

Abstract
This study examines the complex role of family networks in shaping adult psychological well-being over time. We examine the unique and interactive longitudinal influences of family structure (i.e., composition and size) and negative family relationship quality on psychological well-being among young (aged 18-34), middle-aged (aged 35-49), and older adults (aged 50+). A sample of 881 adults (72% White; 26% Black) was drawn from the longitudinal Social Relations, Age and Health Study. Structural equation modeling indicated that among young and middle-aged adults, increasing family negativity was associated with increases in depressive symptoms over time. In contrast, among older adults, lowered proportion of family in network and an increasing number of family members in the network (i.e. family size) were associated with decreases in depressive symptoms. These findings were moderated by family negativity. Among older adults with low family negativity, having a lower proportion family and larger family size were associated with decreasing depressive symptoms, but there was no effect among those reporting high family negativity. Overall, these results contribute to an increased understanding of the complex, developmental nature of how family support influences well-being across the lifespan and highlights unique age differences.
Keywords: Adult development and aging, Social networks, Family, Psychological well-being
The structure and quality of family support networks are known to develop over time (Levitt, Guacci-Franco, & Levitt, 1993; Antonucci, Akiyama, & Takahashi, 2004) and influence psychological well-being across the adult lifespan (Thoits, 2011). A burgeoning body of research suggests that not only the number of family members providing support, but also the quality of support received from family members, particularly negative quality, plays an important role in shaping adult well-being (Merz, Schuengel, & Schulze, 2009). Yet, it is not fully understood whether there are developmental differences in these quantitative and qualitative aspects of family support. In the current study we address the complex nature of family relationships by examining whether changes in the structure (i.e., composition and size) and negative quality of family support differentially or interactively influence changes in psychological well-being (i.e., depressive symptoms) over time among young, middle-aged, and older adults.
How social relations and depressive symptomatology change over time are important questions that contribute to a fuller understanding of individual development across the lifespan. Longitudinal studies of attachment beginning in infancy have clearly demonstrated how such changes can influence later attachments, competency, and accomplishments in childhood, adolescence, and adulthood (i.e., Treboux, Crowell, & Waters, 2004). Similarly, studies of depression have shown that long-term, consistent depressive symptomatology has a considerably different effect on life quality and well-being than short-term, episodic depressive symptomatology (see Gotlib & Hammen, 2008). In the present study we take advantage of two waves of data over twelve years to consider how long-term changes in patterns of social relations are associated with changes in depressive symptomatology.
Theoretical Perspective
Developmental psychology has long recognized the significance of family relationships for child development (Bronfenbrenner, 1986). Decades of research have demonstrated the instrumental role of the parent-child relationship (Bowlby, 1982; Collins et al., 2000; Schneider, Atkinson, & Tardif, 2001), to a lesser extent the sibling relationship (Dunn, Slomkowski, & Beardsall, 1994), and the overall family network (Furman & Buhrmester, 1985) for child and adolescent development. Recent research suggests there are long-term effects of family relationships experienced when one is a child (Overbeek, Stattin, Vermulst, Ha, & Engels, 2007; Mallers, Charles, Neupert, & Almeida, 2010); however, less is known about family influences on development throughout adulthood.
The Convoy Model of Social Relations (Antonucci, 2001; Kahn & Antonucci, 1980), which proposes that there are important and lasting effects of social relationships on development across the entire lifespan, is used as a guiding theoretical framework for this study. A convoy is conceptualized as a dynamic network of social relationships (composed primarily of family and friends) that affects individual development, and is influenced by personal and contextual factors. For example, the structure (i.e., network size, family/friend balance) and the quality of support provided and received (i.e., positive aspects such as trust and encouragement or negative aspects such as conflict and burden) may vary with age (Antonucci et al., 2002; Birditt & Antonucci, 2007). Moreover, with age, family ties become more numerous and represent a greater proportion of the convoy (Antonucci, Birditt, & Akiyama, 2009).
Convoys have been shown to have protective effects, as highlighted by the stress buffering model (e.g., Cohen & Wills, 1985; Thoits, 2011), which suggests family support may reduce the effect of stress on well-being (e.g., by having someone to confide in or provide advice). Yet, convoys may also have detrimental effects; for example, instead of buffering stress, family relationships may cause additional or exacerbate existing stress (Antonucci et al., 2009). Moreover, the structure and quality of the close family convoy may have distinct effects on well-being compared to the entire social convoy (Antonucci, Birditt, Sherman, & Trinh, 2011).
Close Family Network Size
Family relationships are often heralded because they are more likely than non-familial ties to offer instrumental support in times of need (Adams & Bleiszner, 1995; Grundy & Henretta, 2006). Adults' convoys typically include a variety of relationship types; however, family members make up the largest part of most adults' convoys, and are overwhelmingly represented among the closest ties (Ajrouch, Blandon, & Antonucci, 2005). While in childhood and adolescence a larger family convoy has been shown to have positive developmental effects (Levitt, 2005), the implications of family size in adulthood are less well understood. In midlife, some evidence suggests that large families may be burdensome, instead of beneficial, for well-being (Ward, Spitze, & Deane, 2009). In late-life, a larger family suggests more potential avenues or options for accessing the instrumental support that is essential for maintaining well-being (Antonucci, 2001).
Unlike overall family size, a person's close family network refers to the number of family ties that are perceived to provide support (i.e., nominated as one of their close social support relationships). The close social support network has the greatest influence on well-being (e.g., House, 2001; Akiyama, Antonucci, Takahashi, & Langfahl, 2003; Fingerman & Birditt, 2003; Antonucci, 2001) and, therefore, we expect the family members nominated as part of this close support network will have important implications for well-being across adulthood. Given differences in developmental tasks and circumstances, our first hypothesis is that longitudinal changes in close family network size will differentially impact changes in well-being by age. Because young adults tend to rely more on friends for emotional support (Shaw, Krause, Chatters, Connell, & Ingersoll-Dayton, 2004), we do not anticipate that change in close family network size will be associated with change in young adults' well-being. However, given the greater reliance on family members for emotional support in mid to late-life (Shaw, Krause, Liang, & Bennett, 2007; Ward et al., 2009), we expect middle-aged and older adults will benefit from having a larger network of family for close support. Thus, we hypothesize a positive association between changes in close family network size and changes in depressive symptoms among middle-aged and older adults.
Close Network Family Composition
As described earlier, size of the family support network indicates the quantity of family members nominated within one's close social network. In contrast, proportion family in close network indicates the diversity of available close social support resources (e.g., Antonucci & Akiyama, 1987; Ajrouch, Antoucci, & Janevic, 2001; Fingerman & Birditt, 2003; Fast, Keating, Derksen, & Otfinowski, 2004; Haines, Beggs, & Hurlbert, 2008). For instance, an individual who has a family network size of two may be considered at risk for lacking support. However, if this same person's proportion family in their close network is 20%, because they also have eight close friends to rely upon, they do not lack overall support, but rather only lack family support. In contrast, a person with a family network size of seven may be considered to have a good amount of family support available. Yet, if those seven family members represent 100% of the close network, this indicates a lack of network diversity (i.e., mix of close family and friends in network), which has been linked to poor well-being (Fiori, Antonucci, & Cortina, 2006). Because the close social support network has been shown to have the greatest influence on well-being (e.g., Akiyama et al., 2003; Fingerman & Birditt, 2003), understanding its composition and how this varies across the lifespan is essential.
