

Abstract
The British colonization of New Zealand after 1840 was marked by an unusual concern compared to other settler colonies for incorporating the indigenous population Māori population into the new society. But despite a continuing political rhetoric of protection and sovereignty Māori have historically had lower living standards and, since the 1920s, higher rates of incarceration than European-descended New Zealanders (Pākehā). In this paper we examine differences between Māori and Pākehā over 130 years using prison records. Aggregate data from the Ministry of Justice show long-term change and differences in incarceration rates. Using a dataset of all extant registers of men entering New Zealand prisons we show change over time in convictions and in height. The adult statures of Māori and Pākehā were similar for men born before 1900 but marked differences emerged among cohorts born during the twentieth century. By World War II the gap in adult stature widened to around 3 cm, before narrowing for men born after World War II. Periods of divergence in stature are paralleled by divergence in fertility and indicators of family size, suggesting the possibility that increasing fertility stressed the economic situation of Māori families. The prison evidence suggests that inequalities in ‘net nutrition’ between Māori and Pākehā are long-standing but not unchanging, indeed they increased for cohorts born into the early 20th century. A subset of the data describing adolescents confirms that among those born after 1945 the ethnic differential was already visible by the age of 16 years.
Keywords: Heightm New Zealandm Māorim Anthropometric historym Physical standard of living
1. Introduction
Long-term change in the health of families is a key indicator of changing living standards. Unfortunately few measures of health and living standards are consistent over several decades. A large literature has established that a good measure of changing health and living standards is average stature (Steckel, 2008). Yet in New Zealand, only mortality statistics have been published annually in official series allowing researchers to document changing patterns of health for Māori and Pākehā. Anthropometric indicators provide another class of evidence about physical well-being. Since the 1970s modern health surveys in New Zealand have documented change and variation in height and weight, but until recently there has been little accessible historical evidence.1 As in other countries, the most important sources in New Zealand for studying height and weight in the past are military, prison and school records.
New Zealand military records have been used to show that adult stature declined or was stagnant for cohorts born during the middle and late nineteenth century (Inwood, Oxley and Roberts, 2012). And yet military records have some weaknesses for our purpose. They draw disproportionately from the tallest and fittest, and in many periods they under-represent the indigenous Māori population. It is helpful to examine a different source that reflects a slightly different subset of the population. Prison records also describe significant numbers of adolescents too young for enlistment in the military. The pattern of child growth in late adolescence and into early adulthood is largely undocumented in other sources.
The timing and magnitude of stature growth in adolescence and young adulthood can vary significantly in different economic and social conditions. Historically, the growth of younger children (ages 0–12) has often been compromised by repeated bouts of infectious disease or inadequate food intake. Young men’s adolescent growth has more often been restrained by diets inadequate to sustain both growth in stature and the high levels of physical activity that were historically required in agriculture and industry. Thus, the stature of men entering prison in their late teens and early twenties—when they are potentially still growing—can illustrate the living standards of young men and patterns of well-being for different groups in society.
One final advantage of prison records is their continuity. Crimes are committed, and people are admitted to prison, every year. In contrast, the generation of military personnel records tends to be inconsistent over time as military forces expand during major conflicts and downsize subsequently. Prison records thus permit a continuity of both birth and measurement cohorts. For all of these reasons prison records provide a useful source for the study of family health in New Zealand. The use of prison data for biological and medical research has a long and distinguished history in Britain and the United States, although not yet in New Zealand (Carpenter, 2006; Dunlop, 1899; Hall, et al., 2012; Parssinen, 1974; Rector, 1929).
We are especially interested to examine the prison evidence of physical well-being during the early decades of the twentieth century. In the 1890s New Zealand was hit by an economic depression at the same time as the urban population grew rapidly. These economic changes left a permanent imprint on the bodies of men growing up in that era, both Māori (indigenous) and Pākehā (European settlers). While Pākehā stature slowly recovered from the early twentieth century, the Māori experience was quite different. As the Māori population grew rapidly the stature of Māori and Pākehā men diverged around 1900 and grew to a point where Māori men stood nearly an inch shorter than Pākehā. These gaps did not start to close until around World War II.
2. Stature as a measure of health
Stature is a summary measure of the effect of nutrition, environmental conditions, disease, and physical workload on the body during childhood- and early adulthood-growth (Bogin, 1999; Eveleth & Tanner, 1990). Sustained nutritional deficits while a person is growing result in individual stature falling short of maximum potential height. The human body puts calories to the immediate task of replenishing energy and fighting disease, before it can grow taller. If a growing person is persistently sick or expending more calories than they take in, growth will slow. When these nutritional deficits are widespread across the population, average stature will fall (Jelenkovic, et al., 2011; Silventoinen, 2003).
There are three main causes of nutritional deficits, which while analytically separate are not mutually exclusive: (1) limitation in the availability of calories, (2) persistent bouts of infectious disease while energy intake is constant, (3) elevated energy expenditure while energy intake and disease exposure are constant. The incorporation of energy expenditure and loss, alongside food intake, motivates the concept of ‘net nutrition’ (Steckel, 1986).
As a summary measure subject to several influences changes in the average stature of a population do not identify the causes of change. Rather, changes in average stature show when different cohorts, which are presumed to have the same genetic potential for achieving a particular height, have grown at different rates. Once these periods of changing stature are identified, the contemporaneous influences on net nutrition must be investigated to identify the potential causes of changing stature. Since the 1970s stature has been widely and increasingly used to measure the biological standard of living in an historical and comparative context (Floud, Wachter, & Gregory, 1990; Steckel, 2008; Steckel, 2013).
3. Historiographical Context
One of the most significant findings by anthropometric historians has been that the stature of men in North America and parts of Western Europe stagnated and in many cases fell during the late nineteenth century, and only recovered in the twentieth century (Haines, 2004; Komlos, 1998).2 Early industrialization in the United States, for example, contributed to a decline in the stature of Americans born from the 1820s to the 1840s and again later in the century (Haines, Craig and Weiss, 2003; Komlos 1996; Maloney and Carson, 2008; Steckel and Haurin, 1995; Zehetmayer, 2011). Similar patterns are observed in Canada and to some extent in South Africa (Cranfield and Inwood, 2007; Inwood and Masakure 2013). Neither is there evidence of increasing stature in Argentina or Peru (Baten, Pelger, and Twrdek, 2009; Salvatore 2007).
In many of these jurisdictions industrial and/or urban growth meant that despite rising incomes, health-related infrastructure often could not keep pace with population growth. Moreover nutrient-dense food became less affordable; protein deficient diets—especially deficient in milk protein — may have contributed to declines in stature (Baten & Murray, 2000; Koepke & Baten, 2005). In Australia men were taller than European-descended men in North America and Europe. Yet Australian men born in the long economic depression of the 1880s and 1890s may have been shorter than their Australian peers born in the 1870s or early 20th century, although the issue is complicated by differences among the Australasian colonies (Cranfield and Inwood, 2015b; de Souza, 1994; Inwood, Maxwell-Stewart and Oxley, 2014; Nicholas, Gregory, & Kimberley, 1998; Shlomowitz, 2007; Whitwell & Nicholas, 2001).
Was New Zealand different? At first glance, late nineteenth century New Zealand was a healthy country with non-monetary measures suggesting a high standard of living. The New Zealand Official Yearbook for 1912, for example, claims the lowest infant mortality rates anywhere in the world, detailing how infant mortality started declining in the 1890s (Dominion of New Zealand, 1912; Mein Smith, 1991). Population density in New Zealand cities was low compared to population density elsewhere (Ferguson, 1994). Income per-capita also compared favourably with other developed countries. By 1938 New Zealand’s GDP per capita, adjusted for purchasing power parity, was the highest in the world (Greasley & Oxley, 1999, 2009).
