

Abstract
In this report, we present the results of a single patient with optic neuropathy treated within the Stem Cell Ophthalmology Treatment Study (SCOTS). SCOTS is an Institutional Review Board approved clinical trial and is the largest ophthalmology stem cell study registered at the National Institutes of Health to date- www.clinicaltrials.gov Identifier NCT 01920867. SCOTS utilizes autologous bone marrow-derived stem cells in the treatment of optic nerve and retinal diseases. Pre- and post-treatment comprehensive eye exams were independently performed at the Wilmer Eye Institute at the Johns Hopkins Hospital, USA. A 27 year old female patient had lost vision approximately 5 years prior to enrollment in SCOTS. Pre-treatment best-corrected visual acuity at the Wilmer Eye Institute was 20/800 Right Eye (OD) and 20/4,000 Left Eye (OS). Four months following treatment in SCOTS, the central visual acuity had improved to 20/100 OD and 20/40 OS.
Keywords: stem cells, optic nerve, optic neuropathy, ophthalmology, bone marrow-derived stem cells, blindness, visual loss
Introduction
Optic nerve disease is complicated and there are a number of pathophysiologic mechanisms that can lead to retinal ganglion cell impairment or death. Compression, ischemia, inflammation, trauma and hereditary neuronal and mitochondrial diseases are among the causes of optic nerve dysfunction and visual loss. There is substantial support for the use of bone marrow-derived stem cells (BMSCs) in neurologic and ophthalmic diseases as outlined by Ng et al. (2014). Transplanted mesenchymal stem cells (MSCs) have shown significant neuroprotective effects in preclinical models of glaucoma as suggested by Li et al. (2009). After intravitreal transplantation in a rat model of glaucoma, MSCs survived for at least 5 weeks within the vitreous body and some of them migrated into the host retina as reported by Johnson et al. (2010). MSCs from the trabecular meshwork and conjunctivae have produced photoreceptor-like cells in vitro as per Nadri et al. (2013). BMSC transplantation can increase ganglion cell survival in animal models of transient ischemia. Increased survival has also been demonstrated in an ocular hypertension model. These observations are in agreement with Yu et al. (2006).
BMSCs include hematopoietic stem cells and MSCs. MSCs were originally identified in the bone marrow and are also known as marrow stromal cells. These are the adult population of stromal progenitor cells of mesodermal origin that have high proliferative and differentiation capacities and can provide neurons and glial cells. They have shown neuroprotective and immunomodulatory effects and have an important role in the treatment of nervous tissue disease including retinal and optic nerve diseases through brain-derived neurotrophic factor as reported by Wilkins et al. (2009).
Methodology of SCOTS
SCOTS, the Stem Cell Ophthalmology Treatment Study, is the largest ophthalmology stem cell study registered at the National Institutes of Health: Identifier NCT Number 01920867. SCOTS is an open label, non-randomized, efficacy study. There is no placebo or sham arm. All patients enrolled in the study meet eligibility criteria and receive active treatment. Bone marrow aspirated from the posterior iliac crest is separated to provide BMSCs within the stem cell concentrate.
Inclusion criteria for SCOTS include that patients should
Have objective, documented damage to the retina or optic nerve unlikely to improve OR.
Have objective, documented damage to the retina or optic nerve that is progressive.
AND have less than or equal to 20/40 best corrected central visual acuity in one or both eyes AND/OR an abnormal visual field in one or both eyes.
At least 3 months post-surgical treatment, intend to treat any ophthalmologic disease and are stable.
If under current medical therapy (pharmacologic treatment), a retinal or optic nerve disease be considered stable on that treatment and unlikely to have visual function improvement (for example, glaucoma with intraocular pressure stable on topical medications but visual field damage).
Have the potential for improvement with BMSC treatment and are at minimal risk of any potential harm from the procedure.
Be 18 years of age or older.
Be medically stable and able to be medically cleared by their primary care physician or a licensed primary care practitioner for the procedure. Medical clearance means that in the estimation of the primary care practitioner, the patient can reasonably be expected to undergo the procedure without significant medical risk to health.