The composition of close social networks varies greatly by age (Antonucci et al., 2004), with younger adults including fewer family members and more friends in their networks than older adults (Levitt, Weber, & Guacci, 1993) and older adults reporting more kin in their close support networks (Ajrouch et al., 2001). Both the relative absence of, as well as the overwhelming presence of family in the social network have been shown to be detrimental throughout the lifespan (Antonucci, 2001; Levitt, 2005). Peek and Lin (1999) found that people with a higher proportion of family in their networks report fewer depressive symptoms than those with a lower proportion of family. Yet, recent research indicates that people with diverse social networks (i.e., a mix of family and friends) report better well-being than do people who lack either friends or family (Fiori et al., 2006), and others find no association between proportion family and well-being (Haines et al., 2008). These incongruences may be indicative of differential effects of proportion family across the adult lifespan (Cornwell, Laumann, & Schumm, 2008). For instance, a higher proportion family may be more beneficial for younger adults who generally have lower overall proportion family compared to other age groups; whereas among older adults a higher proportion family may indicate a lack of friends and social isolation, and thus be detrimental to well-being (e.g., Gupta & Korte, 1994). Therefore, our second hypothesis suggests distinct effects across age groups. We hypothesize that among young adults, an increase in proportion family among close contacts will be positively associated with increases in psychological well-being, as we anticipate benefits for those who rely on both family and friends for support. In contrast, among older adults, we anticipate that increases in proportion family among close contacts will be associated with decreases in psychological well-being, suggesting benefits of network diversity and not relying entirely on family for support. Because diversity (i.e., mix of family and friends) of network composition in midlife tends to be more balanced (Ajrouch et al., 2001), we do not anticipate a link between change in proportion family in close network and change in well-being in middle adulthood.
Negative Quality of Support
Despite the significance of the structural characteristics of close social networks, the quality of social relationships is documented to have a greater influence on well-being (Merz et al., 2009). Developmental psychology has carefully documented the importance of family relationship quality in childhood and adolescence (e.g., Schneider et al., 2001; Levitt et al., 1993a; Bretherton, 1992); however, less is known about links between family relationship quality and well-being in the broader context of adult development. While much of the research on adult relationship quality has focused on parent-child (see Sechrist, et al., 2012) and spousal ties (see Bookwala, 2012), a growing emphasis is placed on the quality of other family and non-family relationships (Fingerman, Hay, & Birditt, 2004). Since family relationships are obligatory, long lasting, and develop over time, it is difficult to dissolve negative quality family relationships. This is unlike friend relationships which are usually terminated if relationship quality is poor (Antonucci et al., 2009). Some research suggests that with increased age, reports of relational negativity decline (Akiyama et al., 2003; Fingerman & Birditt, 2003; Carstensen, 1993). Other studies have found that age does not predict negative quality (Krause & Rook, 2003; Shaw et al., 2007), while recent research by Birditt and colleagues (2009) suggests that changes in negative qualities vary by relationship type. This latter finding is particularly important as people have different types of immediate family relationships across the lifespan. For example, generally young adults have parents, middle-aged adults have children and parents, and older adults have only children.
Negative relationship quality is consistently associated with well-being, reportedly having a stronger and longer lasting effect than positive support quality (Newsom, Nishishiba, Morgan, & Rook, 2003; Rook, Sorking, & Zettel, 2004;Kawachi & Berkman, 2001). Negative quality has been found to predict worse well-being (e.g., more depressive symptoms, lower life satisfaction, and greater risk of mortality) (Fingerman et al., 2004; Newsom, Mahan, Rook, & Krause, 2008; Turner & Avison, 2003). At the same time, negativity has also been shown to have a positive effect on emotional closeness (e.g., Fung, Yeung, Li, & Lang,2009). Though the growing body of research exploring the link between social relations and mental health has not yet clearly addressed the effect of age (Berkman, Glass, Brissette, & Seeman, 2000), relationship behaviors (e.g., conflict resolution, support, etc.) have often been found to be more influential for well-being in early adulthood (Walen & Lachman, 2000). Thus, our third hypothesis is that among young adults, increases in family negativity will be associated with increases in depressive symptoms. In contrast, we anticipate that changes in negativity will be less influential for changes in psychological well-being in mid and late life, due to both lowered perception of and less internalization of negativity.
Interplay of Quantity and Quality of Support
While providing a more nuanced approach to the study of interpersonal relationships, the distinction between family convoy structure and quality of family relations has unfortunately created a divided focus in which the two are often studied in isolation. Given that family convoy structure and quality are confounded, it is relevant to understand how they interact to influence development. Other research suggests that a diverse social network (Fiori et al., 2006) is more positively associated with well-being, but little research has examined whether the longitudinal effects of family support network structure on well-being varies depending on the quality of family relationships. Research is needed to examine the interaction of family network composition and family quality within the context of age. Such an investigation is consistent with Antonucci and colleagues' (2013) call to explore how social relations influence well-being in a more nuanced manner and within unique contexts. For instance, the effect of family network structure on well-being is likely distinct for an older adult as compared to a younger adult reporting high versus low family negativity. As a fourth hypothesis, we predict that the direction and extent that changes in psychological well-being are influenced by changes in family network size and composition will depend on the extent of changes in family negativity. Specifically, we anticipate that in the context of increasing levels of family negativity, greater family presence in network will be associated with increases in depressive symptomatology. The negative quality of family relationships may be an exemplification of the buffering model in that decreasing negativity among family ties buffers the effects of a convoy that is lacking in either size or family/friend diversity.
The Present Study
The present study has two primary objectives: 1) to examine whether change in close family support network structure (i.e., composition and size) and negative quality of family relationship predict changes in psychological well-being differently among young, middle-aged, and older adults; and 2) to determine whether change in family support network structure and family negativity interact to predict changes in well-being. Among young adults, we hypothesize that change in the number of family members nominated in one's close social network will not be associated with changes in well-being (H1). However, we also expect that among young adults an increase in proportion of family (i.e., better family/friend balance) will be associated with lowered depressive symptoms (H2), while increased family negativity will be associated with more depressive symptoms (H3). Among middle-aged adults, we hypothesize that experiencing an increase of family members in one's close network will be associated with increases in depressive symptoms (H1). However, we do not anticipate a link between change in proportion of family in network or family negativity and well-being in this age group (H2/H3). Among older adults, we hypothesize that increases in family members will be associated with decreases in depressive symptoms (H1), while increases in proportion of family (i.e., less diverse network) will be associated with increases in depressive symptoms (H2). Lastly, we anticipate that family negative relationship quality will moderate the link between family network structure (i.e., composition and size) and depressive symptoms across age groups (H4).
Method
Procedure
The current sample was drawn from the longitudinal Social Relations, Age, and Health Study (Antonucci 1992; Antonucci 2005). At the first wave, collected in 1992 and 1993, a two-stage area probability sampling design was used to randomly select a regionally representative sample from the Detroit metropolitan area. The sample of 1,703 respondents aged 8 to 93 included an oversampling of people ≥60-years-old with a 72% response rate (Antonucci et al., 2004). At Wave 1 respondents between the ages of 8-12 received a modified survey instrument at Wave 1 and thus were excluded from the present study. The time lag of 12 years allows for significant changes in social relationships including major family transitions that are pertinent to studying changes in family convoys. At the second wave (2005) 1,076 of the original respondents participated, 320 were deceased (19%), 43 were incapacitated (3%), and 264 were lost to follow-up, refused, or were unable to participate (16%) resulting in a follow-up response rate of 78%. People who died or were incapacitated were less educated, older, more likely to be male, had lower self-rated health, more depressive symptoms, and fewer social network members. People who did not participate in Wave 2 for other reasons (e.g., refusal, lost) were less educated, younger, and had smaller networks. The study was approved by the University of Michigan Behavioral and Social Science Institutional Review Board. After signing informed consent forms, participants were interviewed in their homes for approximately one hour. The second wave interview was conducted in 2005 by telephone and also lasted about one hour.