Society-wide averages, of course, cannot speak to distributional questions. In a settler economy such as New Zealand, a particularly important question is how colonial settlement affected the health and physique of the indigenous Māori population. International comparisons of indigenous and European-descended stature are limited. North American evidence suggests indigenous populations continued to have adequate protein in their diets because they were more rural (Komlos, 2003; Prince & Steckel, 2003; Steckel & Prince, 2001). Australian indigenous men born between the 1890s and 1920s experienced no improvement in average height, while white stature rose from the early twentieth century after decline during the late nineteenth century (Nicholas, et al., 1998).
There is limited evidence about Māori health prior to and during colonisation. Government reports from the 1880s and 1890s suggest Māori health was quite poor. Tuberculosis, for example, was quite common among Māori living in damp conditions and close proximity to their neighbours (Dow, 1999). During the same period Māori population declined significantly, reaching a nadir of 42,000 people in 1896, a halving of the population in 60 years according to the best estimates (Pool, 1991). This decline is consistent with the hypothesis of deteriorating health under the impact of colonization. The Māori population recovered rapidly in the twentieth century, with delayed declines in fertility, compared to the Pākehā population.
While the Māori population recovered rapidly after 1900, the New Zealand government and Māori leaders were concerned about continuing poor health in the early twentieth century (Lange, 1999). Yet the nature of the concern had shifted from population decline (a “dying race”) to morbidity among the living. High rates of tuberculosis among Māori were a particular concern before World War II (MacIntyre, 1938; Myers, 1937). There had been some rural-to-urban migration in earlier decades but Māori urbanization was especially rapid after World War Two. Pool (1991, 133) observes that this was “arguably the most accelerated shift for a national population anywhere”.3 Rural residence is likely to have benefited Māori through a degree of isolation from some infectious diseases. Yet when medicine became more effective in the early twentieth century, rural Māori likely suffered by comparison through poorer access to medical care and continued poor living conditions. In response to these issues the New Zealand government appointed doctors to serve Māori communities in the inter-war era. They documented outbreaks of infectious disease that hit remote Māori communities, and contributed to significantly higher mortality rates in Māori in the 1920s and 1930s (Department of Health, 1939).
Māori migration to New Zealand cities in the 1950s and 1960s was well-timed to improve Māori health. Urban epidemics of infectious disease were now rare, and cities provided greater access to modern medical care. Yet since the 1950s researchers have documented significant disparities in Māori and European health, measured by both morbidity and mortality (Durie, 1998; Rose, 1960, 1972; Tobias, Blakely, Matheson, Rasanathan, & Atkinson, 2009). While health inequality appears to have been persistent the form of those inequalities has changed. The gap in Māori and Pākehā health today reflects that both groups have been through an epidemiological transition. Chronic diseases, such as cancer and cardiovascular conditions, are the major causes of death for both Māori and Pākehā. However, the burden is significantly higher for Māori. Age-specific mortality rates for cardiovascular conditions are around twice as high in Māori as Pākehā (Robson & Harris, 2008).
Mortality from cardiovascular causes—such as heart attack, stroke, diabetes, or hypertension—can be related to both height and weight. A significant amount of research has shown that nutritional conditions in the growth period (from 0–20 years of age) that lead to short stature are also implicated in later cardiovascular mortality (Lawlor, Ben-Shlomo, & Leon, 2004). Nutrition and physical activity in adulthood is also indicative of later cardiovascular mortality. Obesity and low levels of physical activity are significant adult causes of early mortality from circulatory conditions (Gillman, 2004). Since Māori mortality from cardiovascular conditions has been high, it is important to understand how stature—an indicator of nutrition during the growth period—changed over time.
4. New Zealand prisons and their data
The development of penal institutions in New Zealand was heavily influenced by the British and Australian experience (Pratt, 1993). The example of Australian penal settlement meant that New Zealand policy sometimes was formed in reaction to perceived excesses of British and Australian prisons. After the establishment of British authority in 1840, the unitary colonial government was technically in charge of prisons. In practice, local authority reigned. A shortage of actual structures to hold prisoners saw approximately 100 people transported to Tasmania between 1840 and 1854. The formation of the New Zealand provincial governments in 1853 saw those governments take over responsibility for penal policy; major prisons were established in the “four main centres”: Auckland, Wellington, Christchurch, and Dunedin. The provincial governments put a low priority on prison building. A royal commission in 1868 found over-crowding and poor administration, concluding with a call for a re-centralized prison administration.
Prison administration was re-centralized in 1876 after the abolition of the provincial governments. Captain Arthur Hume, recruited from England, became the first national inspector-general of prisons in 1880; he introduced a strict system of “efficiency, economy and uniformity” in prisons which were meant to be a “reformative deterrent.” Hume’s tenure witnessed a major expansion of the physical capital of the New Zealand prison system, with new prisons built at Mount Cook in Wellington, and Mount Eden in Auckland in the 1880s. A new Dunedin prison was completed in 1897. Hume was served throughout the New Zealand prison system by a significant number of men with experience in colonial conflicts with Māori during the 1860s and 1870s (Belich, 1987; Egarr, 2012).
Hume set a pattern of long tenure among New Zealand prison commissioners when he retired in 1909. The two commissioners who followed Hume, Charles Matthews (1912–1924), and Bert Dallard (1925–49) oversaw a turn towards a more rehabilitative system. Matthews appointed school teachers to prisons, and started prison farms which Dallard expanded as an economy measure during the Great Depression and World War II. Sam Barnett followed Dallard from 1949–1970. Under Barnett’s stewardship penal policy developed more systematic and professional rehabilitation. In the 1950s Barnett introduced rehabilitative reforms largely under his own initiative. In the 1960s a liberal National Party Justice Minister, Ralph Hanan, took a personal interest in improving conditions in prisons. Hanan and Barnett’s aim to improve prison conditions were frustrated by a rapid rise in prison admissions in the 1960s, which was attributed by many contemporary observers to Māori urban migration (M. Jackson, 1988).
Extant registers from New Zealand prisons are our principal source of information on height. We have collected data on all the New Zealand-born individuals in prison registers that have been transferred to Archives New Zealand. As can be seen from Figure 1, these records constitute a minority of all prison records. In each year our data encompass no more than 1/8 of the total number of distinct people admitted to prison. We rely heavily on the records of the New Plymouth and Napier prisons (Table 1). They were at no time the major prisons in the country but they have the considerable advantage of being located in close physical proximity to areas with substantial Māori populations.4 Registers for the largest prisons in the four main centres, by and large, have not been transferred to Archives New Zealand.5 We also include some data from the Police Gazettes, which reprinted identifying details, including stature, from the admission register in a monthly bulletin sent to all police stations. The purpose of the Gazette was to alert police to potential recidivists in their midst.
Figure 1.
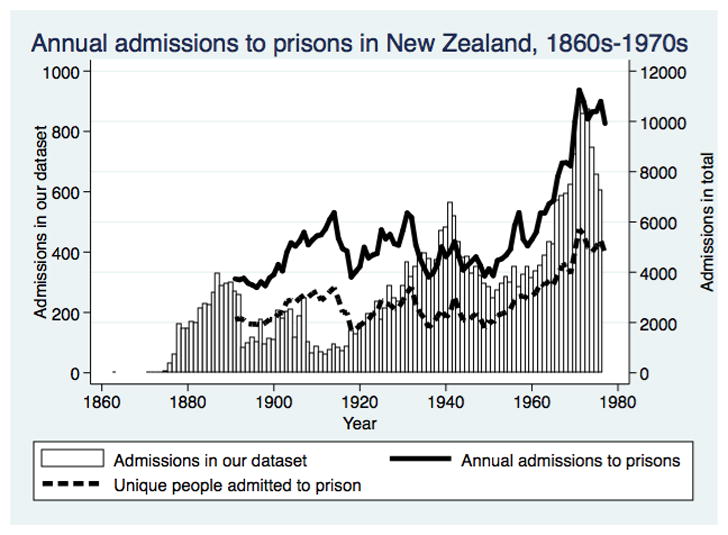
Table 1.
