

Abstract
The present study compared associations between risk and protective factors and adolescent drug use and delinquency in the Netherlands and the United States. Data were collected from students between the ages of 12 and 17 using the same school-administered survey instrument in both countries. Levels of exposure to risk and protective factors were generally similar in both countries. The same risk and protective factors shown to be associated with U.S. adolescents’ drug use and delinquency were related significantly to Dutch youth’s drug use and delinquency. One important exception was that Dutch students perceived their parents’ attitudes to be more favorable toward alcohol use; these attitudes also were more predictive of adolescents’ regular drinking in the Netherlands compared to the United States. The findings indicate that the risk and protective factors measured in this study can be important targets for prevention of health-compromising behaviors among young people in the Netherlands and the United States.
Keywords: Adolescent drug use, delinquency, risk and protective factors, cross-national comparison, prevention
INTRODUCTION
Adolescent health and behavior problems, including alcohol, tobacco, and other drug use, and delinquency, are costly public health problems around the world (European Monitoring Centre for Drugs and Drug Addiction, 2003; Junger-Tas et al., 2010; National Research Council and Institute of Medicine [NRC-IOM], 2009; United Nations, 2005). Fortunately, prevention science has identified malleable risk and protective factors that can be targeted with preventive interventions to reduce rates of youth health and behavior problems (Coie et al., 1993; NRC-IOM, 2009; Woolf, 2008). However, evidence for the relationship between risk and protective factors and adolescent health and behavior problems is based mostly on U.S. samples. Less is known about levels of risk and protective factors in other countries and how they are related to youth drug use and delinquency. Cross-national variation in cultural, normative, legal, and policy settings may affect levels of exposure to risk and protection and also how specific factors are associated with adolescent health and behavior problems (Beyers, Toumbourou, Catalano, Arthur, & Hawkins, 2004; Fagan, Van Horn, Hawkins, & Arthur, 2007; Simons-Morton, Pickett, Boyce, ter Bogt, & Vollebergh, 2010). Examining these relationships should inform the implementation and adaptation of risk- and protection-focused preventive efforts internationally.
LAWS AND NORMS ABOUT ADOLESCENT SUBSTANCE USE IN THE NETHERLANDS AND THE UNITED STATES
The Netherlands and the United States differ in their drug policies and norms toward adolescent drug use (Simons-Morton et al., 2010). The United States has adopted a no-tolerance approach to adolescent substance use that promotes abstinence and criminally penalizes the possession of drugs. It is illegal to sell cigarettes to persons under age 18 and alcohol to persons under age 21. The use, cultivation, and possession of marijuana are illegal at any age in the United States. Although some states have decriminalized the use of medical marijuana, the use of medical marijuana is prohibited under federal law.
The Netherlands uses a harm-reduction policy in which experimentation with alcohol and “soft” drugs (including marijuana) among adolescents is tolerated (European Commission, 2004; Junger-Tas, Marshall, & Ribeaud, 2003; Reinarman, Cohen, & Kaal, 2004). The legal age to purchase alcohol (such as wine and beer) and cigarettes is 16 years, and 18 for hard liquor. Because soft drugs are assumed to pose fewer public health risks than “hard” drugs (such as heroin and cocaine), the Netherlands has decriminalized the possession of small amounts of marijuana (≤ 5 g) and regulates sales in “coffee shops,” in which youths under the age of 18 are not permitted (Ministry of Health Welfare and Sport, 2003; Simons-Morton et al., 2010).
These differences in policies and norms in the Netherlands and the United States likely result not only in different rates of adolescent drug use and associated delinquent behavior in the two countries, but also influence exposure to risk and protective factors associated with substance use and delinquency. Because the use of alcohol and cigarettes is legal for 16- and 17-year-olds in the Netherlands, one would expect that this more tolerant context is reflected in more permissive norms and attitudes about adolescent alcohol use and smoking as well as higher rates of adolescent use of these drugs in the Netherlands compared to the United States. One would expect fewer cross-national differences in risk and protective factors, particularly norms and attitudes, and substance use among younger adolescents (ages 12 – 15) who are exposed to similar legal contexts in both countries. Furthermore, the Netherlands’s harm-reduction policy towards marijuana might lead one to hypothesize that this more permissive context would be reflected in more tolerant attitudes and norms toward adolescent marijuana use among young people and their parents, as well as higher rates of youth marijuana use in the Netherlands than the United States.
Cross-country differences in adolescent substance use and delinquency have been documented, but little is known about cross-cultural differences in levels of risk and protection and whether the same factors in the Netherlands are similarly associated with adolescent substance use and delinquency as in the United States. Consistent with our hypotheses, rates of adolescent alcohol use and cigarette smoking tend to be lower in the United States; however, opposite to what one might expect, rates of adolescent marijuana and hard drug use are lower in the Netherlands (Johnston, O’Malley, Bachman, & Schulenberg, 2006; Monshouwer, van Dorsselaer, Gorter, Verdurmen, & Vollebergh, 2004; Simons-Morton et al., 2010; van Laar, Cruts, Verdurmen, van Ooyen-Houben, & Meijer, 2006). The prevalence of delinquency (among 12- to 15-year olds) is comparable in the two countries (Enzmann et al., 2010).
RISK AND PROTECTIVE FACTORS
Sources of risk and protection exist in multiple domains, including the community, school, family, peers, and the individual. Risk factors such as community disorganization, parental attitudes favorable to drug use, academic failure, friends’ drug use, and rebelliousness have been found to be positively associated with adolescent drug use and delinquency in the United States. Protective factors, including opportunities and rewards for prosocial involvement and attachment to parents, have been shown to be associated with less problem behavior among adolescents in the United States (Hawkins, Arthur, & Catalano, 1995; Hawkins, Catalano, & Miller, 1992).
Few studies have compared risk and protective factors for adolescent problem behaviors cross-nationally, but have found many similarities. Comparisons of data collected from adolescents between the ages of 12 and 17 in Australia and the United States concluded that despite differences in national policies toward adolescent drug use, levels of exposure to risk and protective factors were generally similar (Beyers et al., 2004; Hemphill et al., 2011). Importantly, risk and protective factors in all domains were significantly associated with drug use in Australia as well as in the United States. When there were differences in the strengths of the relationships, the risk and protective factors analyzed were generally more predictive of adolescent drug use in the U.S. samples than in the Australian sample.
The present study compares levels of risk and protective factors and their association with adolescent drug use among 12- to 17-year-olds in the Netherlands and the United States. The present research also examines the relationship of risk and protective factors with delinquency, a behavior that is often closely associated with adolescent drug use and is associated with many of the same risk and protective factors (Hawkins, Catalano, Kosterman, Abbott, & Hill, 1999; Hemphill et al., 2011). Examining common risk and protective factors is important because preventive interventions that address shared risk and protective factors for different adolescent health and behavior problems have produced reductions in multiple outcomes, including drug use, crime, and school dropout (Botvin & Griffin, 2002; Flay, Graumlich, Segawa, Burns, & Holliday, 2004; Haggerty, Skinner, MacKenzie, & Catalano, 2007; Hawkins et al., 1999; Hawkins et al., 2009; Schweinhart et al., 2005). If adolescent drug use and delinquency are associated with the same risk and protective factors in different countries, preventive interventions that address these shared risk and protective factors should have effects on both outcomes across countries.
METHODS
DATA
Data were drawn from two studies that used the same student survey instrument in both countries. In the United States, data were collected in 2004 from all assenting 6th-, 8th-, 10th-, and 12th-grade public school students in 24 communities across 7 states (Colorado, Illinois, Kansas, Maine, Oregon, Utah, and Washington). All U.S. communities were small- to medium-sized incorporated towns (average population size of 15,111 in 2004) with clear community names and boundaries. None of them were suburbs of larger cities. In the Netherlands, surveys of students in Grades 7 – 12 were conducted between 2003 and 2005 in eight cities or boroughs within larger cities (average population size of 35,000) in four provinces (South Holland, North Holland, Flevoland, and Friesland).
Both studies were designed to examine Communities That Care (CTC), a science-based prevention system to prevent adolescent drug use and delinquency community wide. CTC provides training, technical assistance, and tools to enable community coalitions to use advances from prevention science to prevent adolescent drug use and delinquency by identifying elevated risk factors and depressed protective factors experienced by the community’s youth population, and then selecting and implementing preventive interventions that have been shown in experimental or quasi-experimental studies to affect those specific risk and protective factors, and, in turn, adolescent drug use or delinquency. CTC materials are available at www.communitiesthatcare.net. The U.S. study was a randomized controlled trial of CTC in 12 matched pairs of communities (Hawkins et al., 2008). In the Netherlands, surveys were conducted in neighborhoods that were part of an implementation of CTC, and in comparison areas neighboring these sites (Jonkman, Boers, van Dijk, & Rietveld, 2006). Both countries were in the early phases of the CTC process at the time the student data were collected and no intervention effects on risk and protective factors, drug use, and delinquency had been observed at this early point. The present analysis uses data collected from students in both intervention and control communities. Survey completion rates were comparable in intervention and control communities in both countries (83% in the United States and 70% in the Netherlands).
The final analysis samples consisted of 14,608 students in the United States and 18,822 students in the Netherlands. Table 1 shows descriptive statistics. A direct comparison of the racial and ethnic distribution in the two countries was difficult because minority status is defined differently in the two countries. In the U.S. sample, 27.1% of students were of minority status as determined by student reports of their own race or ethnicity as African American, Native American, Hispanic, Asian, Pacific Islander, and other non-White. In the Dutch sample, 29.0% were minority students defined by being born outside the Netherlands or having parents who were born in another country, most commonly in Turkey, Morocco, Surinam, or the Dutch Antilles.
