

Abstract
Background
Improvement in the daily physical activity (PA) is important for the management of chronic obstructive pulmonary disease (COPD). However, the effects of pharmacologic treatment on PA are not well understood. We evaluated the effects of additional medications, including bronchodilator with or without inhaled corticosteroid, based on airflow limitation and breathlessness on the PA in COPD patients and the factors that could predict or affect the improvement in PA.
Methods
A prospective non-randomized observational study was employed. Twenty-one COPD subjects without any other diseases that might reduce PA were recruited. The PA was measured with a triaxial accelerometer for 2 weeks, and pulmonary function tests and incremental shuttle walking tests were administered before and after 4-week treatment with an additional medication.
Results
Bronchodilation was obtained by additional medication. The mean values of PA evaluated by metabolic equivalents (METs) at ≥3.0 METs and the duration of PA at ≥3.0 METs and ≥3.5 METs were improved by medication. The % change in the duration of PA at ≥3.5 METs was significantly correlated with the baseline functional residual capacity (FRC), residual volume, and inspiratory capacity/total lung capacity. However, the % change in the duration of PA at any intensity was not correlated with the % changes of any values of the pulmonary function tests or incremental shuttle walking test except the PA at ≥2.5 METs with FRC.
Conclusion
Medication could improve the PA in patients with COPD, especially at a relatively high intensity of activity when medication was administered based on airflow limitation and breathlessness. The improvement was seen in the patients with better baseline lung volume, but was not correlated with the improvements in the pulmonary function tests or exercise capacity.
Keywords: COPD, accelerometer, bronchodilator, pulmonary function, predictor
Introduction
The daily physical activity (PA) is reduced in patients with chronic obstructive pulmonary disease (COPD) compared to healthy subjects.1–6 As the PA is related to the decline of lung function,7 hospitalizations,8,9 and mortality10 and is a factor reflecting the highest relative risk of death in COPD,11 the maintenance or improvement in PA is an important target for the management of COPD.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommends the use of long-acting bronchodilator (BD), such as anticholinergics, beta-2-adrenoceptor agonists, and in some cases, inhaled corticosteroid (ICS), for the management of stable COPD patients.12 There have been only a few reports about the effect of BD on PA. In some reports, BD, especially indacaterol13,14 and aclidinium,15 improved PA, but in other reports, BD, especially indacaterol16,17 and tiotropium,18 did not. BD can improve exercise capacity,19,20 but it is still unclear whether BD can improve the daily PA in patients with COPD. GOLD also recommends that COPD patients should be assessed using risk factors (airflow limitation or exacerbation) and symptoms or breathlessness for the management.12
We evaluated the effects of additional pharmacologic treatment based on airflow limitation and breathlessness on the PA in patients with COPD monitored using an Actimarker® (Panasonic, Osaka, Japan), a compact-sized, well-validated, triaxial accelerometer.21 Furthermore, we also evaluated the physiological factors that could predict or affect the improvement in PA.
Subjects and methods
Subjects
Stable COPD patients, aged 50 or older and recruited from among the outpatients of Wakayama Medical University Hospital, were either not using a BD or were taking a long-acting muscarinic antagonist (LAMA) or a long-acting beta-2 adrenergic agonist (LABA), but not both. Patients using oxygen therapy or suffering from other diseases that might reduce PA and patients who received respiratory rehabilitation within 6 months before the entry were excluded. COPD was diagnosed as post-BD forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) <0.7. The patients did not have any other pulmonary diseases such as asthma or bronchiectasis.12
Protocol
Patients wore an Actimarker® the whole day, except while bathing, for 2 weeks and performed pulmonary function tests and incremental shuttle walking test (ISWT) on the last day of the PA measurement. They were additionally treated with medication and then evaluated for their PA after 4–6 weeks from the beginning of treatment and performed pulmonary function tests and ISWT on the last day of the PA measurement. The effects of medication on PA and other parameters were evaluated. Then, in order to determine if there were some predictable factors that could improve PA by pharmacologic treatment, % change in PA was compared with the baseline physiological parameters. Furthermore, in order to evaluate the factors that could affect the improvement in PA, % change in PA was compared with % change in physiological parameters.
Written informed consent was obtained from all participants, and the study was approved by the local ethics committee (Committee: IRB Committee of Wakayama Medical University, approval number: 968, approval date: May 30, 2011; Clinical Trial Registration: UMIN, registration number: UMIN000006293, registration date: September 15, 2011 [http://www.umin.ac.jp]).