Exclusion criteria include:
Patients who are not capable of an adequate ophthalmologic examination or evaluation to document the pathology.
Patients who are not capable or not willing to undergo follow up eye exams with the principle investigator or their ophthalmologist or optometrist as outlined in the protocol.
Patients who are not capable of providing informed consent.
Patients who have significant health risk.
There are three arms of SCOTS with the type of treatment chosen based on the degree of visual loss, etiology of visual loss, associated risk factors for the treatment arms and the patient's medical risk status. Bilateral treatment is provided assuming both eyes meet eligibility requirements. As these are autologous stem cells, no immunosuppression is required. An FDA cleared class II medical device is used to separate the bone marrow aspirate into a stem cell concentrate. This concentrate has averaged 1.2 billion total nucleated cells including MSCs in approximately 14–15 cm3 of concentrate. Retrobulbar injection consists of 3 cm3 of concentrate, subtenons injection 1 cm3 of concentrate, intravitreal injection 0.05 cm3 of concentrate, subretinal injection approximately 0.1 cm3 of concentrate, intra-optic nerve injection approximately 0.2 cm3 of concentrate, and intravenous injection the remainder of the concentrate.
Arm 1 consists of retrobulbar and subtenons injection, followed by intravenous infusion, of stem cell concentrate. Patients with ophthalmic conditions which preclude safe or effective utilization of intravitreal injection of concentrate, such as the presence of silicon oil, may be offered Arm 1 if meeting inclusion criteria. Arm 2 consists of retrobulbar, subtenon and intravitreal administration, followed by intravenous infusion, of concentrate. Patients meeting inclusion criteria with visual acuity between 20/40 and 20/200 in one or both eyes and/or visual loss may be offered Arm 2. Arm 3 is reserved for retinal and optic nerve patients with severe visual loss meaning acuity of 20/200 or worse in at least one eye. Typically patients admitted to Arm 3 have much poorer vision. Arm 3 consists of the better-seeing eye receiving the same treatment as Arm 1 or more typically, Arm 2, and the eye with more extensive visual acuity loss receiving a core pars plana vitrectomy with subretinal or intra-optic nerve injection of concentrate followed by intravenous infusion of stem cells. Monocular patients are not eligible for Arm 3. Follow up is required at 1, 3, 6 and 12 months post treatment with reporting of the eye exam results to the principal investigator and study director.
The SCOTS procedure is patient funded and performed under general anesthesia. Treatment is provided in a fully licensed ambulatory surgical center in Coconut Creek, Florida, USA. All human investigations were performed with informed consent. The study was reviewed and approved by our Institutional Review Board. The study was registered at the National Institutes of Health.
Clinical History and Course
The patient is a 27 year old, right-handed female who had normal vision until June 2009, when she developed decreased vision in each eye and pain with eye movement. Over the next several weeks she developed severe, bilateral visual loss. She initially demonstrated swelling of the right optic nerve and ultimately developed significant bilateral temporal pallor with centrocecal scotomas. Differential diagnosis included neuromyelitis spectrum disorder and Leber's hereditary optic neuropathy. There was a history of accidental carbon monoxide poisoning from a leaking boiler 16 months prior to the loss of vision, but given the lengthy intervening period, this was thought not to be the etiology of the present visual loss. The patient was evaluated for neuromyelitis optica or Devic's syndrome and was negative for neuromyelitis optic immunoglobulin G (NMO-IgG) on two separate tests performed at The Johns Hopkins Hospital. Testing for Leber's hereditary optic neuropathy was negative. On fluid attenuation inversion recovery (FLAIR) imaging, the MRI showed mild middle cerebellar peduncle hyperintensity. She received treatment with methylprednisolone but the vision continued to decline. Additional brain MRIs were normal without demyelinating lesions. The final diagnosis was idiopathic bilateral optic neuritis leading to bilateral optic neuropathy.