Participants
Respondents aged 18 and older at the initial data collection (1992-3) were selected from the larger study (N=881). At Wave 2 the selected participants were between the ages of 30 and 100 with a mean age of 55.5 (SD = 15.8). Sixty percent of the sample were women. A majority of the sample (72%) identified their race as White (N = 634), 26% identified as Black (N = 231), and 2% (N=16) identified as Hispanic, Native American, Asian, Other or did not provide a response. Participants had an average of 13.5 (some college) years of education (8 to 17+; SD = 2.1). Sixty-eight percent of the sample were married or living with a partner. In Table 1 a description of the sample is presented separately for young, middle-aged, and older adult groups.
Table 1.
Means, Standard Deviations, and Range for All Model Indicators for Younger, Middle-Aged, and Older Adults.
| Variables | Younger (N = 268) | Middle-aged (N = 297) | Older (N = 281) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | |
| Demographics | |||||||||
| Age (W1) | 27.6 | 4.7 | 18-34 | 40.8 | 4.2 | 35-49 | 62.1 | 7.2 | 50-80 |
| % Female | 63 | 64 | 55 | ||||||
| % White | 63 | 77 | 81 | ||||||
| Years of Education (W2) | 13.4 | 2.1 | 8-17 | 14.0 | 2.2 | 8-17 | 13.1 | 2.5 | 8-17 |
| % Married (W2) | 73 | 72 | 61 | ||||||
| % have mother (W2) | 81 | 55 | 8 | ||||||
| % have father (W2) | 59 | 26 | 2 | ||||||
| % have child (W2) | 58 | 85 | 95 | ||||||
| Wave 1 | |||||||||
| Proportion Family | .81 | .23 | 0-1 | .84 | .21 | 0-1 | .85 | .21 | 0-1 |
| Family Size | 6.39 | 2.8 | 0-10 | 7.03 | 2.62 | 0-10 | 6.74 | 2.80 | 0-10 |
| Family Negativity | 2.82 | .96 | 1-5 | 2.62 | .91 | 1-5 | 2.23 | 1.01 | 1-5 |
| Depressive Symptoms | 12.14 | 9.72 | 0-49 | 10.55 | 10.67 | 0-51 | 7.78 | 7.23 | 0-35 |
| Wave 2 | |||||||||
| Proportion Family | .70 | .21 | 0-1 | .75 | .22 | 0-1 | .81 | .23 | 0-1 |
| Family Size | 5.90 | 2.30 | 0-10 | 6.59 | 2.53 | 0-10 | 6.48 | 2.85 | 0-10 |
| Family Negativity | 2.55 | .94 | 1-5 | 2.37 | .92 | 1-5 | 2.06 | .98 | 1-5 |
| Depressive Symptoms | 8.47 | 9.00 | 0-44 | 7.94 | 10.27 | 0-57 | 7.46 | 7.21 | 0-34 |
Measures
Age
Participants reported their date of birth, and from that, age was calculated as a continuous variable at both waves. The sample was split into young, middle-aged, and older age groups; then models were examined separately for each group. The age groups were defined based on Wave 1 age as follows: young age group consisted of ages 18 to 34 (N=268), the middle age group consisted of ages 35 to 49 (N=297), and the older age group consisted of ages 50 to 80 (N=281). Age divisions were selected to identify changes related to the transition between developmental stages of adulthood (i.e. emerging/young adulthood, mid-life, and latelife) (e.g. Blanchard-Fields & Coats, 2008).
Close Family Support Network Structure: Size and Composition
The hierarchical mapping technique developed by Antonucci (1986) was used to measure social network characteristics identified by the respondents. For this procedure, respondents were first shown a diagram consisting of three concentric circles and asked to identify three levels of close relationship partners. Respondents were asked about their relationship with their close social network (i.e. up to the first 10 people in their network aged 13 or older). Non-family were coded as 0, and family members were coded as 1. At both waves, two variables were calculated to document the presence of family in respondents' close social support networks. Family network size was measured as the total number of immediate or extended family members identified in the close social network. Family network composition (i.e. proportion family) was determined by calculating the percentage of the close social network made up of immediate or extended family members.
Perceived Family Negativity
Participants rated the perceived negative aspects of their relationships with four immediate family members (spouse/partner, mother, father, and child) at both waves regardless of whether they had nominated these family members as part of their close social support network. Participants with more than one child were instructed to report on the child (aged 13 or older) on whom they relied the most. The family negativity scale included two items (Akiyama et al., 2003): “My (family member) gets on my nerves” and “My (family member) makes too many demands on me,” measured on a 5-point scale ranging from 1 (disagree) to 5 (agree). Composite scores were created by averaging the two-item scores across the four reported relationships (w1: α = .73, w2: α = .74). If a respondent was missing one or more of these four family relationships, composite family quality scores were calculated by averaging only the reported relationships. Due to the large age range of the sample and resulting differing life stages, not all respondents reported on the same family members, reflecting the changing meaning and composition of family across the lifespan. In Table 1, the percentage of respondents in each age group who have a spouse, mother, father, and child are presented.
Depressive Symptoms
Psychological well-being was defined as participants' report of depressive symptoms. The 20-item Center for Epidemiological Studies Depression (CESD) scale (Radloff, 1977) was used at both waves to assess depressive symptoms. Participants reported their experience of depressive symptoms in the past week from 0 (rarely/none of the time) to 3 (most of the time). The items were summed to create a total score (w1: α = .89, w2: α = .89) with higher scores representing greater depressive symptoms.
Demographic Controls
Social support and well-being have been shown to vary by age, gender, education level, race, and marital status (Antonucci, 2001), and thus these demographic variables were included as covariates in all analyses. Participants reported their gender, highest grade of school completed, race, and marital status. Gender was coded as 0 (male) and 1 (female). Respondents with 0 to 7 years of education were determined to be univariate outliers, and were, therefore, collapsed into the lowest category for the continuous education level variable (range 8-17+). Race was coded as 0 (Not White) and 1 (White). Marital Status was coded as 0 (not married) and 1 (married or living with partner).
Analysis Strategy
We used Structural Equation Modeling (SEM) to estimate multi-wave static score models with contemporaneous effects. SEM allows for the simultaneous estimation of multiple equations, which has the advantages of correct standard errors, standardized coefficients, and r-square estimates for the second stage equation (Hooper, Coughlin & Mullen, 2008). SPSS Amos 22 was used to compute model outputs. Three generally accepted fit indices were used to assess the goodness of fit for each model: the chi-square statistic, comparative fit index [CFI] and root-mean-square error of approximation [RMSEA]. Models are considered to be of good fit when the chi-square is above .05, CFI is greater than .95, and RMSEA is less than .05 (Kline, 2010).