Prisons included in the sample
| Prison | Number of admissions |
|---|---|
| Napier | 11,484 |
| New Plymouth | 7,371 |
| Witako | 3,307 |
| Wanganui | 3,207 |
| Prison unknown, data from photographs of prisoners | 1,184 |
| Auckland | 774 |
| Tolaga Bay | 348 |
| Onehunga | 341 |
| Wellington | 301 |
| Whangaroa | 234 |
| Lyttleton | 205 |
| Dunedin | 203 |
| Lincoln | 135 |
| Addington | 97 |
| Gisborne | 91 |
| Nelson | 50 |
| Timaru | 47 |
| Invercargill | 44 |
| Hokitika | 42 |
| Oamaru | 35 |
| Picton | 23 |
| Shortland | 20 |
| Tauranga | 17 |
| Westport | 15 |
| Mount Cook | 15 |
| Opotiki | 10 |
| Wairoa | 9 |
| Awanui | 8 |
| Lawrence | 7 |
| Rotorua | 7 |
| Clyde | 5 |
| Greymouth | 3 |
| Naseby | 3 |
| Reefton | 3 |
| Woodville | 2 |
| Arrowtown | 2 |
| Ashburton | 2 |
| Hampden | 1 |
| Newcastle | 1 |
|
| |
| Total | 29,653 |
Release and potential recidivism come last in the sequence of events that may lead a person to be incarcerated. Patterns of criminal convictions and incarceration changed significantly in New Zealand over a century (Figure 2). We use convictions in the Magistrates Court as an indicator of changing patterns of crime and punishment. Magistrates Courts handled the vast majority of criminal cases in New Zealand. In 1871 the Magistrates Courts handled 15,606 cases, increasing to 31,983 in 1906 and 57,579 in 1957. By comparison the Supreme Court handled fewer than 400 cases a year before the 1920s. Extensive statistics on the courts’ annual workload and decisions were presented annually in the official publications Statistics of New Zealand in the nineteenth century, from 1907 to 1920 Statistics of the Dominion of New Zealand, and from 1920 to 1951 Report on the Justice Statistics of the Dominion of New Zealand. After 1951 the series is not always consistent with the earlier statistics, and thus we terminate the series at 1951, although our dataset of admissions extends into the mid-1970s.
Figure 2.

We report the number of cases heard in the Courts about male defendants—separated into Māori and Pākehā —for years in which a census was taken (quinquennially after 1881, excepting 1931 and 1941). In the same manner, we also report the number of Māori and Pākehā prisoners received into prison. It should be noted that individuals could be, and were, received multiple times in a year, however statistics on “distinct prisoners” were less consistently recorded. Although some boys did commit crimes and were tried in the Magistrates Court, the numbers were small. We define the population at risk of offending and being incarcerated as males 15 and older. Marital status was not consistently recorded in New Zealand prison registers. For those for whom it was available, 58% were single, 32% married or otherwise partnered, and the remaining 10% divorced, separated, or widowed. The prison population, in other words, was young and composed of men less likely to be married than men of the same age in the general population.
There are distinct differences in the historical trajectory of convictions and imprisonment for Māori and Pākehā (Figure 2). Pākehā conviction and incarceration rates were initially much higher than Māori rates, with many Pākehā men imprisoned in the 1870s and 1880s for crimes such as assault. In a frontier society many disputes were settled violently (though compared to the United States fatalities were rare). Yet as Pākehā society urbanized in the late nineteenth century conviction rates dropped sharply, before rising again between after 1892. Public sentiment against alcohol in this period led to more prosecutions and convictions for offences related to drunkenness (Fairburn, 1989). Māori conviction and incarceration rates were much lower than Pākehā until the turn of the twentieth century, when many Māori men were also convicted of offences relating to drunkenness. Increasing Māori conviction rates also reflected a gradual loss of Māori sovereignty and its replacement by Pākehā authority. Arrests and convictions were a very important manifestation of governmental authority (Bull, 2004; Hill, 1995). From around 1911 Māori conviction rates in the Magistrates Courts were similar to Pākehā rates. Māori incarceration rates, however, only rose significantly after 1916, and thereafter remained significantly higher than for Pākehā. Thus, for the same level of convictions Māori had a higher chance of going to prison.
Thus, we begin our analysis with 28,292 male prison records. We include the records of those older than 13 years in order to be able to identify the age at which adult or maximum stature was reached. In well-nourished modern populations most men attain adult height before age 20 (Bogin, 1999). Thus evidence of men still growing in their late teens is, in itself, an indicator of living standards below current ones. We exclude men older than 50 years from our analysis of height in order to minimize any complication arising from the diminution of height at advanced ages. We restrict our sample to those born in New Zealand so that we can attribute height entirely to nutritional conditions in New Zealand. While immigrants may have spent much of their life in New Zealand, their exact dates of immigration are unknown. After exclusions for missing information and age we are left with the 26,611 records for males between 13 and 50 years of age with information on age, birth date, birth place, occupation and height. We are careful to distinguish between men and their records because some men appeared more than once because of multiple incarcerations.
We distinguish men who were entirely or largely of European descent (Pākehā) from the indigenous Māori population indigenous by descriptions of nativity made in the prison registers themselves. The nativity descriptions reflect a crude “blood quantum” concept with some men described as being between ¼ and ¾ Māori. Others were merely described as Māori, and we have no way of knowing whether these men were in fact “part Māori” as well. In the nineteenth century it seems likely that some of the Māori not noted as being part-Māori were “full-blooded.” But there has been significant inter-racial marriage in New Zealand since British arrival, and it is uncertain how many men showing up after World War II are “full-blooded” (Callister, Didham, & Potter, 2005; Wanhalla, 2008). Our analyses take all men indicated as Māori, no matter the blood quantum noted, as Māori. This interpretation is a social one, that being noted as Māori of whatever proportion reflects something about the origins of that person. The reporting of someone as Māori points to someone who lived within and identified with the indigenous community, growing up in a Māori environment. This social and environmental influence is what we wish to capture.
Family context is important in understanding stature, since children are initially totally dependent on the resources provided to them by their family, in order to grow. In adolescence, when humans go through the second major growth spurt of their lives, family resources and needs are again crucial in determining how close people will come to reaching their potential height. Adolescent children whose parents can provide them with adequate nutrition for daily living and physical growth are able to both eat sufficient food, and expend less energy by remaining in school and out of the workforce longer. Adolescents who enter the labour force to contribute to family income are often living in a family environment where incomes—and thus expenditure on food—are variable, and enter the labour force without completing their schooling.
And yet, leaving school early to enter the workforce may have complex consequences. Additional resources from an added worker are likely to be helpful, and as a worker the individual may have a strong claim on additional resources. This might lead to some catch-up growth on the part of the young worker. On the other hand, particularly in the early twentieth century, the paid employment available to adolescents with limited schooling was often physically demanding, working as an agricultural or industrial labourer. In early twentieth century New Zealand, Māori boys were less likely to attend secondary school, and tended to work in less-skilled occupations when they entered the labor force (Barrington, 2008; Sutherland, 1935).
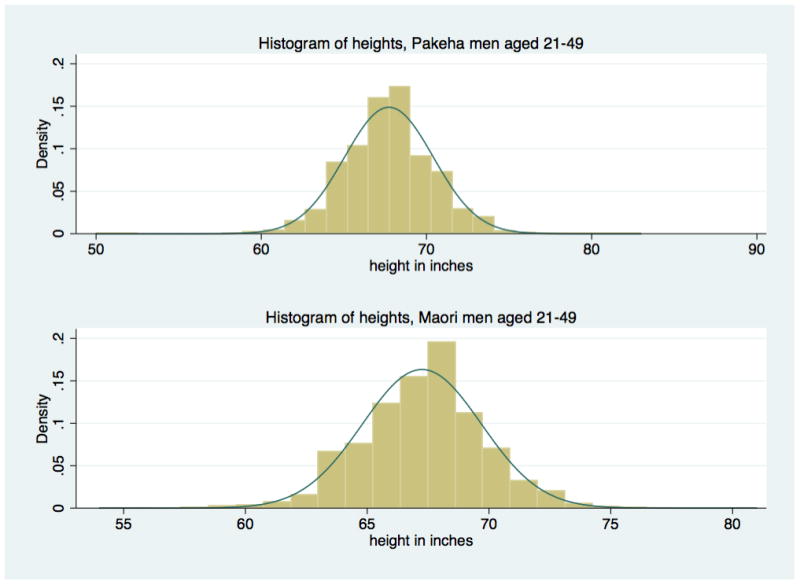
The near-normality of height distribution for those born in New Zealand and over the age of 21 is clear from Figures 3 and 4. Admittedly, there are deviations from a tendency of the distributions to approach normality. The proportion of people reporting the height of 71 inches (180cm) is smaller than expected. It is likely that this is a function of heights being rounded up to 6 feet (72 inches), and reflects instances of imprecise measurement. The second exception for height is a small but noticeable under-representation of those at around 170cm or 5 foot 9. Some heaping around unit values of measurement is evident.