Selection of BD
Which type of additional medication was decided according to the GOLD stage, the Modified Medical Research Council (MMRC) dyspnea scale, and the baseline treatment. The details are presented in Table 1. Briefly, 1) in cases of stage 1 or 2, MMRC 0 or 1 (group A in GOLD classification), and no BD treatment at baseline, the final treatment was either LAMA or LABA; 2) in cases of stage 1 or 2, MMRC 2 or more (group B in GOLD), and no BD; in cases of stage 1 or 2, any MMRC (group A or B in GOLD), and one BD; and in cases of stage 3 or 4, MMRC 0 or 1 (group C in GOLD), and no or one BD, the final treatment was both LAMA and LABA; and 3) in cases of stage 3 or 4, MMRC 2 or more (group D in GOLD), and no or one BD, the final treatment was both LAMA and ICS/LABA combination. The kind of additional LABA was salmeterol 50 μg twice daily or tulobuterol hydrochloride patch 2 mg once a day, the LAMA was tiotropium HandiHaler 18 μg once a day, and the ICS/LABA combination was fluticasone propionate 250 μg with salmeterol 50 μg twice daily or budesonide 320 μg with formoterol fumarate dehydrate 9 μg twice daily.
Table 1.
Criteria for selection of bronchodilator
| GOLD stage | MMRC scale | Baseline treatment | Final treatment | No of patients |
|---|---|---|---|---|
| 1 or 2 | 0–1 | None | LAMA or LABA | 5 |
| 1 or 2 | 2–4 | None | LAMA + LABA | 3 |
| 1 or 2 | Any | LAMA or LABA | LAMA + LABA | 6 |
| 3 or 4 | 0–1 | None or LAMA or LABA | LAMA + LABA | 3 |
| 3 or 4 | 2–4 | None or LAMA or LABA | LAMA + ICS/LABA | 4 |
Abbreviations: GOLD, Global Initiative for Chronic Obstructive Lung Disease; MMRC, Modified Medical Research Council; None, no bronchodilator; LAMA, long-acting muscarinic antagonist; LABA, long-acting beta-2 adrenergic agonist; ICS, inhaled corticosteroid.
Assessment of PA
The Actimarker® is a small (74.5 mm ×13.4 mm ×34.0 mm) and lightweight (36.0 g) triaxial accelerometer that is worn only at the waist and that can continuously monitor activity for over 1 month. It collects the data of triaxial acceleration at 20 Hz, and the standard deviation of the data for 1 minute is defined as the mean value of acceleration. The value of metabolic equivalents (METs) is calculated from the linear regression formula produced by the relationship between the mean value of acceleration and the METs measured using a respiratory gas metabolic system.22,23 Actimarker® has already been validated for evaluating the PA of COPD in terms of the intensities.21
The detection of reproducible data is very important for the evaluation of PA because PA can easily fluctuate day by day. As the PA in COPD could be suppressed on a rainy day21 or holiday,24,25 the data of these days should be excluded to obtain reproducible data. The recommended number of measurement days in most of the previous reports was 3–5.1,24–26 In the case of Actimarker®, we have reported it to be 3.21 Therefore, in order to obtain a representative value of the daily PA, we excluded the data of rainy days, weekend days, and holidays and also excluded the data of the first and last days because data of a whole day were not obtained. Finally, we accepted the data of the first 3 full days from among the included days of the 2 weeks. The mean values of the duration of PA from the extracted 3 days were employed as the representative PA in the patients with COPD.
Assessment of physiological properties
The lung function was evaluated by CHESTAC-8800 DN type (Chest Ltd., Tokyo, Japan) according to the recommendations of the American Thoracic Society/European Respiratory Society.27 ISWT was performed according to Singh’s method (Japanese license number: 410).28
Statistical analysis
Analyses were performed using GraphPad Prism 5 (Graph-Pad Software, Inc., La Jolla, CA, USA). Paired t-test was used for the comparisons of pulmonary functions and ISWT before and after treatment. Wilcoxon signed-rank test was used for the comparisons of PA before and after treatment. One-way analysis of variance (ANOVA) was used for finding the % change in PA among the different intensities of PA. Spearman’s correlation was used for the relationship between % change in PA and baseline values of ISWT or pulmonary function tests by treatment, and between % change in PA and % change in pulmonary function tests or ISWT by treatment. Comparisons were considered significant for P-values of less than 0.05.
