

Abstract
Objective
To identify independent predictors of 30-day VTE events requiring treatment after outpatient surgery.
Summary Background Data
An increasing proportion of surgical procedures are performed in the outpatient setting. The incidence of venous thromboembolism (VTE) requiring treatment after outpatient surgery is unknown.
Methods
Prospective observational cohort study using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2005–2009. Adult patients who had outpatient surgery or surgery with subsequent 23-hour observation were included. The main outcome measure was 30-day VTE requiring treatment. Patients were randomly assigned to derivation (N=173,501) or validation (N=85,730) cohorts. Logistic regression examined independent risk factors for 30-day VTE. A weighted risk index was created and applied to the validation cohort. Stratified analyses examined 30-day VTE by risk level.
Results
30-day incidence of VTE for the overall cohort was 0.15%. Independent risk factors included current pregnancy (adjusted odds ratio (OR) 7.80, p=0.044), active cancer (OR 3.66, p=0.005), age 41–59 (OR 1.72, p=0.008), age ≥60 (OR 2.48, p<0.001), body mass index ≥40 (OR 1.81, p=0.015), operative time ≥120 minutes (OR 1.69, p=0.027), arthroscopic surgery (OR 5.16, p<0.001), sapheno-femoral junction surgery (OR 13.20, p<0.001), and venous surgery not involving the great saphenous vein (OR 15.61, p<0.001). The weighted risk index identified a 20-fold variation in 30-day VTE between low (0.06%) and highest risk (1.18%) patients.
Conclusions
30-day VTE risk after outpatient surgery can be quantified using a weighted risk index. The risk index identifies a high-risk subgroup of patients with 30-day VTE rates of 1.18%.
INTRODUCTION
In the past decade, there has been a major shift from inpatient to outpatient surgery, with more than 60% of procedures now being performed on an outpatient basis.1 Outpatient surgery is now common among multiple surgical specialties, including general surgery, surgical oncology, spine surgery, plastic and reconstructive surgery, and orthopedic surgery.2–11
Outpatient surgical management of many disorders has been shown to be safe. However, the outpatient surgical population has known risk factors for peri-operative venous thromboembolism (VTE). These risk factors include advanced age, obesity, active cancer, abdominal insufflation, arthroscopy, and procedures involving extended operative times.12–20
Although VTE has received significant attention in the inpatient surgical population, it has historically been considered a rare event among outpatient surgical patients. However, existing data focused on VTE after outpatient surgery are limited to retrospective single or two-center studies with small sample sizes. The retrospective and self-reporting methodology of these studies results in reported VTE rates of 0.001% to 0.043% that likely underestimate the true event rate.5, 9, 21
The outpatient surgery population is a pre-screened group expected to achieve excellent postoperative outcomes. Historically, medical personnel preferentially selected young, healthy individuals to undergo surgery in this setting. As the outpatient setting continues to increase its proportion of all procedures,1 a large volume of healthy individuals in the VTE denominator may mask a distinct, higher risk group of patients within the overall outpatient surgery population. Despite an increase in the prevalence of VTE risk factors such as advanced age and obesity, survey data continue to demonstrate that only 50% of institutions have existing protocols for day-case VTE prophylaxis. Among institutions with protocols, compliance has been shown to be poor.22
Using a prospectively collected national 30-day outcomes surgery registry, we sought to establish the definitive VTE incidence after outpatient surgery. We hypothesized that VTE rates were higher than previously reported using retrospective and self-reporting techniques. Next, we sought to identify independent risk factors for 30-day VTE events among outpatient surgery patients and to create and validate a novel risk index. We hypothesized that high-risk patients would exhibit event rates warranting further investigation into outpatient surgery VTE prophylaxis.
METHODS
The American College of Surgeons’ National Surgical Quality Improvement Program Participant Use File (ACS-NSQIP PUF) database is a de-identified, publicly available HIPAA-compliant dataset. We obtained Institutional Review Board approval and exemption prior to undertaking this project. Because no care interventions were mandated and no protected health information was available, signed patient consent was waived.
The ACS-NSQIP methodology has previously been described in detail.23, 24 A systematic sampling method is employed. All operations performed under general, spinal, or epidural anesthesia are eligible for NSQIP inclusion. Operations are divided into eight-day cycles. At each NSQIP site, the first 40 operations performed within each eight-day cycle are included in the database. To ensure heterogeneity, cases with high volume and low risk (such as breast lumpectomy or inguinal hernia repair) are capped at five cases per cycle. At present, there are over 250 medical centers that contribute data to ACS-NSQIP PUF.
At each ACS-NSQIP site, a trained clinical nurse is assigned for data review and collection. Each reviewer completes in-depth training on data collection methods. Periodic site reviews are performed to examine inter-rater reliability. Reliability has been shown to be excellent, with less than 1.5% variable disagreement during formal annual audits.23 Sites with inter-rater reliability rates < 95% are excluded from the ACS-NSQIP PUF. Patient demographic and co-morbidity data are collected prospectively. On postoperative day 30, the clinical nurse obtains outcome data through medical record review and examination of institutional death and complications conferences. Additionally, individual patient follow-up is conducted via letter or telephone to identify complications diagnosed and/or treated at other institutions. Patients with incomplete 30-day outcome data are not included in the database.
ACS-NSQIP PUF variables analyzed
All adult patients whose surgery was listed as outpatient and who had a length of stay equal to zero days were included for analysis in the ACS-NSQIP PUF between 2005 and 2009. This included patients who either had same-day surgery or a 23-hour observation after surgery.
Outcome variables
Our primary outcome was a composite VTE variable, including patients with DVT and/or PE. Our secondary outcome was time to DVT or PE. DVT is considered to be a new thrombus within the venous system that is confirmed using an objective imaging method (e.g. duplex ultrasound or computed tomography scan). Patients must be treated with anti-coagulation, inferior vena cava (IVC) filter placement, or IVC ligation. PE is defined as an obstructing thrombus within the pulmonary arterial system. PE requires confirmation using an objective imaging method (e.g. computed tomography scan or arteriogram). Complete definitions of DVT and PE are provided in the Appendix.
Patient variables
Basic demographic data were analyzed including age, sex, and body mass index (BMI). Patient co-morbidities included: congestive heart failure, chronic obstructive pulmonary disease, peripheral vascular disease, diabetes requiring medication (insulin or oral therapy), renal failure requiring dialysis, current smoking, current pregnancy, and prior operation within 30 days. Intra-operative variables of interest included type of anesthesia (general vs. non-general), operative time, and primary Current Procedural Terminology (CPT) coding for the procedure. The primary CPT codes were used to define surgical variables including venous surgery at the sapheno-femoral junction, venous surgery which did not involve the great saphenous vein (GSV) (e.g. procedures which involved the short saphenous vein, perforator veins, or varicose veins), arthroscopic surgery of major joints (shoulder, elbow, hip, knee), and laparoscopic abdominal surgery. Independent study variables are defined in the Appendix.