Figure 3.
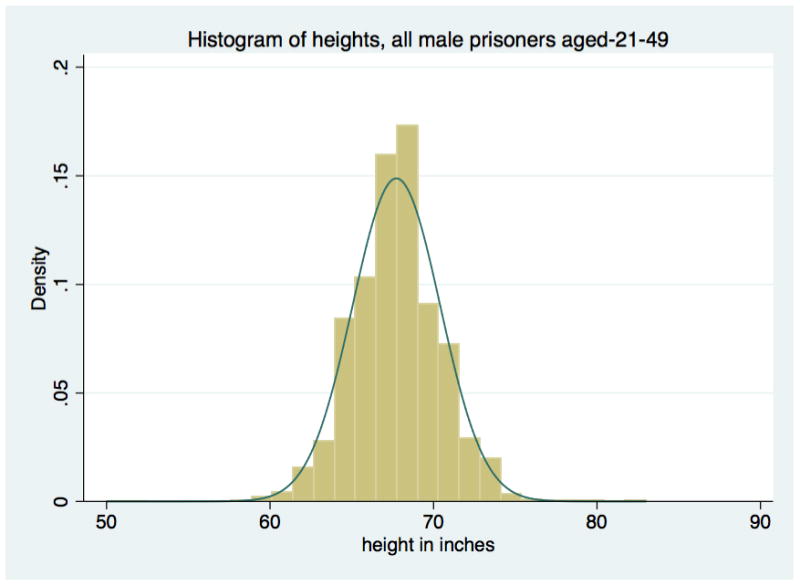
Figure 4.
5. Ethnic differences in the patterns of physical growth
Our goal in the analysis is to assess the extent of social and ethnic differentials, their change over time and the evolution of stature through adolescence and into adulthood. An overview of the experience of stature is provided in Figure 5 by the rolling average of physical stature for men 21 years or older. Here the data are organized by date of birth. Those noted as indigenous—Māori—were significantly shorter than the European-descended Pākehā in the twentieth century. But the average stature of the two ethnic groups overlaps until the early twentieth century, after which there is a growing divergence. After 1900 Pākehā stature began to grow (albeit slowly at first) but Māori stature did not begin to increase until those born in the 1920s, and even then the increase in stature from one Māori cohort to another continued to fall behind Pākehā. This pattern largely replicates findings from an analysis of the same cohorts measured in World War I and World War II records (Inwood, Oxley, & Roberts, 2014).
Figure 5.

Hypothesis-testing in a multiple regression framework provides further insight. We capture change over time by identifying decade-long birth cohorts. These reflect the trends visible in Figure 5 and preserve sufficient sample size at each age for an identification of physical growth from early identification into adulthood.
We examine the influence of socio-economic status via occupations organized into seven classes: professional and managerial (1 per cent of the sample), farmer (2 per cent), farm labourer (12 per cent), other labourers and servants (49 per cent), clerical and sales (9 per cent) and skilled workers in manufacturing, transport and utilities (29 per cent). Records denoting unemployed, disability, student and other conditions not associated with work are assigned to a small miscellaneous category. Our occupational categories are derived from the HISCO coding scheme (van Leeuwen, Maas, & Miles, 2002). The large share of labourers likely reflects both an imprecision and lack of curiosity in recording, and also the low socioeconomic status of prisoners. Skilled and semi-skilled manufacturing workers are the omitted category in the estimation.
The prisoner’s occupational class is assumed to correlate with his father’s occupational class, giving an indirect measurement of the nutritional circumstances in which the prisoner grew up. Occupation is a very rough socio-economic indicator. The presumption of intergenerational persistence further reduces precision, as does any tendency for stature to influence an individual’s choice of occupation.6 Nevertheless, in the absence of other indicators we examine the hypothesis that these occupation-based socio-economic groupings capture the net effect of various influences on adult height.
We hypothesize that rural occupations indicate access as children to a lower relative price of food and limited exposure to infectious disease. The professional and clerical occupations suggest a higher class standing and family circumstances permitting greater spending on food and healthy housing. We anticipate that both groups will have above-average stature. Prisoners born to fathers with labouring occupations, especially those in urban areas and lacking in specific skills, probably grew up with lower family income in less healthy environments, and consequently were shorter as adults. Occupation correlates partially with the indigenous identity indicator discussed above. Nevertheless, to the extent that men with indigenous names report a variety of occupations, inclusion of the indigenous identity variable identifies a ‘pure’ effect of being indigenous over and above any effects of ethnic clustering in particular occupations. More than two thirds of the Māori men in our sample were labourers or farm labourers.
The ordinary least squares regression estimates reported in Table 3 roughly follow the pattern of rolling averages in Figure 5. The model allows the ethnic differential to differ by birth cohort. We also identify height differentials for individual occupations. Pākehā born in the 1890s (the omitted group) were taller than Pākehā born in earlier decades by a statistically significant but quantitatively small margin of 0.6 to 0.9 centimetres (cm). Those born 1900–1920 were of similar stature to the 1890s. Successive cohorts realized steadily increasing adult stature until the 1950s (for which sample size is small). The prison data make clear that Pākehā born in the 1940s were fully 2.5 cm taller than those born 1890–1920.
Table 3. Maximum Likelihood Description of Stature, 21–49 years at Admission Dependent variable: Stature in cm.