Specifically, we examined a two-wave instantaneous effects model, controlling for the effects of both the predictor and outcome variables at Wave 1 and covariates at Wave 2. The model tested causal effects between the predictors (family structure and quality) and outcome (psychological well-being) at Wave 2. Controlling for Wave 1 variables permitted us to examine research questions focused on changes in both the predictors and outcomes over time. Significant interactions were explored with post-hoc analyses to determine the significance of main effects within levels of the moderating variable.
Results
Basic descriptive statistics for the study variables are presented in Table 1. To address both research questions, multi-group SEM (Figure 1) was used to examine instantaneous main effects of family network structure and negativity on well-being separately among younger (aged 18-34), middle-aged (aged 35-49), and older (aged 50+) adults. The longitudinal controls of outcome variables at Wave 1 were included to permit the analysis of change over time. Demographic variables were included as controls at both waves. The model demonstrated good fit on multiple indices: Chi square = 83.9, df = 36; CFI = .99; RMSEA = 0.04. For conciseness, only results related to the two central research questions are presented; however, overall results including those related to demographic and longitudinal controls are noted in Table 2 for younger adults, Table 3 for middle-aged adults, and Table 4 for older adults.
Figure 1.

Model of influence of negativity with family, proportion family, and family network size on depressive symptoms and selfrated health. Not shown: controlled for age, gender, race, education, and marital status. All error terms were allowed to co-vary.
Table 2.
Young Adults (aged 18-34 at wave 1): Unstandardized coefficients and standard error for direct effects of structural equation model.
| YOUNG: N = 268 | Wave 2 Outcome Variables | |||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Proportion Family | Family Network | Family Negativity | Depressive Symptoms | |||||
|
|
|
|
|
|||||
| b | (SE) | b | (SE) | b | (SE) | b | (SE) | |
| Controls: | ||||||||
| Age | .00 | (.00) | .03 | (.03) | .00 | (.01) | -.18 | (.11) |
| Gender | -.01 | (.03) | .80** | (.28) | .20† | (.11) | .15 | (1.12) |
| Race | -.06* | (.03) | -.23 | (.30) | -.04 | (.12) | .41 | (1.19) |
| Education | -.02*** | (.01) | -.08† | (.05) | .00 | (.02) | -.02 | (.21) |
| Marital Status | .14*** | (.03) | 1.36*** | (.32) | .06 | (.13) | -2.36† | (1.28) |
| W1 Proportion Family | .16*** | (.04) | ||||||
| W1 Family Network Size | .16*** | (.04) | ||||||
| W1 Family Negativity | .40*** | (.05) | ||||||
| W1 Depressive Symptoms | .31*** | (.06) | ||||||
| Predictors: | ||||||||
| W2 Proportion Family | 9.88 | (10.40) | ||||||
| W2 Family Network Size | -.29 | (.89) | ||||||
| W2 Family Negativity | 3.26† | (1.87) | ||||||
| W2 Proportion Family × Negativity | -2.41 | (3.46) | ||||||
| W2 Family Network × Negativity | -.02 | (.31) | ||||||
Note. The unstandardized regression coefficients (b, slope) are presented along with the standard error;
p<.10;
p<.05;
p<.01;
p<.001.
Chi square = 83.9, df = 36; CFI = .99; RMSEA = 0.04.
Table 3.
Middle-Aged Adults (Aged 35-49 at wave 1): Unstandardized coefficients and standard error for direct effects of structural equation model.
| MIDDLE AGED: N = 297 | Wave 2 Outcome Variables | |||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Proportion Family | Family Network | Family Negativity | Depressive Symptoms | |||||
|
|
|
|
|
|||||
| b | (SE) | b | (SE) | b | (SE) | b | (SE) | |
| Controls: | ||||||||
| Age | .00 | (.00) | -.04 | (.03) | .00 | (.01) | .06 | (.12) |
| Gender | -.04 | (.00) | .19 | (.27) | .15 | (.10) | -1.04 | (1.11) |
| Race | -.11*** | (.03) | -1.28*** | (.32) | -.04 | (.12) | -1.23 | (1.33) |
| Education | -.01* | (.01) | -.09† | (.05) | .00 | (.02) | -.65 | (.22) |
| Marital Status | .12*** | (.03) | 1.34*** | (.31) | .06 | (.12) | -.12 | (1.33) |
| W1 Proportion Family | .29*** | (.04) | ||||||
| W1 Family Network Size | .28*** | (.04) | ||||||
| W1 Family Negativity | .35*** | (.05) | ||||||
| W1 Depressive Symptoms | .35*** | (.05) | ||||||
| Predictors: | ||||||||
| W2 Proportion Family | 6.36 | (9.60) | ||||||
| W2 Family Network Size | -.16 | (.86) | ||||||
| W2 Family Negativity | 3.52* | (1.62) | ||||||
| W2 Proportion Family × Negativity | -1.40 | (3.96) | ||||||
| W2 Family Network × Negativity | -.17 | (.38) | ||||||
Note. The unstandardized regression coefficients (b, slope) are presented along with the standard error;
p<.10;
p<.05;
**p<.01;
p<.001.
Chi square = 83.9, df = 36; CFI = .99; RMSEA = 0.04.
Table 4.
Older Adults (Aged 50 + at wave 1): Unstandardized coefficients and standard error for direct effects of structural equation model.
| OLDER: N = 281 | Wave 2 Outcome Variables | |||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Proportion Family | Family Network | Family Negativity | Depressive Symptoms | |||||
|
|
|
|
|
|||||
| b | (SE) | b | (SE) | b | (SE) | b | (SE) | |
| Controls: | ||||||||
| Age | .00 | (.00) | -.05* | (.02) | -.02** | (.01) | .12* | (.06) |
| Gender | .01 | (.03) | .56† | (.32) | .05 | (.12) | -.79 | (.86) |
| Race | -.02 | (.03) | .70† | (.39) | .07 | (.14) | .18 | (1.03) |
| Education | .00 | (.01) | .00 | (.05) | -.04† | (.02) | -.34 | (.15) |
| Marital Status | .13*** | (.03) | 1.20*** | (.33) | .06 | (.12) | -.46 | (.92) |
| W1 Proportion Family | .27*** | (.05) | ||||||
| W1 Family Network Size | .36*** | (.04) | ||||||
| W1 Family Negativity | .27*** | (.06) | ||||||
| W1 Depressive Symptoms | .28*** | (.06) | ||||||
| Predictors: | ||||||||
| W2 Proportion Family | 11.89* | (5.04) | ||||||
| W2 Family Network Size | -1.18** | (.43) | ||||||
| W2 Family Negativity | 1.48 | (1.24) | ||||||
| W2 Proportion Family × Negativity | -4.43* | (2.07) | ||||||
| W2 Family Network × Negativity | .45* | (.19) | ||||||
Note. The unstandardized regression coefficients (b, slope) are presented along with the standard error;
p<.10;
p<.05;
p<.01;
p<.001.
Chi square = 83.9, df = 36; CFI = .99; RMSEA = 0.04.
Research Question 1: Do changes in family support network structure (i.e., composition, size) and family negativity influence change in depressive symptoms differently among younger, middle-aged, and older adults?
Change in close family support network structure (i.e., size and composition) was not associated with changes in well-being among young or middle-aged adults but was among older people. We found, consistent with our first hypothesis, that increased family size was not associated with changes in well-being among young or middle-aged adults. However, consistent with expectations, older adults with more family nominated in their close support network reported a decrease in depressive symptoms over time (b = -1.18, β = -.47, p < .01). Turning to the proportion family in close network, contrary to our second hypothesis, change in proportion family in close network was not associated with increased depressive symptoms among young or middle-aged adults. Among older adults, however, increased proportion family in close network was associated with increased depressive symptoms over time. Consistent with our second hypothesis, at Wave 2 older adults with increased proportion of family in their network reported an increase in depressive symptoms (b = 11.89, β = .40, p < .05).