Statistical analysis
Statistical analysis was performed using the SPSS version 19 statistical package (IBM, Armonk NY). All patients meeting our inclusion criteria were randomly allocated to a derivation (67%) and validation (33%) cohort. Descriptive statistics on the incidence of DVT, PE, and VTE were generated. To determine independent predictors and risk scoring of VTE, a non-parsimonious logistic regression model was developed in the derivation cohort. We used the validation cohort to determine risk index validity. Descriptive statistics were performed on all categorical data elements to look for associations with VTE using either Pearson chi-square or Fisher’s Exact Test where appropriate. For ease of usability in creating a risk index, the continuous data elements age, BMI, and operative time were transformed into categorical data. Age was categorized into <40, 40–59, and ≥ 60 years. BMI was categorized into <25, 25–39, and ≥40 kg/m2. Operative time was categorized into <60, 60–119, and ≥120 minutes.
Collinearity and Pearson correlations were evaluated for all variables (Table 1) entered into the model for the derivation cohort. All variables were entered into the non-parsimonious logistic regression model to determine independent predictors of VTE. Since age, BMI, and operative time were categorized, the lowest category was considered the reference variable in the model. Any variable with a p-value <0.05 was considered an independent predictor of VTE. The predictive value of the derivation model was assessed using a receiver operating characteristic curve area under the curve (ROC AUC). The adjusted odds ratio was evaluated as a measure of effect size for each independent predictor.
Table 1.
Comparison of independent variables between patients who did or did not have VTE events.
| No DVT/PE (N=173,247) | Yes DVT/PE (N=254) | Odds Ratio (95% Confidence Interval) | |
|---|---|---|---|
|
| |||
| Male sex | 72,221 (43%) | 106 (41%) | 0.9 (0.7–1.2) |
|
| |||
| Age | |||
| < 40 years | 41,489 (24%) | 33 (13%) | Reference |
| 40–59 years | 76,472 (44%) | 119 (47%) | 2.0 (1.3–2.9) |
| ≥ 60 years | 55,286 (32%) | 102 (40%) | 2.3 (1.6–3.4) |
|
| |||
| Body mass index | |||
| < 25 kg/m2 | 51,685 (30%) | 64 (25%) | Reference |
| 25–39 kg/m2 | 105,728 (61%) | 162 (64%) | 1.2 (0.9–1.7) |
| ≥ 40 kg/m2 | 12,616 (7.3%) | 26 (10%) | 1.7 (1.1–2.6) |
|
| |||
| Current smoker | 32,831 (19%) | 39 (15%) | 0.8 (0.6–1.1) |
|
| |||
| Pregnancy | 241 (0.1%) | 1 (0.4%) | 2.8 (0.4–20.1) |
|
| |||
| Active cancer | 1,455 (0.8%) | 5 (2.0%) | 2.4 (1.0–5.8) |
|
| |||
| Congestive heart failure | 201 (0.1%) | 1 (0.4%) | 3.4 (0.5–24.4) |
|
| |||
| Chronic obstructive pulmonary disease | 3,492 (2.0%) | 9 (3.5%) | 1.8 (0.9–3.5) |
|
| |||
| Diabetes | 15,063 (8.7%) | 18 (7.1%) | 0.8 (0.5–1.3) |
|
| |||
| Peripheral vascular disease | 1,360 (0.8%) | 2 (0.8%) | 1.0 (0.2–4.0) |
|
| |||
| Preoperative dialysis | 2,473 (1.4%) | 3 (1.2%) | 0.8 (0.2–2.6) |
|
| |||
| Prior operation within 30 days | 2,295 (1.4%) | 5 (2.1%) | 1.5 (0.6–3.5) |
|
| |||
| General anesthesia | 136,899 (79%) | 206 (81%) | 1.1 (0.8–1.6) |
|
| |||
| Arthroscopy procedure | 6,899 (4.0%) | 30 (12%) | 3.2 (2.2–4.7) |
|
| |||
| Abdominal laparoscopic procedure | 37,134 (21%) | 38 (15%) | 0.6 (0.5–0.9) |
|
| |||
| Sapheno-femoral junction procedure | 5,575 (3.2%) | 59 (23%) | 9.1 (6.6–12.2) |
|
| |||
| Non-GSV venous surgery | 2,584 (1.5%) | 30 (12%) | 8.8 (6.0–13.0) |
|
| |||
| Operative time | |||
| < 60 minutes | 109,113 (63%) | 135 (53%) | Reference |
| 60–119 minutes | 53,017 (31%) | 95 (38%) | 1.4 (1.1–1.9) |
| ≥ 120 minutes | 8,717 (5.0%) | 23 (9.1%) | 2.1 (1.4–3.3) |
An unweighted and weighted risk index was calculated for each patient in the derivation cohort. The unweighted risk index assigned one point for each independent predictor as identified in the logistic regression model. To create the weighted risk index, the β coefficient for each independent predictor was divided by the smallest β coefficient of the independent predictors. This value was multiplied by two and rounded to the nearest integer, in a manner previously described by others.25 The unweighted and weighted risk indices were each treated as a continuous independent variable.
The discriminating capacity of unweighted and weighted risk scores for VTE were compared using ROC AUC and stratified analysis. The weighted risk score was subsequently applied to the validation cohort. A stratified analysis examining 30-day VTE incidence by risk score was performed in the validation cohort. These results were compared to stratified analysis performed in the derivation cohort.
RESULTS
Using ACS-NSQIP 2005–2009 data, a total of 259,231 patients had length of stay equal to zero days and an “In/Out-patient Status” variable value of “outpatient”. 173,501 patients were randomly assigned to the derivation cohort. Among derivation cohort patients, the incidence of DVT was 0.12% (209 patients) and PE was 0.038% (66 patients). The incidence of VTE, defined as patients with DVT and/or PE, was 0.15% (254 patients). Among patients with VTE, 8.2% (21 patients) had both DVT and PE. A description of primary procedure type is provided in Table 2.
Table 2.