Results
The numbers of patients with stages I, II, III, and IV were 4, 10, 4, and 3, respectively, and those with MMRC 0, 1, 2, 3, and 4 were 7, 7, 5, 2 and 0, respectively (Table 2). The numbers of patients in groups A, B, C, and D of GOLD classification were 10, 4, 4, and 3, respectively. At baseline, eleven patients received no BD, nine received LAMA, and one received LABA. Finally, five patients received either LAMA or LABA, 12 both LAMA and LABA, and four both LAMA and ICS/LABA combination (Table 1).
Table 2.
Characteristics of patients
| Sex (M/F) | 21/0 |
| Age (years) | 70.7±7.7 |
| BMI (kg/m2) | 21.3±3.3 |
| Smoking | |
| Cur/Ex/Non | 6/15/0 |
| Pack-year | 63.7±31.1 |
| MMRC scale (0/1/2/3/4) | 7/7/5/2/0 |
| Staging (I/II/III/IV) | 4/10/4/3 |
| Pulmonary function | |
| FVC (L) | 3.50±0.65 |
| FEV1 (L) | 1.72±0.63 |
| FEV1 % (%) | 48.2±13.3 |
| FEV1 % predicted (%) | 59.8±21.7 |
| IC (L) | 2.13±0.37 |
| IC/TLC (%) | 33.3±6.4 |
| FRC (L) | 4.32±0.81 |
| RV (L) | 2.84±0.62 |
| TLC (L) | 6.47±0.85 |
| DLCO (mL/min/mmHg) | 14.87±5.16 |
| DLCO/VA (mL/min/mmHg/L) | 3.24±1.15 |
Abbreviations: BMI, body mass index; Cur, current smoker; Ex, ex smoker; Non, nonsmoker; MMRC, Modified Medical Research Council; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; FEVl%, 100 × FEVl/FVC; FEVl% predicted, 100 × FEVl/predicted FEVl; IC, inspiratory capacity; TLC, total lung capacity; FRC, functional residual capacity; RV, residual volume; DLCO, pulmonary carbon monoxide diffusing capacity; min, minute; VA, alveolar volume.
After pharmacologic treatment, vital capacity, inspiratory capacity (IC), FVC, FEV1, residual volume (RV), and ISWT were significantly improved, and the changes in the mean values of IC, FEV1, and ISWT were 0.14 L, 0.14 L, and 35 m, respectively (Table 3), suggesting that effective bronchodilation had been obtained. The PA level evaluated by the values of the summation of METs multiplied by hours (METs·hr) at ≥3.0 METs was significantly improved (P=0.02) (Figure 1). The durations of activity were improved at intensities ≥3.0 METs and ≥3.5 METs, but not at ≥2.0 METs and ≥2.5 METs (Figure 2). Three patients at ≥3.0 METs and five patients at ≥3.5 METs improved their PA by more than 100%. Among these patients, only one patient improved at both intensities and the others improved only at one of the intensities. Furthermore, eight patients at ≥3.0 METs and five patients at ≥3.5 METs improved their PA by more than 50%, and numerically, 15 of 21 patients (71.4%) improved at ≥3.0 METs and 16 (76.2%) improved at ≥3.5 METs (Figure 3). The mean value of the % change in PA was increased as the intensity of activity increased, but the difference was not statistically significant by one-way ANOVA (P=0.193) (Figure 3).
Table 3.
Effects of medication on pulmonary function tests and ISWT
| Variables | Pre | Post | P-value |
|---|---|---|---|
| VC (L) | 3.58±0.65 | 3.76±0.63 | 0.007 |
| IC (L) | 2.13±0.37 | 2.27±0.35 | 0.001 |
| FVC (L) | 3.50±0.65 | 3.63±0.55 | 0.008 |
| FEV1 (L) | 1.72±0.63 | 1.86±0.58 | 0.001 |
| FRC (L) | 4.32±0.81 | 4.24±0.85 | 0.249 |
| RV (L) | 2.84±0.62 | 2.67±0.61 | 0.015 |
| TLC (L) | 6.47±0.85 | 6.46±0.97 | 0.936 |
| DLCO (mL/min/mmHg) | 14.87±5.16 | 14.61±5.15 | 0.293 |
| DLCO/VA (mL/min/mmHg/L) | 3.24±1.15 | 3.20±1.15 | 0.438 |
| ISWT (m) | 464.7±118.0 | 499.4±108.7 | 0.033 |
Abbreviations: ISWT, incremental shuttle walking test; VC, vital capacity; IC, inspiratory capacity; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; FRC, functional residual capacity; RV, residual volume; TLC, total lung capacity; DLCO, pulmonary carbon monoxide diffusing capacity; VA, alveolar volume; min, minute.