With regards to Hypothesis 3, changes in family negativity were associated with changes in depressive symptoms among young and middle-aged, but not older adults. Among young adults there was a trend towards family negativity being associated with increases in depressive symptoms (b = 3.26, β = .34, p < .10). This pattern was significant among middle-aged adults, with increasing family negativity associated with an increase in depressive symptoms (b = 3.52, β = .32, p < .05). These findings are contrary to our expectation that the association between negativity and well-being would be the strongest among young adults.
Research Question 2: Does change in family negativity moderate links between change in family structure (i.e., composition, size) and change in depressive symptoms across age groups?
Change in family negativity was found to moderate the influence of family structure on changes in depressive symptoms among older, but not young or middle-aged adults. Among young and middle-aged adults, there were no significant interactive effects between changes in family negativity and family network structure on depressive symptom change. However, among older adults both interaction effects examined were significant.
As expected in Hypothesis 4, among older adults, the interaction of proportion family and family negativity was significantly associated with changes in depressive symptoms (b = -4.43, β = -.58, p < .05) as illustrated in Figure 2A. Post-hoc regression analyses were conducted within low and high levels of family negativity to explore the nature of the significant interaction. Lower proportion family significantly predicted a decline in depressive symptoms in the context of low family negativity (b = 7.91, p < .05). In contrast, proportion family did not significantly predict a change in depressive symptoms in the context of high family negativity.
Figure 2.
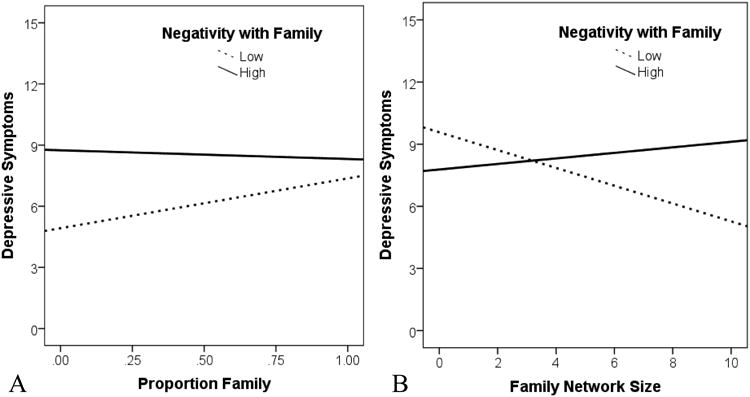
Significant interactions predicting older adults' depressive symptoms at Wave 2. (A) Negativity with family moderated the relationship between proportion family and depressive symptoms, and (B) Negativity with family moderated the relationship between family network size and depressive symptoms.
As demonstrated in Figure 2B, the interaction of close family network size and negativity was significantly associated with changes in older adults' depressive symptoms (b = .45, β = .53, p < .05). Post-hoc regression analyses conducted within low and high levels of family negativity suggest that larger family network size significantly predicted a decline in depressive symptoms in the context of low family negativity (b = -.43, p < .05). In contrast, family network size did not significantly predict depressive symptoms in the context of high family negativity. These significant interactions partially confirmed our moderation hypotheses; however, the moderating effect of change in negativity was significant only among older adults.
Discussion
The influence of attachment, social support and other social relations among infants, children, adolescents and their parents has long been of interest to developmental psychologists (Bowlby, 1982; Collins et al., 2000; Schneider et al., 2001; Levitt et al., 1993a). Among adults, some limited prior theoretical and empirical work has highlighted age differences in family convoys and their differential impact on well-being (Antonucci et al., 2011). The current study furthers research on family implications for well-being over time by examining the interplay of family convoy structure and quality among young, middle-aged, and older adults. Our findings demonstrate that changes in the psychological well-being of young and middle-aged adults is influenced by changes in the qualitative aspects of family relationships; whereas, older adults are more influenced by quantitative aspects of family relationships. In addition to differences found across the lifespan, a more complex picture emerged for older adults in which differential effects emerged for family network size and proportion family in network. In later-life, increasing numbers of family members nominated within one's close social support network and balance of family and friends in this network was found to improve psychological well-being over time, however only in the context of declining family negativity. In sum, these results contribute to an increased understanding of the developmental nature of family support and well-being across the adult lifespan and over time.
Age Implications
Interesting age differences were evident in the main effects of family convoy structure and negativity predicting changes in well-being suggesting important developmental differences. Among young and middle-aged adults only family negativity predicted changes in well-being; whereas among older adults family network composition and size predicted changes in well-being. This suggests age effects in how family convoys influence well-being, with qualitative aspects of support more influential in early to middle adulthood and structural aspects more influential in later adulthood. This highlights developmental differences in the support dynamic. Young and middle-aged adults may have fewer instrumental support needs, but qualitative aspects of relationships are likely to take greater precedence in shaping their well-being over time. In later life people are often in need of more instrumental support, thus explaining why structural characteristics matter more. In addition, because older adults have been shown to have achieved better emotional regulation (Carstensen, Pasupathi, Mayr, & Nesselroade, 2000), they are therefore, less likely to be impacted by relationship quality (i.e., family negativity).
Family Negativity in Young and Middle Adulthood
Among young and middle-aged adults family negativity was associated with increases in depressive symptoms over time, consistent with our expectations and the broader research literature (Kawachi & Berkman, 2001). It is interesting, however, that this effect was significant among middle-aged while only a trend for younger adults. When we consider the patterns in close family members across age groups, this finding suggests the quality of certain relationships may have more impact at different developmental stages. The average young adult reported on relationship quality with all four relationships (spouse, mother, father, and child). On the other hand, the average middle-aged adult reported on spouse, mother, and child, but to a lesser extent father. Whereas the older adult group reported primarily on spouse and child, and rarely had living parents. This may suggest that as children become more salient and parents less salient as close support partners, the implications for well-being become stronger. The young adult group encompasses a wide array of family stages, ranging from 18-year-olds who may still be living at home, to 34-year-olds who may be married and have growing children. Thus, the lack of a strong effect in this group may indicate the variability within this age group and suggest important distinctions between late adolescence and early adulthood in terms of family support. Moreover, the lack of a link between negativity and well-being among the older adult group (who reported primarily on child and spouse) suggests that as parents are no longer living and rates of widowhood increase, quality of relationships are not as influential for well-being. Qualitative aspects of adults' relationships with children may have more nuanced effects, though much of this nuance may be lost in the current study because respondents reported on only one child (their most relied upon), thus reducing the variability in these responses. While negativity influenced changes in middle-aged and young adults' well-being over time, the influence of negativity for older adults depended on the structural context of the convoy.
Close Family Support Network in Late-life
Findings for the number of family members in the support network highlight the beneficial effects of having a larger family convoy in late-life. A greater close family size suggests having more resources to draw on for instrumental support, which becomes increasingly important for well-being in late-life. Typically, researchers recognize that family members provide the types of support that benefit physical health, such as encouragement of healthy lifestyles and discouragement of poor health behaviors, or the provision of caregiving and health related information (Lewis & Rook, 1999; August & Sorkin, 2010). These findings suggest that support from family members is also protective for mental health in late-life, in particular older adults with larger close family networks experienced improvements in psychological well-being in the context of low family negativity. This finding lends support to the body of research emphasizing the importance of family support resources in later-life (Grundy & Henretta, 2006; Walen & Lachman, 2000), yet emphasizes that not just the availability, but the quality, of family support matters when it comes to promoting better well-being.