Derivation cohort categorized by primary procedure type.
| CPT Range of Primary Procedure | Type of Operation by Organ System or Area of Body | Total Patients N=173,501 n (% of total population) | Patients with DVT/PE N=254 n (% incidence within CPT group) |
|---|---|---|---|
| 10000–19999 | Integument | 37,389 (22) | 16 (0.04) |
| 20000–29999 | Musculoskeletal | 15,824 (9.1) | 40 (0.25) |
| 30000–33999 | Respiratory and cardiovascular | 177 (0.1) | 0 (0) |
| 34000–37799 | Arteries and veins | 11,097 (6.4) | 94 (0.85) |
| 38000–39999 | Hemic and lymphatic system, mediastinum, and diaphragm | 1,640 (0.9) | 8 (0.49) |
| 40000–43499 and 69500–69650 | Head and neck, esophagus | 2,529 (1.5) | 0 (0) |
| 43500–43999 | Foregut (stomach, including gastric bypass procedure) | 2,824 (1.6) | 2 (0.07) |
| 44000–46999 | Hindgut (small bowel, large bowel, rectum and anus) | 8,074 (4.7) | 8 (0.10) |
| 47000–48999 | Liver, biliary system, and pancreas | 23,436 (13) | 20 (0.09) |
| 49000–49490 | Miscellaneous peritoneal procedures | 1,530 (0.9) | 4 (0.26) |
| 49491–49999 | Herniorrhaphy | 57,349 (33) | 54 (0.09) |
| 50000–53999 | Urinary system | 2,147 (1.2) | 1 (0.05) |
| 54000–59999 | Genital system (male or female) | 3,398 (2.0) | 2 (0.06) |
| 60000–60999 | Endocrine | 5,161 (3.0) | 5 (0.10) |
| 61000–64999 | Nervous system structures | 926 (0.5) | 0 (0) |
Collinearity diagnostics did not demonstration any condition index above 30. Therefore all variables in Table 1 were entered into the non-parsimonious logistic regression model with the development of VTE as the dependent dichotomous variable. In the derivation cohort, the logistic model included 89.4% (n=155,151) patients with complete data and demonstrated the following as independent predictors (p<0.05) of VTE: arthroscopic surgery, current pregnancy, active cancer, non-GSV venous surgery, sapheno-femoral junction surgery, age 40–59 years, age ≥60 years, BMI ≥40 kg/m2, and operative time ≥120 minutes (Table 3). The Omnibus Tests of Model Coefficients demonstrated a chi-square of 300.774, degrees of freedom of 21 and p<0.001. The Hosmer and Lemeshow test demonstrated a chi-square of 4.334, degrees of freedom of 8 and p=0.826. The ROC AUC was 0.77 ± 0.02 (ROC AUC ± standard error). The median time-to-event for VTE was post-operative day 8 (inter-quartile range post-operative day 5–13).
Table 3.
Independent predictors of VTE from multivariable logistic regression model.
| Risk Factor | Adjusted Odds Ratio (95% Confidence Interval) | p value |
|---|---|---|
|
| ||
| Male gender | 1.09 (0.83–1.42) | 0.530 |
|
| ||
| General anesthesia | 1.38 (0.98–1.95) | 0.062 |
|
| ||
| Arthroscopic surgery | 5.16 (3.33–7.99) | <0.001 |
|
| ||
| Abdominal laparoscopy | 1.32 (0.88–1.96) | 0.177 |
|
| ||
| Current pregnancy | 7.80 (1.06–57.54) | 0.044 |
|
| ||
| Active cancer | 3.66 (1.49–8.99) | 0.005 |
|
| ||
| Congestive heart failure | 3.20 (0.425–24.06) | 0.259 |
|
| ||
| Chronic obstructive pulmonary disease | 1.89 (0.95–3.77) | 0.071 |
|
| ||
| Diabetes requiring medication | 0.69 (0.42–1.13) | 0.143 |
|
| ||
| Peripheral vascular disease | 0.68 (0.17–2.78) | 0.593 |
|
| ||
| Current smoker | 1.01 (0.71–1.43) | 0.965 |
|
| ||
| Renal failure on dialysis | 1.42 (0.44–4.53) | 0.560 |
|
| ||
| Prior operation within 30 days | 1.49 (0.61–3.65) | 0.384 |
|
| ||
| Saphenofemoral junction surgery | 13.20 (9.31–18.73) | <0.001 |
|
| ||
| Non-GSV venous surgery | 15.61 (10.23–23.83) | <0.001 |
|
| ||
| Age | ||
| <40 years | Reference | --- |
| 41–60 years | 1.72 (1.15–2.57) | 0.008 |
| ≥60 years | 2.48 (1.64–3.77) | <0.001 |
|
| ||
| Body mass index | ||
| <25 kg/m2 | Reference | --- |
| 25–39 kg/m2 | 1.15 (0.85–1.57) | 0.358 |
| ≥40 kg/m2 | 1.81 (1.12–2.92) | 0.015 |
|
| ||
| Total operative time | ||
| <60 minutes | Reference | --- |
| 60–119 minutes | 1.21 (0.92–1.60) | 0.175 |
| ≥120 minutes | 1.69 (1.06–2.67) | 0.027 |
The unweighted and weighted risk indices were based on the independent predictors. The unweighted risk index in the derivation cohort demonstrated a ROC AUC of 0.71 ± 0.02. The weighted risk index in the derivation cohort demonstrated a ROC AUC of 0.76 ± 0.02. The 95% confidence intervals between the unweighted and weighted risk index in the derivation cohort did overlap which indicates they were not statistically different. However, when compared to the unweighted index, the weighted risk index provided a clinically relevant improvement in risk discrimination between low, moderate, high, and highest risk patients. The weighted risk-index from the derivation model is shown in Figure 1 and was applied to the validation cohort.
Figure 1.

Weighted risk index for 30-day VTE events after outpatient surgery.
A total of 85,730 patients had been randomly assigned to the validation cohort. The incidence of DVT was 0.10% (87 patients) and PE was 0.043% (37 patients). VTE incidence was 0.13% (112 patients). At each risk level, the observed incidence of VTE was very similar between the derivation and validation sets (Figure 2). The weighted risk index in the validation model demonstrated a ROC AUC of 0.78 ± 0.03 which is nearly identical to the weighted risk index in the derivation model.
Figure 2.
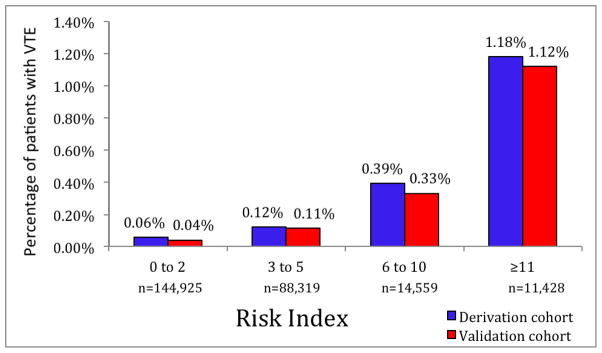
Observed rates of VTE stratified by weighted risk index.