Dr. Malkin examined the patient on January 21, 2010. The past medical history was significant for a history of asthma, migraines, and memory loss secondary to carbon monoxide exposure in the past. The best corrected visual acuity was 5/400 right eye (OD) equivalent to 20/1,600 with eccentric fixation, and 5/700 left eye (OS) equivalent to 20/2,800. Contrast sensitivity was 1.00 log units.
On March 21, 2013, the patient's visual acuity was 5/225 OD, equivalent to 20/900 with eccentric fixation, and 5/300 OS equivalent to 20/1,200 with eccentric fixation. Contrast sensitivity was moderately reduced to 1.28 log units.
On January 16, 2014, the visual acuity was 5/200 OD and 5/400 OS. Contrast sensitivity was 1.32 log units. Biomicroscopic examination was unremarkable and fundus examination revealed 3+ pallor of the optic nerve bilaterally (OU).
Neuro-ophthalmology evaluation at Wilmer Eye Institute on February 5, 2014, demonstrated a best corrected visual acuity of 5/200 OD with eccentric fixation and 1/200 OS with eccentric fixation. The pupils were equal, round and slowly reactive to light in both eyes (OU). The extraocular movements were unaffected. The biomicroscopic examination was unremarkable OU. The fundus examination was significant for 3+ optic nerve pallor OU.
The patient was accepted into SCOTS in early February 2014, and underwent the preoperative assessment and informed consent with Dr. Jeffrey Weiss on March 3, 2014. Preoperative testing demonstrated a visual acuity of Count Fingers at 1 foot OD and Count Fingers at 2 feet OS. The biomicroscopic examination was unremarkable. Fundus examination was significant for pale optic nerves OU. Humphrey automated visual field testing demonstrated significant loss OU (Figures 1, 2).
Figure 1.
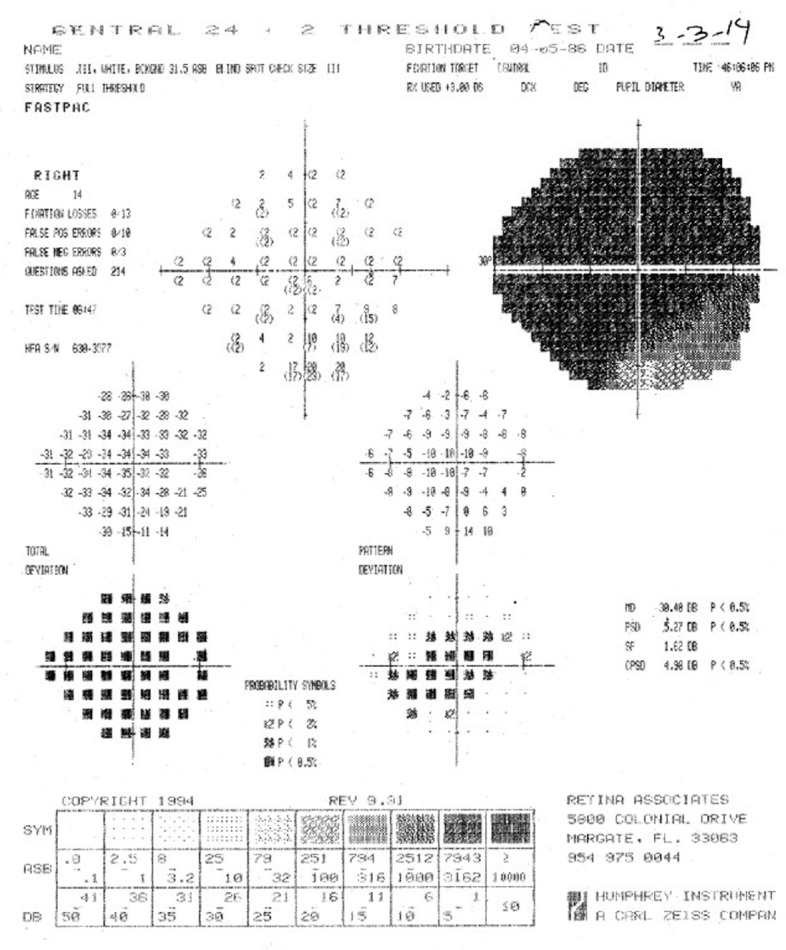
Preoperative visual field of the right eye.