The second set of columns modifies the regression by inclusion of a ‘business cycle’ variable that captures the state of the business cycle (deviation of real wage from its trend) at the year of admission
| Variable | co-eff | t-stat | P>|t| | co-eff | t-stat | P>|t| |
|---|---|---|---|---|---|---|
| Business cycle at admission | 0.65 | 0.8 | 0.44 | |||
| Professional | 1.40 | 3.6 | 0.00 | 1.40 | 3.6 | 0.00 |
| Clerical, sales or service | 0.07 | 0.4 | 0.69 | 0.07 | 0.4 | 0.69 |
| Labourer | −0.38 | −3.3 | 0.00 | −0.37 | −3.3 | 0.00 |
| Farmer | 1.88 | 6.3 | 0.00 | 1.88 | 6.3 | 0.00 |
| Farm labourer | −0.15 | −0.9 | 0.35 | −0.15 | −0.9 | 0.36 |
| Unknown occupation | −2.33 | −7.2 | 0.00 | −2.34 | −7.2 | 0.00 |
| Born 1830s | −2.59 | −1.0 | 0.33 | −2.65 | −1.0 | 0.32 |
| Born 1840s | 0.21 | 0.4 | 0.70 | 0.13 | 0.2 | 0.82 |
| Born 1850s | −0.56 | −1.6 | 0.11 | −0.64 | −1.8 | 0.08 |
| Born 1860s | −0.70 | −2.4 | 0.02 | −0.78 | −2.6 | 0.01 |
| Born 1870s | −0.88 | −3.2 | 0.00 | −0.92 | −3.2 | 0.00 |
| Born 1880s | −0.63 | −2.4 | 0.02 | −0.63 | −2.4 | 0.01 |
| Born 1900s | −0.10 | −0.4 | 0.67 | −0.11 | −0.5 | 0.61 |
| Born 1910s | 0.32 | 1.4 | 0.16 | 0.28 | 1.2 | 0.23 |
| Born 1920s | 0.64 | 2.8 | 0.01 | 0.59 | 2.4 | 0.02 |
| Born 1930s | 1.48 | 5.8 | 0.00 | 1.43 | 5.4 | 0.00 |
| Born 1940s | 2.59 | 10.2 | 0.00 | 2.53 | 9.5 | 0.00 |
| Born 1950s | 1.74 | 4.7 | 0.00 | 1.62 | 4.1 | 0.00 |
| Māori born 1830s | 1.37 | 0.5 | 0.63 | 1.35 | 0.5 | 0.63 |
| Māori born 1840s | 0.32 | 0.5 | 0.66 | 0.32 | 0.5 | 0.65 |
| Māori born 1850s | 1.03 | 2.4 | 0.02 | 1.03 | 2.4 | 0.02 |
| Māori born 1860s | 0.62 | 1.4 | 0.15 | 0.62 | 1.4 | 0.15 |
| Māori born 1870s | 0.64 | 0.9 | 0.36 | 0.64 | 0.9 | 0.36 |
| Māori born 1880s | 0.08 | 0.1 | 0.89 | 0.09 | 1.6 | 0.87 |
| Māori born 1890s | −0.94 | −2.2 | 0.03 | −0.94 | −2.2 | 0.03 |
| Māori born 1900s | −0.39 | −1.1 | 0.26 | −0.39 | −1.1 | 0.26 |
| Māori born 1910s | −1.42 | −5.0 | 0.00 | −1.42 | −5.0 | 0.00 |
| Māori born 1920s | −1.66 | −6.0 | 0.00 | −1.66 | −6.0 | 0.00 |
| Māori born 1930s | −2.22 | −8.1 | 0.00 | −2.22 | −8.1 | 0.00 |
| Māori born 1940s | −3.02 | −12.2 | 0.00 | −3.02 | −12.2 | 0.00 |
| Māori born 1950s | −1.69 | −3.9 | 0.00 | −1.69 | −3.9 | 0.00 |
| constant | 172 | 898 | 0.00 | 172 | 862 | 0.00 |
The Māori coefficients convey the ethnic differential for each cohort. Māori born in the nineteenth century were taller than Pākehā, but the margins are small and for the most part lack statistical significance. Still, the contrast with Pākehā coefficients lends support to the qualitative observation that among those born before 1890s Māori tended to be taller. Beginning in the 1890s, however, the Māori coefficients are consistently negative and increase in both size and significance.
Thus, the two groups were of comparable stature until the 1890s and thereafter, diverged notably. The differential becomes substantively and statistically significant for those born in the 1920s and then grows to a substantial size for the 1930s and 1940s birth cohorts. Despite Māori falling behind decisively during the World War I and interwar period, there is no sign of prolonged immiserization. Māori did not become substantially shorter.7 Nevertheless, while Pākehā born at mid-century were 2cm taller than their peers born c1900, average stature for Māori had barely changed. The prolonged delay in Māori realization of stature gains set them back considerably in a relative sense. The stature evidence suggests strongly that whereas New Zealand economy and environment provided rising living standards for Pākehā during the first half of the twentieth century, Māori did not share in these gains.
The occupational effects also reflect considerable inequality in the standard of living. Separate estimations for Māori and Pākehā (not shown) confirm that farmers and men in the professional-managerial class were taller for both groups. Manufacturing and transport workers and service sector tradesmen were taller than general labourers among Pākehā but not among Māori. Admittedly, the occupational differentials also reflect any endogenous sorting into occupations, for example that taller men became farmers because they were taller, as well as being born into farm families.8
Recent discussion has renewed interest in potential distortions arising from the effect of the business cycle on prison admissions. It is hypothesized that periods of high unemployment drive a larger share of the population into crime and hence into prison. Jailing a broader share of the population may increase the mean stature of prisoners relative to the entire population, as taller and hitherto more successful workers move out of the formal labor market and into criminal activity (Bodenhorn et al 2014). There is no easy way to predict the impact of this cyclically-sensitive selection bias on our estimation. As a precaution, therefore, we implement an ad hoc check by including in the estimation a measure of the state of the business cycle, deviation of real wages from their trend, at the time of imprisonment. Comparing the two sets of estimates, with and without the business cycle effect, points to considerable robustness. More sophisticated testing for the effect of the business cycle might produce a different result, however at present we see no evidence of any qualitative impact on our analysis.
The patterns of adult height are a cumulative product of growth in each year of life. The disease and nutritional environment very early in life matters most but growth can accelerate or falter at any age depending on circumstances. It is useful to be able to pinpoint the ages at which a stature differential first becomes visible. The prison records contain reports of stature for children as young as 11 years. No other source provides systematic evidence for Māori child stature before the 1960s. We focus on records from the early and mid-twentieth century because they describe children from the cohorts in which the ethnic differential widened.
Sample size allows us to estimate average height by age in mid and late adolescence with a series of age-specific dummy variables; height from 30 to 50 years is the omitted category.9 We organize the data to examine mean stature by age for two groups of adolescents, those born before 1914 and after 1945. We restrict attention to children who had reached the age of 16 years because they are sufficiently numerous for a meaningful estimate; sample size at lower ages is small. These are not longitudinal data, and the two birth cohorts are very broad. Nevertheless, in spite of its simplicity, this exercise provides additional insight into the twentieth century experience of changing health for Māori and Pākehā. We illustrate the age-stature profile in Figure 6.
Figure 6.

The patterns of child growth clearly changed during the first half of the twentieth century. Children who were born after 1945 were taller, by the age of 16 years, than those born before 1914. Adult stature increased from one cohort to the next, but not as much as stature at the age of 16. Thus a greater share of lifetime growth was experienced at early ages, for both ethnicities.
No ethnic differential is visible amongst adolescents in the pre-1914 cohort, but amongst those born after 1945 Pākehā were taller than Māori at every age 16 years and above. Thus the widening ethnic gap that is visible in adult stature can be traced back to the age of 16 years. Unfortunately, it is not yet possible to say if the differential appears at an even earlier age.
The timing of stature divergence in the early twentieth century is coincident with a period when Māori and Pākehā family forms changed most dramatically. Both Pākehā and Māori fertility, as best we can tell, was high in the late nineteenth century. Notably, fertility decline among Pākehā occurred slightly later than in North America or Britain (Sardon, 2006). In the late twentieth century fertility rates have again converged for Māori and Pākehā, though they remain somewhat higher for Māori, with recent total fertility rates for Māori women around 2.8, compared to 1.9 for Pākehā women (N. Jackson, Pool, & Cheung, 1994; Statistics New Zealand, 2011). In the first half of the twentieth century, the differences were more extreme as declining infant mortality led to the average Māori family having 7 children in the 1920s and 1930s, compared to 3 or fewer for Pākehā women in the same decades (Pool, Dharmalingam, & Sceats, 2007).
The correlation of fertility and family differences with stature differences can be seen in Figure 7. We measure fertility differences as the excess of Māori over Pākehā total fertility rates (Pool, et al., 2007). Family structure is more complicated to measure with the New Zealand census. Individual census returns were destroyed, and the census reported information on household and family inconsistently over time. Thus, we use the ratio of children (aged 0–14) to adult women (15–60) as a rough indicator of average family size in the Māori and Pākehā population. This index can be constructed for every census year after 1886, except 1906 when the census did not record Māori ages precisely. By and large the fertility and child:women series run parallel to each other. When total fertility rates are high variation in family size is low. Thus, between 1900 and World War II when Māori total fertility rates ranged between 6.5 and 7, Māori men had a high chance of growing up in a large household.
Figure 7.

Divergence in stature coincident with these trends suggests that larger Māori families were under some economic pressure, and unable to provide fully for large numbers of children. The period of stature convergence after World War II also corresponds with a period of declining family size, and convergence (but not equality) in Māori and Pākehā earnings (Brosnan, 1984; Brosnan, Rea, & Wilson, 1995; Sorrenson, 1990).