Of 11,428 “highest risk” patients, 97% (11,106 patients) had either sapheno-femoral junction surgery or non-GSV venous surgery. However, the majority of patients in the “highest risk” group also had multiple VTE risk factors: 8,976 patients (78.5%) had two risk factors, 1,727 (15.1%) had three risk factors, and 86 (0.8%) had four risk factors which independently contributed to VTE risk. Only 644 (5.6%) “highest risk” patients had non-GSV venous surgery as an isolated risk factor. Using the weighted risk index, a total of 14,559 patients were classified as “high risk”. Only 9.1% (1,335 patients) of “high risk” patients had some form of venous procedure.
DISCUSSION
Using a multicenter, prospective observational surgical outcomes database of more than 200,000 procedures, we have demonstrated that the 30-day incidence of VTE requiring therapy after outpatient surgery is 0.15% overall and 1.18% among “highest risk” patients. In a logistic regression model, multiple independent predictors of VTE were identified (Table 3). The weighted risk index (Figure 1) explained 78% of the variability in VTE in a distinct validation cohort and allowed discrimination between low and high risk patients. Patients categorized as “highest risk” using our risk index were at almost twenty-fold increased risk for 30-day VTE events when compared to those categorized as “low risk” (1.18% vs. 0.06%, Figure 2). While this novel risk index explains a large proportion of the variability in 30-day VTE risk and is the first risk index targeted toward outpatient surgery patients, it is not a definitive risk prediction tool. Important predictor variables such as personal or family history of VTE, use of hormone replacement therapy, and inflammatory bowel disease, among others, are not tracked as independent variables in ACS-NSQIP. Incorporation of these recognized risk factors into the presented risk index is an important next step for further research.
The scope of ambulatory surgery continues to expand, driven both by economics and patient convenience. Recent systematic reviews confirm that patients previously considered to be high risk can safely undergo outpatient operative procedures. These patients include those with morbid obesity, obstructive sleep apnea, coronary artery disease, diabetes, and advanced age.26, 27 Current ambulatory surgery risk scoring systems have been focused on composite outcomes such as unanticipated hospital admission, ability to be discharged from the post-anesthesia care unit, and mortality.28–31
Fleisher and colleagues have used a representative sample from 5 years of Medicare data (1994–1999) to examine hospital readmission after outpatient surgery.32 Subsequently, Fleisher’s group used Agency for Healthcare Research and Quality data to create and validate a weighted risk assessment model (RAM) to predict hospital readmission after outpatient surgery.33 These studies identified (among others) advanced age, operative time >120 minutes, and malignancy as predictors of hospital readmission. Interestingly, these three factors were also significantly associated with post-operative VTE in our analysis of the ACS-NSQIP PUF data.
VTE has been identified as a major patient safety and quality of care issue by policymakers and payers.34–38 The US Surgeon General’s 2008 Call to Action promoted development of evidence-based guidelines for VTE risk assessment and prophylaxis.34, 35 The Surgical Care Improvement Project (SCIP), a national partnership whose goal is to improve the quality of surgical care through reduction in post-operative complications, has identified VTE prevention and VTE prophylaxis as indicators of quality care.39 These efforts have been focused on the inpatient surgical population and identifying appropriate VTE chemoprophylaxis guidelines.
Our data are the first to demonstrate that even in the pre-screened ambulatory setting, VTE requiring therapy afflicts one in every 84 highest risk patients. Although the vast majority (97%) of these “highest risk” patients had some form of venous procedure, a similar proportion of patients (94%), had risk factors others than the surgical procedure which contributed to their elevated risk level. This underscores the importance of a weighted risk-stratification model as opposed to a risk assessment based upon procedure type alone. Among the 14,559 “high risk” patients, fewer than 10% had a venous procedure performed, yet one out of every 250 patients (0.39%) experienced VTE requiring treatment. These data are in stark contrast to provider and patient expectations that outpatient surgery is a low risk event. As an increasing proportion of procedures are transitioned to the outpatient setting, policymakers, providers, and researchers must focus attention on developing VTE mechanical prophylaxis and chemoprophylaxis guidelines for this unique patient population with challenging follow-up logistics. Currently, fewer than 50% of outpatient centers have guidelines, and even fewer adhere to them.22
Our data provide internists, proceduralists, and anesthesiologists with a method to estimate a proportion of patient’s VTE risk during the pre-operative optimization, intra-operative, and follow-up period. Additionally, the risk index may improve the informed consent process by providing clear, data-driven information to patients.40, 41 However, those who use these data to estimate VTE risk must understand its inherent limitations as discussed below. When estimating perioperative VTE risk, providers must take into account the independent risk factors identified by our study and plausible risk factors that we were unable to evaluate, including personal or family history of VTE, known thrombophilia, use of hormone replacement therapy or oral contraceptive pills, and inflammatory bowel disease, among others.
Prior research has attempted to quantify VTE risk using weighted, point-based risk models. Variations of the widely used Caprini RAM have been validated in a variety of patients and surgery types.42–48 However, no VTE risk model has either been developed or validated specifically for the outpatient surgery population. Using our risk index, the highest-risk outpatients had observed 30-day VTE rates of 1.18%. Interestingly, this rate is approximately twice as high as low-risk inpatients who underwent general, vascular, urologic, or plastic and reconstructive surgery (0.61%-0.70%) and similar to the observed VTE rate among the overall inpatient population (1.44%).42, 46
Limitations
Our results have several limitations, many of which are secondary to inherent limitations of the ACS-NSQIP database. ACS-NSQIP does not track personal or family history of VTE or known thrombophilia as independent variables, although these are recognized contributors to VTE risk.12,13,16,34,35,38 Absence of these variables may account for the 22% of the variability in VTE events not explained by our risk index. Additionally, ACS-NSQIP has no data on administration of VTE prophylaxis. There is no recorded data on use of mechanical prophylaxis, such as elastic compression stockings or sequential compression devices, and/or use of chemoprophylaxis, such as unfractionated heparin or low-molecular weight heparin. Thus, we cannot provide a data-driven discussion of VTE prevention after day-case surgery. Prevention of VTE after outpatient surgery is an important topic for future research.