Table 1.
Characteristics of Study Participants (Across 10 Imputed Data Sets)
| United States | Netherlands | |||
|---|---|---|---|---|
| Age 12 – 15 (n = 10,107) % |
Age 16 – 17 (n = 4,501) % |
Age 12 – 15 (n = 14,979) % |
Age 16 – 17 (n = 3,843) % |
|
| Age | ||||
| 12 | 29.6 | 16.1 | ||
| 13 | 22.5 | 29.1 | ||
| 14 | 29.0 | 29.2 | ||
| 15 | 18.9 | 25.7 | ||
| 16 | 60.4 | 66.2 | ||
| 17 | 39.6 | 33.8 | ||
| Mean Age | 13.4 | 16.4 | 13.6 | 16.3 |
| (Std. Dev.) | (1.1) | (0.5) | (1.0) | (0.5) |
| Gender | ||||
| Boys | 48.3 | 48.8 | 47.9 | 48.0 |
| Girls | 51.7 | 51.2 | 52.1 | 52.0 |
INSTRUMENT AND MEASURES
Student data were collected in both countries using the school-based CTC Youth Survey (Arthur et al., 2007). The survey was translated into Dutch and back-translated into English to check for linguistic equivalence (Peña, 2007). In both countries, the survey was group administered in schools during a regular class hour using a paper-and-pencil questionnaire, except in one Dutch community that used a web survey. Passive consent for participation was obtained from parents of all eligible students, with the exception of Utah, where active consent was required by state law. Consented students gave their assent for participation at the beginning of survey administration in schools. Identification numbers but no names or other identifying information were included on the surveys. In the U.S. study, students did not receive incentives to participate. However, U.S. schools eligible to participate in the survey received $500 once all survey activities were completed. In the Netherlands, students had the chance to win prizes in a lottery (e.g., a digital music player). The University of Washington Human Subjects Review Committee and the University Medical Center Utrecht Medical Ethics Review Committee approved these protocols.
RISK AND PROTECTIVE FACTORS
The risk and protective factor constructs included in the present study were created following Arthur et al. (2002). Table 2 presents all risk and protective factor scales included in the analysis, sample items for each scale, and their reliabilities. Because some questions were not asked in the Dutch survey or were not comparable in the two countries, some risk and protective factor scales could not be created or were composed of fewer items than those described in Arthur et al. (2002). Risk and protective factor scales in both countries demonstrated similar internal consistencies, with Cronbach alpha coefficients ranging from .66 to .84 in the United States and from .54 to .86 in the Netherlands (see Table 2). Individual items were analyzed where only one cross-nationally comparable question was available (e.g., low commitment to school), or where reliabilities were too low to justify use of a composite scale. For example, despite the availability of three items with similar question wording and response categories, the reliability of the scale belief in the moral order was α = .44 in the Dutch sample and α = .70 in the U.S. sample. The three individual items were, therefore, analyzed separately. Given the different laws and policies for adolescent use of alcohol, tobacco, marijuana, and other drugs in the United States and the Netherlands, some scales were disaggregated to allow examination of drug-specific risk and protective factors (e.g., parental attitudes favorable to alcohol, cigarette, and marijuana use).
Table 2.
Risk and Protective Factors
| Risk and protective factor scales | Number of items | Range | Reliabilitya
|
Sample item | |
|---|---|---|---|---|---|
| US | NL | ||||
| Community risk factors | |||||
| Community disorganization | 3 | 1–4 | .67 | .67 | How much do each of the following statements describe your neighborhood? Crime and/or drug selling, graffiti. |
| Perceived availability of hard drugs | 1 | 1–4 | NA | NA | If you wanted to get a drug like cocaine, LSD, or amphetamines, how easy would it be for you to get some? |
| Low neighborhood attachment | 3 | 1–4 | .84 | .86 | I’d like to get out of my neighborhood. |
| Community protective factors | |||||
| Rewards for prosocial behavior | 3 | 1–4 | .84 | .77 | There are people in my neighborhood who encourage me to do my best. |
| Family risk factors | |||||
| Family history of antisocial behavior | 1 | 0/1 | NA | NA | Has anyone in your family ever had a severe alcohol or drug problem? |
| Parental attitudes favorable to… | How wrong do your parents feel it would be for you to… | ||||
| Alcohol use | 1 | 1–3 | NA | NA | …drink beer, wine or hard liquor (for example, vodka, whiskey or gin) regularly (at least once or twice a month)? |
| Cigarette use | 1 | 1–3 | NA | NA | …smoke cigarettes? |
| Marijuana use | 1 | 1–3 | NA | NA | …smoke marijuana? |
| Family conflict | 2 | 1–4 | .72 | .71 | We argue about the same things in my family over and over. |
| Poor family management | 6 | 1–3 | .81 | .67 | My family has clear rules about alcohol and drug use. (reversed) |
| Parental attitudes favorable to antisocial behavior | 3 | 1–3 | .74 | .68 | How wrong do your parents feel it would be for you to steal something worth more than $5? |
| Family protective factors | |||||
| Attachment to parents | 4 | 1–4 | .76 | .75 | Do you feel very close to your mother/father? |
| Prosocial opportunities | 3 | 1–4 | .78 | .71 | My parents give me lots of chances to do fun things with them. |
| Rewards for prosocial behavior | 4 | 1–4 | .76 | .72 | My parents notice when I am doing a good job and let me know about it. |
| School risk factors | |||||
| Low commitment to school | 1 | 0–11 | NA | NA | During the last four weeks how many whole days of school have you missed because you skipped or “cut”? |
| Academic failure | |||||
| Low grades | 1 | 1–3 | NA | NA | Putting them all together, what were your grades like last year? |
| Worse grades than peers | 1 | 1–3 | NA | NA | Are your school grades better than the grades of most students in your class? |
| School protective factors | |||||
| Rewards for prosocial behavior | 3 | 1–4 | .66 | .54 | My teachers notice when I am doing a good job and let me know about it. |
| Peer/individual risk factors | |||||
| Rebelliousness | 3 | 1–4 | .73 | .60 | I ignore rules that get in my way. |
| Favorable attitudes toward marijuana/soft drug use | 1 | 1–3 | NA | NA | How wrong do you think it is for someone your age to smoke marijuana? |
| Favorable attitudes toward illegal/hard drug use | 1 | 1–3 | NA | NA | How wrong do you think it is for someone your age to use LSD, cocaine, amphetamines, or another illegal drug? |
| Favorable attitudes toward antisocial behavior | 3 | 1–3 | .76 | .62 | How wrong do you think it is for someone your age to steal something worth more than $5? |
| Peer drug use of… | |||||
| Marijuana/soft drugs | 1 | 0–4 | NA | NA | How many of your best friends have used marijuana/soft drugs (e.g. cannabis or hash)? |
| Illegal/hard drugs | 1 | 0–4 | NA | NA | How many of your best friends have used LSD, cocaine, amphetamines, or other illegal drugs/hard drugs (e.g. cocaine or ecstasy (XTC))? |
| Peer/individual protective factors | |||||
| Moral beliefs | |||||
| Disapproval of cheating | 1 | 1–4 | NA | NA | I think sometimes it’s okay to cheat at school (reverse coded) |
| Disapproval of stealing | 1 | 1–4 | NA | NA | It is okay to take something without asking if you can get away with it. (reverse coded) |
| Importance of honesty | 1 | 1–4 | NA | NA | It is important to be honest with your parents, even if they become upset or you get punished. |
Notes:
Cronbach’s alpha reliability of internal consistency based on standardized items.
DRUG USE
In both countries, alcohol use was defined as drinking beer, wine, or hard liquor, and tobacco use was defined as smoking cigarettes. Marijuana use in the United States was compared to the use of “soft drugs, such as hash or marijuana (cannabis or weed)” in the Netherlands. To measure other illicit drug use in the U.S. sample, self-reports of the use of LSD or other psychedelics, cocaine or crack, and MDMA (“ecstasy”) were combined. In the Netherlands, other illicit drugs referred to the use of “hard drugs, such as cocaine, heroin, speed, or amphetamines” and “XTC (ecstasy).”
For each type of drug, a measure indicating use versus no use was created. Regular alcohol use was defined as having drunk alcohol in the past 30 days on three or more occasions (Beyers et al., 2004; Toumbourou et al., 2005). Daily smoking was defined as having smoked at least one cigarette per day in the past 30 days. Past-month marijuana and other illicit drug use were defined as using each type of drug at least once in the past 30 days. If students had not used any of the four substances in the past month, they were identified as currently not using any drugs.
DELINQUENCY
Students were asked about their participation in three different delinquent behaviors in the 12 months prior to the survey: attacking someone, shoplifting, and damaging property. The number of different delinquent acts reported was calculated across the three behaviors (range = 0 to 3).
ANALYSIS
Because the legal age for alcohol and tobacco use differed in the United States and the Netherlands, the sample was divided into two age groups for analysis: students between the ages of 12 and 15 (for whom alcohol and cigarette use was illegal in both countries) and students ages 16 and 17 (for whom alcohol and cigarette use was legal in the Netherlands, but illegal in the United States).