Proportion Family in Late-life
The finding that greater proportion of family was linked to older adults' improved well-being demonstrates the distinction of relying primarily on family for support versus relying on a balance of family and friends for support. Network diversity (i.e., balance of family and friends) is indeed influential for well-being in later life, consistent with research on the importance of diverse network types (Fiori et al., 2006). This highlights potential risk when older adults rely exclusively on family members for support. However, older adults reporting lower proportion family experienced improvements in psychological well-being only in the context of low family negativity. In effect, when family relationships are good quality (i.e. low negativity), older adults may gain unique benefits from non-family support partners (e.g., confiding in and receiving emotional support from friends) that increase their well-being or resiliency (Sherman, de Vries, & Lansford, 2000).
One explanation for this finding is that older adults with healthy family relationships may be better able to seek out and benefit from diverse social networks. As with the childhood attachment literature (for review see Bretherton, 1992) that suggests that a secure parental attachment base allows the child to better explore their social environment, older adults with higher quality family relationships may be better able to expand beyond family relationships and reap the benefits of both high quality family and friend relationships. This effect may be suggestive of healthy or ‘secure’ patterns of adult attachment (Treboux et al., 2004). These findings suggest that psychological well-being is highest when older adults have a lower proportion of family in network paired with low family negativity. This conclusion may seem counterintuitive, as previous research demonstrates the protective effect of family ties. It is important to note, however, that the mean proportion family in network for older adults in this study was 79%, with the majority of participants having more than half of their network made up of family. Thus, these findings reflect the differences among older adults with primarily family as compared to those with a balance of family and friends in their network. Rather than contradicting the value of family ties, these findings may stress the importance of having a diverse network comprised of a mix of family and friends paired with low family strain.
Future Directions and Limitations
In general, the findings are consistent with the Social Convoy Model which suggests that convoys are both developmental and contextual. A unique contribution of this study is the examination of effects separately for young, middle-aged, and older adults over time. Generally, concurrent relationship support has been found to be more predictive than longitudinal support (Antonucci, 2001). Our specific goal in this study, however, was to examine change over time in order to address long-term implications of family convoys. The hypothesized direct causal lag between social relations and health is proposed to be short (e.g., Umberson, Chen, House, Hopkins, & Slaten, 1996), and because of the 12-year-lag, we were not able to examine direct short-term cross-lag effects, but instead examined indirect longitudinal effects. While the 12-year longitudinal data provides unique insights, it is also a limitation of this study. Future longitudinal research should seek to explore similar questions with multiple waves and gaps of less than five years between each wave in order to further establish the strength and directionality of the associations and interactions addressed in this study.
The family structure variables were limited in that they only assessed number of family and proportion of family within only the closest ten convoy members, not the entire support network. It is also important to note that even though detailed data (i.e., family v. not) are constrained to the first 10 network members nominated by respondents, the median total network size for this sample (at both waves) was 10, and only 37% of the sample reported a network size greater than 10. Therefore, for the majority of the sample, the first 10 people captures their full network. Although we expect the closest ten convoy members to have the most powerful effects on social support (i.e., House, 2001; Akiyama et al., 2003; Antonucci, 2001), future research should consider these questions within the entire support network.
Though its use has been validated and supported by previous research (Akiyama et al., 2003), the negativity scale consisted of only two items and thus could benefit from the inclusion of additional items. Future studies should assess more aspects of negative relationship quality. In light of the current findings about negativity, future studies should examine the effects of negativity within varying levels of positivity, since both have been found to simultaneously occur in relationships. Furthermore, relationship quality was not assessed for all family members listed in the close social network, but instead only for specific targeted relationships, i.e., father, mother, spouse, and child relied on most. In some instances the participants did not have all four of these family members, or the four family members might not necessarily have been included as part of their close social convoy. Future studies should assess the quality and function of relationships with every member listed in the social network so that family convoy and quality variables can be matched. Furthermore, this would allow for the examination of relationship quality more broadly, including both close immediate and extended family members. While the current study contributes to our understanding of the family convoy holistically, future research should continue to examine specific relationships and additionally compare the impact of support received from both family and non-family.
Finally, although this is a relatively racially diverse sample, evidence of cultural distinctions in family convoy structure and family solidarity suggest the importance of examining these questions across cultures (i.e., Ajrouch et al., 2001; Fuller-Iglesias & Antonucci, 2009). As noted above, 67% of the sample was white and 31% black. While this is representative of the Detroit metropolitan area at the time of the Wave 1 data collection (i.e., early 1990's), this is not representative of the ethnic diversity across the country as a whole. Thus, care should be taken when applying these findings across ethnic groups. Future studies should examine similar issues across more representative and specific ethnic groups (i.e., Hispanic and Asian Americans).
Conclusions
This study makes several important contributions to the literature concerning developmental implications of social relations, particularly family convoys, over time. While it has long been understood that social relationships and social support exchanges are complex, the present findings lend specificity and a longitudinal view to our understanding of adult family support relationships. Within the research literature it is too often assumed that family support has a beneficial effect, but the current findings detail a more complex picture. Developmentally, qualitative aspects of family support were influential during early and middle adulthood, whereas quantitative aspects of family support were influential during late adulthood. Moreover, these findings demonstrate that in late-life, when negativity with family is low, there is optimal value to networks with a large family presence and a diverse blend of family and friends, suggesting that the challenges of old age are best handled with a strong and diverse network.
Acknowledgments
Research conducted by Heather Fuller-Iglesias, Human Development and Family Science, North Dakota State University; Noah J. Webster, Institute for Social Research, University of Michigan; and Toni C. Antonucci, Department of Psychology and Institute for Social Research, University of Michigan. This research was supported in part by grants from the National Institute of Mental Health (MH46549 and MH066876) and the National Institute on Aging (AG13490 and AG030569). Special thanks to Kira Birditt and Kristine Ajrouch who provided helpful feedback on earlier drafts of this paper.
