

Abstract
Big Events are processes like macroeconomic transitions that have lowered social well-being in various settings in the past. Greece has been hit by the global crisis and experienced an HIV outbreak among people who inject drugs. Since the crisis began (2008), Greece has seen population displacement, inter-communal violence, cuts in governmental expenditures, and social movements. These may have affected normative regulation, networks, and behaviors. However, most pathways to risk remain unknown or unmeasured. We use what is known and unknown about the Greek HIV outbreak to suggest modifications in Big Events models and the need for additional research.
Keywords: Big Events, economic crisis, HIV, Greece, drugs, injectors, epidemics, epidemiology, drug use networks, risk environments
INTRODUCTION
HIV transmission events cannot be explained solely by individual risk-taking behaviors. Numerous studies in the 1990s and early 2000s have shown that sexual or injecting networks also play a crucial role (Friedman, Curtis, Neaigus, Jose, & Des Jarlais, 2002; Friedman et al., 1997, 2000; Potterat et al., 2002; Rothenberg et al., 1998). The rate of transmission and the social and behavioral distribution of who gets infected are determined by the known and knowable structures and dynamics of sexual and drug use networks. Friedman et al. introduced their “Big Events” theory during the last decade, as a thesis designed to give an insight into the complex pathway and interrelationship of factors at various levels that can result in HIV transmission or in other epidemics of infectious agents (Friedman, Rossi, & Braine, 2009; Friedman, Rossi, & Flom, 2006). They coined the term “Big Events” to describe transitions and serious economic crises but also wars and ecological disasters. Friedman et al. exemplified their model through the large HIV epidemic among people who inject drugs (PWID) in post-Soviet Russia (Friedman et al., 2009; Rhodes & Simic, 2005; Rhodes et al., 1999; Strathdee et al., 2006) and discussed how the political transition during the 1980s and 1990s was followed by economic instability, deepening poverty, changes in the effectiveness or content of normative regulation and by youth alienation creating an HIV risk environment characterized by growing alcohol consumption and injecting drug use, sexual hazardous behaviors, and female sex work, and, thus, paving the way to a large-scale epidemic (Friedman et al., 2009; Stuckler, Basu, Suhrcke, & Mc-Kee, 2009). On the other hand, however, due to the mixture of causal patterns1 plus random chance, Big Events do not always unleash HIV outbreaks. In the Philippines in the 1980s and in Argentina in the late 1990s to the early 2000s, the serious political and economical crisis and the following social unrest did not result in increased HIV spread (Friedman et al., 2009, 2006).
The Big Events model (Figure 1) provides reasonable pathways to explain HIV transmission in complex situations although many of its components deserve further research and more generalizable evidence. Wars, transitions, economic collapse, and ecological catastrophes differ in their nature and in many of their effects on peoples and communities but there are some social and economical parameters that are often influenced by them. Destabilizing events can cause the destruction of housing, force population displacement, disrupt or harm economic processes, produce economic difficulties in many population layers, incur changes in law and/or public policy, promote police violence, weaken, disrupt or destroy medical and other services, and trigger social mobilizations, insurrections, and inter-communal violence—which, in turn, impact on norms and values, the social organization of gender and sexuality, youth alienation, social and risk networks, and, of course, on behaviors. As a consequence, even in the short term, the riskiness of behaviors may increase or more people can engage in high-risk practices and in denser drug and sexual networks. Sexual or injection events that result in HIV transmission are embedded in sexual and injection partnership patterns and community networks. The Big Events theory also focuses on the risk event per se, and discusses proximate causal factors that affect the probabilistic functions of (i) one partner being infected and the other not and of (ii) their involvement together in a risky sexual act or injection that leads to a new HIV infection. Finally, the theory also takes into account the fact that autonomous actions and local struggles of activists and at-risk people to protect themselves2 and others against damages and to keep their welfare might help vulnerable individuals or groups resist sexual or drug-use-related risk (Friedman et al., 2009, 2006).
FIGURE 1.
