

James Bernat has been a leading advocate of donation after brain death (DBD) (Bernat 2014) and donation after circulatory death (DCD) (Bernat et al. 2010), as well as an eminent scholar regarding their philosophical foundations. He points out that brain death is still widely misunderstood—the misunderstanding is that those who are brain dead are not really dead. According to a seminal survey, two-thirds of Americans believe that patients diagnosed as brain dead are not legally dead (Siminoff, Burant, and Youngner 2004). Bernat argues that the biophilosophical justification for DBD is incomplete and that a more firmly grounded justification for DBD will improve public understanding of what brain death means through education; the latter seems unlikely because widespread confusion and misunderstanding has persisted 30 years after adoption of the Uniform Determination of Death Act (UDDA) (UDDA 1981). A brain-dead donor’s beating heart, rhythmic respiration, warm skin, and urine flow from a Foley catheter simply do not appear to be “real death” to most families and health professionals.
The concept of brain death was developed, articulated, and adopted by all 50 states over 30 years ago for the purpose of increasing the number of organs available for transplantation (Giacomini 1997). The concept has been successful in moving toward that goal, as Bernat (2014) has indicated, but despite the successes of organ donation and transplantation, a major problem remains: the growing gap between the number of organ donors and the need for medically suitable organs, resulting in thousands of deaths a year (Figure 1). Brain death was codified in law by the UDDA to satisfy the dead donor rule (DDR: removal of organs must not cause the death of the donor), so that physicians could determine and declare death without fear of criminal prosecution (Miller and Truog 2008). Increasing the supply of transplantable organs would lead to survival of more patients with end-organ failure. Yet paradoxically, the DDR may be responsible for several thousand deaths every year.
Figure 1.
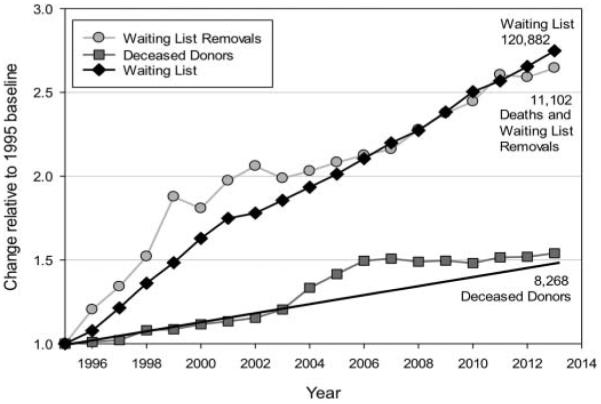
Relative change in transplant data. This graph depicts the change in deceased donors, all-organ waiting list, and deaths plus waiting list removals (virtually all are patients who became too sick to transplant and died off the list) relative to the 1995 baseline. The sharp rise in deceased donors in 2003–2006 reflects the results of intensive efforts to increase donation by the Organ Donation Breakthrough Collaborative (HRSA 2014b). The trend line shows that after the Collaborative ended, donation plateaued, placing the 2013 donation rate where it would have been if the collaborative had not occurred (source of data: HRSA 2014a).
Both DBD and DCD are useful legal fictions intended to satisfy the DDR (Truog and Miller 2014); they involve donation by individuals who are legally dead but are not biologically dead. DBD donors are not biologically dead because there has not been “irreversible cessation of all functions of the entire brain, including the brain stem” (as required by the UDDA)—for example, many patients who meet the criteria for brain death retain some homeostatic functions of the brainstem, such as temperature control and water and electrolyte balance.
DCD protocols require that circulation cease spontaneously after withdrawal of life support (a process that may take up to 60 minutes) and that an additional 2–5 minutes of circulatory arrest elapse before death is pronounced. As in the case of DBD, these donors are not biologically dead because death is pronounced a few minutes after circulatory arrest but the arrest is not irreversible—circulation can usually be restored even after much longer periods in individuals who have suffered unplanned circulatory arrest. Despite the absence of biological death, these individuals are legally dead because a physician has declared death “in accordance with accepted medical standards” (as required by the UDDA) (Sade 2011).