To avoid biases in parameter estimates and standard errors because of missing data (Schafer & Graham, 2002), multiple imputation procedures employing the expectation-maximization (EM) algorithm as implemented in the NORM 2.03 computer program were used (Schafer, 1997). We report results averaged across 10 datasets imputed separately for each country. After imputation, the Dutch and U.S. datasets were merged for analysis. Because students in both countries were nested in communities, a two-level hierarchical general linear model for continuous dependent variables (risk and protective factors), a hierarchical generalized linear model using a logit-link function for binomially distributed dichotomous dependent variables (drug use variables), and a log-link function for Poisson-distributed count variables (delinquency) were estimated using the HLM 6.04 software (Raudenbush & Bryk, 2002; Raudenbush, Bryk, Cheong, & Congdon, 2004). To control for demographic and socioeconomic differences between the study communities in the United States and the Netherlands, all analyses included community-level variables for population size and the percentage of children under the age of 18 living in poverty (Statistics Netherlands, 2007; Steketee, Tierolf, & Mak, 2007; U.S. Census Bureau, 2001, 2002). The average child poverty rate in analysis communities was 17.3% in the United States and 13.7% in the Netherlands. To adjust for differences in student characteristics, all analyses included covariates at the student level for age, grade, gender, and parental education. To adjust for possible cohort and period effects, a variable for year of data collection was included. All covariates were grand-mean centered. Because samples in both countries were part of an intervention study, all analyses also included a community-level variable indicating whether communities were in the CTC or control condition. No significant intervention effects were observed in any of the analyses.
To examine country differences in levels of risk and protective factors, a random intercept model was estimated that included a dummy variable representing country as a community-level predictor. To examine whether risk and protective factors were significantly associated with drug use and delinquency, we first estimated models separately for the United States and the Netherlands. Models comparing country differences in the association between risk and protective factors with drug use and delinquency included a cross-level interaction between country (a community-level variable) and risk and protective factors (student-level variables). Analyses of delinquent behavior were based on 20 communities instead of 24 in the United States because four communities in one U.S. state did not ask the delinquency questions. Because of the multiple significance tests performed in the analyses, which can increase the false discovery rate, p-values for inference testing were adjusted using the Benjamini-Hochberg procedure for each outcome within age groups (Benjamini & Hochberg, 1995; Thissen, Steinberg, & Kuang, 2002).
RESULTS
PREVALENCE OF DRUG USE AND DELINQUENCY
Figure 1 shows estimated past-month drug use prevalence rates and adjusted odds ratios [AOR]. Adjusted prevalence rates and patterns of differences between the United States and the Netherlands mirrored those found in nationally representative data (e.g., Simons-Morton et al., 2010). The odds of regular alcohol use and daily smoking were twice as high in the Netherlands as in the United States for younger adolescents and almost four times as high for regular alcohol use among 16- and 17-year-olds. The odds of marijuana and other drug use, however, were higher in the United States. The odds of marijuana use among Dutch students was about half that of U.S. students among 12- to 15-year-olds, and about two thirds among 16- and 17-year-olds. The difference in hard drug use was even greater, with Dutch students reporting much lower rates of hard drug use than U.S. students. The percentage of students not using any drugs in the past month was significantly lower among Dutch students compared to U.S. students. These patterns of findings were almost identical for lifetime drug use (analyses not shown). Figure 2 shows the distribution of the number of delinquent behaviors in which students engaged in the past year. Dutch students in both age groups reported significantly fewer delinquent behaviors than U.S. students.
Figure 1.
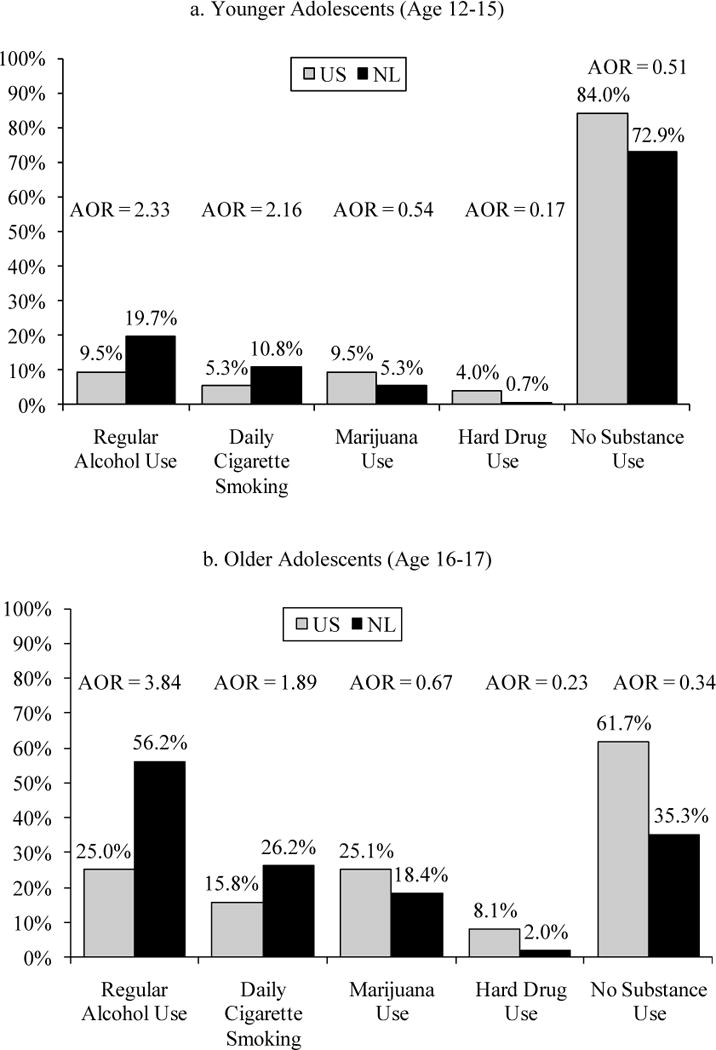
Adjusted rates of past-month substance use in the United States and the Netherlands.
Note: AOR = Adjusted Odds Ratio comparing the rate in the Netherlands to the rate in the United States. All differences between countries are statistically significant (p < .01). Adjusted for year of data collection, student characteristics (age, gender, grade, and parental education), and community characteristics (population size, percentage of children in poverty, and intervention status).
Figure 2.
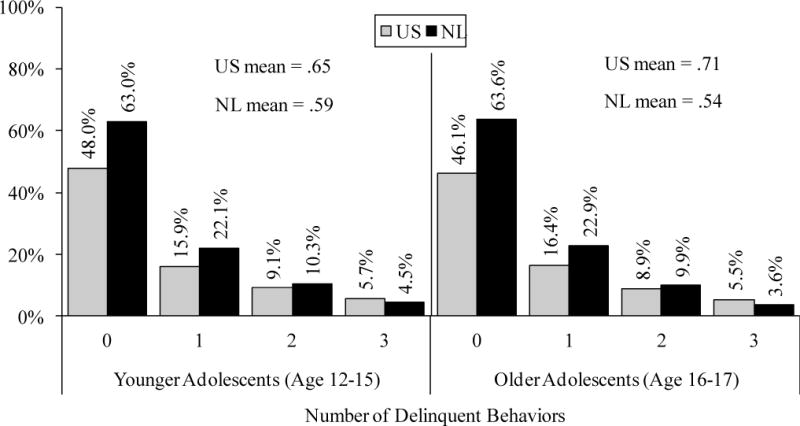
Number of delinquent behaviors in the past year in the United States and the Netherlands.
Note: Mean differences between countries are statistically significant (p < .05). Means are adjusted for year of data collection, student characteristics (age, gender, grade, and parental education), and community characteristics (population size, percentage of children in poverty, and intervention status).
CROSS-NATIONAL DIFFERENCES IN LEVELS OF RISK AND PROTECTION
Comparison of risk and protective factors in the United States and the Netherlands demonstrated statistically significant mean-level differences between the two countries for many factors, but the differences were substantively small, with effect sizes of d = .20 or less (Cohen, 1988). Figure 3 shows effect sizes for risk and protective factors that had significantly different mean levels in the two countries. Only five risk and protective factors showed cross-national differences with at least a medium, or close to medium, effect size (≥ .50). Dutch students perceived their parents’ attitudes to be more favorable toward alcohol and cigarette use than U.S. students, particularly among older adolescents. Students’ perceptions of their parents’ attitudes toward marijuana use, however, did not differ significantly in the two countries for younger or older adolescents. Yet, students’ own attitudes toward marijuana use were more favorable among Dutch compared to U.S. 16- and 17-year-olds. Cross-national differences in attitudes toward marijuana use were smaller among 12- to 15-year-olds. U.S. students, especially younger adolescents, reported higher levels of family conflict and were more likely to disapprove of cheating at school compared to Dutch youth of the same age.
Figure 3.