Our current risk model is not definitive as it could not include many recognized risk factors for VTE. This may explain the 22% of variability in 30-day VTE which was not explained in our model. Inclusion of well-recognized risk factors and prophylaxis measures like personal or family history of VTE, known thrombophilia, and use of mechanical or chemoprophylaxis as independent variables in future versions of ACS-NSQIP will augment the results presented here and allow a more robust, comprehensive risk stratification tool to be created. Additionally, we have reported on the importance of active cancer as an independent risk factor. Surgery for breast cancer is often performed in the outpatient setting. Thus, confounding may be present for our active cancer variable as the NSQIP does not contain data on use of tamoxifen, which is a recognized risk factor for VTE.57 Inclusion of both active cancer and tamoxifen use in future regression models could control for this potential confounding factor. Our model identifies current pregnancy as an independent risk factor for VTE after outpatient surgery. The presumed mechanism of this risk is increased estrogen levels. Oral contraceptive pills (OCP) or hormone replacement therapy (HRT) are additional source of exogenous estrogen. Unfortunately, these could not be included as risk factors in our risk index. Use of OCP or HRT are not tracked as independent variables by ACS-NSQIP.
The ACS-NSQIP database contains 30-day outcomes based on both medical record review and mandatory phone or letter contact. Thus, the reported DVT and PE rates are likely to represent the vast majority of VTE events within 30 days. However, previous studies demonstrate that VTE risk remains elevated for at least 60 to 90 days after surgery.46, 49 Events which occur after post-operative day 30 are not recorded in the ACS-NSQIP database. Thus, our reported rates of DVT and PE likely underestimate the true incidence of post-operative VTE.
Finally, VTE events in ACS-NSQIP most likely represent symptomatic VTE because screening duplex ultrasound is not routinely used in the outpatient setting. One notable exception is great saphenous vein ablation procedures, in which routine post-operative duplex is performed to assess endovenous closure level.50, 51 We controlled for this potential confounder by creating a separate sapheno-femoral junction surgery variable, which was used as an independent variable in our logistic regression model. Rates of post-surgical, asymptomatic VTE have been shown to be high in other patient populations.52–56
CONCLUSION
We present a weighted risk index to assist clinicians in understanding factors that contribute to 30-day VTE risk in the outpatient surgery population. The risk index provides excellent discrimination between high and low risk patients. We have observed that “highest risk” patients undergoing outpatient surgery have an almost twenty-fold increase in risk of VTE requiring therapy and demonstrate a VTE burden similar to the inpatient surgical population. Further research is necessary to 1) create a comprehensive VTE risk model for outpatient surgery patients by combining our risk index with other recognized VTE risk factors and 2) examine the risks, benefits, and cost of mechanical and chemoprophylaxis for patients at high risk for VTE after outpatient surgery
Acknowledgments
Source of Funding:
Dr. Pannucci receives salary support through NIH grant T32 GM-08616.
Appendix
Definitions of selected study covariates
Arthroscopic surgery: Patients whose operative CPT codes included:
CPT 29805–29828 (shoulder arthroscopy); CPT 29830–29838 (elbow arthroscopy); CPT 29860–29863 (hip arthroscopy); CPT 29866–29889 (knee arthroscopy)
Abdominal laparoscopy: Patients whose operative CPT codes included:
CPT 44970, CPT 44979 (laparoscopic appendectomy); CPT 44186, CPT 44187 (laparoscopic jejunostomy for decompression or feeding); CPT 47562–47570 (laparoscopic cholecystectomy); CPT 49650–49659 (laparoscopic hernia surgery); CPT 49320–49329 (diagnostic and other laparoscopy); CPT 58660–58679 (laparoscopy for ovarian surgery); CPT 58541–58554 (laparoscopic hysterectomy)
Current pregnancy: Pregnancy is the process by which a woman carries a developing fetus in her uterus, beginning at conception and ending in birth, miscarriage or abortion. Male patients with pregnancy values of “missing” were re-coded to “not pregnant”.
Sapheno-femoral junction surgery: Includes both endovascular great saphenous vein ablation procedures (radiofrequency ablation, steam ablation, laser ablation, etc) and direct ligation of the sapheno-femoral junction. Includes CPT codes 36475, 36476, 36478, 36479, 37700, 37722, and 37735.
Venous surgery not involving the great saphenous vein: Includes surgical procedures performed on the short saphenous vein or perforator/varicose veins (e.g. open ligation, stab phlebectomy). Includes CPT codes 37500, 37718, 37760, 37765, 37766, 37780, and 37785.
Peripheral vascular disease: includes patients with 1) History of revascularization/amputation for PVD, such as any type of angioplasty (including stent placement) or revascularization procedure for atherosclerotic peripheral vascular disease (PVD) (for example, aorta-femoral, femoral-femoral, femoral-popliteal) or a patient who has had any type of amputation procedure for PVD (for example, toe amputations, transmetatarsal amputations, below the knee or above the knee amputations). Does not include patients who have had amputation for trauma or a resection of abdominal aortic aneurysms OR 2) Rest pain/gangrene: Rest pain secondary to occlusive disease occurs at rest and is manifested as a severe, unrelenting pain aggravated by elevation and often preventing sleep. Gangrene is a marked skin discoloration and disruption indicative of death and decay of tissues in the extremities due to severe and prolonged ischemia. This includes patients with ischemic ulceration and/or tissue loss related to peripheral vascular disease but does not include patients with Fournier’s gangrene.
Chronic obstructive pulmonary disease: chronic obstructive pulmonary disease (such as emphysema and/or chronic bronchitis) resulting in any one or more of the following: -Functional disability from COPD (e.g., dyspnea, inability to perform ADLs) -Hospitalization in the past for treatment of COPD -Requires chronic bronchodilator therapy with oral or inhaled agents. -An FEV1 of <75% of predicted on pulmonary function testing. Patients are not included whose only pulmonary disease is asthma, an acute and chronic inflammatory disease of the airways resulting in bronchospasm. Patients are not included with diffuse interstitial fibrosis or sarcoidosis.
Diabetes requiring medication: A patient is not included if diabetes is controlled by diet alone. A diagnosis of diabetes requiring therapy with an oral hypoglycemic agent or daily insulin therapy.
Congestive heart failure: Only newly diagnosed CHF within the previous 30 days or a diagnosis of chronic CHF with new signs or symptoms in the 30 days prior to surgery fulfills this definition.
Current smoker: Includes patients who have smoked cigarettes in the year prior to admission to admission for surgery. Does not include patients who smoke cigars or pipes or use chewing tobacco.
Prior operation within 30 days: The patient has had a major surgical procedure performed within 30 days prior to the assessed operation that is listed on the CPT Code Inclusion List. Also include any transplant procedures or trauma procedures if performed within 30 days prior to the assessed operation.