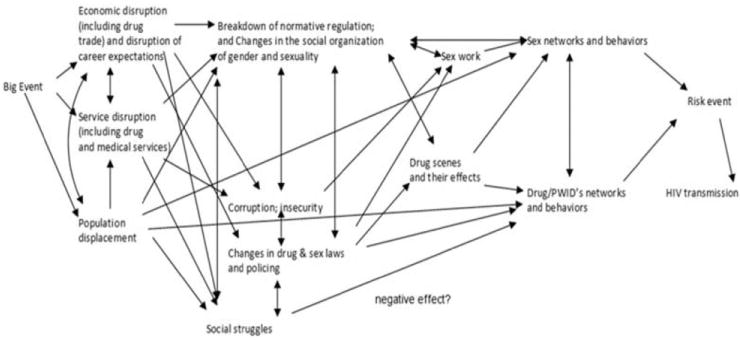
* Historically situated pathways through which Big Events may sometimes unleash HIV epidemics and other harms**.*This model was published in Friedman, S. R., Rossi, D., & Braine, N. (2009). Theorizing “Big Events” as a potential risk environment for drug use, drug-related harm and HIV epidemic outbreaks. The International Journal on Drug Policy, 20(3), 283–291. **In some cases, such as with normative regulation and the organization of gender and sexuality, and as with corruption and insecurity (fear for one’s personal safety), variables that fit together in homologous places in the system of arrows (pathways) have been grouped together so the model remains readable.
Note. PWID: People Who Inject Drugs.
Greece has been experiencing a tremendous economic downturn (International Monetary Fund, 2013), and this has been accompanied by periods of considerable social movement activity and conflict. At around the same time, a low-level HIV epidemic among drug injectors before 2011 was followed by a tremendous outbreak of almost 1,000 new HIV infections in less than 3 years (Hellenic Centre for Disease Control and Prevention, 2013; Paraskevis et al., 2011, 2013; Pharris et al., 2011). Little, however, is known about how the macro-level economic changes in Greece precipitated HIV spread in PWID. We will try to understand how the Big Events in Greece—if they have done so—influenced sexual and drug injection behaviors and also how they have affected the size, turnover, and topologies of risky networks since these affect the probability that a susceptible person will engage in sexual or injection behaviors with an infectious partner. We will attempt to identify what kind of information is needed to develop a better sense of whether the Big Events model on the Greek paradigm is meaningful and usable. In addition, further consequences of the current crisis may be yet to come. We will thus consider hypotheses about the recent outbreak, examine evidence about potential HIV spread to and in other population groups, discuss ways in which the crises might create serious socio-epidemiological vulnerability in the long term, explore opportunities for further research and, finally, discuss how these thoughts might guide prevention strategies.
METHODS
This paper reviews the existing literature and used published information to formulate hypotheses and make suggestions for future needed research. In addition, preliminary data on 128 participants of the Transmission Reduction Intervention Project (TRIP) in Athens, Greece are being reported. TRIP is a 5 year multidisciplinary intervention funded by the United States (US) National Institutes of Health (NIH) in 2012 and is being implemented in three sites: Athens (Greece), Odessa (Ukraine), and Chicago (US) (Friedman, Downing, et al., 2013). The research protocol has been reviewed by the Institutional Review Board (IRB) of the National Development and Research Institutes (NDRI) in New York City and by local IRBs. All participants are asked to sign an informed consent form.
BIG EVENTS IN GREECE
Background
Greece is a southeastern European country of around 11 million people (Hellenic Statistical Authority, 2014). It is a member of the European Union (EU) and has belonged to the Euro zone since the early 2000s. Greece experienced substantial economic growth in the 1990s and the early 2000s (Hellenic Statistical Authority, 2014), which improved people’s prosperity and reduced, to some degree, economic inequalities. Despite being in crisis, even in 2013, Greece ranked close to the average on many topics measured by the Organization for Economic Co-operation and Development (OECD) Better Life Index (The Organization for Economic Co-operation and Development, 2013). As an EU member, it also became an attractive destination for migrants from developing areas who were seeking a safer and prosperous working environment and an entry point to the rest of the EU.
Despite these time-limited economic achievements, Greece has a history of corruption and indebtedness that dates back to the birth of the modern Greek state (Georgakas, 2013; Mungiu-Pippidi, 2013). Greece was recognized as a sovereign entity in 1829/1830 following the revolution but the Greek people became highly dependent on local elites, middlemen, speculators, and external creditors as a price for gaining political freedom. Build on the ruins of Ottoman Empire, the Greek state was later involved in many local and imperialist wars (Balkan wars, First World War, and Second World War with its catastrophic 4 year occupation by Nazis’ troops and the post-War II civil war), which, along with civil conflicts and periods of authoritarianism, corrupted governance and political malpractice, had adverse consequences on various economic and social parameters (Georgakas, 2013). Excluding the current financial downturn, Greece has already experienced five default/rescheduling episodes, spaced some years or decades apart (1826, 1843, 1860, 1893, and 1932) and, rather amazingly, stood for half of its sovereign existence in default or rescheduling (Reinhart & Rogoff, 2008).