Figure 1.
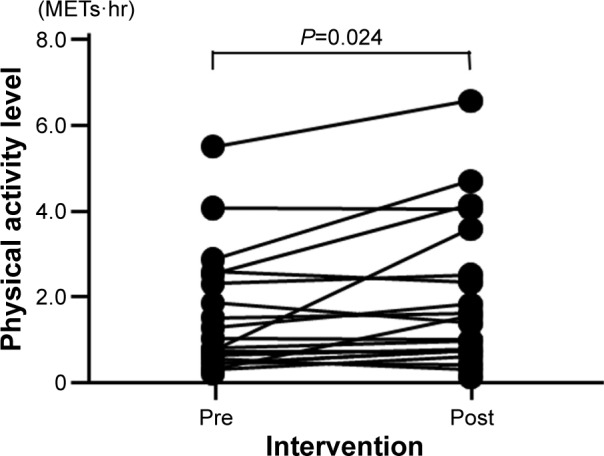
Effect of medication on the PA level.
Abbreviations: PA, physical activity; METs·hr, metabolic equivalents multiplied by hours.
Figure 2.

Effects of medication on the duration of PA.
Abbreviations: PA, physical activity; METs, metabolic equivalents; min, minutes.
Figure 3.
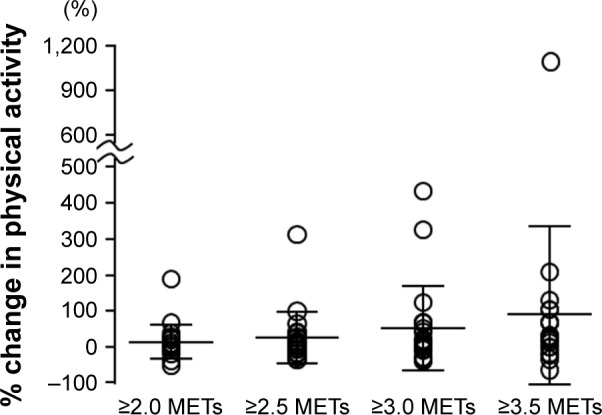
The degree of improvement in PA according to the intensity.
Notes: Horizontal lines indicate mean ± SD. P=0.193 with one-way analysis of variance.
Abbreviations: PA, physical activity; SD, standard deviation; METs, metabolic equivalents.
The % change in PA at ≥3.5 METs by medication was correlated with the baseline values of functional residual capacity (FRC), RV, and IC/total lung capacity (TLC), and the % change in PA at ≥3.0 METs was correlated with the baseline values of FVC (Table 4). Although the % change in PA at ≥2.5 METs by medication was weakly correlated only with the % change in FRC, the % changes in PA at other intensities were not correlated with the % changes in any pulmonary function tests or ISWT (Table 5).
Table 4.
Correlation coefficients between % change in PA and baseline pulmonary function tests or ISWT
| Variables | ≥2.0 METs | ≥2.5 METs | ≥3.0 METs | ≥3.5 METs | ≥3.0 METs⋅hr |
|---|---|---|---|---|---|
| VC | 0.094 | 0.326 | 0.418 | 0.237 | 0.352 |
| FVC | 0.094 | 0.334 | 0.473a | 0.228 | 0.407 |
| FEV1 | 0.405 | 0.387 | 0.427 | 0.104 | 0.365 |
| FRC | −0.247 | 0.068 | 0.008 | −0.537a | −0.052 |
| RV | −0.396 | −0.179 | −0.384 | −0.543a | −0.425 |
| TLC | −0.271 | 0.086 | −0.085 | −0.298 | −0.162 |
| IC/TLC | 0.326 | 0.216 | 0.395 | 0.518a | 0.442 |
| DLCO | 0.381 | 0.147 | 0.352 | 0.262 | 0.382 |
| ISWT | 0.060 | 0.265 | 0.335 | −0.065 | 0.233 |
Note:
P<0.05.
Abbreviations: PA, physical activity; ISWT, incremental shuttle walking test; METs, metabolic equivalents; METs·hr, METs multiplied by hours; VC, vital capacity; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; FRC, functional residual capacity; RV, residual volume; IC, inspiratory capacity; TLC, total lung capacity; DLCO, pulmonary carbon monoxide diffusing capacity.