Renal failure on dialysis: Includes patients with either acute renal failure, defined as the clinical condition associated with rapid, steadily increasing azotemia (increase in BUN) and a rising creatinine of above 3 mg/dl, within 24 hours prior to surgery. Additionally includes patients with acute or chronic renal failure requiring treatment with peritoneal dialysis, hemodialysis, hemofiltration, hemodiafiltration, or ultrafiltration within 2 weeks prior to surgery.
Active cancer: Includes patients who have cancer that: (1) Has spread to one site or more sites in addition to the primary site AND (2) In whom the presence of multiple metastases indicates the cancer is widespread, fulminant, or near terminal OR patients who had chemotherapy for malignancy within 30 days prior to surgery (chemotherapy includes both oral or parenteral treatments but cannot solely be comprised of hormonal therapy) OR patients who received any radiotherapy (including radiation seed implantation) for malignancy within 90 days prior to surgery.
Definitions of dependent variables
Deep venous thrombosis: “the identification of a new blood clot or thrombus within the venous system, which may be coupled with inflammation. This diagnosis is confirmed by a duplex, venogram or CT scan. The patient must be treated with anticoagulation therapy and/or placement of a vena cava filter or clipping of the vena cava.”
Pulmonary embolism: “lodging of a blood clot in a pulmonary artery with subsequent obstruction of blood supply to the lung parenchyma…Enter “YES” if the patient has a V-Q scan interpreted as high probability of pulmonary embolism or a positive CT spiral exam, pulmonary arteriogram or CT angiogram.”
Footnotes
Authorship
This manuscript represents the aggregate efforts of ten authors. Peri-operative risk stratification for venous thromboembolism after outpatient surgery is a broad topic that has relevance to a wide range of clinicians, administrators, and policymakers. Our author list reflects a cross section of the clinical care team to whom our manuscript is targeted, and has representation from general surgery, plastic and reconstructive surgery, vascular surgery, anesthesiology, hospital administration, and our office of clinical affairs. Each of the ten authors has fulfilled the criteria for authorship established by Annals of Surgery. Their specific contributions are listed below. All authors have reviewed this manuscript and give their final approval for submission.
- Pannucci: Conception and design, analysis and interpretation of data, drafting of manuscript, statistical analysis
- Shanks: Conception and design, acquisition of data, analysis and interpretation of data, drafting of manuscript, statistical analysis
- Moote: Conception and design, critical revision of manuscript for important intellectual content, administrative, technical, or material support
- Bahl: Conception and design, critical revision of manuscript for important intellectual content, administrative, technical, or material support
- Cederna: Conception and design, critical revision of manuscript for important intellectual content, administrative, technical, or material support
- Naughton: Conception and design, critical revision of manuscript for important intellectual content, no additional contributions
- Wakefield: Analysis and interpretation of data, critical revision of manuscript for important intellectual content, supervision
- Henke: Conception and design, critical revision of manuscript for important intellectual content, supervision
- Campbell: Conception and design, critical revision of manuscript for important intellectual content, supervision
- Kheterpal: Conception and design, acquisition of data, analysis and interpretation of data, drafting of manuscript, administrative, technical, or material support, supervision
Conflicts of Interest
For the remaining authors none were declared.
Contributor Information
Christopher J. Pannucci, Email: cpannucc@umich.edu, Section of Plastic Surgery, University of Michigan.
Amy Shanks, Email: amysha@umich.edu, Department of Anesthesiology, University of Michigan.
Marc J. Moote, Email: mmoote@umich.edu, Office of Clinical Affairs, University of Michigan.
Vinita Bahl, Email: vbahl@umich.edu, Clinical Information and Decision Support Services, University of Michigan.
Paul S. Cederna, Email: cederna@umich.edu, Section of Plastic Surgery, University of Michigan.
Norah N. Naughton, Email: norahnau@umich.edu, Department of Anesthesiology, University of Michigan.
Thomas W. Wakefield, Email: thomasww@umich.edu, Section of Vascular Surgery, University of Michigan.
Peter K. Henke, Email: henke@umich.edu, Section of Vascular Surgery, University of Michigan.
Darrell A. Campbell, Email: darrellc@umich.edu, Office of Clinical Affairs, University of Michigan.
Sachin Kheterpal, Email: sachinkh@umich.edu, Department of Anesthesiology, University of Michigan.
References
- 1.Russo CA, Elixhauser A, Steiner C, et al. [Accessed March 23, 2011];Hospital-based ambulatory surgery, 2007. Published by Healthcare Cost and Utilization Project and Agency for Healthcare Research and Quality. 2010 Feb; http://www.hcup-us.ahrq.gov/reports/statbriefs/sb86.pdf. [PubMed]
- 2.Dhumale R, Tisdale J, Barwell N. Over a thousand ambulatory hernia repairs in a primary care setting. Ann R Coll Surg Engl. 2010;92:127–130. doi: 10.1308/003588410X12518836439281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ford SJ, Wheeler JM, Borley NR. Factors influencing selection for a day-case or 23-h stay procedure in transanal endoscopic microsurgery. Br J Surg. 2010;97:410–414. doi: 10.1002/bjs.6857. [DOI] [PubMed] [Google Scholar]
- 4.Gurusamy K, Junnarkar S, Farouk M, et al. Meta-analysis of randomized controlled trials on the safety and effectiveness of day-case laparoscopic cholecystectomy. Br J Surg. 2008;95:161–168. doi: 10.1002/bjs.6105. [DOI] [PubMed] [Google Scholar]
- 5.Keyes GR, Singer R, Iverson RE, et al. Mortality in outpatient surgery. Plast Reconstr Surg. 2008;122:245–50. doi: 10.1097/PRS.0b013e31817747fd. discussion 251–3. [DOI] [PubMed] [Google Scholar]
- 6.Keyes GR, Singer R, Iverson RE, et al. Analysis of outpatient surgery center safety using an internet-based quality improvement and peer review program. Plast Reconstr Surg. 2004;113:1760–1770. doi: 10.1097/01.prs.0000124743.75839.11. [DOI] [PubMed] [Google Scholar]
