

Abstract
Purpose
We evaluated the socio-personal and clinical factors that can affect preoperative quality of life to determine how to improve preoperative quality of life in patients with gastric cancer.
Materials and Methods
The preoperative quality of life data of 200 patients (68 females and 132 males; mean age 58.9±12.6 years) with gastric cancer were analyzed according to socio-personal and clinical factors. The Korean versions of the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core (QLQ) 30 and the EORTC QLQ-STO22, a gastric cancer-specific module, were used to assess quality of life. Patients were asked to complete the questionnaire preoperatively by themselves.
Results
Patients with a higher academic background and stage I disease tended to have higher global health status scores. Highly educated younger men had better physical functioning scores. Highly educated and well-nourished patients with stage I cancer had higher role functioning scores. Married patients had better emotional scores. The symptom scales were affected by sex, age, education level, nutrition, and cancer stage.
Conclusions
Preoperative quality of life in patients with gastric cancer can be improved by nutritional support and treatment of symptoms caused by disease progression. Psychological support may be helpful for patients with a poor quality of life.
Keywords: Stomach neoplasms; Quality of life; Preoperative period; Health records, personal; Patients
Introduction
Quality of life (QoL) is important when evaluating treatments for cancer.1 Many studies have been performed to evaluate treatment outcomes based on QoL in patients with gastric cancer. Most of these studies have investigated postoperative QoL according to the extent of gastric resection and the reconstruction method.2,3,4,5 Relatively few reports have evaluated preoperative QoL in patients with gastric cancer.
Growing evidence suggests that baseline measures of self-reported health predict survival in patients with cancer. Many studies have shown that baseline QoL is a prognostic factor for survival.6,7,8 Surgical treatment appears to be particularly suited to clinical studies designed to measure QoL before and after therapeutic intervention. Operative procedures are almost always elective; therefore, adequate time is available for a preoperative assessment of the patient's psychosocial and functional status. The QoL after treatment can be assessed accordingly.9 Therefore, baseline data on QoL in patients with gastric cancer is important.
Among the many available tools to assess health-related QoL in patients with gastric cancer, the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) with the gastric cancer-specific module (QLQ-STO22), has been utilized most frequently.10,11,12