Table 5.
Correlation coefficients between % change in PA and % change in pulmonary function tests or ISWT
| Variables | ≥2.0 METs | ≥2.5 METs | ≥3.0 METs | ≥3.5 METs | ≥3.0 METs⋅hr |
|---|---|---|---|---|---|
| VC | −0.170 | −0.102 | −0.020 | 0.277 | −0.003 |
| IC | −0.130 | 0.118 | 0.071 | −0.031 | 0.081 |
| FVC | 0.072 | 0.079 | 0.114 | 0.153 | 0.166 |
| FEV1 | −0.116 | 0.117 | 0.283 | 0.302 | 0.319 |
| FRC | −0.296 | −0.468a | −0.374 | 0.065 | −0.375 |
| RV | 0.062 | −0.130 | −0.209 | 0.059 | −0.235 |
| TLC | −0.238 | −0.300 | −0.304 | 0.101 | −0.316 |
| DLCO | −0.186 | −0.309 | −0.250 | −0.298 | −0.201 |
| ISWT | −0.332 | −0.401 | −0.123 | 0.439 | −0.059 |
Note:
P<0.05.
Abbreviations: PA, physical activity; ISWT, incremental shuttle walking test; METs, metabolic equivalents; METs·hr, METs multiplied by hours; VC, vital capacity; IC, inspiratory capacity; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; FRC, functional residual capacity; RV, residual volume; TLC, total lung capacity; DLCO, pulmonary carbon monoxide diffusing capacity.
Discussion
We demonstrated that pharmacologic treatment significantly improved the PA at a relatively high intensity in patients with COPD when medication was administered based on airflow limitation and breathlessness. The degree of the improvement in PA at ≥3.5 METs was correlated with the baseline pulmonary function, but was not correlated with the degree of improvement in pulmonary function or ISWT.
Pharmacologic treatment improved the PA level (METs·hr) and the duration of PA. Hataji et al13 and Watz et al14 reported that indacaterol improved PA, and Beeh et al15 reported that aclidinium improved PA, which were compatible with our results. However, O’Donnell et al16 and Nishijima et al17 reported that indacaterol did not improve PA and Troosters et al18 reported that tiotropium did not improve PA. The differences in these reports might be caused by differences in several factors, including the index of PA, the duration of medication, the kind of accelerometers, the conditions of data collection, and also the distribution of airflow limitation or breathlessness of patients.
In the current study, we selected additional medication based on airflow limitation, breathlessness, and baseline treatment of BD, which is in accordance with the GOLD recommendations12 and a realistic approach to treatment. In all the previous reports,13–18 the effects of BD were evaluated without taking into account breathlessness or airflow limitation. This might be one of the reasons for the difference in their results.
We recruited patients with both no and one BD at baseline. Among the patients who improved their PA by more than 100% at ≥3.0 METs (three patients) or ≥3.5 METs (five patients), two patients received no BD at baseline (two of eleven patients with no BD), one patient received one BD (one of ten patients with one BD) at ≥3.0 METs (P=0.593 with chi-square test), three patients received no BD (three of eleven), and two patients received one BD (two of ten) at ≥3.5 METs (P=0.696). Among the patients who improved their PA by more than 50% at ≥3.0 METs (five patients) or ≥3.5 METs (eight patients), three patients received no BD (three of eleven) and two received one BD (two of ten) at ≥3.0 METs (P=0.696) and five received no BD (five of eleven) and three received one BD (three of ten) at ≥3.5 METs (P=0.466). Though the rate of improvement in patients with no BD was numerically higher than the patients with one BD at the baseline, there was no significant difference between the two groups.
Concerning the index of PA, in addition to the current study, Hataji et al13 and Watz et al14 employed the duration of PA and the mean intensity of PA as indices and both were improved by BD. Beeh et al15 reported that the duration of PA was improved, but the mean intensity of PA was not. O’Donnell et al16 employed only the mean intensity of PA as an index, and it was not improved by BD. Vorrink et al reported that the average percentage of PA for COPD patients vs controls was as follows: for intensity, 75%; for duration, 57%; and for PA counts, 56%,29 which implies that the mean intensity of PA might be a less sensitive index than the duration of PA.