- 7.Marla S, Stallard S. Systematic review of day surgery for breast cancer. Int J Surg. 2009;7:318–323. doi: 10.1016/j.ijsu.2009.04.015. [DOI] [PubMed] [Google Scholar]
- 8.Liu JT, Briner RP, Friedman JA. Comparison of inpatient vs. outpatient anterior cervical discectomy and fusion: A retrospective case series. BMC Surg. 2009;9:3. doi: 10.1186/1471-2482-9-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Riber C, Alstrup N, Nymann T, et al. Postoperative thromboembolism after day-case herniorrhaphy. Br J Surg. 1996;83:420–421. doi: 10.1002/bjs.1800830341. [DOI] [PubMed] [Google Scholar]
- 10.Sasse KC, Ganser JH, Kozar MD, et al. Outpatient weight loss surgery: Initiating a gastric bypass and gastric banding ambulatory weight loss surgery center. JSLS. 2009;13:50–55. [PMC free article] [PubMed] [Google Scholar]
- 11.Weale AE, Ackroyd CE, Mani GV, et al. Day-case or short-stay admission for arthroscopic knee surgery: A randomised controlled trial. Ann R Coll Surg Engl. 1998;80:146–149. [PMC free article] [PubMed] [Google Scholar]
- 12.Caprini JA. Thrombosis risk assessment as a guide to quality patient care. Dis Mon. 2005;51:70–78. doi: 10.1016/j.disamonth.2005.02.003. [DOI] [PubMed] [Google Scholar]
- 13.Caprini JA. Risk assessment as a guide for the prevention of the many faces of venous thromboembolism. Am J Surg. 2010;199(1 Suppl):S3–10. doi: 10.1016/j.amjsurg.2009.10.006. [DOI] [PubMed] [Google Scholar]
- 14.Coleridge-Smith PD, Hasty JH, Scurr JH. Venous stasis and vein lumen changes during surgery. Br J Surg. 1990;77:1055–1059. doi: 10.1002/bjs.1800770933. [DOI] [PubMed] [Google Scholar]
- 15.Comerota AJ, Stewart GJ, Alburger PD, et al. Operative venodilation: A previously unsuspected factor in the cause of postoperative deep vein thrombosis. Surgery. 1989;106:301–8. discussion 308–9. [PubMed] [Google Scholar]
- 16.Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American college of chest physicians evidence-based clinical practice guidelines (8th edition) Chest. 2008;133(6 Suppl):381S–453S. doi: 10.1378/chest.08-0656. [DOI] [PubMed] [Google Scholar]
- 17.Nguyen NT, Cronan M, Braley S, et al. Duplex ultrasound assessment of femoral venous flow during laparoscopic and open gastric bypass. Surg Endosc. 2003;17:285–290. doi: 10.1007/s00464-002-8812-z. [DOI] [PubMed] [Google Scholar]
- 18.Patel MI, Hardman DT, Nicholls D, et al. The incidence of deep venous thrombosis after laparoscopic cholecystectomy. Med J Aust. 1996;164:652–4. [PubMed] [Google Scholar]
- 19.Schaepkens Van Riempst JT, Van Hee RH, Weyler JJ. Deep venous thrombosis after laparoscopic cholecystectomy and prevention with nadroparin. Surg Endosc. 2002;16:184–187. doi: 10.1007/s004640090048. [DOI] [PubMed] [Google Scholar]
- 20.Sobolewski AP, Deshmukh RM, Brunson BL, et al. Venous hemodynamic changes during laparoscopic cholecystectomy. J Laparoendosc Surg. 1995;5:363–369. doi: 10.1089/lps.1995.5.363. [DOI] [PubMed] [Google Scholar]
- 21.Engbaek J, Bartholdy J, Hjortso NC. Return hospital visits and morbidity within 60 days after day surgery: A retrospective study of 18,736 day surgical procedures. Acta Anaesthesiol Scand. 2006;50:911–919. doi: 10.1111/j.1399-6576.2006.01090.x. [DOI] [PubMed] [Google Scholar]
- 22.Shabbir J, Ridgway PF, Shields W, et al. Low molecular weight heparin prophylaxis in day case surgery. Ir J Med Sci. 2006;175:26–29. doi: 10.1007/BF03167963. [DOI] [PubMed] [Google Scholar]
- 23.Shiloach M, Frencher SK, Jr, Steeger JE, et al. Toward robust information: Data quality and inter-rater reliability in the american college of surgeons national surgical quality improvement program. J Am Coll Surg. 2010;210:6–16. doi: 10.1016/j.jamcollsurg.2009.09.031. [DOI] [PubMed] [Google Scholar]
- 24.Kheterpal S, O’Reilly M, Englesbe MJ, et al. Preoperative and intraoperative predictors of cardiac adverse events after general, vascular, and urological surgery. Anesthesiology. 2009;110:58–66. doi: 10.1097/ALN.0b013e318190b6dc. [DOI] [PubMed] [Google Scholar]
- 25.Rassi A, Jr, Rassi A, Little WC, et al. Development and validation of a risk score for predicting death in chagas’ heart disease. N Engl J Med. 2006;355:799–808. doi: 10.1056/NEJMoa053241. [DOI] [PubMed] [Google Scholar]
- 26.Bryson GL, Chung F, Cox RG, et al. Patient selection in ambulatory anesthesia - an evidence-based review: Part II. Can J Anaesth. 2004;51:782–794. doi: 10.1007/BF03018450. [DOI] [PubMed] [Google Scholar]
- 27.Bryson GL, Chung F, Finegan BA, et al. Patient selection in ambulatory anesthesia - an evidence-based review: Part I. Can J Anaesth. 2004;51:768–781. doi: 10.1007/BF03018449. [DOI] [PubMed] [Google Scholar]
- 28.Awad IT, Chung F. Factors affecting recovery and discharge following ambulatory surgery. Can J Anaesth. 2006;53:858–872. doi: 10.1007/BF03022828. [DOI] [PubMed] [Google Scholar]
- 29.Chung F, Chan VW, Ong D. A post-anesthetic discharge scoring system for home readiness after ambulatory surgery. J Clin Anesth. 1995;7:500–506. doi: 10.1016/0952-8180(95)00130-a. [DOI] [PubMed] [Google Scholar]
- 30.Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100:1043–1049. doi: 10.1161/01.cir.100.10.1043. [DOI] [PubMed] [Google Scholar]
- 31.Fleisher LA American College of Cardiology/American Heart Association. . Cardiac risk stratification for noncardiac surgery: Update from the american college of Cardiology/American heart association 2007 guidelines. Cleve Clin J Med. 2009;76 (Suppl 4):S9–15. doi: 10.3949/ccjm.76.s4.02. [DOI] [PubMed] [Google Scholar]
- 32.Fleisher LA, Pasternak LR, Herbert R, et al. Inpatient hospital admission and death after outpatient surgery in elderly patients: importance of patient and system characteristics and location of care. Arch Surg. 2004;139:67–72. doi: 10.1001/archsurg.139.1.67. [DOI] [PubMed] [Google Scholar]
- 33.Fleisher LA, Pasternak LR, Lyles A. A novel index of elevated risk of inpatient hospital admission immediately following outpatient surgery. Arch Surg. 2007;142:263–268. doi: 10.1001/archsurg.142.3.263. [DOI] [PubMed] [Google Scholar]
- 34.Wakefield TW, McLafferty RB, Lohr JM, et al. Call to action to prevent venous thromboembolism. J Vasc Surg. 2009;49:1620–1623. doi: 10.1016/j.jvs.2009.01.058. [DOI] [PubMed] [Google Scholar]
- 35. [Accessed March 23, 2011];The Surgeon General’s Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism. http://www.surgeongeneral.gov/library/calls/index.html.