Contributor Information
Heather R. Fuller-Iglesias, North Dakota State University
Noah J. Webster, University of Michigan
Toni C. Antonucci, University of Michigan
References
- Adams RG, Blieszner R. Aging well with friends and family. American Behavioral Scientist. 1995;39(2):209. doi: 10.1177/0002764295039002008. [DOI] [Google Scholar]
- Ajrouch KJ, Blandon AY, Antonucci TC. Social networks among men and women: The effects of age and socioeconomic status. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2005;60(6):311–317. doi: 10.1093/geronb/60.6.S311. [DOI] [PubMed] [Google Scholar]
- Ajrouch KJ, Antonucci TC, Janevic MR. Social networks among blacks and whites the interaction between race and age. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2001;56(2):112–118. doi: 10.1093/geronb/56.2.S112. [DOI] [PubMed] [Google Scholar]
- Akiyama H, Antonucci T, Takahashi K, Langfahl ES. Negative interactions in close relationships across the life span. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2003;58(2):70–79. doi: 10.1093/geronb/58.2.P70. [DOI] [PubMed] [Google Scholar]
- Antonucci TC. Hierarchical mapping technique. Generations: Journal of the American Society on Aging. 1986;10(4):10–12. [Google Scholar]
- Antonucci TC. Social relations: An examination of social networks, social support, and sense of control. In: Birren JE, Schaie KW, editors. Handbook of the psychology of aging. 5th. San Diego, CA: Academic Press; 2001. pp. 427–453. [Google Scholar]
- Antonucci TC, Ajrouch KJ, Birditt KS. The convoy model: Explaining social relations from a multidisciplinary perspective. The Gerontologist. 2013;54(1):82–92. doi: 10.1093/geront/gnt118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Antonucci TC, Akiyama H. An examination of sex differences in social support among older men and women. Sex roles. 1987;17(11-12):737–749. doi: 10.1007/BF00287685. [DOI] [Google Scholar]
- Antonucci TC, Akiyama H, Takahashi K. Attachment and close relationships across the life span. Attachment & Human Development. 2004;6(4):353–370. doi: 10.1080/1461673042000303136. [DOI] [PubMed] [Google Scholar]
- Antonucci TC, Birditt KS, Akiyama H. Convoys of social relations: An interdisciplinary approach. In: Bengston V, Silverstein M, Putney N, Gans D, editors. Handbook of theories of aging. New York, NY: Springer Publishing Company; 2009. [Google Scholar]
- Antonucci TC, Birditt KS, Sherman C, Trinh S. Stability and change in the intergenerational family: A convoy approach. Ageing & Society. 2011;31(7):1084–1106. doi: 10.1017/S0144686X1000098X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Antonucci TC, Lansford JE, Akiyama H, Smith J, Baltes MM, Takahashi K, Dartigues JF. Differences between men and women in social relations, resource deficits, and depressive symptomatology during later life in four nations. Journal of Social Issues. 2002;58(4):767–783. doi: 10.1111/1540-4560.00289. [DOI] [Google Scholar]
- August KJ, Sorkin DH. Marital status and gender differences in managing a chronic illness: The function of health-related social control. Social Science & Medicine. 2010;71(10):1831–1838. doi: 10.1016/j.socscimed.2010.08.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berkman LF, Glass T, Brissette I, Seeman TE. From social integration to health: Durkheim in the new millennium. Social Science & Medicine. 2000;51(6):843–857. doi: 10.1016/S0277-9536(00)00065-4. [DOI] [PubMed] [Google Scholar]
- Birditt KS, Antonucci TC. Relationship quality profiles and well-being among married adults. Journal of Family Psychology. 2007;21(4):595–604. doi: 10.1037/0893-3200.21.4.595. [DOI] [PubMed] [Google Scholar]
- Birditt KS, Rott LM, Fingerman KL. ‘If you can't say something nice, don't say anything at all’: Coping with interpersonal tensions in the parent-child relationship during adulthood. Journal of Family Psychology. 2009;23(6):769–778. doi: 10.1037/a0016486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blanchard-Fields F, Coats AH. The experience of anger and sadness in everyday problems impacts age differences in emotion regulation. Developmental psychology. 2008;44(6):1547–56. doi: 10.1037/a0013915. [DOI] [PubMed] [Google Scholar]
- Bookwala J. Marriage and other partnered relationships in middle and late adulthood. In: Blieszner R, Bedford VH, editors. Handbook of aging and the family. 2nd. Santa Barbara, CA: ABC-CLIO; 2012. pp. 91–124. [Google Scholar]
- Bowlby J. Attachment and loss: Attachment. New York: Basic Books; 1982. [Google Scholar]
- Bretherton I. The origins of attachment theory: John Bowlby and Mary Ainsworth. Developmental Psychology. 1992;28(5):759–775. doi: 10.1037/0012-1649.28.5.759. [DOI] [Google Scholar]
- Bronfenbrenner U. Ecology of the family as a context for human development: Research perspectives. Developmental Psychology. 1986;22(6):723–742. doi: 10.1037/0012-1649.22.6.723. [DOI] [Google Scholar]
- Carstensen LL. Motivation for social contact across the life span: A theory of socioemotional selectivity. In: Jacobs JE, editor. Nebraska symposium on motivation: Developmental perspectives on motivation. University of Nebraska Press; 1993. pp. 209–254. [PubMed] [Google Scholar]
- Carstensen LL, Pasupathi M, Mayr U, Nesselroade JR. Emotional experience in everyday life across the adult life span. Journal of personality and social psychology. 2000;79(4):644. doi: 10.1037/0022-3514.79.4.644. [DOI] [PubMed] [Google Scholar]
- Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychological Bulletin. 1985;98(2):310–357. doi: 10.1037/0033-2909.98.2.310. [DOI] [PubMed] [Google Scholar]
- Collins WA, Maccoby EE, Steinberg L, Hetherington EM, Bornstein MH. Contemporary research on parenting: The case for nature and nurture. American Psychologist. 2000;55(2):218–232. doi: 10.1037/0003-066x.55.2.218. [DOI] [PubMed] [Google Scholar]
- Cornwell B, Laumann EO, Schumm LP. The social connectedness of older adults: A national profile. American Sociological Review. 2008;73(2):185–203. doi: 10.1177/000312240807300201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunn J, Slomkowski C, Beardsall L. Sibling relationships from the preschool period through middle childhood and early adolescence. Developmental Psychology. 1994;30(3):315–324. doi: 10.1037/0012-1649.30.3.315. [DOI] [PubMed] [Google Scholar]
- Fast J, Keating NC, Derksen L, Otfinowski P. Characteristics of family/friend care networks of frail seniors. Canadian Journal on Aging/La Revue Canadienne du Vieillissement. 2004;23(1):5–19. doi: 10.1353/cja.2004.0003. [DOI] [PubMed] [Google Scholar]
- Fingerman KL, Birditt KS. Do age differences in close and problematic family ties reflect the pool of available relatives? The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2003;58(2):80–87. doi: 10.1093/geronb/58.2.p80. [DOI] [PubMed] [Google Scholar]
- Fingerman KL, Hay EL, Birditt KS. The best of ties, the worst of ties: Close, problematic, and ambivalent social relationships. Journal of Marriage & Family. 2004;66(3):792–808. doi: 10.1111/j.0022-2445.2004.00053.x. [DOI] [Google Scholar]
- Fiori KL, Antonucci TC, Cortina KS. Social network typologies and mental health among older adults. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2006;61(1):25–32. doi: 10.1093/geronb/61.1.p25. [DOI] [PubMed] [Google Scholar]
- Fuller-Iglesias H, Antonucci TC. Social Networks, Familism, and Well-being among Older Adults in Mexico. Gerontological Society of America Scientific Meeting 2009 [Google Scholar]