Figure 2.
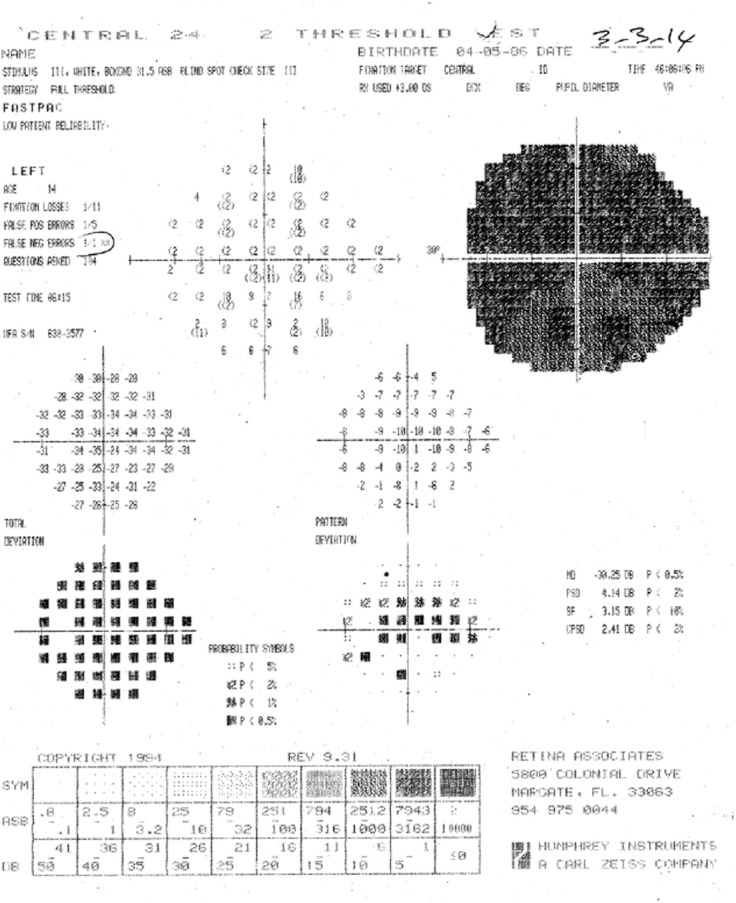
Preoperative visual field of the left eye.
She was approved for Arm 3 of SCOTS because her vision was 20/200 or less in at least one eye. This consists of retrobulbar injection, subtenon injection and intravitreal injection of BMSC for the right eye (OD), and vitrectomy and direct intra-optic nerve injection of BMSC for the left eye (OS), followed by intravenous infusion. She underwent the procedure uneventfully on March 4, 2014. On March 7, the vision was Count Fingers 5 feet/ Pinhole, Count Fingers 6 feet OD, and Count Fingers 2 feet/ Pinhole, Count Fingers 3 feet OS. Side effects included some initial tearing and conjunctival ecchymosis. There were no complications.
Three months postoperatively, the patient reported that she was able to “find spaces in the scotomas”. She was examined by Dr. Malkin on August 5, 2014. On that date, the patient's visual acuity was 5/300 OD and 20/40–2 OS. The pupils were equal and reactive to light. The optic nerve was graded as 3+ pallor OD and 2+ pallor OS.
On August 21, 2014, approximately 6 months following the SCOTS procedure, she again underwent neuro-ophthalmology evaluation at the Wilmer Eye Institute. On examination, the uncorrected visual acuity was 20/100+1 OD and 20/40–2 OS. She was now Jaeger 4 (J-4) OS (near vision). Humphrey automated visual field testing (Figures 3, 4) performed at the Retina Associates of South Florida demonstrated post-operative improvement OU compared to the preoperative studies. On March 11, 2015, 12 months following the procedure, the uncorrected visual acuity was 20/100–1/ Pinhole, 20/80+1 OD and 20/60+2/Pinhole, 20/40+2 OS.