- 36.Lembitz A, Clarke TJ. Clarifying “never events and introducing “always events”. Patient Saf Surg. 2009;3:26. doi: 10.1186/1754-9493-3-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. [Accessed March 23, 2011];Centers for Medicare and Medicaid Services press release. 2008 Apr 14; www.cms.hhs.gov.
- 38.Henke PK, Pannucci CJ. Venous thromboembolism risk factor assessment and prophylaxis. Phlebology. 2010;25:219–223. doi: 10.1258/phleb.2010.010018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. [Accessed March 23, 2011];Surgical Care Improvement Project VTE Core Measures Set. Available at www.jointcommission.org.
- 40.Mitka M. Data-based risk calculators becoming more sophisticated--and more popular. JAMA. 2009;302:730–731. doi: 10.1001/jama.2009.1142. [DOI] [PubMed] [Google Scholar]
- 41.Cohen ME, Bilimoria KY, Ko CY, et al. Development of an american college of surgeons national surgery quality improvement program: Morbidity and mortality risk calculator for colorectal surgery. J Am Coll Surg. 2009;208:1009–1016. doi: 10.1016/j.jamcollsurg.2009.01.043. [DOI] [PubMed] [Google Scholar]
- 42.Bahl V, Hu HM, Henke PK, et al. A validation study of a retrospective venous thromboembolism risk scoring method. Ann Surg. 2010;251:344–50. doi: 10.1097/SLA.0b013e3181b7fca6. [DOI] [PubMed] [Google Scholar]
- 43.Zakai NA, Wright J, Cushman M. Risk factors for venous thrombosis in medical inpatients: Validation of a thrombosis risk score. J Thromb Haemost. 2004;2:2156–2161. doi: 10.1111/j.1538-7836.2004.00991.x. [DOI] [PubMed] [Google Scholar]
- 44.Hatef DA, Kenkel JM, Nguyen MQ, et al. Thromboembolic risk assessment and the efficacy of enoxaparin prophylaxis in excisional body contouring surgery. Plast Reconstr Surg. 2008;122:269–279. doi: 10.1097/PRS.0b013e3181773d4a. [DOI] [PubMed] [Google Scholar]
- 45.Seruya M, Venturi ML, Iorio ML, et al. Efficacy and safety of venous thromboembolism prophylaxis in highest risk plastic surgery patients. Plast Reconstr Surg. 2008;122:1701–1708. doi: 10.1097/PRS.0b013e31818dbffd. [DOI] [PubMed] [Google Scholar]
- 46.Pannucci CJ, Bailey SH, Dreszer G, et al. Validation of the caprini risk assessment model in plastic and reconstructive surgery patients. J Am Coll Surg. 2011;212:105–112. doi: 10.1016/j.jamcollsurg.2010.08.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Rogers SO, Jr, Kilaru RK, Hosokawa P, et al. Multivariable predictors of postoperative venous thromboembolic events after general and vascular surgery: Results from the patient safety in surgery study. J Am Coll Surg. 2007;204:1211–1221. doi: 10.1016/j.jamcollsurg.2007.02.072. [DOI] [PubMed] [Google Scholar]
- 48.Yale SH, Medlin SC, Liang H, et al. Risk assessment model for venothromboembolism in post-hospitalized patients. Int Angiol. 2005;24:250–254. [PubMed] [Google Scholar]
- 49.Sweetland S, Green J, Liu B, et al. Duration and magnitude of the postoperative risk of venous thromboembolism in middle aged women: Prospective cohort study. BMJ. 2009;339:b4583. doi: 10.1136/bmj.b4583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Knipp BS, Blackburn SA, Bloom JR, et al. Endovenous laser ablation: Venous outcomes and thrombotic complications are independent of the presence of deep venous insufficiency. J Vasc Surg. 2008;48:1538–1545. doi: 10.1016/j.jvs.2008.07.052. [DOI] [PubMed] [Google Scholar]
- 51.Lawrence PF, Chandra A, Wu M, et al. Classification of proximal endovenous closure levels and treatment algorithm. J Vasc Surg. 2010;52:388–393. doi: 10.1016/j.jvs.2010.02.263. [DOI] [PubMed] [Google Scholar]
- 52.Efficacy and safety of enoxaparin versus unfractionated heparin for prevention of deep vein thrombosis in elective cancer surgery: A double-blind randomized multicentre trial with venographic assessment. ENOXACAN study group. Br J Surg. 1997;84:1099–1103. [PubMed] [Google Scholar]
- 53.Kim EK, Eom JS, Ahn SH, et al. The efficacy of prophylactic low-molecular-weight heparin to prevent pulmonary thromboembolism in immediate breast reconstruction using the TRAM flap. Plast Reconstr Surg. 2009;123:9–12. doi: 10.1097/PRS.0b013e3181904be7. [DOI] [PubMed] [Google Scholar]
- 54.Lemaine V, McCarthy C, Kaplan K, et al. Venous thromboembolism following microsurgical breast reconstruction: An objective analysis in 225 consecutive patients using low-molecular-weight heparin prophylaxis. Plast Reconstr Surg. 2011;127:1399–1406. doi: 10.1097/PRS.0b013e318208d025. [DOI] [PubMed] [Google Scholar]
- 55.Lapidus L, de Bri E, Ponzer S, et al. High sensitivity with color duplex sonography in thrombosis screening after ankle fracture surgery. J Thromb Haemost. 2006;4:807–812. doi: 10.1111/j.1538-7836.2006.01832.x. [DOI] [PubMed] [Google Scholar]
- 56.Rasmussen MS, Jorgensen LN, Wille-Jorgensen P, et al. Prolonged prophylaxis with dalteparin to prevent late thromboembolic complications in patients undergoing major abdominal surgery: A multicenter randomized open-label study. J Thromb Haemost. 2006;4:2384–2390. doi: 10.1111/j.1538-7836.2006.02153.x. [DOI] [PubMed] [Google Scholar]
- 57.Goldhaber SZ. Tamoxifen: Preventing breast cancer and placing the risk of deep vein thrombosis in perspective. Circulation. 2005;111:539–41. doi: 10.1161/01.CIR.0000156099.83394.A7. [DOI] [PubMed] [Google Scholar]