The period following the 1967–1974 military regime was politically stable and characterized by a bourgeois parliamentary democracy, the participation in EU, the gradual growth of Gross Domestic Product (GDP) (Hellenic Statistical Authority, 2014), and the moderate improvement of living conditions. Nonetheless, the economic success was not the result of autonomous and sustainable economic development but rather a domestic-demand-driven explosion based on excessive optimism, capital inflows-driven cheap credit, particularly after Euro circulation, and fiscal profligacy (Kang & Shambaugh, 2013). The prominent features of the 1990s and 2000s were the enormous public external borrowing, the huge government and private debt, and increasing fiscal deficits from year to year.
The Recent Crisis
After many years of development, in 2008, the real GDP growth rate in Greece decreased as a consequence of (and part of) the global financial crisis (Eurostat, 2014d; Hellenic Statistical Authority, 2014; International Monetary Fund, 2013). The financial distress soon turned into economic and political turbulence. In 2010, the situation became worse when the Greek government imposed harsh austerity policies and made the first cuts to public expenditures (for instance, minimum wages have been reduced by more than 20%) (Karanikolos et al., 2013). Even though the government deficit, as percent of GDP, has been reduced from −15.7% in 2009 to −8.9% in 2012 (Eurostat, 2014a), the Greek economy shrank for 6 years in a row with a total GDP squeeze of more than 20% (Eurostat, 2014d; International Monetary Fund, 2013). In spite of a big restructuring of the Greek debt in 2012 (The Economist, 2012), government finances still deteriorate: the public debt was 304 billion Euros in 2012 and reached 319 billion Euros or 175% as share of GDP in 2013 (Eurostat, 2014b). The unemployment rate rocketed from 7.7% in 2008 to 27.3% in 2013 (Eurostat, 2014e; International Monetary Fund, 2013; World Health Organization – Regional Office for Europe, 2013), being the highest in the EU. Youth unemployment, now over 50% (World Health Organization – Regional Office for Europe, 2013), is of particular concern and forces talented and highly trained young Greeks to seek a professional career abroad. Early in the crisis era, by 2010, almost one quarter of the Greek population was at risk for poverty with income below 60% of national median and was experiencing serious material deprivation (Kondilis et al., 2013).
Attacks against labor and social rights by three single party or coalition governments in 4 years resulted in massive demonstrations, numerous union, and general strikes, and many spontaneous gatherings mainly in Athens but also in other populous cities that culminated in a huge summer (2011) protest at the central Syntagma square near the Greek parliament (Arampatzi & Nicholls, 2012; Georgakas, 2013). The workers’ response, despite being vigorous in absolute terms, having its roots in the longstanding traditions of grassroots and leftist movements during the previous decades, was disproportionately low compared to the magnitude and the negative consequences of the imposed policies. Working people’s resistance was attacked rather brutally by the police, and was undermined by the efforts of union officialdom (Friedman, 1982) and seems now to be subsiding. During the crisis years, Greece also observed the rise of the major nationalistic group (Popular Association – Golden Dawn) who won 18 seats (out of 300) in the Greek parliament in the legislative election (share of vote 7%) of June, 2012 (Seymour, 2013) and finished third in the recent election of the delegation of Greece to the European parliament (May 2014) receiving 9% of the popular vote. On the other hand, massive antifascist protests have also been observed along with the growing popularity of one of the leftist parties (SYRIZA) (Georgakas, 2013), who won the 2014 European parliament election and its platform supports human rights and prioritizes the needs of vulnerable and marginalized sections of the Greek society.
Non-HIV Health Consequences
As part of Greece’s austerity cuts, public spending on health should not exceed 6% of GDP (Karanikolos et al., 2013). These cuts included reductions in public spending on drugs, decreases in workforce, cuts in salaries of health care staff, changes to purchasing of health services, closure of facilities, and restructuring of the public hospitals sector (Karanikolos et al., 2013; Kentikelenis & Papanicolas, 2012; Kondilis et al., 2012). Compared to previous years, public health spending declined by 12.39% in 2010 and by 12.38% in 2011 (Kondilis et al., 2013; World Health Organization – Regional Office for Europe, 2013). In a country with a household net-adjusted disposable income per capita of around 19,000 US dollars (USD) that is even lower in poorer groups and almost 5,000 USD less than the OECD average (The Organization for Economic Co-operation and Development, 2013), costs have been gradually shifted to patients by instituting user charges for public health services (for instance 5 Euros fee for outpatient visits to public hospitals). General public hospitals that were performing better than not-for-profit competitors (Kondilis et al., 2011) now need to face elevated demand and service utilization with dwindling resources, which created increased workloads and long waiting lists, especially in emergency rooms (Kentikelenis & Papanicolas, 2012; Kondilis et al., 2013). The linkage between health coverage and employment status in Greece has been a critical issue: Given the tremendous unemployment, especially among youth, the inability of the self-employed population to cover social insurance costs, and a limited period of entitlement to unemployment benefits, a large pool of uninsured people has gradually been created whose access to and receipt of essential treatment and care is endangered.