The timing of Māori stature decline suggests a life-course explanation for a Māori cardiovascular disease epidemic in the last quarter of the twentieth century (Blakely, Ajwani, Robson, Tobias, & Bonné, 2004; Curtis, Harwood, & Riddell, 2008; Tobias, et al., 2009). Longitudinal studies of European populations have shown that cardiovascular disease and mortality risk is elevated in populations deprived in childhood who then experience more abundant nutritional conditions as adults (Lawlor, et al., 2004). The stagnant stature of Māori men growing up from the 1900s to the 1940s, despite considerable improvement in medical knowledge in this period, suggests relatively deprived conditions for nutrition, disease exposure and/or child workload. In the second half of the twentieth century, however, calorie availability increased, disease impact abated and/or child workload diminished allowing these men to become taller and, more importantly, even heavier with corresponding cardiovascular disease risks.
7. Conclusion
The experience of stature for men born in late nineteenth-century New Zealand was very different than that of men born a century later. Socio-economic variations in height were pronounced for those born in the 1880s and 1890s. One hundred years later the differentials were reduced (although not eliminated) by the long-term diminution of economic inequality and reduced marginal significance of income for height at high income levels. Another point of contrast is that during the late twentieth century each generation was significantly taller than the one preceding. This was not true for nineteenth-century cohorts. As in other lands of overseas European settlements New Zealanders born during the 1890s grew up shorter than those born earlier. This may reflect a cyclical pattern. It remains clear, though, that any cohort differences were small compared with the occupational and ethnic effects. This is entirely the opposite of the twentieth century experience.
We began the paper recognising the importance of historical origins for Māori-Pākehā health differentials. Our evidence suggests that Māori stature in the early 1900s began to differ from Pākehā stature even after controlling for generational and occupational effects.10 There is at best limited evidence in this sample of an earlier Māori advantage in physique that would accord with popular qualitative observations from the time. Pākehā stature began to grow for cohorts born in the 1920s, but Māori stature did not begin to increase until cohorts born around the end of World War II. The timing of this divergence is intriguing, coming nearly a century after European colonization, and coincident with divergence in family and household structures. It suggests that inequalities in family resources for children were sharpest not on the frontier, but in an era of urbanization and welfare state development (Labrum 2004). Stature adds another dimension to this picture of ethnic inequality since colonization, and points to a need to examine Māori and Pākehā well-being from other perspectives in the modern era. Viewed together the evidence from New Zealand’s prisons suggests that inequalities in nutrition between Māori and Pākehā are long-standing, but not unchanging.
Table 2.
New Zealand Prisons, Summary Statistics
| Mean Height (cm) | Mean Weight (kg) | Mean BMI | |
|---|---|---|---|
| Māori or Pākehā | |||
| Pākehā | 172.1 | 70.3 | 23.7 |
| Māori | 171.1 | 77.5 | 26.5 |
| Occupation | |||
| Professional or managerial | 173.5 | 74.4 | 24.6 |
| Clerical | 172.8 | 70.6 | 23.6 |
| Sales | 172.9 | 71.2 | 23.8 |
| Service | 171.4 | 71.3 | 24.2 |
| Manufacturing, utilities, transport | 172.2 | 72.8 | 24.5 |
| Labourer (not farm) | 171.4 | 71.9 | 24.5 |
| Farmer or farm manager | 173.6 | 74.9 | 24.9 |
| Farm labourer | 171.9 | 75.2 | 25.4 |
| Unknown or not in labor force | 169.7 | 70.8 | 24.4 |
| Total | 171.8 | 72.6 | 24.6 |
Acknowledgments
Comments from participants at the 2012 Social Science History Association meetings, 2013 World Congress of Cliometrics and several anonymous referees improved this paper. We thank Archives New Zealand, the New Zealand Ministry of Justice and the New Zealand Police for access to prison registers restricted for 100 years after the final admission. Sam Ritchie, Tristan Egarr, Adeline Cumings, Anthony Gerbi and Chelsea Jack provided exemplary research assistance. This work was supported by the New Zealand Health Research Council under Grant HRC 08/231; and the Marsden Fund under Grant UoC 0807. Evan Roberts gratefully acknowledges additional support from the Minnesota Population Center (5R24HD041023), funded through grants from the Eunice Kennedy Shriver National Institute for Child Health and Human Development (NICHD).
Comments from participants at the Social Science History Association, Population Association of America, and World Congress of Cliometrics conferences and several anonymous referees improved this paper. We thank Archives New Zealand and the New Zealand Ministry of Justice for access to confidential prison registers. Sam Ritchie, Tristan Egarr, Adeline Arulandu, and Anthony Gerbi provided exemplary research assistance. Data collection was supported by the Health Research Council under Grant HRC 08/231 and the Marsden Fund under Grant UoC 0807. The Victoria University of Wellington Human Ethics Committee granted ethical permission for this research. Evan Roberts acknowledges further support from the Minnesota Population Center (5R24HD041023), funded through grants from the Eunice Kennedy Shriver National Institute for Child Health and Human Development (NICHD).
Footnotes
Government reports since the early 1900s have documented the changing stature of children. Adult data was not published until the 1970s.
Admittedly, the European experience is complex, in part because the timing of industrialization was earlier and varied. In the UK, for example, the adverse health effects of industrial growth were most evident in the 1820s, 1830s and 1840s. Heights by birth cohort appear to have been increasing either from the 1850s. Elsewhere, men born in the early 1890s appear to have been taller than men born between 1886–90 in Austria, France, Germany, Great Britain, Ireland, Italy, the Netherlands, Spain and Sweden (Hatton and Bray, 2010). In contrast, many overseas locations saw declining stature during the 1890s.
Gibson (1973) attributes fast urbanization beginning in the 1930s to “an increased rate of population growth, the lack of opportunity for advancement in agriculture, and the demand for labor in the cities”. Hill (2012) states that the “reasons for this demographic phenomenon are complex, but the main push factor was the inability of a burgeoning population (demographic revival had begun at the turn of the century) to find sustenance from the remaining lands in Maori ownership. Among the several pull factors, state encouragement came to be important, with a Maori urban workforce needed to boost wartime productivity and postwar industrialization”. Metge (1964) and Keenan (2013, chapter five) emphasize social as well as labour market aspects of the World War Two.
The limited regional variation in Pākehā stature implies that a spatial distribution favouring Māori does not generate an unrepresentative Pākehā sample. Other prisons in our sample held men from across the country.
Inquiries with archivists suggest that in the case of the Mount Eden (Auckland) prison a major prison riot in 1965 contributed to reluctance on the part of prison officials to transfer records to Archives New Zealand.
Cranfield and Inwood (2015a) confirm a considerable degree of occupational persistence in this period by linking soldiers with their fathers, admittedly for another country and for soldiers rather than prisoners. Prisoners are more likely than soldiers to have experienced a degree of downward mobility. A life-cycle evolution of occupation is a further complication. Incarceration or enlistment often occurred at a younger age than that of the father at the birth of the soldier or prisoner.
The calculation is based on a summation of the omitted 1890s Pākehā stature (constant term in the regression) and cohort-specific effects. For Māori, we sum the omitted group, general cohort effects and Māori-specific cohort effects.
In this period occupational differentials may reflect labour market selection as well as early life conditions (under the assumption of occupational persistence), and if so the relative importance of the two effects is unknown.
This is a simple regression of stature on age, with no occupational controls, in order to identify an average growth curve for each cohort.
The divergence in stature broadly coincides with a divergence in incarceration rates. There is no evidence that the latter influenced the former, although Bodenhorn et al (2014) argue that in some circumstances jailing a broader share of the population may increase the mean stature of prisoners relative to the entire population. If this influence were at work here, the prison data would understate the true divergence in stature between Māori and Pākehā.
Contributor Information
Kris Inwood, Departments of Economics and History, University of Guelph.