The legal fictions underlying DBD and DCD satisfy the DDR, and physicians’ feeling of freedom from the threat of prosecution led to the availability of a large number of organs for transplantation from deceased donors; these gains did not come without a cost, however. By observing the DDR, substantial numbers of organs have been lost to transplantation. In DCD, after withdrawal of life support, blood pressure declines over time (up to 60 minutes) before circulatory arrest occurs; during this time, when the falling mean arterial pressure reaches 50 mm Hg or less, organ perfusion becomes inadequate and organ damage ensues due to warm ischemia. Death is pronounced 2–5 minutes after circulatory arrest, adding to the warm ischemic time. Thus, many organs can no longer be transplanted because of tissue damage; for example, in 2013 not a single heart was transplanted from a DCD donor because of warm ischemia. Instead of allowing such damage and loss of organs, donors facing imminent death could be brought to the operating room, with the donor’s circulation allowed to remain intact until organs are removed. For the purpose of this discussion, we call this procedure donation by the imminently dead (DID).
We can make crude estimates of how many organs could be generated if the DDR were abandoned by analyzing the most recent available national data on organ donation and transplantation (Table 1) (Health Resources and Services Administration. [HRSA] 2014a). In 2013, 22,073 organs were transplanted from 8,268 deceased donors (both DBD and DCD), averaging 2.67 organs per donor. We have no way of knowing how many additional organs could be recovered from donors who were not subjected to organ-damaging processes, but by treating all potential donors as DID donors, much organ damage can be avoided: in DCD donors, ischemic damage from extensive hypoperfusion, and in DBD donors, the damaging transition from recognition of imminent death to brain death. Hard data on avoidable tissue damage are not available, so we cannot accurately calculate the number of organs that are now being lost and could be saved. Nevertheless, we have crudely estimated the possible increase in transplanted organs by assuming that DID could achieve the Organ Donation Breakthrough Collaborative national goal for recovery of organs per deceased donor: 3.75 (HRSA 2014b). Based on these calculations, we roughly estimate a gain of 2,248 organs from DCD donors (Table 1).
Table 1.
Number of organs potentially generated under a DID protocol
| Organs transplanted (2013) |
Donors (2013) |
Organs/donor (2013) |
Projected increase in number of organs |
Projected total number of organs |
|
|---|---|---|---|---|---|
| DCD | 2,271 | 1,205 | 1.88 | 2,248 | 4,519 |
| DBD | 19,802 | 7,063 | 2.80 | 6,684 | 26,486 |
| Total | 22,073 | 8,268 | 2.67 | 8,932 | 31,005 |
Note. Crude estimates are based on available national data on organ donation and transplantation for 2013 (HRSA 2014a). The Organ Donation Breakthrough Collaborative national goal for recovery of organs per deceased donor is 3.75 (HRSA 2014b). Projected increase in number of organs D [3.75 – (organs/donor) × (number of donors)]. Projected total number of organs D (organs transplanted C projected increase in number of organs).
DBD, donation after brain death; DCD, donation after circulatory death; DDR, dead donor rule; DID, donation by the imminently dead.
But that is not the end of the benefits of abandoning the DDR. In DBD donation, rather than allowing brain-injured patients to progress to brain death, as soon as they are identified as facing imminent death they could be considered DID donors, avoiding the physiological abnormalities and damage associated with the time delays and neurological and hormonal changes of brain death. Fewer organs would be damaged, allowing recovery of as many as 6,684 additional organs, saving thousands more lives (Table 1).
Thus, treating all imminently dead patients as potential DID donors could add nearly 9,000 organs to the national transplant program. If the actual number of organs were only a fraction of this admittedly rough approximation, there is still the potential for saving thousands of lives a year. In order to arrive at this point, the DDR would have to be replaced by an understanding that it is permissible to recover organs from those who are nearly dead and have requested to be organ donors after a thoroughgoing process of informed consent. Arguably, all that is ethically required for organs to be removed is that consent for donation be voluntary and informed (i.e., informed consent), and that death be imminent (Miller and Truog 2008).
An important ethical reason for using a DID rather than DCD or DBD protocol arises from one of the fundamental principles of ethics: respect for the patient’s autonomy. A DID protocol will result in transplantation of a greater number of healthier organs than DCD or DBD. When individuals decide to be organ donors, their best interest lies in making the best possible use of their organs for the purpose they intend; that is, their autonomous decision to donate is best respected with the DID protocol. The wastage of organs associated with the DCD and the DBD protocols is clearly contrary to the wishes of the donor.