Various scientists and organizations described the early effects of the economic crisis in Greece and other European countries (Arie, 2013; Bonovas & Nikolopoulos, 2012; Brand, Rosenkötter, Clemens, & Michelsen, 2013; Chang, Stuckler, Yip, & Gunnell, 2013; Karanikolos et al., 2013; Kentikelenis et al., 2011; Kondilis et al., 2013; Stuckler, Basu, Suhrcke, Coutts, & McKee, 2009; Stuckler & Basu, 2009). Early reports from Greece provide estimates of annual or bi-annual increases in suicides between 19% (2007–2009) (Economou, Madianos, Peppou, Theleritis, & Stefanis, 2012; Kentikelenis et al., 2011) and 40% (first half 2011/first half 2010) (Kentikelenis et al., 2011). Homicide rates also increased by 25% between 2007 and 2009 (Kondilis et al., 2013). Research based on telephone surveys in 2008, 2009, and 2011 reported an increase in the prevalence of suicide attempts from 0.6% in 2008 to 1.5% in 2011 (Economou, Madianos, Peppou, Theleritis, et al., 2013; Kondilis et al., 2013). The 1 month prevalence of major depression also escalated from 3.3% in 2008 to 6.8% in 2009 (Madianos, Economou, Alexiou, & Stefanis, 2011) and to 8.2% in 2011 (Economou, Madianos, Peppou, Patelakis, & Stefanis, 2013).
Following a steady decreasing trend from 2001 to 2008 (2.7 per 1,000 live births), infant mortality in Greece increased in 2009 (3.1 per 1,000 live births) and in 2010 (3.8 per 1,000 live births), and remained higher in 2011 (3.4 per 1,000 live births) and in 2012 (2.9 per 1,000 live births) compared to 2008 (Eurostat, 2014c; World Health Organization – Regional Office for Europe, 2013). A recent letter reported also a 32% rise in the number of stillbirths (Vlachadis & Kornarou, 2013; World Health Organization – Regional Office for Europe, 2013).
During the last years in Greece, surveillance data indicated substantial increases in some infectious diseases (Bonovas & Nikolopoulos, 2012). In 2010, the first clinical cases of West-Nile virus (WNV) infection were documented in humans in Central Macedonia and the virus has since spread southward affecting the metropolitan area of Athens, which may herald a long-term establishment in Greece (Bonovas & Nikolopoulos, 2012; Danis, Papa, Papanikolaou, et al., 2011; Danis, Papa, Theocharopoulos, et al., 2011; Ladbury et al., 2013). Following decades of zero reports, between 2009 and 2012, 62 locally acquired malaria cases were identified, particularly in a well-defined agricultural area (Bonovas & Nikolopoulos, 2012; Danis et al., 2013; Danis, Baka, Lenglet, et al., 2011). Although there is no clear evidence to connect the appearance of WNV infection and the re-emergence of malaria with the economic instability in Greece, the increased epidemiological numbers of these two mosquito-borne diseases during the crisis epoch are very important and, given the unique regional conditions in some areas (Kousoulis et al., 2013), constraining resources and vector-control measures could facilitate their transmission with unpredictable consequences (Bonovas & Nikolopoulos, 2012).
HIV Epidemic
The HIV epidemic in Greece (Figure 2) was traditionally concentrated in Men who have Sex with Men (MSM) (Nikolopoulos, Paraskevis, & Hatzakis, 2008). Before 2011, sporadic HIV cases reported among drug injectors ranged between 10 and 20 per year (Hellenic Centre for Disease Control and Prevention, 2013; Nikolopoulos et al., 2008; Paraskevis et al., 2013). Early in 2011, the Hellenic Centre for Disease Control and Prevention (HCDCP) received HIV reports in excess of expectancy and, finally, by the end of that year, 266 drug injectors had been diagnosed with HIV—a 16-fold increase compared to 2010 (Hellenic Centre for Disease Control and Prevention, 2013; Paraskevis et al., 2013). At the beginning of the outbreak, the HCDCP tested 62 samples of drug injectors diagnosed in 2011 using avidity assays, which documented that the majority of infectees (57%) had acquired the virus quite recently (European Centre for Disease Prevention and Control, 2012). Most of the newly diagnosed PWID (~70%) in 2011 were residents of Athens (Paraskevis et al., 2013), suggesting that the outbreak was localized there (at least for the moment). In treatment facilities, the picture also indicated a large outbreak. The percentage of HIV positives among drug users contacting treatment services in Athens increased to 8% in 2011 from less than 2% in 2010 (European Centre for Disease Prevention and Control, 2012; European Monitoring Centre for Drugs and Drug Addiction, 2012). In 2012, HIV continued to spread in drug injectors—547 new infections were diagnosed among them (Hellenic Centre for Disease Control and Prevention, 2013; Paraskevis et al., 2013). During the same year, the total number of HIV reports reached a historical peak (1,188) and injecting drug use became the most frequently reported probable route of transmission (46% versus 28% of infections in MSM) (Hellenic Centre for Disease Control and Prevention, 2013; Paraskevis et al., 2013).