In this study, we evaluated the socio-personal and clinical factors that might affect preoperative QoL to determine how to improve the preoperative QoL of patients with gastric cancer.
Materials and Methods
The QoL data of 212 patients with gastric cancer who underwent gastrectomy between March 2011 and April 2012 at the Kyungpook National University Medical Center were analyzed. Twelve patients with comorbidities that could influence QoL were excluded: five patients with another malignancy (lung cancer and colon cancer), four with chronic respiratory disease, and three with cerebrovascular disease. The patient demographic data are summarized in Table 1.
Table 1. Characteristics of patients.
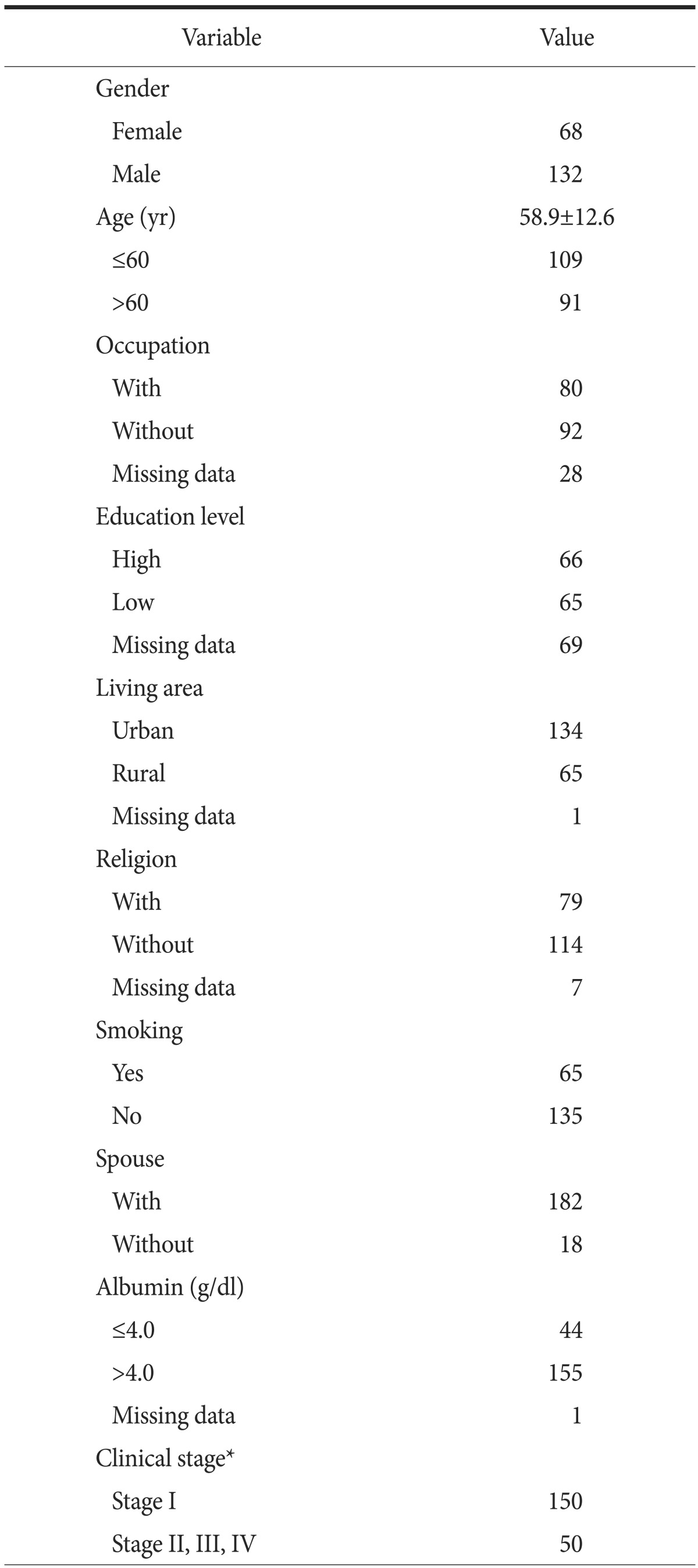
Values are presented as number only or mean±standard deviation. *International Union against Cancer Classification 7th edition
The Korean versions of the EORTC QLQ-C30 and the QLQ-STO22 were used. The EORTC QLQ-C30 is composed of both multi-item scales and single-item measures. These include five functional scales, three symptom scales, a global health status/QoL scale, and six single items. These 15 scales and items can be categorized into three groups of a global health status/QoL scale, five functional scales, and nine symptom scales. QLQ-STO22 is composed of five multi-item scales and four single-item measures.
Patients were asked to complete the questionnaire by themselves on the day of admission. The answers were translated into a score from 0 to 100, according to the scoring manual provided by the EORTC. Higher scores on the functioning scales and lower scores on the symptom scales represent better QoL. Higher scores represent high QoL for the global health status/QoL and the five functional scales, but higher scores on the symptom scales indicate low QoL. A high score on the EORTC QLQ-STO22 indicates low QoL.10
Preoperative QoL was analyzed according to sex, age, occupation (with or without), education level (graduated high school or higher), living area (urban or rural), religion (with or without), smoking, spouse, nutritional status (preoperative serum albumin level), and cancer clinical stage (International Union against Cancer Classification 7th edition).13
We classified patients into older and younger age groups based on the mean age of the participants, 60 years. A smoker was a person that was smoking at the time of diagnosis with gastric cancer. The normal albumin level in our medical center is 3.2 to 4.8 g/dl. Most of the patient's albumin levels were >3.5 g/dl, so we classified the patients into high and low albumin level groups based on a cut-off value of 4.0 g/dl.
The QoL score data are presented as means and were analyzed using Student's t-test. The chi-square test was used to analyze the categorical data and compare the groups. A P-value <0.05 was considered significant.
The data form were used on Microsoft Excel program (Microsort, Rodmond, WA, USA).