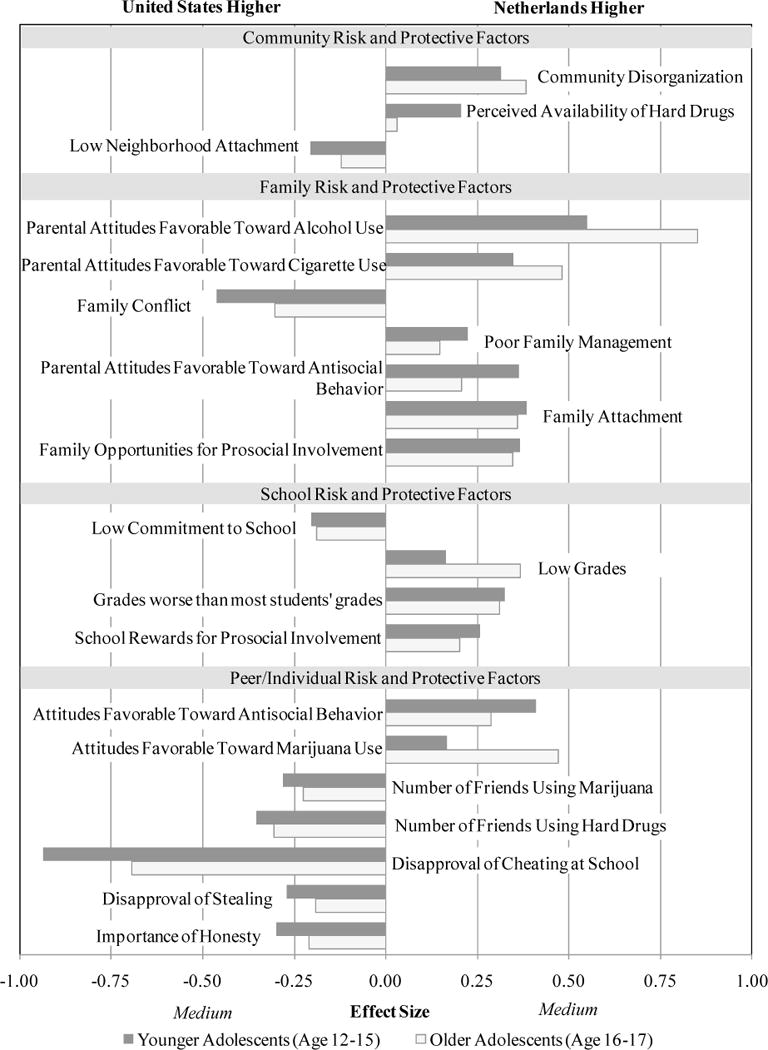
Cross-national differences in levels of risk and protective factors.
Generally, Dutch students had higher risk exposure than U.S. students, but also showed higher levels of protective factors, particularly in the family and school domains. U.S. students were more likely than Dutch students to be exposed to substance-using peers, but also showed higher levels of beliefs in the moral order. In general, findings were similar for younger and older adolescents.
CROSS-NATIONAL DIFFERENCES IN THE ASSOCIATION OF RISK AND PROTECTIVE FACTORS WITH DRUG USE AND DELINQUENCY
Tables 3 to 6 show the AORs for the relationships between risk and protective factors and drug use and delinquency outcomes for 12- to 15-year olds (Tables 3 and 5) and for 16- to 17-year-olds (Tables 4 and 6). The AORs for the interaction term (labeled “NL × RPF” in the tables) indicate whether the strength of the relationships differed significantly in the two countries. AORs less than 1 for risk factors and greater than 1 for protective factors indicate a weaker relationship in the Netherlands than in the United States, except for the outcome of no drug use, where it is the reverse.
Table 3.
Associations Between Risk and Protective Factors and Regular Alcohol Use, Daily Cigarette Smoking, and Marijuana Use Among 12- to 15-Year-Olds in the United States and the Netherlands: Adjusted Odds Ratiosa
| Regular alcohol use
|
Daily cigarette smoking
|
Marijuana use
|
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Risk and protective factors | US | NL | NL × RPF | US | NL | NL × RPF | US | NL | NL × RPF |
| Risk factors | |||||||||
| Community disorganization | 1.65*** | 1.33*** | 0.77* | 1.88*** | 1.47*** | 0.76* | 1.80*** | 1.65*** | 0.90 |
| Perceived availability of hard drugs | 1.94*** | 1.46*** | 0.75* | 1.93*** | 1.64*** | 0.85* | 1.85*** | 1.68*** | 0.93 |
| Low neighborhood attachment | 1.22*** | 1.08*** | 0.89 | 1.23*** | 1.09*** | 0.87 | 1.28*** | 1.23*** | 0.96 |
| Family history of antisocial behavior | 1.64*** | 1.19*** | 0.70** | 1.77*** | 1.38*** | 0.79* | 1.64*** | 1.40*** | 0.85* |
| Parental attitudes favorable to alcohol use | 1.89*** | 2.19*** | 1.15* | 1.69*** | 1.50*** | 0.88* | 1.54*** | 1.53*** | 0.99 |
| Parental attitudes favorable to smoking | 1.54*** | 1.46*** | 0.92 | 1.88*** | 2.04*** | 1.08 | 1.52*** | 1.72*** | 1.11* |
| Parental attitudes favorable to marijuana use | 1.54*** | 1.30*** | 0.83* | 1.63*** | 1.37*** | 0.82* | 1.71*** | 1.59*** | 0.92 |
| Family conflict | 1.60*** | 1.40*** | 0.85* | 1.66*** | 1.45*** | 0.88 | 1.54*** | 1.54*** | 0.99 |
| Poor family management | 2.11*** | 1.54*** | 0.72* | 2.04*** | 1.43*** | 0.69** | 2.09*** | 1.74*** | 0.83** |
| Parental attitudes favorable to antisocial behavior | 1.84*** | 1.40*** | 0.73* | 1.79*** | 1.36*** | 0.75*** | 1.77*** | 1.44*** | 0.79** |
| Low commitment to school | 1.85*** | 1.27*** | 0.67*** | 1.83*** | 1.45*** | 0.78** | 1.88*** | 1.56*** | 0.81** |
| Academic failure – low grades | 1.53*** | 1.31*** | 0.84* | 1.83*** | 1.60*** | 0.85* | 1.63*** | 1.53*** | 0.93 |
| Academic failure – worse grades | 1.73*** | 1.25*** | 0.70* | 2.13*** | 1.52*** | 0.71* | 1.88*** | 1.46*** | 0.76** |
| Rebelliousness | 2.59*** | 1.87*** | 0.70* | 2.78*** | 1.91*** | 0.69* | 2.54*** | 2.18*** | 0.84 |
| Attitudes favorable to marijuana use | 2.40*** | 1.80*** | 0.77** | 2.52*** | 2.24*** | 0.87* | 3.28*** | 3.64*** | 1.09 |
| Attitudes favorable to hard drug use | 1.68*** | 1.28*** | 0.75** | 1.66*** | 1.38*** | 0.83* | 1.70*** | 1.45*** | 0.85** |
| Attitudes favorable to antisocial behavior | 2.26*** | 1.52*** | 0.67** | 2.26*** | 1.69*** | 0.75** | 2.28*** | 1.82*** | 0.79** |
| Peer use of marijuana | 2.70*** | 1.71*** | 0.66** | 3.48*** | 2.41*** | 0.70** | 5.18*** | 4.07*** | 0.81 |
| Peer use of hard drugs | 1.83*** | 1.41*** | 0.76** | 2.03*** | 1.61*** | 0.80** | 1.97*** | 1.75*** | 0.89 |
| Protective factors | |||||||||
| Community rewards for prosocial behavior | 0.67*** | 0.90*** | 1.36* | 0.62*** | 0.86*** | 1.40* | 0.62*** | 0.77*** | 1.24* |
| Attachment to parents | 0.66*** | 0.73*** | 1.14* | 0.64*** | 0.64*** | 1.00 | 0.63*** | 0.57*** | 0.93 |
| Prosocial opportunities in the family | 0.62*** | 0.80*** | 1.31* | 0.60*** | 0.72*** | 1.21* | 0.61*** | 0.65*** | 1.06 |
| Family rewards for prosocial behavior | 0.62*** | 0.76*** | 1.26* | 0.62*** | 0.67*** | 1.09 | 0.59*** | 0.62*** | 1.07 |
| Rewards for prosocial behavior at school | 0.61*** | 0.82*** | 1.30* | 0.62*** | 0.82*** | 1.35** | 0.60*** | 0.72*** | 1.17** |
| Disapproval of cheating | 0.41*** | 0.62*** | 1.43** | 0.42*** | 0.62*** | 1.48** | 0.41*** | 0.53*** | 1.26** |
| Disapproval of stealing | 0.46*** | 0.70*** | 1.53** | 0.45*** | 0.70*** | 1.58** | 0.45*** | 0.64*** | 1.44** |
| Importance of honesty | 0.58*** | 0.80*** | 1.42** | 0.57*** | 0.77*** | 1.36** | 0.56*** | 0.71*** | 1.29*** |
Notes
p < .05
p < .01
p < .001.
Adjusted for year of data collection, student characteristics (age, gender, grade, and parental education), and community characteristics (population size, percentage of children in poverty, and intervention status).
Table 6.