FIGURE 2.
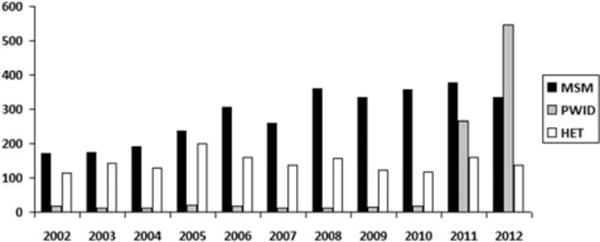
HIV cases in Greece by year of report and route of transmission (Men who have Sex with Men—MSM, People Who Inject Drugs—PWID, Heterosexuals—HET).
In August 2012, a respondent-driven sampling (RDS) program named “Aristotle” began in Athens consisting of five successive rounds of HIV screening. During the first round (August–October 2012), 1,404 drug injectors were tested and around 20% were HIV positive (Sypsa et al., 2014). In collaboration with the new, multidisciplinary TRIP project (Friedman, Downing, et al., 2013), most first round positive samples (271) were further tested by Limiting-Antigen Avidity assay (LAg) (Duong et al., 2012), which showed that approximately one fourth of positives (71) had acquired HIV recently, perhaps within 4–6 months from their diagnosis. Molecular analyses on PWID’s samples in 2011 and in 2012 revealed transmission networking in more than 90% of them in high contrast to extremely low-level clustering (5%) before 2010 (Paraskevis et al., 2013). In addition, new HIV strains have been circulating in the infected drug-using population during the outbreak years (Paraskevis et al., 2011, 2013). Taken together these data further support the newness of the epidemic and the large HIV spread in drug injectors in 2012.
Surveillance data for 2013 (Table 1) suggest that HIV transmission in drug injectors may have started to decrease (Hellenic Centre for Disease Control and Prevention, 2013). A total number of 262 HIV infections was reported in 2013 in PWID, which is lower than the 547 reported in 2012. Although surveillance numbers are influenced by testing and reporting patterns, it is likely that, despite cuts in health spending, large-scale responses of health agencies, universities, and non-governmental organizations (NGOs) may have reduced HIV transmission. Prevention coverage before the start of the outbreak fell far short of internationally recommended standards (European Monitoring Centre for Drugs and Drug Addiction, 2012; Nikolopoulos et al., 2008; Paraskevis et al., 2013). The waiting list at Opioid Substitution Treatment (OST) facilities in Athens was 8 years in September 2011, and annual syringe/needle distribution per drug injector by Needle/Syringe Programs (NSP) was less than 20 before 2011 (European Monitoring Centre for Drugs and Drug Addiction, 2012). Rapid response to the HIV outbreak cut the drug treatment waiting list in Athens to 4 years in August of 2012 and estimated OST coverage reached 35% from 20% in 2010 (European Monitoring Centre for Drugs and Drug Addiction, 2012; Malliori, Golna, Souliotis, & Hatzakis, 2013). Syringe distribution also escalated and exceeded 40 (per drug injector) in 2011 (European Monitoring Centre for Drugs and Drug Addiction, 2012; Malliori et al., 2013). According to more recent reports, approximately 407,000 syringes were distributed in 2012, almost seven times the number in 2010 (61,500), and the annual NSP coverage probably reached 133 needles/syringes per injector in the capital city of Athens in 2012 (European Monitoring Centre for Drugs and Drug Addiction, 2014).
TABLE 1.