Results
Two hundred patients (68 females and 132 males; mean age, 58.9±12.6 years) were included. The global health status score of patients with a higher education level was greater than that of patients with less education (P=0.001). A significant difference was also detected between the global health status scores of patients with stage 1 disease and those of patients with more advanced cancer (P=0.049; Table 2).
Table 2. Global health status/QoL of the EORTC QLQ-30.
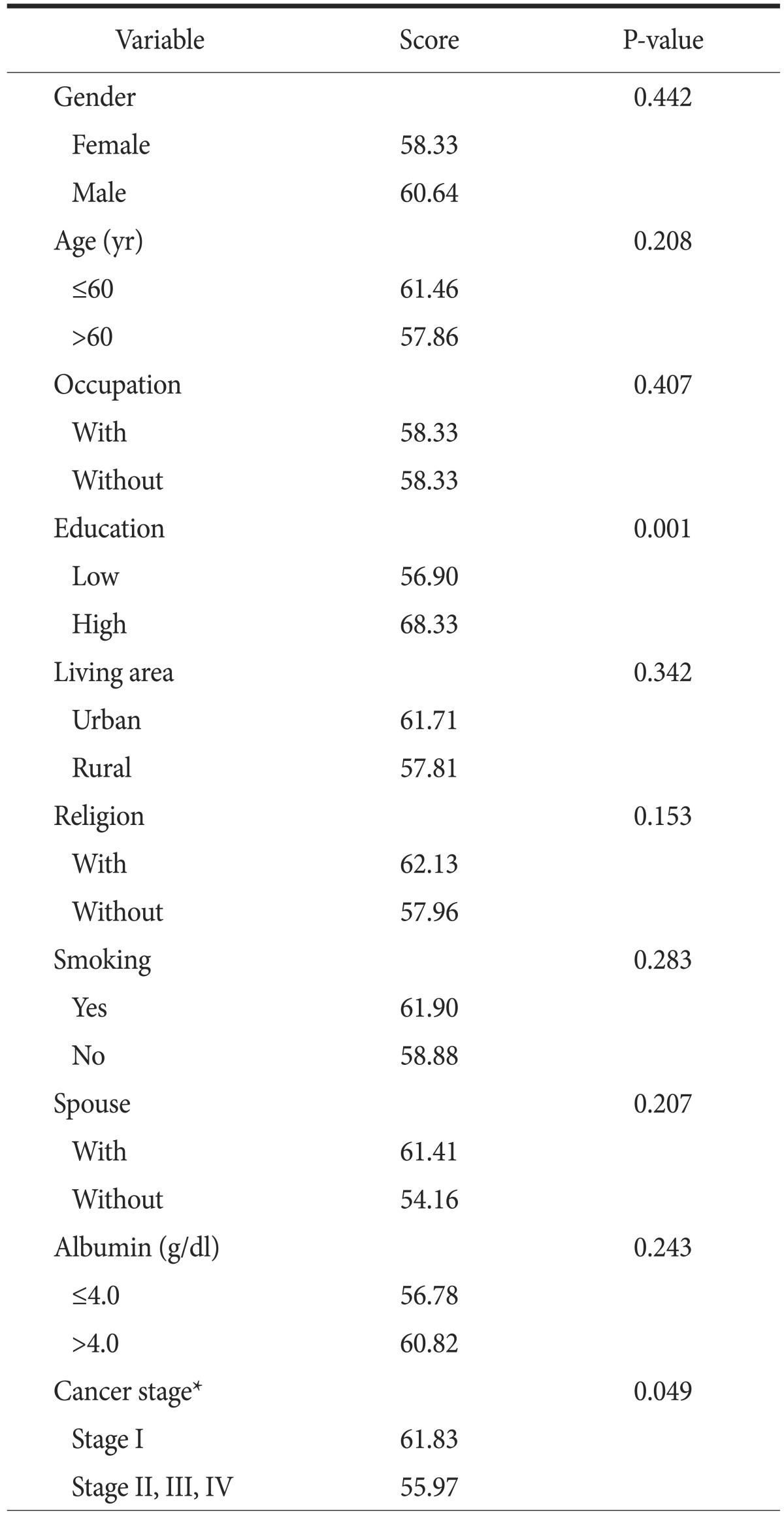
QoL = quality of life; EORTC QLQ-30 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30. *International Union against Cancer Classification 7th edition.