Les Oxley, Department of Economics, University of Waikato.
Evan Roberts, Email: eroberts@umn.edu, Department of History and Minnesota Population Center, University of Minnesota.
References
- Barrington JM. Separate but Equal?: Maori Schools and the Crown 1867–1969. Wellington: Victoria University Press; 2008. [Google Scholar]
- Baten J, Murray J. Heights of Men and Women in Nineteenth-Century Bavaria: Economic, Nutritional, and Disease Influences. Explorations in Economic History. 2000;37:351–361. [Google Scholar]
- Baten J, Pelger I, Twrdek L. The anthropometric history of Argentina, Brazil and Peru during the 19thand early 20th century. Economics and Human Biology. 2009;7:319–333. doi: 10.1016/j.ehb.2009.04.003. [DOI] [PubMed] [Google Scholar]
- Belich J. The New Zealand Wars and the Victorian Interpretation of Racial Conflict. Auckland: Penguin; 1987. [Google Scholar]
- Blakely T, Ajwani S, Robson B, Tobias M, Bonné M. Decades of disparity: widening ethnic mortality gaps from 1980 to 1999. New Zealand Medical Journal. 2004;117 [PubMed] [Google Scholar]
- Bogin B. Patterns of human growth. 2. Cambridge: Cambridge University Press; 1999. [Google Scholar]
- Bodenhorn H, Guinnane T, Mroz T. Caveat Lector: Sample Selection in Historical Heights and the Interpretation of Early Industrializing Economies. 2014 National Bureau of Economic Research Working Paper 19955. [Google Scholar]
- Brosnan P. Age, education and Maori-Pakeha income differences. New Zealand Economic Papers. 1984;18:49–61. [Google Scholar]
- Brosnan P, Rea D, Wilson M. Labour market segmentation and the state: the New Zealand experience. Cambridge Journal of Economics. 1995;19:667–696. [Google Scholar]
- Bull S. ‘The Land of Murder, Cannibalism, and All Kinds of Atrocious Crimes?’: Maori and Crime in New Zealand, 1853–1919. British Journal of Criminology. 2004;44:496–519. [Google Scholar]
- Callister P, Didham R, Potter D. Ethnic Intermarriage in New Zealand. Official Statistics Research Series. 2005;1:1–73. [Google Scholar]
- Carpenter KJ. Nutritional studies in Victorian prisons. The Journal of nutrition. 2006;136:1–8. doi: 10.1093/jn/136.1.1. [DOI] [PubMed] [Google Scholar]
- Cranfield J, Inwood K. The great transformation: A long-run perspective on physical well-being in Canada. Economics and Human Biology. 2007;5:204–228. doi: 10.1016/j.ehb.2007.02.001. [DOI] [PubMed] [Google Scholar]
- Cranfield J, Inwood K. Lives in Transition: Longitudinal Research from Historical Sources. Kingston and Montreal: McGill-Queens University Press; 2015a. Genes, Class or Culture? French-English Height Differences in Canada; pp. 231–253. [Google Scholar]
- Cranfield J, Inwood K. A Tale of Two Armies: Comparative Growth in the Mirror of WWI. Australian Economic History Review. 2015b:50. forthcming. [Google Scholar]
- Curtis E, Harwood M, Riddell T. Cardiovascular disease. In: Robson B, Harris R, editors. Hauora: Màori Standards of Health IV. A study of the years 2000–2005. Wellington: Te Rōpū Rangahau Hauora a Eru Pōmare; 2008. pp. 141–159. [Google Scholar]
- de Souza C. Unpublished M.Com. University of Melbourne; Melbourne: 1994. Height, Health and Living Standards of Australian Men, 1861–1902. [Google Scholar]
- Department of Health. Appendices to the Journal of the House of Representatives. H-31. Wellington: New Zealand Parliament; 1939. Annual Report of the Director General of Health. [Google Scholar]
- Dominion of New Zealand.; Government Statistician, editor. New Zealand Official Yearbook. Wellington: Government Printer; 1912. [Google Scholar]
- Dow D. Maori Health and Government Policy. Wellington: Victoria University Press; 1999. [Google Scholar]
- Dunlop JC. Report on Prison Dietaries. London: Eyre & Spottiswoode; 1899. [Google Scholar]
- Durie M. Whaiora: Maori health development. Auckland: Oxford University Press; 1998. [Google Scholar]
- Egarr T. Discipline and Defence: The Military Influence on Policing and Imprisonment. Victoria University of Wellington; Wellington: 2012. pp. c.1870–1913. [Google Scholar]
- Eveleth PB, Tanner JM. Worldwide variation in human growth. 2. Cambridge: Cambridge University Press; 1990. [Google Scholar]
- Fairburn M. The ideal society and its enemies : the foundations of modern New Zealand society, 1850–1900. Auckland, N.Z: Auckland University Press; 1989. [Google Scholar]
- Ferguson G. Building the New Zealand Dream. Palmerston North: Dunmore Press; 1994. [Google Scholar]
- Floud R, Wachter K, Gregory A. Height, Health and History: Nutritional Status in the United Kingdom, 1750–1980. Cambridge: Cambridge University Press; 1990. [Google Scholar]
- Gibson C. Urbanization in New Zealand: A Comparative Analysis. Demography. 1973;10:71–84. [PubMed] [Google Scholar]
- Gillman MW. A life course approach to obesity. In: Kuh Diana, Ben-Shlomo Yoav., editors. A life course approach to chronic disease epidemiology. Oxford: Oxford University Press; 2004. pp. 189–217. [Google Scholar]
- Greasley D, Oxley L. Growing apart? Australia and New Zealand growth experiences, 1870–1913. New Zealand Economic Papers. 1999;33:1–14. [Google Scholar]
- Greasley D, Oxley L. The pastoral boom, the rural land market, and long swings in New Zealand economic growth, 1873–1939. Economic History Review. 2009;62:324–349. [Google Scholar]
- Haines MR. Growing Incomes, Shrinking People - Can Economic Development Be Hazardous To Your Health? Historical Evidence For The United States, England, And The Netherlands In The Nineteenth Century. Social Science History. 2004;28:249–270. [Google Scholar]
- Haines M, Craig L, Weiss T. The short and the dead: Nutrition, mortality and the ‘Antebellum Puzzle’ in the United States. Journal of Economic History. 2003;63:382–413. [Google Scholar]
- Hall KD, Heymsfield SB, Kemnitz JW, Klein S, Schoeller DA, Speakman JR. Energy balance and its components: implications for body weight regulation. The American Journal of Clinical Nutrition. 2012;95:989–994. doi: 10.3945/ajcn.112.036350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hatton TJ, Bray BR. Long run trends in the heights of European men, 19th–20th centuries. Economics and Human Biology. 2010;8:405–413. doi: 10.1016/j.ehb.2010.03.001. [DOI] [PubMed] [Google Scholar]
- Hill R. The Iron Hand in the Velvet Glove: The Modernisation of Policing in New Zealand 1886–1917. Wellington: Dunmore Press; 1995. [Google Scholar]
- Hill R. Maori Urban Migration and the Assertion of Indigeneity in Aotearoa/New Zealand, 1945–1975. Interventions: International Journal of Postcolonial Studies. 2012;14:256–278. [Google Scholar]
- Inwood K, Masakure O. Poverty and physical well-being among the coloured population in South Africa. Economic History of Developing Regions. 2013;28:56–82. [Google Scholar]
- Inwood K, Oxley L, Roberts E. Physical stature in nineteenth century New Zealand: A preliminary interpretation. Australian Economic History Review. 2010;50:262–283. [Google Scholar]
- Inwood K, Oxley L, Roberts E. ‘Tall, active and well made’: New insights into Māori health. Unpublished conference paper presented to the Economic History Association; Columbus. 2014. pp. 1700–1990. [Google Scholar]
- Inwood K, Maxwell-Stewart H, Oxley D. Growing incomes, growing people in nineteenth-century Tasmania. Unpublished conference paper presented to the Social Science History Association; Toronto. 2014. [Google Scholar]