Cases of HIV infection in Greece by route of transmission and year of report (2009–2013) (Hellenic Centre for Disease Control and Prevention, 2013)
| Year of report
|
|||||
|---|---|---|---|---|---|
| Route of HIV transmission | 2009 | 2010 | 2011 | 2012 | 2013 |
| Men who have Sex with Men (MSM) | 334 (55.02%) | 356 (58.36%) | 378 (39.05%) | 333 (28.03%) | 307 (33.37%) |
| People Who Inject Drugs (PWID) | 15 (2.47%) | 16 (2.62%) | 266 (27.48%) | 547 (46.04%) | 262 (28.48%) |
| Heterosexuals | 122 (20.10%) | 116 (19.02%) | 159 (16.43%) | 137 (11.53%) | 122 (13.26%) |
| Undetermined route/other | 136 (22.41%) | 122 (20.00%) | 165 (17.05%) | 171 (14.39%) | 229 (24.89%) |
| Total | 607 | 610 | 968 | 1188 | 920 |
BIG EVENTS AND THE HIV EPIDEMIC IN GREECE
Hypothesized Partial Model of Pathways From the Economic Crisis to HIV Transmission in PWID
Has the economic crisis as a Big Event contributed to the HIV outbreak in PWID? It may well be true, but it is difficult to describe the pathways through which that occurred given the lack of studies to collect necessary information. We can nevertheless formulate reasonable hypotheses based on the evidence we now have (Figure 3). We have already conducted ecologic analyses that connect the economic crisis with the recent HIV outbreak among drug injectors in Greece (Paraskevis et al., 2013). By using regression models, we found that the diagnosis rate of HIV in drug injectors was increasing while GDP was declining (Paraskevis et al., 2013). In addition, we observed significant associations between GDP growth rate and a couple of other variables including HIV prevalence in PWID in Athens, hepatitis C virus (HCV) prevalence in new injectors and the homelessness and unemployment rates in PWID in Athens. Furthermore, in the first round of the “Aristotle” program in Athens, lack of stable accommodation was the most important predictor of HIV seropositivity (Sypsa et al., 2014). It seems thus reasonable to assume that the general economic instability quickly affected vulnerable parts of the Greek population like drug injectors and their families in Athens (which was perhaps the place most devastated by Greece’s economic crisis). Many injectors who lost jobs or whose families became unable to support them had decreased income, they likely became unable to pay rents or mortgages and thus became homeless and began to gather and live in the traditional central drug user settings of Athens where, as shown before, the epidemic is confined. Unstable housing or the lack of accommodation has previously been connected with behaviors and network characteristics that result in HIV transmission (Des Jarlais, Braine, & Friedmann, 2007; Friedman et al., 2002; Linton, Celentano, Kirk, & Mehta, 2013; Reyes et al., 2005).
FIGURE 3.
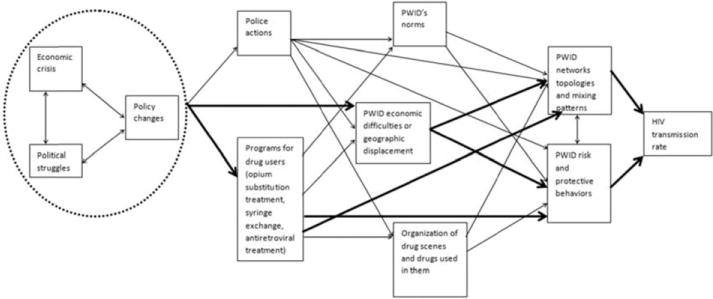
Hypothesized partial model of pathways from the economic crisis in Greece to HIV transmission among People Who Inject Drugs (PWID). Arrows that are in bold represent associations for which there are supporting data.
It is likely that previously small networks of injectors, both of Greeks and of migrants, started to mix in these localities. The high HCV prevalence and the reportedly frequent sharing of injecting equipment among drug injectors who were contacting treatment services in the pre-epidemic period indicate the long-term presence of risky practices in the drug-using community (Nikolopoulos et al., 2008). We can argue that the limited HIV spread before 2011 could thus be either due to pure chance or more likely the result of selective sharing in small size networks. The new conditions in the centre of Athens brought together previously separate clusters of people, thus increasing the size of risk networks. As a matter of fact, in the “Aristotle” program, unstably housed people did report larger network sizes (Sypsa et al., 2014). It is also very important that the new environment allowed groups with different HIV prevalence to interact. Data from the first round of the “Aristotle” project showed that HIV prevalence in Athenian drug injectors from Iran/Afghanistan was around 31%, but was 19% among Greek-national injectors (Sypsa et al., 2014). Furthermore, molecular analyses (Paraskevis et al., 2013) identified four major transmission clusters in infected PWID who were diagnosed in 2011/2012: Circulating Recombinant Form (CRF) 14_BG, CRF35_AD, Subtype B, and Subtype A. In one of these networks (CRF35_AD), the most similar sequences could be found in Iran/Afghanistan. Generally, the geographic origin of most HIV isolates was consistent with the migratory waves in Greece. Police operations in central Athens against drug sellers and users that can result in relocation of PWID may have also facilitated the mixing of different networks. To the best of our knowledge there are no studies that have measured injecting norms in Greece, which are very likely to be affected by economic turbulence. However, sharing injecting equipment was common before the epidemic boom (Nikolopoulos et al., 2008) and we can hypothesize that new and rapidly established normative rules in the street probably allowed sharing between otherwise distant ethnic groups with different levels of HIV. The NSP coverage and control measures were at that time completely inadequate (European Monitoring Centre for Drugs and Drug Addiction, 2012) and could not stop transmission chains or contain the outbreak.