Male (P=0.029), young (P=0.044), and highly educated patients (P=0.001) had better physical functioning scores. Other socio-personal and clinical factors were not significantly associated with the functioning scores (Table 3). Role functioning is the level of limitation for work or rest. The highly educated (P=0.013), well nourished patients (P=0.022) with stage I cancer (P=0.013) had higher role functioning scores. Married patients had better emotional scores (P=0.039). No significant differences in cognitive functioning or social functioning scores were observed for any of the 10 factors.
Table 3. Functioning scales of QLQ-C30.
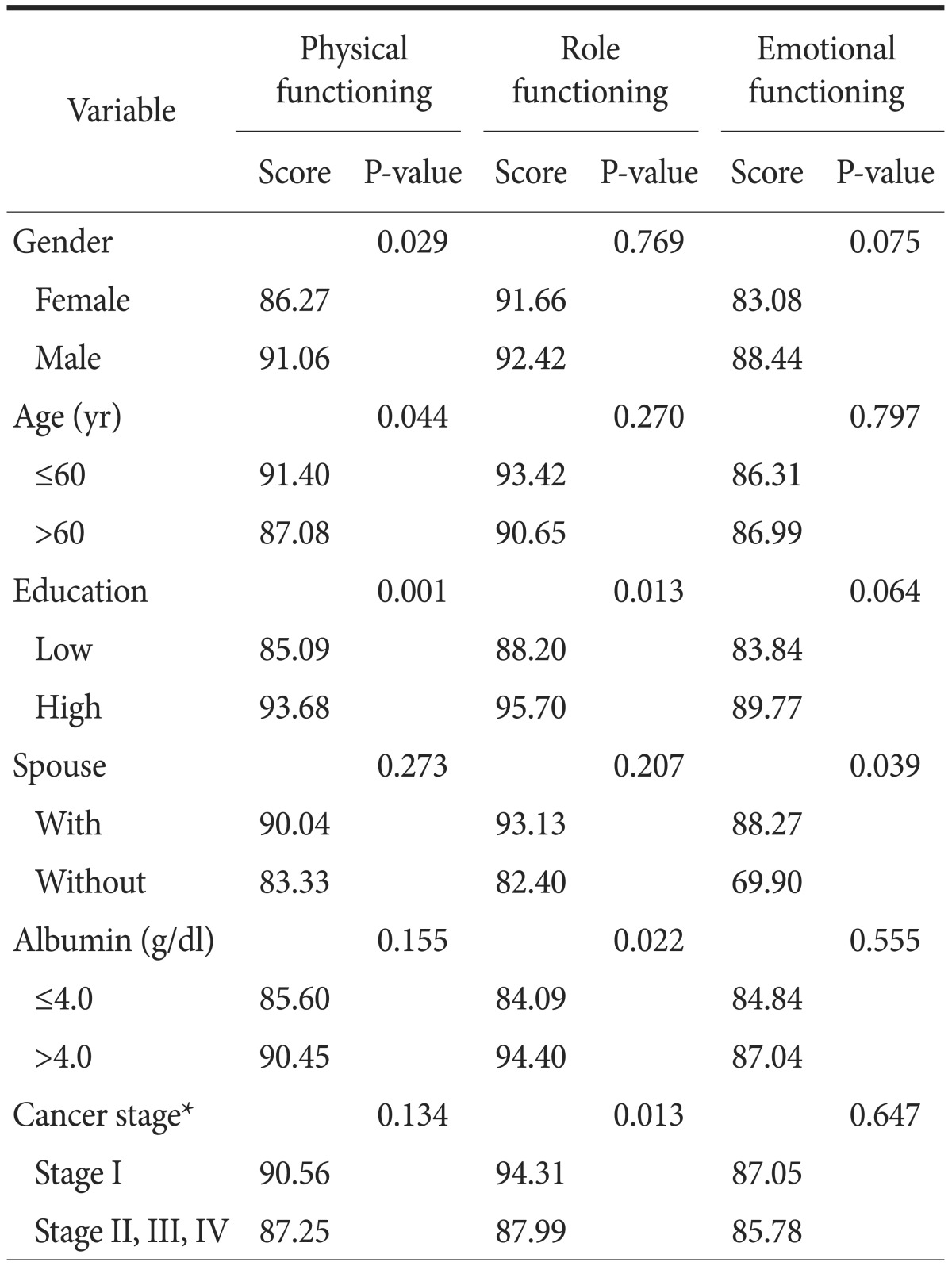
QLQ-C30 = Quality of Life Questionnaire Core 30. *International Union against Cancer Classification 7th edition.