A positive effect of medication was observed in the duration of PA at relatively high intensities (≥3.0 METs and ≥3.5 METs), but not at low intensities. In the report of Hataji et al13 indacaterol improved the duration of PA at 2.9 METs or more but not at 2.3 METs or less. This is compatible with our results. Furthermore, our recent pilot study demonstrated that transdermal tulobuterol improved PA only at ≥3.5 METs in patients with COPD.30 These results suggest that pharmacologic treatment could facilitate a relatively high intensity of PA.
The degree of the improvement in PA at ≥3.5 METs by medication was correlated with the baseline values of FRC, RV, and IC/TLC, suggesting that patients with better baseline pulmonary function might show greater improvements in their PA. Walker et al reported that the improvement in PA measured by a uniaxial accelerometer after 8-week rehabilitation was positively correlated with the baseline FEV1,31 which was compatible with our results. The decline in FEV1 was suppressed by BD more in stage II than in stage III or IV.32–34 BD might improve PA and pulmonary function in patients with better baseline pulmonary function.
Unexpectedly, the % change in the duration of PA by medication was not correlated with the % changes of any values of pulmonary function tests or ISWT. It has been reported that the increased PA was not correlated with the improved pulmonary function test score14 or increased exercise capacity.15 These reports are compatible with our results. The reason why they were not correlated is unclear, but one possibility is that the rapidity of improvement in PA might differ among parameters. Exercise capacity, quality of life, and FEV1 were improved by pulmonary rehabilitation at 3 months, while walking time was not improved at 3 months but was improved at 6 months in COPD patients.35 In most of the studies about the efficacy of BD on PA, the efficacy was evaluated at 3 weeks or 4 weeks.13–16,30 The appearance of an adequate effect on PA might require more time than that on exercise capacity or pulmonary function. There was only one report with a 24-week placebo-control design in which the PA was not improved by tiotropium compared to placebo.18 In this report, however, the effects of seasonal differences, especially temperature, were not eliminated, and the baseline values of the duration of PA were largely different between the tiotropium group and placebo group.
Another possible reason for the non-correlation between % change in PA and those of pulmonary function tests or ISWT was that the improvement in PA by medication was derived not only from pulmonary function but also from other factors, including psychological or cardiovascular components. In some patients, medication might directly or indirectly influence factors other than pulmonary function.
There are several limitations that need to be addressed. First, the number of recruited patients was small. Though consideration of the conditions of data collection could provide us more reproducible results with a relatively smaller number of subjects, this study may not be conclusive. A larger study is required to clarify further the effect of pharmacologic treatment on PA in patients with COPD. Second, this study was a non-randomized and short-term study. A randomized study with a longer treatment duration considering seasonal effects should be performed. Third, the baseline and additional treatments were not fixed. As we aimed to evaluate the effect of pharmacologic treatment but not the effect of a specific BD, we recruited patients with no or one BD at baseline and added another BD according to the recommendation of the GOLD guideline.12 Fourth, though the study subjects had not been diagnosed as having comorbidities, subclinical conditions, including cardiovascular dysfunction, depression, osteoporosis, or muscular weakness, were not completely excluded. The influence of comorbidities and muscular weakness on the PA in patients with COPD should be elucidated in future studies.
In conclusion, pharmacologic treatment could improve the duration of a relatively high intensity of PA in patients with COPD when medication was administered based on airflow limitation and breathlessness. The improvement in PA was correlated with the baseline pulmonary function but not with the improvement in pulmonary function test scores or exercise capacity.
Acknowledgments
The authors thank Manabu Nishigai, Yuichi Honda, and Akihito Sugino for technical support and assistance with statistical analysis and also Brent Bell for reading the manuscript. This study was supported by JSPS KAKENHI grant number 24591136.
Footnotes
Author contributions
Y Minakata performed all procedures; Y Morishita set and analyzed the accelerometer; and T Ichikawa, K Akamatsu, T Hirano, M Nakanishi, K Matsunaga, and M Ichinose recruited subjects. All authors contributed to the writing of the manuscript and have approved the final version for submission. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest in this work.