Will There be Further Spread of HIV in Greece Among Groups Other Than PWID? Medium-Term HIV Risk Associated With Big Events
HIV outbreaks among non-PWID could happen due to spread from the PWID epidemic and/or from Greek Big Events shaping transmission within and among other subpopulations. As of this writing, there are more than 1,000 PWID who have recently become HIV infected—some of whom still have high viral loads (and infectivity) as a result. There is thus a high short-term probability for HIV transmission from PWID to non-drug using heterosexuals (and lesbians) and also to MSM. The extent to which this occurs will primarily be determined by efforts to reduce HIV infection among PWID and to get infected PWID into antiretroviral treatment; the characteristics and magnitude of sexual networks and group sex events that connect PWID to heterosexuals, lesbians, and MSM; and the social network locations of those PWID who have high viral loads. In addition, rates of unprotected sex in these sexual networks will also help determine the magnitude of HIV transmission within them. Beyond that, sexual networks, group sex participation, and sexual behaviors within each Key Population will shape the extent to which HIV continues to transmit within each of them. It is likely that people who use drugs, but do not inject them, may be an important bridge population with high rates of sexual risk behaviors, increased contact with PWID as a result of drug use, and perhaps high rates of involvement in sex work (Figure 4).
FIGURE 4.
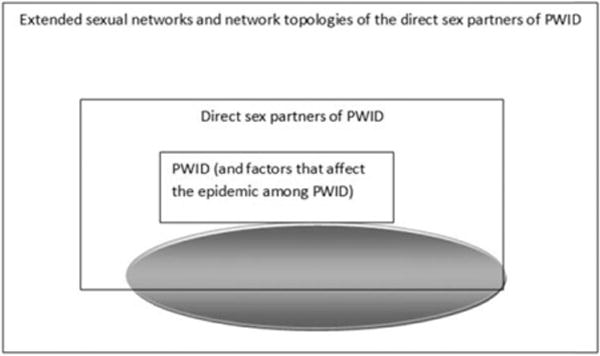
Once an HIV epidemic breaks out among People Who Inject Drugs (PWID), there are factors that may affect medium-term spread of the epidemic to people who do not inject drugs. These factors are not fixed, but may change either due to the Big Events or in response to the HIV epidemic itself. The oval represents people who use but do not inject drugs. Some evidence suggests that they are more likely than other non-PWID members of the population to have sex with PWID, and also to engage in high-risk behaviors.
We have a limited amount of data about sexual networks, group sex participation, and behaviors of PWID and about epidemic trends among MSM and heterosexuals. In “Aristotle,” information was collected on the sexual behaviors and partners of respondents including those who were infected with HIV at the time of their interview—and thus were potential transmitters of infection to others. From the analysis of the first round, when asked about the person with whom they last had sex, 48% of men and 22% of women said their most recent partner had not injected any drugs (Sypsa et al., 2014). This is very important—it documents sexual links between PWID and non-injecting population groups. Condoms were not often used by infected drug users. In the first wave of the “Aristotle” project, around 40% of positive males and one third of positive females reported that they usually do not or never use condoms during vaginal or anal intercourse. Female drug injectors also engage in sex work, with 37% of “Aristotle” round 1 HIV-positive women reporting sex in exchange for money or drugs.