Table 4 shows the QLQ-C30 symptom scales. Highly educated (P=0.044) with stage I cancer (P=0.026) had lower fatigue scores. Married patients had lower nausea and vomiting scores (P=0.032). Patients with stage I cancer had lower pain scores (P=0.005). The dyspnea score was lower in young (P=0.027), highly educated (P=0.001), well-nourished patients (P=0.047) with stage I cancer (P=0.006). The appetite loss score was lower in patients with stage I cancer (P=0.001). Constipation was more frequent in women (P=0.028). The diarrhea score was lower in patients living in an urban area (P=0.037).
Table 4. Symptom scales of QLQ-C30.
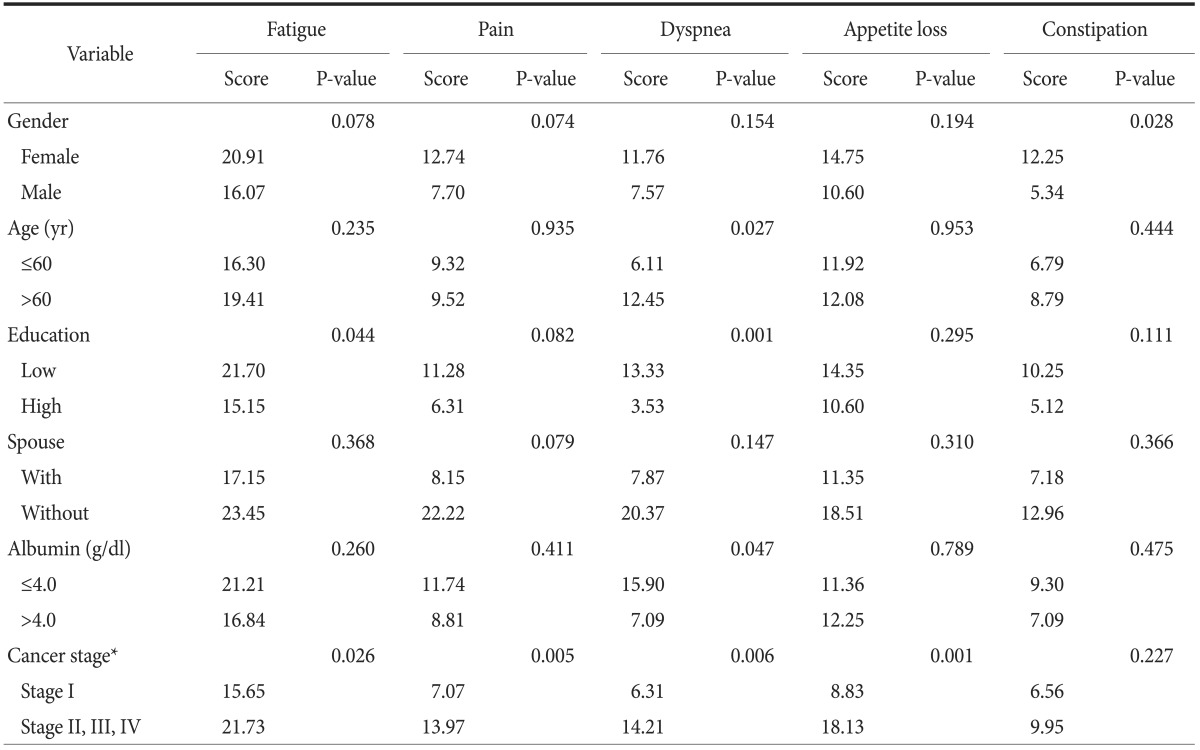
QLQ-C30 = Quality of Life Questionnaire Core 30. *International Union against Cancer Classification 7th edition.