References
- 1.Steele BG, Holt L, Belza B, Ferris S, Lakshminaryan S, Buchner DM. Quantitating physical activity in COPD using a triaxial accelerometer. Chest. 2000;117(5):1359–1367. doi: 10.1378/chest.117.5.1359. [DOI] [PubMed] [Google Scholar]
- 2.Watz H, Waschki B, Boehme C, Claussen M, Meyer T, Magnussen H. Extrapulmonary effects of chronic obstructive pulmonary disease on physical activity: a cross-sectional study. Am J Respir Crit Care Med. 2008;177(7):743–751. doi: 10.1164/rccm.200707-1011OC. [DOI] [PubMed] [Google Scholar]
- 3.Pitta F, Troosters T, Spruit MA, Probst VS, Decramer M, Gosselink R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(9):972–977. doi: 10.1164/rccm.200407-855OC. [DOI] [PubMed] [Google Scholar]
- 4.Esteban C, Quintana JM, Aburto M, et al. Impact of changes in physical activity on health-related quality of life among patients with COPD. Eur Respir J. 2010;36(2):292–300. doi: 10.1183/09031936.00021409. [DOI] [PubMed] [Google Scholar]
- 5.Benzo RP, Chang CC, Farrell MH, et al. NETT Research Group Physical activity, health status and risk of hospitalization in patients with severe chronic obstructive pulmonary disease. Respiration. 2010;80(1):10–18. doi: 10.1159/000296504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Minakata Y, Sugino A, Kanda M, et al. Reduced level of physical activity in Japanese patients with chronic obstructive pulmonary disease. Respir Investig. 2014;52(1):41–48. doi: 10.1016/j.resinv.2013.06.002. [DOI] [PubMed] [Google Scholar]
- 7.Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Anto JM. Regular physical activity modifies smoking-related lung function decline and reduces risk of chronic obstructive pulmonary disease: a population-based cohort study. Am J Respir Crit Care Med. 2007;175(5):458–463. doi: 10.1164/rccm.200607-896OC. [DOI] [PubMed] [Google Scholar]
- 8.Garcia-Aymerich J, Farrero E, Felez MA, Izquierdo J, Marrades RM, Anto JM. Risk factors of readmission to hospital for a COPD exacerbation: a prospective study. Thorax. 2003;58(2):100–105. doi: 10.1136/thorax.58.2.100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pitta F, Troosters T, Probst VS, Spruit MA, Decramer M, Gosselink R. Physical activity and hospitalization for exacerbation of COPD. Chest. 2006;129(3):536–544. doi: 10.1378/chest.129.3.536. [DOI] [PubMed] [Google Scholar]
- 10.Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Anto JM. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax. 2006;61(9):772–778. doi: 10.1136/thx.2006.060145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Waschki B, Kirsten A, Holz O, et al. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohort study. Chest. 2011;140(2):331–342. doi: 10.1378/chest.10-2521. [DOI] [PubMed] [Google Scholar]
- 12.global Initiative for Chronic Obstructive Lung Disease Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2014. [Accessed November, 2014]. Available from: www.goldcopd.org/
- 13.Hataji O, Naito M, Ito K, Watanabe F, Gabazza EC, Taguchi O. Indacaterol improves daily physical activity in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2013;8:1–5. doi: 10.2147/COPD.S38548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Watz H, Krippner F, Kirsten A, Magnussen H, Vogelmeier C. Indacaterol improves lung hyperinflation and physical activity in patients with moderate chronic obstructive pulmonary disease – a randomized, multicenter, double-blind, placebo-controlled study. BMC Pulm Med. 2014;14:158. doi: 10.1186/1471-2466-14-158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Beeh KM, Watz H, Puente-Maestu L, et al. Aclidinium improves exercise endurance, dyspnea, lung hyperinflation, and physical activity in patients with COPD: a randomized, placebo-controlled, crossover trial. BMC Pulm Med. 2014;14(1):209. doi: 10.1186/1471-2466-14-209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.O’Donnell DE, Casaburi R, Vincken W, et al. INABLE 1 Study Group Effect of indacaterol on exercise endurance and lung hyperinflation in COPD. Respir Med. 2011;105(7):1030–1036. doi: 10.1016/j.rmed.2011.03.014. [DOI] [PubMed] [Google Scholar]