Figure 3.
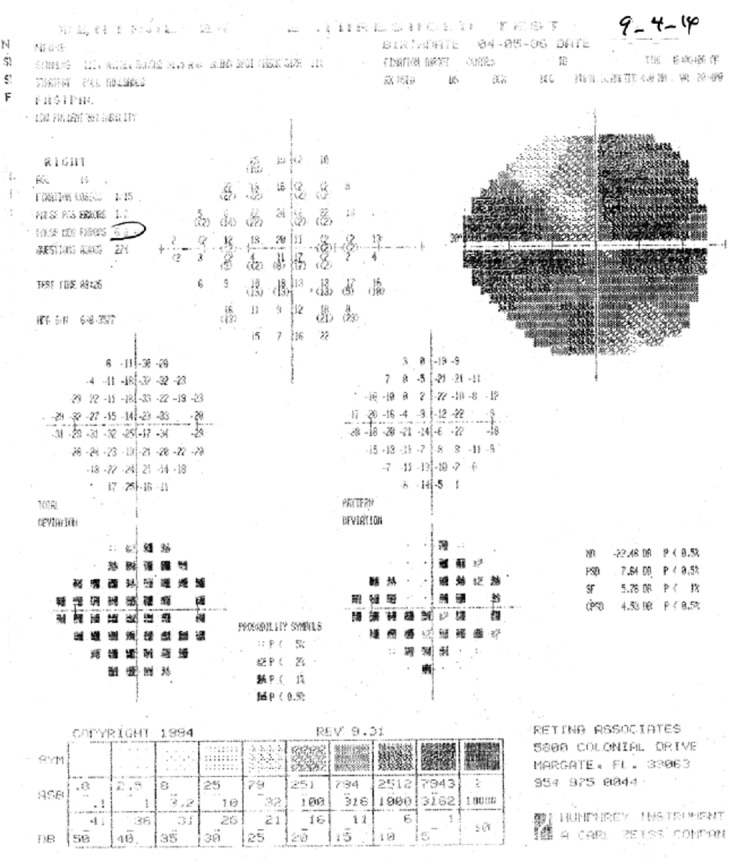
Postoperative visual field of the right eye.
Figure 4.
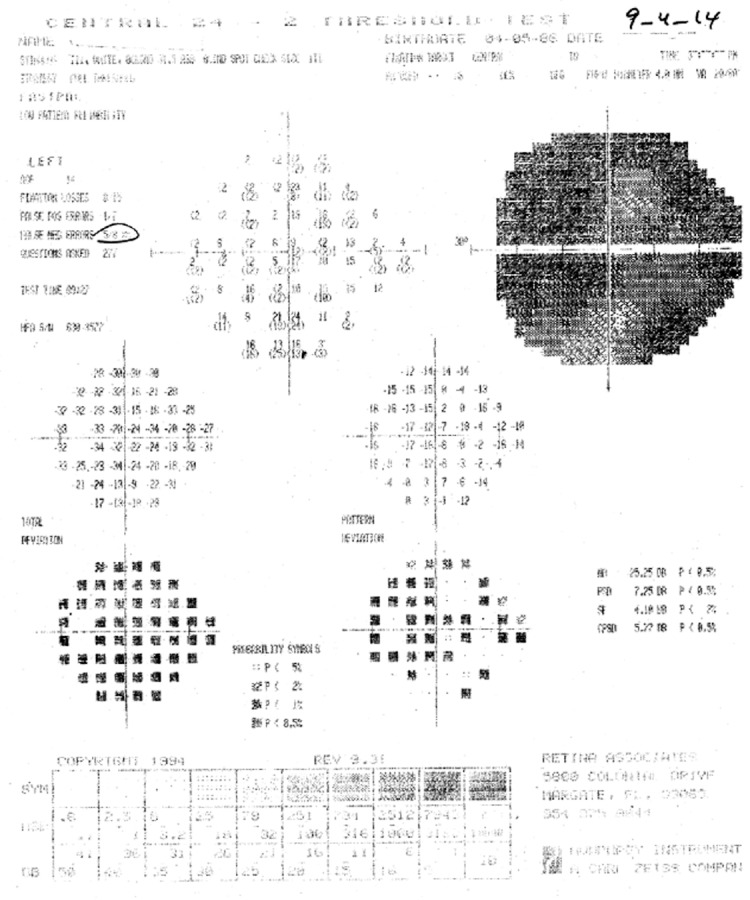
Postoperative visual field of the left eye.