No significant differences were detected for the other symptom scales (nausea, vomiting, and financial difficulties) for any of the 10 factors. No significant differences were observed on the EORTC QLQ-STO22 symptom scales for any of the 10 factors, except for the pain and anxiety scores (Table 5).
Table 5. Symptom scales of EORTC QLQ-STO22.
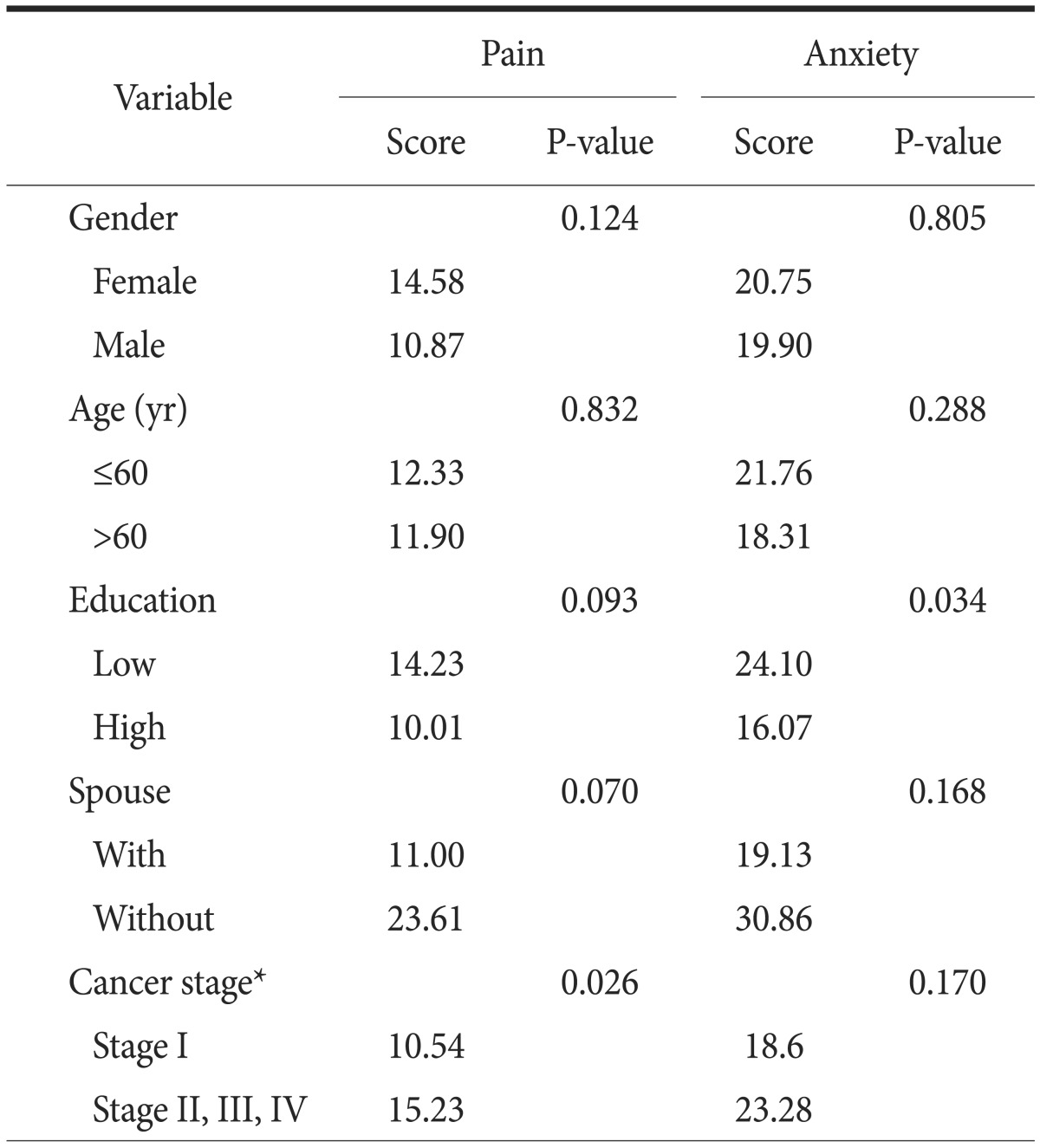
EORTC QLQ-30 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30. *International Union against Cancer Classification 7th edition.