- Jackson M. The Maori and the Criminal Justice System. Wellington: Department of Justice; 1988. [Google Scholar]
- Jackson N, Pool I, Cheung MC. Maori and non-Maori fertility. Convergence divergence or parallel trends? New Zealand Population Review. 1994;20:31–57. [Google Scholar]
- Keenan E. PhD dissertation. Victoria University of Wellington; 2013. Māori Urban Migrations and Identities, ‘Ko Ngā Iwi Nuku Whenua’. [Google Scholar]
- Koepke N, Baten J. The Biological Standard Of Living In Europe During The Last Two Millennia. European Review of Economic History. 2005;9:61–95. [Google Scholar]
- Komlos J. Anomalies in economic history: Toward a resolution of the ‘Antebellum Puzzle’. Journal of Economic History. 1996;56:202–14. [Google Scholar]
- Komlos J. Shrinking in a Growing Economy? The Mystery of Physical Stature during the Industrial Revolution. Journal Of Economic History. 1998;58:779–802. [Google Scholar]
- Komlos J. Access to Food and the Biological Standard of Living: Perspectives on the Nutritional Status of Native Americans. American Economic Review. 2003;93:252–255. doi: 10.1257/000282803321455250. [DOI] [PubMed] [Google Scholar]
- Labrum B. Developing “the essentials of good citizenship and responsibilities” in Maori women: family life, social change, and the state in new zealand, 1944–70. Journal of Family History. 2004;29:445–465. [Google Scholar]
- Lange R. May the People Live: A History of Māori Health Development 1900–1918. Auckland: Auckland University Press; 1999. [Google Scholar]
- Lawlor DA, Ben-Shlomo Y, Leon DA. Pre-adult influences on cardiovascular disease. In: Kuh Diana, Ben-Shlomo Yoav., editors. A life course approach to chronic disease epidemiology. Oxford: Oxford University Press; 2004. pp. 41–76. [Google Scholar]
- Maloney T, Carson S. Living standards in Black and White: Evidence from the heights of Ohio Prison inmates, 1829–1913. Economics & Human Biology. 2008:237–251. doi: 10.1016/j.ehb.2008.04.002. [DOI] [PubMed] [Google Scholar]
- Mein Smith P. Infant welfare services and infant mortality: a historian’s view. The Australian Economic Review. 1991;24:22–34. doi: 10.1111/j.1467-8462.1991.tb00379.x. [DOI] [PubMed] [Google Scholar]
- Metge J. A New Maori Migration. Rural and Urban Relations in Northern New Zealand. London: The Athlone Press; 1964. [Google Scholar]
- Nicholas S, Gregory R, Kimberley S. The welfare of Indigenous and White Australians 1890–1955. Stuttgart: Franz Steiner Verlag; 1998. [Google Scholar]
- Parssinen TM. Popular science and society: the phrenology movement in early Victorian Britain. Journal of Social History. 1974;8:1–20. doi: 10.1353/jsh/8.1.1. [DOI] [PubMed] [Google Scholar]
- Pool I. Te Iwi Maori : a New Zealand population past present & projected. Auckland: Auckland University Press; 1991. [Google Scholar]
- Pool I, Dharmalingam A, Sceats J. The New Zealand Family From 1840: A Demographic History. Auckland: Auckland University Press; 2007. [Google Scholar]
- Pratt J. Punishment in a Perfect Society. Wellington: Victoria University Press; 1993. [Google Scholar]
- Prince JM, Steckel RH. Nutritional Success On The Great Plains: Nineteenth-century Equestrian Nomads. Journal of Interdisciplinary History. 2003;33:353–384. [Google Scholar]
- Rector FL. Health and medical service in American prisons and reformatories. New York: The National Society of Penal Information, Inc; 1929. [Google Scholar]
- Robson B, Harris R. Hauora: Màori Standards of Health IV. A study of the years 2000–2005. Wellington: Te Rōpū Rangahau Hauora a Eru Pōmare; 2008. [Google Scholar]
- Rose RJ. Maori-European Standard of Health. Wellington: Medical Statistics Branch, Department of Health; 1960. [Google Scholar]
- Rose RJ. Maori-European comparisons in mortality. Wellington: National Health Statistics Centre, Dept. of Health; 1972. [Google Scholar]
- Salvatore RD. Heights, nutrition, and well-being in Argentina, ca. 1850–1950: Preliminary Results. Revista de Historia Económica. 2007;25:53–85. [Google Scholar]
- Sardon JP. Fertility in the Developed English-speaking Countries Outside Europe: Canada, United States, Australia and New Zealand. Population (english edition) 2006;61:267–291. [Google Scholar]
- Shlomowitz R. Did the mean height of Australian-born men decline in the late nineteenth century? A comment. Economics and Human Biology. 2007;5:484–488. doi: 10.1016/j.ehb.2007.09.002. [DOI] [PubMed] [Google Scholar]
- Silventoinen K. Determinants of variation in adult body height. Journal of Biosocial Science. 2003;35:263–285. doi: 10.1017/s0021932003002633. [DOI] [PubMed] [Google Scholar]
- Sorrenson MPK. Modern Māori: The Young Māori Party to Mana Motuhake. In: Sinclair Keith., editor. The Oxford Illustrated History of New Zealand. Auckland: Oxford University Press; 1990. [Google Scholar]
- Statistics New Zealand. Demographic Trends: 2011. Wellington: Statistics New Zealand; 2011. [Google Scholar]
- Steckel RH. A Peculiar Population: The Nutrition, Health, and Mortality of American Slaves from Childhood to Maturity. Journal of Economic History. 1996;46:721–741. doi: 10.1017/s0022050700046842. [DOI] [PubMed] [Google Scholar]
- Steckel RH. Biological Measures of the Standard of Living. Journal of Economic Perspectives. 2008;22:129–152. doi: 10.1257/jep.22.1.129. [DOI] [PubMed] [Google Scholar]
- Steckel RH. Biological Measures of Economic History. Annual Review of Economics. 2013;5:401–423. [Google Scholar]
- Steckel RH, Haurin DR. Health and Nutrition in the American Midwest: Evidence from the Height of Ohio National Guardsmen, 1850–1910. In: Komlos J, editor. Stature, Living Standards, and Economic Development. Chicago: University of Chicago Press; 1995. pp. 117–128. [Google Scholar]
- Steckel RH, Prince JM. Tallest in the World: Native Americans of the Great Plains in the Nineteenth Century. American Economic Review. 2001;91:287–294. [Google Scholar]
- Sutherland ILG. The Maori Situation. Wellington: Harry H. Tombs; 1935. [Google Scholar]
- Tobias M, Blakely T, Matheson D, Rasanathan K, Atkinson J. Changing trends in indigenous inequalities in mortality: lessons from New Zealand. International Journal of Epidemiology. 2009;38:1711–1722. doi: 10.1093/ije/dyp156. [DOI] [PubMed] [Google Scholar]
- van Leeuwen MHD, Maas I, Miles A. Historical International Standard Classification of Occupations. Leuven: Leuven University Press; 2002. [Google Scholar]
- Wanhalla A. One White Man I Like Very Much. Journal of Women’s History. 2008;20:34–56. [Google Scholar]
- Whittin ES. The Caged Man. New York: Columbia University; 1913. [Google Scholar]
- Whitwell G, de Souza C, Nicholas S. Height, Health and Economic Growth in Australia, 1860–1940. In: Floud Roderick, Steckel Richard H., editors. Health and Welfare during Industrialization. Chicago: University of Chicago Press; 1997. pp. 379–422. [Google Scholar]
- Whitwell G, Nicholas S. Weight and Welfare of Australians, 1890–1940. Australian Economic History Review. 2001;41:159–175. doi: 10.1111/1467-8446.00080. [DOI] [PubMed] [Google Scholar]
- Zehetmayer M. The postbellum continuation of the antebellum puzzle: stature in the US, 1847–1894. European Review of Economic History. 2011;15:313–327. [Google Scholar]