Associations Between Risk and Protective Factors and Hard Drug Use, No Drug Use, and Delinquency Among 16- To 17-Year-Olds in the United States and the Netherlands: Adjusted Odds Ratiosa
| Hard drug use
|
No drug use
|
Delinquency
|
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Risk and protective factors | US | NL | NL × RPF | US | NL | NL × RPF | US | NL | NL × RPF |
| Risk factors | |||||||||
| Community disorganization | 1.80*** | 1.95*** | 1.00 | 0.73*** | 0.82*** | 1.15 | 1.35*** | 1.27*** | 0.94 |
| Perceived availability of hard drugs | 2.81*** | 2.23*** | 0.76 | 0.56*** | 0.67*** | 1.21* | 1.38*** | 1.37*** | 0.99 |
| Low neighborhood attachment | 1.32*** | 1.64*** | 1.23 | 0.80*** | 1.00 | 1.25** | 1.19*** | 1.10*** | 0.91 |
| Family history of antisocial behavior | 1.57*** | 1.64*** | 1.03 | 0.67*** | 0.85*** | 1.30** | 1.30*** | 1.18*** | 0.90* |
| Parental attitudes favorable to alcohol use | 1.54*** | 1.20 | 0.78 | 0.57*** | 0.46*** | 0.82** | 1.28*** | 1.14*** | 0.89** |
| Parental attitudes favorable to smoking | 1.58*** | 2.16*** | 1.36 | 0.57*** | 0.53*** | 0.99 | 1.21*** | 1.28*** | 1.06 |
| Parental attitudes favorable to marijuana use | 1.62*** | 1.87*** | 1.16 | 0.59*** | 0.62*** | 1.07 | 1.24*** | 1.19*** | 0.97 |
| Family conflict | 1.41*** | 1.60*** | 1.09 | 0.73*** | 0.77*** | 1.07 | 1.31*** | 1.18*** | 0.89** |
| Poor family management | 1.86*** | 1.64*** | 0.85 | 0.58*** | 0.71*** | 1.20* | 1.43*** | 1.16*** | 0.82** |
| Parental attitudes favorable to antisocial behavior | 1.58*** | 1.60*** | 1.03 | 0.60*** | 0.80*** | 1.35 | 1.28*** | 1.21*** | 0.96 |
| Low commitment to school | 2.16*** | 1.82*** | 0.83 | 0.50*** | 0.68*** | 1.40** | 1.41*** | 1.31*** | 0.94 |
| Academic failure – low grades | 1.63*** | 1.28* | 0.78 | 0.66*** | 0.74*** | 1.15 | 1.31*** | 1.16*** | 0.90 |
| Academic failure – worse grades | 1.44*** | 1.12 | 0.75 | 0.68*** | 0.82*** | 1.24** | 1.31*** | 1.07*** | 0.82** |
| Rebelliousness | 2.32*** | 2.21*** | 0.94 | 0.51*** | 0.58*** | 1.14 | 1.77*** | 1.59*** | 0.90 |
| Attitudes favorable to marijuana use | 2.93*** | 3.22*** | 1.12 | 0.28*** | 0.41*** | 1.46** | 1.57*** | 1.46*** | 0.94 |
| Attitudes favorable to hard drug use | 2.13*** | 2.20*** | 1.03 | 0.53*** | 0.72*** | 1.37** | 1.30*** | 1.22*** | 0.94 |
| Attitudes favorable to antisocial behavior | 2.23*** | 1.81*** | 0.84 | 0.46*** | 0.62*** | 1.33** | 1.59*** | 1.50*** | 0.98 |
| Peer use of marijuana | 3.63*** | 2.67*** | 0.74 | 0.33*** | 0.48*** | 1.44*** | 1.73*** | 1.51*** | 0.87** |
| Peer use of hard drugs | 3.12*** | 3.29*** | 1.02 | 0.51*** | 0.52*** | 1.06 | 1.44*** | 1.37*** | 0.95 |
| Protective factors | |||||||||
| Community rewards for prosocial behavior | 0.75*** | 0.79 | 1.06 | 1.37*** | 1.10*** | 0.82 | 0.79*** | 0.90*** | 1.14 |
| Attachment to parents | 0.66*** | 0.57*** | 1.09 | 1.36*** | 1.25*** | 0.91 | 0.80*** | 0.83*** | 1.04 |
| Prosocial opportunities in the family | 0.66*** | 0.68*** | 1.09 | 1.40*** | 1.17*** | 0.84 | 0.78*** | 0.85*** | 1.07 |
| Family rewards for prosocial behavior | 0.59*** | 0.63*** | 1.11 | 1.39*** | 1.24*** | 0.89 | 0.76*** | 0.83*** | 1.10 |
| Rewards for prosocial behavior at school | 0.59*** | 0.69*** | 1.20 | 1.34*** | 1.21*** | 0.91 | 0.78*** | 0.85*** | 1.08 |
| Disapproval of cheating | 0.55*** | 0.77*** | 1.36 | 1.88*** | 1.56*** | 0.86 | 0.60*** | 0.74*** | 1.20** |
| Disapproval of stealing | 0.48*** | 0.51*** | 1.07 | 1.94*** | 1.35*** | 0.72** | 0.61*** | 0.74*** | 1.18** |
| Importance of honesty | 0.62*** | 0.67*** | 1.10 | 1.55*** | 1.15*** | 0.74** | 0.73*** | 0.90*** | 1.22** |
Notes:
p < .05
p < .01
p < .001.
Adjusted for year of data collection, student characteristics (age, gender, grade, and parental education), and community characteristics (population size, percentage of children in poverty, and intervention status).
Table 5.
Associations Between Risk and Protective Factors and Hard Drug Use, No Drug Use, and Delinquency Among 12- To 15-Year-Olds in the United States and the Netherlands: Adjusted Odds Ratiosa
| Hard drug use
|
No drug use
|
Delinquency
|
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Risk and protective factors | US | NL | NL × RPF | US | NL | NL × RPF | US | NL | NL × RPF |
| Risk factors | |||||||||
| Community disorganization | 2.27*** | 2.32*** | 1.03 | 0.58*** | 0.73*** | 1.30* | 1.41*** | 1.32*** | 0.93* |
| Perceived availability of hard drugs | 2.58*** | 2.65*** | 1.07 | 0.53*** | 0.65*** | 1.20* | 1.37*** | 1.35*** | 0.96 |
| Low neighborhood attachment | 1.29*** | 1.18 | 1.00 | 0.77*** | 0.92*** | 1.19 | 1.24*** | 1.09*** | 0.87* |
| Family history of antisocial behavior | 1.93*** | 1.61*** | 0.80 | 0.60*** | 0.79*** | 1.35** | 1.34*** | 1.19*** | 0.88** |
| Parental attitudes favorable to alcohol use | 1.71*** | 1.79*** | 1.06 | 0.56*** | 0.50*** | 0.88* | 1.25*** | 1.24*** | 0.96 |
| Parental attitudes favorable to smoking | 1.65*** | 2.04*** | 1.24 | 0.59*** | 0.60*** | 1.01 | 1.19*** | 1.23*** | 1.02 |
| Parental attitudes favorable to marijuana use | 1.70*** | 1.78*** | 1.04 | 0.58*** | 0.73*** | 1.28* | 1.19*** | 1.15*** | 0.96 |
| Family conflict | 1.85*** | 1.69*** | 0.94 | 0.62*** | 0.69*** | 1.13* | 1.42*** | 1.27*** | 0.88* |
| Poor family management | 2.51*** | 2.25*** | 0.94 | 0.47*** | 0.66*** | 1.43** | 1.52*** | 1.29*** | 0.85* |
| Parental attitudes favorable to antisocial behavior | 2.00*** | 1.97*** | 0.97 | 0.50*** | 0.71*** | 1.45** | 1.33*** | 1.30*** | 0.98 |
| Low commitment to school | 2.01*** | 1.72*** | 0.85 | 0.53*** | 0.73*** | 1.43** | 1.35*** | 1.23*** | 0.90** |
| Academic failure – low grades | 1.61*** | 1.53*** | 0.95 | 0.61*** | 0.71*** | 1.18* | 1.31*** | 1.19*** | 0.91* |
| Academic failure – worse grades | 1.79*** | 1.46*** | 0.85 | 0.53*** | 0.75*** | 1.46** | 1.36*** | 1.13*** | 0.84* |
| Rebelliousness | 3.42*** | 2.58*** | 0.73 | 0.39*** | 0.51*** | 1.36* | 1.92*** | 1.69*** | 0.88** |
| Attitudes favorable to marijuana use | 2.58*** | 2.59*** | 1.06 | 0.33*** | 0.48*** | 1.43*** | 1.44*** | 1.43*** | 0.96 |
| Attitudes favorable to hard drug use | 1.93*** | 2.04*** | 1.07 | 0.57*** | 0.74*** | 1.34* | 1.23*** | 1.20*** | 0.97 |
| Attitudes favorable to antisocial behavior | 2.66*** | 2.39*** | 0.95 | 0.41*** | 0.61*** | 1.51** | 1.62*** | 1.53*** | 0.96 |
| Peer use of marijuana | 3.44*** | 2.48*** | 0.78 | 0.31*** | 0.49*** | 1.54** | 1.68*** | 1.47*** | 0.86** |
| Peer use of hard drugs | 2.91*** | 2.15*** | 0.77 | 0.51*** | 0.64*** | 1.25* | 1.40*** | 1.26*** | 0.89*** |
| Protective factors | |||||||||
| Community rewards for prosocial behavior | 0.58*** | 0.83* | 1.37 | 1.55*** | 1.12*** | 0.72* | 0.74*** | 0.90*** | 1.24** |
| Attachment to parents | 0.56*** | 0.54*** | 0.91 | 1.56*** | 1.44*** | 0.91 | 0.72*** | 0.78*** | 1.10* |
| Prosocial opportunities in the family | 0.50*** | 0.59*** | 1.11 | 1.64*** | 1.31*** | 0.79* | 0.71*** | 0.82*** | 1.17* |
| Family rewards for prosocial behavior | 0.51*** | 0.58*** | 1.12 | 1.63*** | 1.38*** | 0.83* | 0.72*** | 0.80*** | 1.13* |
| Rewards for prosocial behavior at school | 0.50*** | 0.50*** | 1.00 | 1.61*** | 1.24*** | 0.78** | 0.74*** | 0.84*** | 1.16* |
| Disapproval of cheating | 0.36*** | 0.54*** | 1.44 | 2.39*** | 1.67*** | 0.72** | 0.55*** | 0.68*** | 1.22** |
| Disapproval of stealing | 0.39*** | 0.54*** | 1.40 | 2.16*** | 1.45*** | 0.66** | 0.61*** | 0.74*** | 1.22** |
| Importance of honesty | 0.48*** | 0.63*** | 1.29 | 1.73*** | 1.27*** | 0.73** | 0.69*** | 0.86*** | 1.25** |
Notes:
p < .05
p < .01
p < .001.