Discussion
QoL is now considered an important outcome measure in cancer research and practice. In our study, we found that the physical functioning of women was lower than that of men, and their constipation score was higher on average than that of men. The women showed a tendency toward lower emotional functioning and higher fatigue and pain, which may have been due to differences between women and men in physical and emotional status. Older patients had lower physical functioning and more dyspnea symptoms than those of younger patients. Bize et al.14 reported a positive association between physical activity level and health-related QoL
Education level affected physical and role functioning. Patients with less education had more fatigue, dyspnea, and anxiety. Accordingly, their global health status/QoL scores tended to be lower than that of the highly educated patients. However, these results are limited due to missing data. Kempen et al.15 reported that education level contributes to physical and social functioning, health perception, and mental health. Emotional functioning in married patients was higher in our study.
Preoperative albumin level might represent nutritional status. Patients with low albumin levels showed poorer role functioning; however, no differences were detected on the other symptom scales or on the global health status score. Cancer-related nutritional deterioration has traditionally been attributed to anorexia and metabolic derangement.16 Nutrition-related symptoms, such as anorexia and fatigue, reflect impaired nutritional status, which is often associated with reduced QoL.17 In this study, patients with low serum albumin levels tended toward lower functioning, more fatigue, and lower global health status/QoL scores. Because most patients (77.5%) in this study had adequate serum albumin levels, more patients are needed to study this issue further.
Patients with stage II or higher cancer revealed lower role functioning and more fatigue, pain, and loss of appetite. Thus, the global health status/QoL score of these patients was lower than that of patients with stage I cancer. Few reports are available on the progression of gastric cancer and associated changes in QoL. The progression of cancer leads to a poor prognosis and high mortality. Patients with advanced gastric cancer have complications that affect QoL, such as obstructions or bleeding due to ulcerations and huge mass lesions. They complained of more symptoms than patients with early stages of cancer and consequently showed a poorer QoL.
We found that sex and age, education level, marital status, serum albumin level, and cancer stage affected preoperative QoL in patients with gastric cancer. Therefore, preoperative QoL can be improved in patients with gastric cancer through nutritional support and treatment of symptoms caused by disease progression. Psychological support may be helpful in patients with poor QoL.
References
- 1.Kobayashi D, Kodera Y, Fujiwara M, Koike M, Nakayama G, Nakao A. Assessment of quality of life after gastrectomy using EORTC QLQ-C30 and STO22. World J Surg. 2011;35:357–364. doi: 10.1007/s00268-010-0860-2. [DOI] [PubMed] [Google Scholar]
- 2.Díaz De Liaño A, Oteiza Martínez F, Ciga MA, Aizcorbe M, Cobo F, Trujillo R. Impact of surgical procedure for gastric cancer on quality of life. Br J Surg. 2003;90:91–94. doi: 10.1002/bjs.4011. [DOI] [PubMed] [Google Scholar]
- 3.Yu W, Lee CH, Chung HY. Quality of life after curative surgery in patients with gastric cancer: comparison between a subtotal gastrectomy and a total gastrectomy. J Korean Gastric Cancer Assoc. 2001;1:44–49. [Google Scholar]