Discussion
In this case report, an idiopathic optic neuropathy resulted in significant loss of central vision of approximately 5 years of duration. As independently documented at the Wilmer Eye Institute, approximately 6 months following treatment in SCOTS using BMSCs, the visual acuity improved from 20/800 to 20/100+1 OD in the eye receiving stem cell injections and from 20/4,000 to 20/40–2 OS in the eye receiving vitrectomy and intra-optic nerve injection of BMSCs. The visual acuity improvement remained stable at the 12 month post operative examination.
In addition to potential proliferation and differentiation of BMSCs, we can postulate several potential mechanisms for the visual improvements. There may be secretion of neurotrophic factors by the BMSCs before or after differentiation. BMSCs release certain neurotrophic growth factors including BDNF which may offer neuroprotection (Wilkins et al., 2009). BMSCs also show neural phenotypes ameliorating ischemic brain deficits in animal models likely based on upregulation of host brain plasticity by proteins secreted by the transplanted human MSCs as outlined by Zhao et al. (2002).
In a murine model of ischemia/reperfusion injury caused by increased intraocular pressure, BMSCs provided by intravitreal injection were shown to migrate to the surface of the retina and integrate into the nerve fiber layer ultimately forming the optic nerve. Some were observed to express markers of neuron specific enolase, neurofilament and various neurotrophic factors which are thought to be of value in retinal and optic nerve neuroprotection as reported by Li et al. (2009).
The mechanism of BMSC effects may include mitochondrial transfer to stressed or damaged cells resulting in increased ATP concentrations, as evidenced in a pulmonary injury model as per Islam et al. (2012).
Transplantation of BMSCs can induce the synthesis of nerve growth factor, BDNF, glial cell line-derived neurotrophic factor, and neurotrophin-3 and may provide functional recovery in animal models of brain trauma noted by Chen et al. (2005).
Mechanisms of immune modulation by MSCs include both pro- and anti-inflammatory mechanisms which may affect multiple cellular processes such as apoptosis and angiogenesis as per Bunnell et al. (2010). As reported by Schwartz et al. (2014), the subretinal placement of retinal pigment epithelial cells derived from human embryonic stem cells resulted in visual improvements in two retinal diseases: age-related macular degeneration and Stargardt's disease. The Schwartz study utilized processed non-autologous cells and patients received a 13 week course of immunosuppression post surgery. In our study, autologous BMSCs were used and no immunosuppression was performed.
To conclude, SCOTS continues to enroll and evaluate the clinical responses of patients with various retinal and optic nerve diseases. In the patient presented, optic neuropathy of uncertain etiology leading to optic atrophy resulted in long-standing and severe visual loss. Treatment with BMSCs using the specific injection methods provided within SCOTS achieved a dramatic improvement in vision. The exact mechanisms of visual improvement remain uncertain but likely involve more than simple proliferation and differentiation of the BMSCs. The type of local delivery of stem cells utilized within SCOTS may be critical to achieve such positive responses. Autologous stem cell therapy has proven to be a safe and promising treatment approach in a number of diseases, including retinal and optic nerve conditions. Patient enrollment in monitored clinical studies such as SCOTS is an important means to evaluate autologous stem cell treatment and its role in treating eye disease.
Footnotes
Conflicts of Interest: None declared.