Adjusted for year of data collection, student characteristics (age, gender, grade, and parental education), and community characteristics (population size, percentage of children in poverty, and intervention status).
Table 4.
Associations Between Risk and Protective Factors and Regular Alcohol Use, Daily Cigarette Smoking, And Marijuana Use Among 16- to 17-Year-Olds in the United States and the Netherlands: Adjusted Odds Ratiosa
| Regular alcohol use
|
Daily cigarette smoking
|
Marijuana use
|
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Risk and protective factors | US | NL | NL × RPF | US | NL | NL × RPF | US | NL | NL × RPF |
| Risk factors | |||||||||
| Community disorganization | 1.33*** | 1.15*** | 0.82 | 1.38*** | 1.29*** | 0.92 | 1.44*** | 1.37*** | 0.91 |
| Perceived availability of hard drugs | 1.83*** | 1.38*** | 0.74** | 1.75*** | 1.53*** | 0.86 | 1.80*** | 1.69*** | 0.93 |
| Low neighborhood attachment | 1.18*** | 0.95 | 0.81* | 1.27*** | 1.03 | 0.79** | 1.28*** | 1.17*** | 0.90 |
| Family history of antisocial behavior | 1.46*** | 1.08* | 0.71** | 1.64*** | 1.24*** | 0.75** | 1.46*** | 1.33*** | 0.89 |
| Parental attitudes favorable to alcohol use | 1.85*** | 2.37*** | 1.25* | 1.49*** | 1.29*** | 0.85 | 1.52*** | 1.25*** | 0.83 |
| Parental attitudes favorable to smoking | 1.49*** | 1.48*** | 0.94 | 2.01*** | 2.31*** | 1.13 | 1.55*** | 1.57*** | 0.98 |
| Parental attitudes favorable to marijuana use | 1.52*** | 1.39*** | 0.90 | 1.50*** | 1.41*** | 0.93 | 1.72*** | 1.63*** | 0.96 |
| Family conflict | 1.34*** | 1.25*** | 0.91 | 1.32*** | 1.29*** | 0.97 | 1.34*** | 1.37*** | 0.99 |
| Poor family management | 1.71*** | 1.41*** | 0.82* | 1.60*** | 1.17*** | 0.71*** | 1.66*** | 1.50*** | 0.91 |
| Parental attitudes favorable to antisocial behavior | 1.57*** | 1.20*** | 0.75* | 1.46*** | 1.21*** | 0.86 | 1.47*** | 1.19*** | 0.82 |
| Low commitment to school | 1.95*** | 1.30*** | 0.66*** | 1.81*** | 1.44*** | 0.78** | 1.90*** | 1.67*** | 0.87 |
| Academic failure – low grades | 1.37*** | 1.22*** | 0.87 | 1.69*** | 1.50*** | 0.90 | 1.48*** | 1.31*** | 0.89 |
| Academic failure – worse grades | 1.36*** | 1.17*** | 0.82* | 1.72*** | 1.25*** | 0.73** | 1.41*** | 1.22*** | 0.83 |
| Rebelliousness | 1.95*** | 1.58*** | 0.79** | 1.87*** | 1.67*** | 0.91 | 1.93*** | 1.74*** | 0.91 |
| Attitudes favorable to marijuana use | 2.54*** | 1.92*** | 0.76** | 2.77*** | 2.26*** | 0.81 | 4.16*** | 3.98*** | 0.94 |
| Attitudes favorable to hard drug use | 1.64*** | 1.27*** | 0.77** | 1.65*** | 1.44*** | 0.88 | 1.84*** | 1.50*** | 0.82** |
| Attitudes favorable to antisocial behavior | 2.05*** | 1.43*** | 0.69** | 1.88*** | 1.53*** | 0.86 | 1.94*** | 1.55*** | 0.83 |
| Peer use of marijuana | 2.59*** | 1.67*** | 0.65** | 2.76*** | 2.32*** | 0.83* | 5.12*** | 3.94*** | 0.74 |
| cPeer use of hard drugs | 1.82*** | 1.52*** | 0.81* | 2.05*** | 1.83*** | 0.88* | 2.05*** | 1.82*** | 0.88 |
| Protective factors | |||||||||
| Community rewards for prosocial behavior | 0.75*** | 0.94 | 1.24* | 0.72*** | 0.93 | 1.29** | 0.68*** | 0.78*** | 1.16 |
| Attachment to parents | 0.77*** | 0.86*** | 1.16 | 0.74*** | 0.77*** | 1.06 | 0.73*** | 0.69*** | 0.97 |
| Prosocial opportunities in the family | 0.74*** | 0.90** | 1.25* | 0.71*** | 0.82*** | 1.16 | 0.71*** | 0.71*** | 1.01 |
| Family rewards for prosocial behavior | 0.74*** | 0.86*** | 1.21 | 0.71*** | 0.80*** | 1.14 | 0.69*** | 0.71*** | 1.05 |
| Rewards for prosocial behavior at school | 0.76*** | 0.82*** | 1.11 | 0.74*** | 0.86*** | 1.13 | 0.76*** | 0.87*** | 1.12 |
| Disapproval of cheating | 0.51*** | 0.64*** | 1.24* | 0.65*** | 0.76*** | 1.16 | 0.53*** | 0.69*** | 1.26** |
| Disapproval of stealing | 0.54*** | 0.74*** | 1.36** | 0.59*** | 0.84*** | 1.38** | 0.52*** | 0.75*** | 1.40** |
| Importance of honesty | 0.66*** | 0.89*** | 1.37** | 0.69*** | 0.89** | 1.28** | 0.65*** | 0.86*** | 1.33*** |
Notes:
p < .05
p < .01
p < .001.
Adjusted for year of data collection, student characteristics (age, gender, grade, and parental education), and community characteristics (population size, percentage of children in poverty, and intervention status).
With very few exceptions, risk and protective factors were significantly associated with all of the drug use and delinquency outcomes in both countries. The only consistent exception was low neighborhood attachment, which was weakly or not significantly associated with some of the outcomes in the Netherlands, including hard drug use for younger adolescents and regular alcohol use, daily smoking, and no drug use for 16- and 17-year-olds; however, low neighborhood attachment was significantly associated with higher risk of marijuana use and delinquency in both age groups in both countries. In both countries, rebelliousness, peer use of marijuana, attitudes favorable to marijuana use, and parental and student attitudes favorable toward the use of specific drugs were the strongest risk factors (with a 2.5 to 5 times increase in odds) for most drug use and delinquency outcomes.
Overall, the relationships between risk and protective factors and regular alcohol use, daily smoking, and no drug use were weaker in the Netherlands than in the United States, particularly among 12- to 15-year-olds. There were far fewer cross-national differences, however, in the strength of the relationships between risk and protective factors and marijuana use, hard drug use, and delinquency for both younger and older adolescents. Where there were significant cross-national differences for these outcomes, the relationships also were weaker in the Netherlands than in the United States. Several risk and protective factors showed no cross-national variation in the relationship with any of the outcomes for 16- and 17-year-olds. These included community disorganization, parental attitudes favorable to smoking, parental attitudes favorable to marijuana use, low grades, attachment to parents, family rewards for prosocial behavior, and school rewards for prosocial behavior. There was one notable exception to this general pattern of weaker associations in the Netherlands. Parental attitudes favorable to alcohol use was a significantly stronger predictor of regular alcohol use and no drug use for younger and older Dutch, compared to U.S., adolescents.
DISCUSSION
This study indicates that levels of risk and protection were similar in the United States and the Netherlands and that the same risk and protective factors are associated with both U.S. and Dutch adolescents’ drug use and delinquency. One important exception was that Dutch adolescents perceived their parents’ attitudes to be more favorable toward alcohol use than students in the United States, and these attitudes also were more predictive of adolescents’ regular drinking in the Netherlands. This finding is important given the comparatively high drinking rates among even young adolescents in the Netherlands who are legally not allowed to purchase alcohol. The Dutch harm-reduction approach, with its focus on cannabis, may underestimate the risk that permissive norms about adolescent alcohol use pose for regular alcohol use among young teenagers. In contrast, the abstinence-focused U.S. policy may inadvertently increase the prevalence of the use of marijuana and other illicit drugs.
Although this study did not directly test the consequences of different drug policies and laws in the Netherlands and the United States for adolescent health-compromising behavior, the finding that rates of regular alcohol use and daily smoking were higher among Dutch than among U.S. 16- and 17-year-olds is consistent with the Dutch harm-reduction policy and younger legal drinking and smoking ages compared to the United States. However, that higher rates of alcohol use and smoking were found also for younger adolescents, for whom it is illegal in both countries to drink and smoke, suggests that more permissive norms about adolescent alcohol use and smoking in the Netherlands is a possible risk factor for adolescent health-compromising behaviors. This hypothesis is supported by the finding that Dutch students perceived their parents’ attitudes to be more favorable toward alcohol and cigarette use than did U.S. students and that parents’ attitudes toward adolescent alcohol use also were more strongly associated with an increased risk for adolescents to drink regularly in the Netherlands. Parents’ attitudes toward adolescent smoking, however, were similarly associated with youths’ daily smoking in both countries. Combined, these findings provide a plausible partial explanation for the higher rates of regular drinking and daily smoking among Dutch compared to U.S adolescents.