Bernat and many others have argued that abandoning the DDR would be socially unacceptable, but several observations undermine that objection (Fost 1999). The concept of brain death was meaningless until technological advances produced ventilators and other means of life support in the 1950s and 1960s; thus, brain death is clearly a social construction. Revision of social constructions has been frequent in the past; for example, in vitro fertilization and recombinant DNA research were once widely condemned and are now routinely accepted. Kidney donation by living persons into the general pool for undesignated recipients (Good Samaritan donation) was once considered prima facie evidence of mental illness, but now is considered acceptable and even laudable after appropriate psychosocial evaluation. Moreover, for several years organs were recovered from donors in states that had not yet adopted the UDDA, so the practice violated the DDR and was supposedly illegal, yet no public outcry condemned these practices. Although the majority of Americans believe that brain-dead individuals are not really dead, there has been no general outcry against procuring organs from these presumably living donors. It is extremely difficult to predict public reaction, and the assumption that the response to taking organs from those who are imminently dead would be negative may be greatly exaggerated.
The space allowed for this brief commentary does not permit consideration of the many challenging questions raised by DID—we present these thoughts as matters for future discussion. Changing widespread misunderstandings is never easy, but if the goal is maximizing the number of organs available for transplantation in an ethically justifiable manner, the facts presented here could help move public opinion toward recovering organs from the imminently dead, thus abandoning the DDR. This would have the salutary effect of producing intellectual clarity and consistency, and also would save lives by substantially increasing the number of organs available for transplantation.
ACKNOWLEDGMENTS
We are grateful for the assistance, advice, and support of Nancy Kay, President and Chief Executive Officer of LifePoint, Inc., South Carolina’s organ procurement organization.
FUNDING
Dr. Sade’s role in this publication was supported by the South Carolina Clinical & Translational Research Institute, Medical University of South Carolina’s Clinical and Translational Science, award number UL1RR029882. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Contributor Information
Robert M. Sade, Medical University of South Carolina
Andrea D. Boan, Medical University of South Carolina
REFERENCES
- Bernat JL. Whither brain death? American Journal of Bioethics. 2014;14(8):3–8. doi: 10.1080/15265161.2014.925153. [DOI] [PubMed] [Google Scholar]
- Bernat JL, Capron AM, Bleck TP, et al. The circulatory-respiratory determination of death in organ donation. Critical Care Medicine. 2010;38(3):963–970. doi: 10.1097/CCM.0b013e3181c58916. [DOI] [PubMed] [Google Scholar]
- Fost N. The unimportance of death. In: Youngner SJ, Arnold RM, Shapiro R, editors. The definition of death: Contemporary controversies. Johns Hopkins University Press; Baltimore, MD: 1999. pp. 161–178. [Google Scholar]
- Giacomini M. A change of heart and a change of mind? Technology and the redefinition of death in 1968. Social Science & Medicine. 1997;44(10):1465–1482. doi: 10.1016/s0277-9536(96)00266-3. [DOI] [PubMed] [Google Scholar]
- Health Resources and Services Administration Health Resources and Services Administration. Data reports: National data. 2014a Available at: http://optn.transplant.hrsa.gov/latestData/step2.asp (accessed May 8, 2014)
- Health Resources and Services Administration Health Resources and Services Administration. Donation and Transplantation community of practice. 2014b Available at: http://organdonor.gov/dtcp/dtcp.html (accessed May 8, 2014)
- Miller FG, Truog RD. Rethinking the ethics of vital organ donations. Hastings Center Report. 2008;38(6):38–46. doi: 10.1353/hcr.0.0085. [DOI] [PubMed] [Google Scholar]
- Sade RM. Brain death, cardiac death, and the dead donor rule. Journal of the South Carolina Medical Association. 2011;107(4):146–149. [PMC free article] [PubMed] [Google Scholar]
- Siminoff LA, Burant C, Youngner SJ. Death and organ procurement: Public beliefs and attitudes. Kennedy Institute of Ethics Journal. 2004;14(3):217–234. doi: 10.1353/ken.2004.0034. [DOI] [PubMed] [Google Scholar]
- Truog RD, Miller FG. Changing the conversation about brain death. American Journal of Bioethics. 2014;14(8):9–14. doi: 10.1080/15265161.2014.925154. [DOI] [PubMed] [Google Scholar]
- Uniform Determination of Death Act National Council of Commissioners of Uniform State Laws. Uniform Determination of Death Act. 1981 Available at: http://pntb.org/wordpress/wpcontent/uploads/Uniform-Determination-of-Death-1980_5c.pdf (accessed May 8, 2014)