- 4.Adachi Y, Suematsu T, Shiraishi N, Katsuta T, Morimoto A, Kitano S, et al. Quality of life after laparoscopy-assisted Billroth I gastrectomy. Ann Surg. 1999;229:49–54. doi: 10.1097/00000658-199901000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kong H, Kwon OK, Yu W. Changes of quality of life after gastric cancer surgery. J Gastric Cancer. 2012;12:194–200. doi: 10.5230/jgc.2012.12.3.194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Djärv T, Metcalfe C, Avery KN, Lagergren P, Blazeby JM. Prognostic value of changes in health-related quality of life scores during curative treatment for esophagogastric cancer. J Clin Oncol. 2010;28:1666–1670. doi: 10.1200/JCO.2009.23.5143. [DOI] [PubMed] [Google Scholar]
- 7.Quinten C, Coens C, Mauer M, Comte S, Sprangers MA, Cleeland C, et al. EORTC Clinical Groups. Baseline quality of life as a prognostic indicator of survival: a meta-analysis of individual patient data from EORTC clinical trials. Lancet Oncol. 2009;10:865–871. doi: 10.1016/S1470-2045(09)70200-1. [DOI] [PubMed] [Google Scholar]
- 8.Chau I, Norman AR, Cunningham D, Waters JS, Oates J, Ross PJ. Multivariate prognostic factor analysis in locally advanced and metastatic esophago-gastric cancer: pooled analysis from three multicenter, randomized, controlled trials using individual patient data. J Clin Oncol. 2004;22:2395–2403. doi: 10.1200/JCO.2004.08.154. [DOI] [PubMed] [Google Scholar]
- 9.Fayers P, Bottomley A EORTC Quality of Life Group; Quality of Life Unit; European organisation for research and treatment of cancer. Quality of life research within the EORTC-the EORTC QLQ-C30. Eur J Cancer. 2002;38(Suppl 4):S125–S133. doi: 10.1016/s0959-8049(01)00448-8. [DOI] [PubMed] [Google Scholar]
- 10.Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85:365–376. doi: 10.1093/jnci/85.5.365. [DOI] [PubMed] [Google Scholar]
- 11.Vickery CW, Blazeby JM, Conroy T, Arraras J, Sezer O, Koller M, et al. EORTC Quality of Life Group. Development of an EORTC disease-specific quality of life module for use in patients with gastric cancer. Eur J Cancer. 2001;37:966–971. doi: 10.1016/s0959-8049(00)00417-2. [DOI] [PubMed] [Google Scholar]
- 12.Blazeby JM, Conroy T, Bottomley A, Vickery C, Arraras J, Sezer O, et al. European Organisation for Research and Treatment of Cancer Gastrointestinal and Quality of Life Groups. Clinical and psychometric validation of a questionnaire module, the EORTC QLQ-STO 22, to assess quality of life in patients with gastric cancer. Eur J Cancer. 2004;40:2260–2268. doi: 10.1016/j.ejca.2004.05.023. [DOI] [PubMed] [Google Scholar]
- 13.Washington K. 7th edition of the AJCC cancer staging manual: stomach. Ann Surg Oncol. 2010;17:3077–3079. doi: 10.1245/s10434-010-1362-z. [DOI] [PubMed] [Google Scholar]
- 14.Bize R, Johnson JA, Plotnikoff RC. Physical activity level and health-related quality of life in the general adult population: a systematic review. Prev Med. 2007;45:401–415. doi: 10.1016/j.ypmed.2007.07.017. [DOI] [PubMed] [Google Scholar]
- 15.Kempen GI, Brilman EI, Ranchor AV, Ormel J. Morbidity and quality of life and the moderating effects of level of education in the elderly. Soc Sci Med. 1999;49:143–149. doi: 10.1016/s0277-9536(99)00129-x. [DOI] [PubMed] [Google Scholar]
- 16.Ravasco P, Monteiro-Grillo I, Vidal PM, Camilo ME. Cancer: disease and nutrition are key determinants of patients' quality of life. Support Care Cancer. 2004;12:246–252. doi: 10.1007/s00520-003-0568-z. [DOI] [PubMed] [Google Scholar]
- 17.Marín Caro MM, Laviano A, Pichard C. Impact of nutrition on quality of life during cancer. Curr Opin Clin Nutr Metab Care. 2007;10:480–487. doi: 10.1097/MCO.0b013e3281e2c983. [DOI] [PubMed] [Google Scholar]