Copyedited by Jackson C, Li CH, Song LP, Liu WJ, Zhao M
References
- Bunnell BA, Betancourt AM, Sullivan DE. New concepts on the immune modulation mediated by mesenchymal stem cells. Stem Cell Res Ther. 2010;1:34. doi: 10.1186/scrt34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen Q, Long Y, Yuan X, Zou L, Sun J, Chen S, Perez-Polo JR, Yang K. Protective effects of bone marrow stromal cell transplantation in injured rodent brain: synthesis of neurotrophic factors. J Neurosci Res. 2005;80:611–619. doi: 10.1002/jnr.20494. [DOI] [PubMed] [Google Scholar]
- Islam MN, Das SR, Emin MT, Wei M, Sun L, Westphalen K, Rowlands DJ, Quadri SK, Bhattacharya S, Bhattacharya J. Mitochondrial transfer from bone-marrow-derived stromal cells to pulmonary alveoli protects against acute lung injury. Nat Med. 2012;18:759–765. doi: 10.1038/nm.2736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson TV, Bull ND, Hunt DP, Marina N, Tomarev SI, Martin KR. Neuroprotective effects of intravitreal mesenchymal stem cell transplantation in experimental glaucoma. Invest Ophthalmol Vis Sci. 2010;51:2051–2059. doi: 10.1167/iovs.09-4509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li N, Li XR, Yuan JQ. Effects of bone-marrow mesenchymal stem cells transplanted into vitreous cavity of rat injured by ischemia/reperfusion. Graefes Arch Clin Exp Ophthalmol. 2009;247:503–514. doi: 10.1007/s00417-008-1009-y. [DOI] [PubMed] [Google Scholar]
- Nadri S, Yazdani S, Arefian E, Gohari Z, Eslaminejad MB, Kazemi B, Soleimani M. Mesenchymal stem cells from trabecular meshwork become photoreceptor-like cells on amniotic membrane. Neurosci Lett. 2013;541:43–48. doi: 10.1016/j.neulet.2012.12.055. [DOI] [PubMed] [Google Scholar]
- Ng TK, Fortino VR, Pelaez D, Cheung HS. Progress of mesenchymal stem cell therapy for neural and retinal diseases. World J Stem Cells. 2014;6:111–119. doi: 10.4252/wjsc.v6.i2.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwartz SD, Regillo CD, Lam BL, Eliott D, Rosenfeld PJ, Gregori NZ, Hubschman JP, Davis JL, Heilwell G, Spirn M, Maguire J, Gay R, Bateman J, Ostrick RM, Morris D, Vincent M, Anglade E, Del Priore LV, Lanza R. Human embryonic stem cell-derived retinal pigment epithelium in patients with age-related macular degeneration and Stargardt's macular dystrophy: follow-up of two open-label phase 1/2 studies. Lancet. 2015;385:509–516. doi: 10.1016/S0140-6736(14)61376-3. [DOI] [PubMed] [Google Scholar]
- Wilkins A, Kemp K, Ginty M, Hares K, Mallam E, Scolding N. Human bone marrow-derived mesenchymal stem cells secrete brain-derived neurotrophic factor which promotes neuronal survival in vitro. Stem Cell Res. 2009;3:63–70. doi: 10.1016/j.scr.2009.02.006. [DOI] [PubMed] [Google Scholar]
- Yu S, Tanabe T, Dezawa M, Ishikawa H, Yoshimura N. Effects of bone marrow stromal cell injection in an experimental glaucoma model. Biochem Biophys Res Commun. 2006;344:1071–1079. doi: 10.1016/j.bbrc.2006.03.231. [DOI] [PubMed] [Google Scholar]
- Zhao LR, Duan WM, Reyes M, Keene CD, Verfaillie CM, Low WC. Human bone marrow stem cells exhibit neural phenotypes and ameliorate neurological deficits after grafting into the ischemic brain of rats. Exp Neurol. 2002;174:11–20. doi: 10.1006/exnr.2001.7853. [DOI] [PubMed] [Google Scholar]