Ross MJ, McKeown DW, Ray DC. Tracheal intubation in the critically ill: a multi-centre national study of practice and complications. Br J Anaesth. 2012;108:792–799. doi: 10.1093/bja/aer504. [DOI] [PubMed] [Google Scholar]
- 19.Auriant I, Reignier J, Pibarot ML, Bachat S, Tenaillon A, Raphael JC. Critical incidents related to invasive mechanical ventilation in the ICU: preliminary descriptive study. Intensive Care Med. 2002;28:452–458. doi: 10.1007/s00134-002-1251-4. [DOI] [PubMed] [Google Scholar]
- 20.Le Gall JR, Neumann A, Hemery F, Bleriot JP, Fulgencio JP, Garrigues B, et al. Mortality prediction using SAPS II: an update for French intensive care units. Crit Care. 2005;9:R645–R652. doi: 10.1186/cc3821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C, et al. Weaning from mechanical ventilation. Eur Respir J. 2007;29:1033–1056. doi: 10.1183/09031936.00010206. [DOI] [PubMed] [Google Scholar]
- 22.Jabre P, Avenel A, Combes X, Kulstad E, Mazariegos I, Bertrand L, et al. Morbidity related to emergency endotracheal intubation - a substudy of the KETAmine SEDation trial. Resuscitation. 2011;82:517–522. doi: 10.1016/j.resuscitation.2011.01.015. [DOI] [PubMed] [Google Scholar]
- 23.Heffner AC, Swords DS, Nussbaum ML, Kline JA, Jones AE. Predictors of the complication of postintubation hypotension during emergency airway management. J Crit Care. 2012;27:587–593. doi: 10.1016/j.jcrc.2012.04.022. [DOI] [PubMed] [Google Scholar]
- 24.Farmery AD, Roe PG. A model to describe the rate of oxyhaemoglobin desaturation during apnoea. Br J Anaesth. 1996;76:284–291. doi: 10.1093/bja/76.2.284. [DOI] [PubMed] [Google Scholar]
- 25.Benumof JL, Dagg R, Benumof R. Critical hemoglobin desaturation will occur before return to an unparalyzed state following 1 mg/kg intravenous succinylcholine. Anesthesiology. 1997;87:979–982. doi: 10.1097/00000542-199710000-00034. [DOI] [PubMed] [Google Scholar]
- 26.Mort TC. Emergency tracheal intubation: complications associated with repeated laryngoscopic attempts. Anesth Analg. 2004;99:607–613. doi: 10.1213/01.ANE.0000122825.04923.15. [DOI] [PubMed] [Google Scholar]
- 27.Davis DP, Dunford JV, Poste JC, Ochs M, Holbrook T, Fortlage D, et al. The impact of hypoxia and hyperventilation on outcome after paramedic rapid sequence intubation of severely head-injured patients. J Trauma. 2004;57:1–8. doi: 10.1097/01.TA.0000135503.71684.C8. [DOI] [PubMed] [Google Scholar]
- 28.Smith DC, Bergen JM, Smithline H, Kirschner R. A trial of etomidate for rapid sequence intubation in the emergency department. J Emerg Med. 2000;18:13–16. doi: 10.1016/S0736-4679(99)00154-7. [DOI] [PubMed] [Google Scholar]
- 29.Walz JM, Zayaruzny M, Heard SO. Airway management in critical illness. Chest. 2007;131:608–620. doi: 10.1378/chest.06-2120. [DOI] [PubMed] [Google Scholar]
- 30.Jackson WL., Jr Should we use etomidate as an induction agent for endotracheal intubation in patients with septic shock? A critical appraisal. Chest. 2005;127:1031–1038. doi: 10.1378/chest.127.3.1031. [DOI] [PubMed] [Google Scholar]
- 31.Bergen JM, Smith DC. A review of etomidate for rapid sequence intubation in the emergency department. J Emerg Med. 1997;15:221–230. doi: 10.1016/S0736-4679(96)00350-2. [DOI] [PubMed] [Google Scholar]
- 32.Jabre P, Combes X, Lapostolle F, Dhaouadi M, Ricard-Hibon A, Vivien B, et al. Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: a multicentre randomised controlled trial. Lancet. 2009;374:293–300. doi: 10.1016/S0140-6736(09)60949-1. [DOI] [PubMed] [Google Scholar]
- 33.Perkins ZB, Wittenberg MD, Nevin D, Lockey DJ, O'Brien B. The relationship between head injury severity and hemodynamic response to tracheal intubation. J Trauma Acute Care Surg. 2013;74:1074–1080. doi: 10.1097/TA.0b013e3182827305. [DOI] [PubMed] [Google Scholar]
- 34.Forbes AM, Dally FG. Acute hypertension during induction of anaesthesia and endotracheal intubation in normotensive man. Br J Anaesth. 1970;42:618–624. doi: 10.1093/bja/42.7.618. [DOI] [PubMed] [Google Scholar]
- 35.Jung B, Clavieras N, Nougaret S, Molinari N, Roquilly A, Cisse M, et al. Effects of etomidate on complications related to intubation and on mortality in septic shock patients treated with hydrocortisone: a propensity score analysis. Crit Care. 2012;16:R224. doi: 10.1186/cc11871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sechzer PH, Egbert LD, Linde HW, Cooper DY, Dripps RD, Price HL. Effect of carbon dioxide inhalation on arterial pressure, ECG and plasma catecholamines and 17-OH corticosteroids in normal man. J Appl Physiol. 1960;15:454–458. doi: 10.1152/jappl.1960.15.3.454. [DOI] [PubMed] [Google Scholar]