Bi-national differences in rates of adolescent marijuana and hard drug use were less consistent with differences in U.S. and Dutch laws and policies. The Netherlands has a unique harm-reduction policy towards marijuana, regulating and supervising the sales of marijuana in “coffee shops” (although youths under age 18 are not permitted). One might expect that this more tolerant context also would be reflected in higher rates of youth marijuana use, but this was not found in this study. Rates of adolescent marijuana use were, in fact, higher among U.S. adolescents compared to Dutch adolescents. The goal of the Dutch policy is a separation of markets for soft and hard drugs to keep criminal behavior and the prevalence of hard drug use low (van Laar & Ooijen-Houber, 2009). The finding that rates of hard drug use and the number of delinquent behaviors among adolescents were lower in the Netherlands than the United States provides some supportive evidence for the success of the Dutch policy goal in this regard.
The findings of the present study suggest that norms toward adolescent marijuana use among young people are, in fact, not more tolerant in the Netherlands than the United States. Students’ perceptions of their parents’ attitudes toward marijuana use did not differ significantly in the two countries and predicted youths’ marijuana use similarly. Students’ own attitudes toward marijuana use were more favorable among Dutch than U.S. 16- and 17-year-olds (but not among younger students), but not less of a risk factor for marijuana use. In fact, few other risk and protective factors (except some family and school risk and protective factors) were differentially associated with marijuana use in the Netherlands compared to the United States. Thus, it remains unclear why rates of youth marijuana use are lower in the Netherlands than the United States. One possible hypothesis is that in the no-tolerance context of the United States, adolescent alcohol use is viewed as more deviant than it is in the Dutch context, and therefore, alcohol use may be more likely to serve as a gateway to the use of marijuana and other illicit drugs in the United States. This hypothesis is partially supported by the finding that attitudes and beliefs reflecting tolerance or disapproval of deviance (e.g., parents’ and students’ attitudes about antisocial behavior and students’ moral beliefs) were more strongly associated with adolescents’ regular alcohol use in the United States, but also with daily smoking, marijuana use, and no drug use. Furthermore, parental attitudes favorable to alcohol use were more strongly associated with delinquent behavior for U.S. compared to Dutch 16- and 17-year-olds.
Because the use of alcohol and cigarettes is legal for 16- and 17-year-olds in the Netherlands, one would expect risk and protective factors to be less of a contributing factor to these behaviors among Dutch adolescents. However, the risk and protective factors examined in this study were for the most part associated similarly with drug use and delinquent behaviors in both countries. This finding is important because it stresses the relevance of the risk and protective factors measured in this study for adolescent health-compromising behaviors in different cultural and policy contexts.
Fewer differences in the relationships between risk and protective factors and adolescent drug use and delinquency would have been expected for younger adolescents (ages 12 – 15) who are exposed to similar legal contexts in both countries. However, differences in the association of risk and protective factors and drug use and delinquency were more often observed among 12- to 15-year-olds than 16- and 17-year-olds, and generally with stronger relationships in United States than the Netherlands, and more so for alcohol use and smoking than marijuana use, hard drug use, and delinquency. It may be that the broader normative environment is more important than the specific laws about legal drinking/smoking ages in affecting the relationship between risk and protective factors and these outcomes.
The current study has several limitations. It is based on U.S. and Dutch community samples, which were not designed to be nationally representative of each country’s population of 12- to 17-year-olds. However, the rates of adolescent substance use and delinquency observed in this study were comparable to those reported by national data in both countries. The samples were very similar in their age and gender composition. They differed the most with respect to the communities included in the study. U.S. communities were small- to medium-sized towns, while students in the Netherlands were sampled from neighborhoods in larger cities. To account for country differences in the composition of the student and community samples, all analyses included demographic and socioeconomic covariates. Nevertheless, the reader should interpret country comparisons with these cautions in mind, as observed differences may in part reflect urban-rural differences rather than cross-national differences. Also, this study does not directly test the effect of different drug policies. The results may reflect other unobserved differences between countries not attributable to drug policies, such as the availability of drugs and street prices.
The study also has important strengths. In both countries, data were collected from more than 14,000 students using the same school-based survey instrument and procedures. The CTC student survey provides reliable and valid measures of an empirically derived set of risk and protective factors and drug use and antisocial behavior outcomes (Arthur et al., 2002; Glaser, Van Horn, Arthur, Hawkins, & Catalano, 2005). Analysis strategies applied state-of-the art methods: using multiple imputation to avoid biases in parameter estimates and standard errors due to missing data; estimating multilevel models to account for the nesting of students in communities; adjusting p-values for inference testing to correct for an increase in the false discovery rate because of multiple significance tests; and including covariates to adjust for differences in student and community characteristics.
The same pattern of findings as in this study has been reported in comparisons of student samples from the United States and Australia, a country whose national policies rely on a harm-reduction approach (Beyers et al., 2004; Hemphill et al., 2011). The replication of findings from different cross-national comparisons lends further validity to the results and conclusions of the present study.
The findings of the present study have important implications for international preventive efforts because risk and protective factors are important targets of preventive interventions aimed at reducing rates of youth health-risking behavior community wide. These findings indicate that the risk and protective factors measured here are important targets for efforts to prevent health-compromising behaviors among young people.
Acknowledgments
This research was supported by research grants # R01 DA015183-03S1 from the U.S. National Institute on Drug Abuse and #311000002/1896 from the Netherlands Organization for Health Research and Development (ZonMw). Points of view are those of the authors and are not the official positions of the funding agencies.
Biographies
Sabrina Oesterle is Research Associate Professor with the Social Development Research Group, School of Social Work, University of Washington. Dr. Oesterle’s work is in life course research, the transition to adulthood, longitudinal research methods, and the prevention of health and behavior problems and the promotion of well-being. She is a co-investigator of the Community Youth Development Study, a randomized controlled trial of the Communities That Care prevention system.
J. David Hawkins is Endowed Professor of Prevention, Social Development Research Group, School of Social Work, University of Washington; past President of the Society for Prevention Research; and a fellow of the American Society of Criminology and the Academy of Experimental Criminology. He is the principal investigator of the Community Youth Development Study, a randomized controlled trial of the Communities That Care prevention system. His research over the past 35 years has sought to identify risk and protective factors for health and behavior problems across multiple domains and to understand how these factors interact in the development of healthy behavior and the prevention of problem behaviors.
Majone Steketee is a Senior Researcher at the Verwey-Jonker Institute Utrecht, Netherlands. Her research includes the study of youth mental health, youth and child protection, and the prevention of youth problem behaviors. She conducts evaluation research on evidence-based programs and engages in international comparative work on juvenile delinquency.
Harrie Jonkman is a Senior Researcher at the Verwey-Jonker Institute in Utrecht, Netherlands. His work focuses on the social and cognitive development of children and adolescents, prevention of health, developmental, and behavioral problems, and the impact of community, school, and family settings. He has studied the implementation of the Communities That Care prevention system in the Netherlands.
Eric C. Brown is a Research Assistant Professor with the Social Development Research Group, School of Social Work, University of Washington. His research includes applying advanced methods and designs to investigate the efficacy of school- and community-based preventive interventions.
Marit Moll is a data analysis specialist at the VU University Amsterdam and was a Policy Researcher at the Verwey-Jonker Institute in Utrecht, Netherlands. Her research focuses on youth, delinquency, and substance use.
Kevin P. Haggerty is the Assistant Director of the Social Development Research Group, School of Social Work, University of Washington. He specializes in the development and implementation of prevention programs at community, school, and family levels. He is the principal investigator of Staying Connected, an evaluation of the feasibility of disseminating an evidence-based, self-directed, family-focused substance abuse prevention program (Staying Connected with Your Teen) within the foster care system.
Footnotes
A prior version of this paper was presented at the 2007 and 2011 Annual Meetings of the Society for Prevention Research in Washington, DC.
Contributor Information
Sabrina Oesterle, Email: soe@u.washington.edu.
J. David Hawkins, Email: jdh@u.washington.edu.
Majone Steketee, Email: MSteketee@verwey-jonker.nl.
Harrie Jonkman, Email: HJonkman@verwey-jonker.nl.
Eric C. Brown, Email: ricbrown@u.washington.edu.
Marit Moll, Email: marit.moll@webmail.politieacademie.nl.
Kevin P. Haggerty, Email: haggerty@u.washington.edu.
References
- Arthur MW, Briney JS, Hawkins JD, Abbott RD, Brooke-Weiss BL, Catalano RF. Measuring risk and protection in communities using the Communities That Care Youth Survey. Evaluation and Program Planning. 2007;30:197–211. doi: 10.1016/j.evalprogplan.2007.01.009. [DOI] [PubMed] [Google Scholar]
- Arthur MW, Hawkins JD, Pollard JA, Catalano RF, Baglioni AJ., Jr Measuring risk and protective factors for substance use, delinquency, and other adolescent problem behaviors: The Communities That Care Youth Survey. Evaluation Review. 2002;26:575–601. doi: 10.1177/0193841X0202600601. [DOI] [PubMed] [Google Scholar]
- Benjamini Y, Hochberg Y. Controlling the false discovery rate – a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society Series B-Methodological. 1995;57:289–300. [Google Scholar]
- Beyers JM, Toumbourou JW, Catalano RF, Arthur MW, Hawkins JD. A cross-national comparison of risk and protective factors for adolescent substance use: The United States and Australia. Journal of Adolescent Health. 2004;35:3–16. doi: 10.1016/j.jadohealth.2003.08.015. [DOI] [PubMed] [Google Scholar]
- Botvin GJ, Griffin KW. Life skills training as a primary prevention approach for adolescent drug abuse and other problem behaviors. International Journal of Emergency Mental Health. 2002;4:41–48. [PubMed] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd. Hillsdale, NJ: Lawrence Erlbaum; 1988. [Google Scholar]
- Coie JD, Watt NF, West SG, Hawkins JD, Asarnow JR, Markman HJ, et al. The science of prevention. A conceptual framework and some directions for a national research program. American Psychologist. 1993;48:1013–1022. doi: 10.1037//0003-066x.48.10.1013. [DOI] [PubMed] [Google Scholar]
- Enzmann D, Marshall IH, Killias M, Junger-Tas J, Steketee M, Gruszczynska B. Self-reported youth delinquency in Europe and beyond: First results of the Second International Self-Report Delinquency Study in the context of police and victimization data. European Journal of Criminology. 2010;7:159–183. [Google Scholar]
- European Commission. Flash Eurobarometer 158: Young People and Drugs. 2004 Retrieved November 1, 2007 from http://ec.europa.eu/public_opinion/flash/fl158_en.pdf.