- Fung HH, Yeung DY, Li K, Lang FR. Benefits of negative social exchanges for emotional closeness. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2009;64B(5):612–621. doi: 10.1093/geronb/gbp065. [DOI] [PubMed] [Google Scholar]
- Furman W, Buhrmester D. Children's perceptions of the personal relationships in their social networks. Developmental Psychology. 1985;21(6):1016–1024. doi: 10.1037/0012-1649.21.6.1016. [DOI] [Google Scholar]
- Gotlib IH, Hammen CL, editors. Handbook of depression. Guilford Press; 2008. [Google Scholar]
- Grundy E, Henretta JC. Between elderly parents and adult children: A new look at the intergenerational care provided by the ‘sandwich generation’. Ageing & Society. 2006;26(5):707–722. doi: 10.1017/s0144686x06004934. [DOI] [Google Scholar]
- Gupta V, Korte C. The effects of a confidant and a peer group on the well-being of single elders. International Journal of Aging and Human Development. 1994;39(4):293–302. doi: 10.2190/4yyh-9xau-wqf9-apvt. [DOI] [PubMed] [Google Scholar]
- Haines VA, Beggs JJ, Hurlbert JS. Contextualizing health outcomes: Do effects of network structure differ for women and men? Sex Roles. 2008;59(3-4):164–175. doi: 10.1007/s11199-008-9441-3. [DOI] [Google Scholar]
- Hooper D, Coughlan J, Mullen MR. Structural equation modeling: Guidelines for determining model fit. Electronic Journal of Business Research Methods. 2008;6(1):53–60. [Google Scholar]
- Kahn RL, Antonucci TC. Convoys over the life course: Attachment, roles, and social support. In: Baltes PB, Brim O, editors. Life-span development and behavior. Vol. 3. New York: Academic Press; 1980. pp. 253–268. [Google Scholar]
- Kawachi I, Berkman LF. Social ties and mental health. Journal of Urban Health: Bulletin of the New York Academy of Medicine. 2001;78(3):458–467. doi: 10.1093/jurban/78.3.458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline RB. Principles and practice of structural equation modeling. 3rd. New York: Guilford Press; 2010. [Google Scholar]
- Krause N, Rook KS. Negative interaction in late life: Issues in the stability and generalizability of conflict across relationships. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2003;58(2):88–99. doi: 10.1093/geronb/58.2.p88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levitt MJ. Social relations in childhood and adolescence: The convoy model perspective. Human Development. 2005;48(1-2):28–47. doi: 10.1159/000083214. [DOI] [Google Scholar]
- Levitt MJ, Guacci-Franco N, Levitt JL. Convoys of social support in childhood and early adolescence: Structure and function. Developmental Psychology. 1993a;29(5):811–818. doi: 10.1037/0012-1649.29.5.811. [DOI] [Google Scholar]
- Levitt MJ, Weber RA, Guacci N. Convoys of social support: An intergenerational analysis. Psychology and Aging. 1993b;8(3):323–326. doi: 10.1037/0882-7974.8.3.323. [DOI] [PubMed] [Google Scholar]
- Lewis MA, Rook KS. Social control in personal relationships: Impact on health behaviors and psychological distress. Health Psychology. 1999;18(1):63–71. doi: 10.1037//0278-6133.18.1.63. [DOI] [PubMed] [Google Scholar]
- Mallers MH, Charles ST, Neupert SD, Almeida DM. Perceptions of childhood relationships with mother and father: Daily emotional and stressor experiences in adulthood. Developmental Psychology. 2010;46(6):1651–1661. doi: 10.1037/a0021020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merz EM, Schuengel C, Schulze HJ. Intergenerational relations across 4 years: Well-being is affected by quality, not by support exchange. The Gerontologist. 2009;49(4):536–548. doi: 10.1093/geront/gnp043. [DOI] [PubMed] [Google Scholar]
- Newsom JT, Nishishiba M, Morgan DL, Rook KS. The relative importance of three domains of positive and negative social exchanges: A longitudinal model with comparable measures. Psychology & Aging. 2003;18(4):746–754. doi: 10.1037/0882-7974.18.4.746. [DOI] [PubMed] [Google Scholar]
- Newsom JT, Mahan TL, Rook KS, Krause N. Stable negative social exchanges and health. Health Psychology. 2008;27(1):78–86. doi: 10.1037/0278-6133.27.1.78. [DOI] [PubMed] [Google Scholar]
- Overbeek G, Stattin H, Vermulst A, Ha T, Engels RC. Parent-child relationships, partner relationships, and emotional adjustment: A birth-to-maturity prospective study. Developmental Psychology. 2007;43(2):429–437. doi: 10.1037/0012-1649.43.2.429. [DOI] [PubMed] [Google Scholar]
- Peek MK, Lin N. Age differences in the effects of network composition on psychological distress. Social Science & Medicine. 1999;49(5):621–636. doi: 10.1016/s0277-9536(99)00139-2. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1(3):385–401. doi: 10.1177/014662167700100306. [DOI] [Google Scholar]
- Rook KS, Sorkin DH, Zettel LA. Stress in social relationships: Coping and adaptation across the life span. In: Lang FR, Fingerman KL, editors. Growing together: Personal relationships across the lifespan. Cambridge, UK: Cambridge University Press; 2004. pp. 210–239. [Google Scholar]
- Schneider BH, Atkinson L, Tardif C. Child–parent attachment and children's peer relations: A quantitative review. Developmental Psychology. 2001;37(1):86–100. doi: 10.1037/0012-1649.37.1.86. [DOI] [PubMed] [Google Scholar]
- Sechrist J, Suitor JJ, Pillemer K, Gilligan M, Howard AR, Keeton SA. Aging parents and adult children: Determinants of relationship quality. In: Blieszner R, Bedford VH, editors. Handbook of families and aging. 2nd. Santa Barbara, CA: Praeger; 2012. [Google Scholar]
- Shaw BA, Krause N, Liang J, Bennett J. Tracking changes in social relations throughout late life. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2007;62(2):90–99. doi: 10.1093/geronb/62.2.s90. [DOI] [PubMed] [Google Scholar]
- Shaw BA, Krause N, Chatters LM, Connell CM, Ingersoll-Dayton B. Emotional support from parents early in life, aging, and health. Psychology and aging. 2004;19(1):4. doi: 10.1037/0882-7974.19.1.4. [DOI] [PubMed] [Google Scholar]
- Sherman AM, de Vries B, Lansford JE. Friendship in childhood and adulthood: Lessons from across the lifespan. International Journal of Aging & Human Development. 2000;51(1):31–51. doi: 10.2190/4qfv-d52d-tpyp-rlm6. [DOI] [PubMed] [Google Scholar]
- Thoits PA. Mechanisms linking social ties and support to physical and mental health. Journal of Health and Social Behavior. 2011;52(2):145–161. doi: 10.1177/0022146510395592. [DOI] [PubMed] [Google Scholar]
- Treboux D, Crowell JA, Waters E. When “new” meets“old”: Configurations of adult attachment representations and their implications for marital functioning. Developmental Psychology. 2004;40(2):295–314. doi: 10.1037/0012-1649.40.2.295. [DOI] [PubMed] [Google Scholar]
- Turner RJ, Avison WR. Status variations in stress exposure: Implications for the interpretation of research on race, socioeconomic status, and gender. Journal of Health & Social Behavior. 2003;44(4):488–505. doi: 10.2307/1519795. [DOI] [PubMed] [Google Scholar]
- Umberson D, Chen MD, House JS, Hopkins K, Slaten E. The effect of social relationships on psychological well-being: Are men and women really so different? American Sociological Review. 1996;61(5):837–857. doi: 10.2307/2096456. [DOI] [Google Scholar]
- Walen HR, Lachman ME. Social support and strain from partner, family, and friends: Costs and benefits for men and women in adulthood. Journal of Social & Personal Relationships. 2000;17(1):5–30. doi: 10.1177/0265407500171001. [DOI] [Google Scholar]
- Ward RA, Spitze G, Deane G. The More the Merrier? Multiple Parent‐Adult Child Relations. Journal of Marriage and family. 2009;71(1):161–173. doi: 10.1111/j.1741-3737.2008.00587.x. [DOI] [Google Scholar]