- 17.Nishijima Y, Minami S, Yamamoto S, et al. Influence of indacaterol on daily physical activity in patients with untreated chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2015;10(1):439–444. doi: 10.2147/COPD.S76836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Troosters T, Sciurba FC, Decramer M, et al. Tiotropium in patients with moderate COPD naive to maintenance therapy: a randomised placebo-controlled trial. NPJ Prim Care Respir Med. 2014;24:14003. doi: 10.1038/npjpcrm.2014.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.O’Donnell DE, Voduc N, Fitzpatrick M, Webb KA. Effect of salmeterol on the ventilatory response to exercise in chronic obstructive pulmonary disease. Eur Respir J. 2004;24(1):86–94. doi: 10.1183/09031936.04.00072703. [DOI] [PubMed] [Google Scholar]
- 20.Bedard ME, Brouillard C, Pepin V, et al. Tiotropium improves walking endurance in COPD. Eur Respir J. 2012;39(2):265–271. doi: 10.1183/09031936.00059511. [DOI] [PubMed] [Google Scholar]
- 21.Sugino A, Minakata Y, Kanda M, et al. Validation of a compact motion sensor for the measurement of physical activity in patients with chronic obstructive pulmonary disease. Respiration. 2012;83(4):300–307. doi: 10.1159/000330046. [DOI] [PubMed] [Google Scholar]
- 22.Hara T, Matsumura Y, Yamamoto M, et al. The relationship between body weight reduction and intensity of daily physical activities assessed with 3-dimension accelerometer. Jpn J Phys Fitness Sports Med. 2006;55:385–391. [Google Scholar]
- 23.Matsumura Y, Yamamoto M, Kitado T, Nakamura H, Kidera K, Fujimoto S. High-accuracy physical activity monitor utilizing three-axis accelerometer. Natl Tech Rep. 2008;56(2):60–66. [Google Scholar]
- 24.Watz H, Waschki B, Meyer T, Magnussen H. Physical activity in patients with COPD. Eur Respir J. 2009;33(2):262–272. doi: 10.1183/09031936.00024608. [DOI] [PubMed] [Google Scholar]
- 25.Demeyer H, Burtin C, Van Remoortel H, et al. Standardizing the analysis of physical activity in patients with COPD following a pulmonary rehabilitation program. Chest. 2014;146(2):318–327. doi: 10.1378/chest.13-1968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Trost SG, McIver KL, Pate RR. Conducting accelerometer-based activity assessments in field-based research. Med Sci Sports Exerc. 2005;37(11 suppl):S531–S543. doi: 10.1249/01.mss.0000185657.86065.98. [DOI] [PubMed] [Google Scholar]
- 27.Miller MR, Hankinson J, Brusasco V, et al. ATS/ERS Task Force Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi: 10.1183/09031936.05.00034805. [DOI] [PubMed] [Google Scholar]
- 28.Singh SJ, Morgan MD, Scott S, Walters D, Hardman AE. Development of a shuttle walking test of disability in patients with chronic airways obstruction. Thorax. 1992;47(12):1019–1024. doi: 10.1136/thx.47.12.1019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Vorrink SN, Kort HS, Troosters T, Lammers JW. Level of daily physical activity in individuals with COPD compared with healthy controls. Respir Res. 2011;12:33. doi: 10.1186/1465-9921-12-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Minakata Y, Morishita Y, Hiramatsu M, et al. Tulobuterol patch on the physical activity in eight male subjects with chronic obstructive pulmonary disease. Clin Res Pulmonol. 2014;2(1):1010. [Google Scholar]
- 31.Walker PP, Burnett A, Flavahan PW, Calverley PM. Lower limb activity and its determinants in COPD. Thorax. 2008;63(8):683–689. doi: 10.1136/thx.2007.087130. [DOI] [PubMed] [Google Scholar]
- 32.Jenkins CR, Jones PW, Calverley PM, et al. Efficacy of salmeterol/fluticasone propionate by GOLD stage of chronic obstructive pulmonary disease: analysis from the randomised, placebo-controlled TORCH study. Respir Res. 2009;10:59. doi: 10.1186/1465-9921-10-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Tashkin DP, Celli B, Senn S, et al. UPLIFT Study Investigators A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359(15):1543–1554. doi: 10.1056/NEJMoa0805800. [DOI] [PubMed] [Google Scholar]
- 34.Decramer M, Celli B, Kesten S, Lystig T, Mehra S, Tashkin DP. Effect of tiotropium on outcomes in patients with moderate chronic obstructive pulmonary disease (UPLIFT): a prespecified subgroup analysis of a randomised controlled trial. Lancet. 2009;374(9696):1171–1178. doi: 10.1016/S0140-6736(09)61298-8. [DOI] [PubMed] [Google Scholar]
- 35.Pitta F, Troosters T, Probst VS, Langer D, Decramer M, Gosselink R. Are patients with COPD more active after pulmonary rehabilitation? Chest. 2008;134(2):273–280. doi: 10.1378/chest.07-2655. [DOI] [PubMed] [Google Scholar]