- European Monitoring Centre for Drugs and Drug Addiction. 2003 annual report: The state of the drugs problem in the acceding and candidate countries to the European Union. 2003 Retrieved November 1, 2007 from http://www.emcdda.europa.eu/attachements.cfm/att_37262_EN_candidates_ar2003-en.pdf.
- Fagan AA, Van Horn ML, Hawkins JD, Arthur MW. Gender similarities and differences in the association between risk and protective factors and self-reported serious delinquency. Prevention Science. 2007;8:115–124. doi: 10.1007/s11121-006-0062-1. [DOI] [PubMed] [Google Scholar]
- Flay BR, Graumlich S, Segawa E, Burns JL, Holliday MY. Effects of 2 prevention programs on high-risk behaviors among African American youth: a randomized trial. Archives of Pediatrics & Adolescent Medicine. 2004;158:377–384. doi: 10.1001/archpedi.158.4.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glaser RR, Van Horn ML, Arthur MW, Hawkins JD, Catalano RF. Measurement properties of the Communities That Care Youth Survey across demographic groups. Journal of Quantitative Criminology. 2005;21:73–102. [Google Scholar]
- Haggerty KP, Skinner ML, MacKenzie EP, Catalano RF. A randomized trial of Parents Who Care: Effects on key outcomes at 24-month follow-up. Prevention Science. 2007;8:249–260. doi: 10.1007/s11121-007-0077-2. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Arthur MW, Catalano RF. Preventing substance abuse. In: Tonry M, Farrington D, editors. Crime and justice: Vol. 19. Building a safer society: Strategic approaches to crime prevention. Chicago: University of Chicago Press; 1995. pp. 343–427. [Google Scholar]
- Hawkins JD, Catalano RF, Arthur MW, Egan E, Brown EC, Abbott RD, et al. Testing Communities That Care: The rationale, design and behavioral baseline equivalence of the Community Youth Development Study. Prevention Science. 2008;9:178–190. doi: 10.1007/s11121-008-0092-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, Kosterman R, Abbott R, Hill KG. Preventing adolescent health-risk behaviors by strengthening protection during childhood. Archives of Pediatrics and Adolescent Medicine. 1999;153:226–234. doi: 10.1001/archpedi.153.3.226. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance-abuse prevention. Psychological Bulletin. 1992;112:64–105. doi: 10.1037/0033-2909.112.1.64. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Oesterle S, Brown EC, Arthur MW, Abbott RD, Fagan AA, et al. Results of a type 2 translational research trial to prevent adolescent drug use and delinquency: A test of Communities That Care. Archives of Pediatrics and Adolescent Medicine. 2009;163:789–798. doi: 10.1001/archpediatrics.2009.141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hemphill SA, Kotevski A, Herrenkohl TI, Bond L, Kim MJ, Toumbourou JW, et al. Longitudinal consequences of adolescent bullying perpetration and victimisation: A study of students in Victoria, Australia. Criminal Behaviour and Mental Health. 2011;21:107–116. doi: 10.1002/cbm.802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future: National Survey Results on Drug Use, 1975–2005. Volume I: Secondary School Students. Bethesda, MD: National Institute on Drug Abuse; 2006. (NIH Publication 06-5883). [Google Scholar]
- Jonkman H, Boers R, van Dijk B, Rietveld M. Wijken Gewogen: Gedrag van Jongeren in Kaart Gebracht. Utrecht, The Netherlands: NIZW; 2006. [Google Scholar]
- Junger-Tas J, Marshall IH, Enzmann D, Killias M, Steketee M, Gruszczynska B, editors. Juvenile delinquency in Europe and beyond: Results of the Second International Self-Report Delinquency Study. Berlin: Springer; 2010. [Google Scholar]
- Junger-Tas J, Marshall IH, Ribeaud D. Delinquency in an international perspective: The International Self-Reported Delinquency Study (ISRD) Monsey, NY: Criminal Justice Press; 2003. [Google Scholar]
- Ministry of Health Welfare and Sport. Drug policy in the Netherlands: Basic principles and enforcement in practice. The Hague, The Netherlands: Ministry of Health, Welfare and Sport; 2003. [Google Scholar]
- Monshouwer K, van Dorsselaer S, Gorter A, Verdurmen J, Vollebergh W. Jeugd en Riskant Gedrag: Kerngegevens uit het Peilstationsonderzoek 2003. Roken, Drinken, Drugsgebruik en Gokken Onder Scholieren Vanaf Tien Jaar. Utrecht, The Netherlands: Trimbos Institute; 2004. [Google Scholar]
- Committee on the Prevention of Mental Disorders and Substance Abuse Among Children, Youth, and Young Adults: Research Advances and Promising Interventions. O’Connell Mary Ellen, Boat Thomas, Warner Kenneth E., editors. National Research Council and Institute of Medicine. Preventing mental, emotional, and behavioral disorders among young people: Progress and possibilities. Washington, DC: The National Academies Press; 2009. (Board on Children, Youth, and Families, Division of Behavioral and Social Sciences and Education). [PubMed] [Google Scholar]
- Peña ED. Lost in translation: Methodological considerations in cross-cultural research. Child Development. 2007;78:1255–1264. doi: 10.1111/j.1467-8624.2007.01064.x. [DOI] [PubMed] [Google Scholar]
- Raudenbush SW, Bryk AS. Hierarchical linear models: Applications and data analysis methods. 2nd. Newbury Park, CA: Sage; 2002. [Google Scholar]
- Raudenbush SW, Bryk AS, Cheong YF, Congdon RT., Jr . HLM 6: Hierarchical linear and nonlinear modeling. Lincolnwood, IL: Scientific Software International; 2004. [Google Scholar]
- Reinarman C, Cohen PDA, Kaal HL. The limited relevance of drug policy: Cannabis in Amsterdam and in San Francisco. American Journal of Public Health. 2004;94:836–842. doi: 10.2105/ajph.94.5.836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schafer JL. NORM: Multiple imputation of incomplete multivariate data under a normal model. Windows Version 2.03. University Park, PA: The Methodology Center at Penn State; 1997. [Google Scholar]
- Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychological Methods. 2002;7:147–177. [PubMed] [Google Scholar]
- Schweinhart LJ, Montie J, Xiang Z, Barnett WS, Belfield CR, Nores M. Lifetime effects: The High/Scope Perry Preschool study through age 40. Ypsilanti, MI: High/Scope Press; 2005. (Monographs of the High/Scope Educational Research Foundation, 14). [Google Scholar]
- Simons-Morton B, Pickett W, Boyce W, ter Bogt TFM, Vollebergh W. Cross-national comparison of adolescent drinking and cannabis use in the United States, Canada, and the Netherlands. International Journal of Drug Policy. 2010;21:64–69. doi: 10.1016/j.drugpo.2009.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Statistics Netherlands. Population dynamics by birth, death, and migration per region, 2004. 2007 Retrieved July 23, 2007 from http://statline.cbs.nl.
- Steketee M, Tierolf B, Mak J. Kinderen in Tel Databoek 2007: Kinderrechten als Basis voor Lokaal Jeugdbeleid. Utrecht, The Netherlands: Verwey-Jonker Institute; 2007. [Google Scholar]
- Thissen D, Steinberg L, Kuang D. Quick and easy implementation of the Benjamini-Hochberg procedure for controlling the false positive rate in multiple comparisons. Journal of Educational and Behavioral Statistics. 2002;27:77–83. [Google Scholar]
- Toumbourou JW, Beyers JM, Catalano RF, Hawkins JD, Arthur MW, Evans-Whipp T, et al. Youth alcohol and other drug use in the United States and Australia: A cross-national comparison of three state-wide samples. Drug and Alcohol Review. 2005;24:515–523. doi: 10.1080/09595230500293779. [DOI] [PubMed] [Google Scholar]
- U.S. Census Bureau. Census 2000, Summary File 1, United States. 2001 Retrieved November 1, 2007 from http://factfinder.census.gov/
- U.S. Census Bureau. Census 2000, Summary File 3, United States. 2002 Retrieved November 1, 2007 from http://factfinder.census.gov/
- United Nations. World youth report 2005. New York: Author; 2005. [Google Scholar]
- van Laar M, Cruts AAN, Verdurmen JEE, van Ooyen-Houben MMJ, Meijer RF, editors. The Netherlands national drug monitor: Annual report 2005. Utrecht, The Netherlands: Trimbos Institute; 2006. [Google Scholar]
- van Laar M, Ooijen-Houber M, editors. Evaluatie van het Nederlandse drugsbeleid [Evaluation of Dutch Drug Policy] Utrecht, Den Haag: Trimbos Instituut, WODC; 2009. [Google Scholar]
- Woolf SH. The power of prevention and what it requires. Journal of the American Medical Association. 2008;299:2437–2439. doi: 10.1001/jama.299.20.2437. [DOI] [PubMed] [Google Scholar]