The multidisciplinary TRIP project collects data about group sex events, which can be considered as HIV risk and potential bridge environments that in non-Greek studies have been found to involve wide-spread participation of people who take drugs by non-injection routes, of MSM, lesbians, and sex workers (Friedman et al., 2008; Friedman, Mateu-Gelabert, & Sandoval, 2011). By mid-November 2013, 128 individuals, mostly drug injectors, had participated in TRIP. The sample included 20 recently infected PWID and their first/second degree contacts (84), 4 long-term HIV infectees and their 2 first degree network members, and 18 HIV negatives (the chronically infected seeds and the negatives are control groups of the intervention). Only 6 male participants (4.7%) reported that during the last 6 months they had been present when group sex was taking place. Among these six subjects, four were HIV positive, including three recently infected cases. Half of them (the two negatives and the chronically infected positive who were all network contacts of recent infectees) said that they also had sex once in the group sex event place without using condoms. Therefore, at the moment, it seems that group sex is either not very popular in the drug-injecting population, perhaps because of the type of drugs used (mostly opiates), or is being under-reported by respondents. TRIP, of course, will continue to enroll subjects including their network members who may not inject or use drugs. Along with follow-up interviews, we will soon be able to analyze a substantial volume of longitudinal data on group sex events that will help us draw firmer conclusions.
Routine surveillance data offer little support of large increases having yet occurred in transmission rates in other population groups such as MSM and heterosexuals, although these patterns are somewhat uneven. As shown in Table 1, fewer HIV infections were reported in 2013 in PWID than in 2012. Sexually acquired infections seem to predominate but the number of reports in 2013, both in MSM and in heterosexuals, still remain lower than the corresponding figures in 2012. If, however, we compare the 2012/2013 years with the pre-outbreak period (2009/2010), we observe that the heterosexually acquired HIV transmissions in the last 2 years are slightly more than those occurred in 2009/2010.
None of these variables should be considered to be stable. In a Big Events situation like that of Greece, in which both economic and political instability are high and in which many people face lives of increasing poverty, the extent and social distribution of sex in exchange for money, goods, or a place to spend the night is likely to change. So are popular norms toward what forms of sexual relationship are acceptable.
Little is known about what the political, economic, and social future of Greece is likely to be. Little is known about if and how changes in these will affect sexual mixing patterns (networks, group sex events, etc.), norms or behaviors in the country, nor about how such changes will affect the amount and social locations of HIV transmission and care. Research is needed on these issues—both for the sake of the Greek people and for that of other countries that face similar situations now and in the future.
Will Big Events Increase the Size of the at-Risk Populations? What is Happening Among Youth and Newly Marginalized Populations? Long-Term HIV Risk Associated With Big Events
The economic and political Big Events have now lasted for several years and may well continue for many years more. They are likely to lead to many deep transformations in the lives of the people and to their forms of social organization and culture (Figure 1) (Friedman et al., 2009). As we discussed in two earlier papers (Friedman et al., 2009; Friedman, Sandoval, et al., 2013), the consequences of these transformations for the future of the HIV epidemic after Big Events may be heavily mediated by the extent of youth experiencing despair over their future prospects and the related degree to which intergenerational normative regulation breaks down such that a large number of youth gravitate toward drug use, sexual hedonism, and perhaps toward trading sex and/or drugs for money, goods, or services. This mediation can be better understood in terms of Cultural Historical Activity Theory (CHAT) (Friedman, Sandoval, et al., 2013), aspects of which appear in the “CHAT processes” box in the third column of Figure 5. This points to complex and nondeterministic interactions among the activities in which they engage (which can be thought of in terms of how they use their time and of their organizational commitments as well as in terms of their behaviors); the intersubjective communication they engage in with their friends, neighbors, employers (if any) and other people, including the ways in which this leads them to define their own and others’ life situations; and the creative and routinized ways in which they respond to changes in their environment and activities.
FIGURE 5.
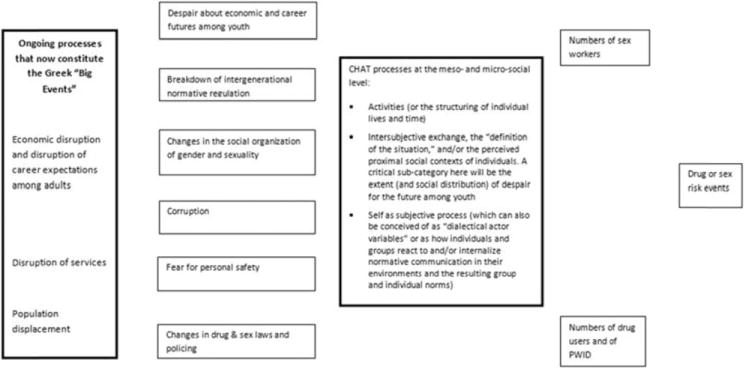
Interacting pathways that may affect longer-term developments of drug use and of the HIV and related epidemics in Greece. PWID: People Who Inject Drugs. CHAT: Cultural Historical Activity Theory (Friedman, Sandoval, et al., 2013).
In the current Greek situation, little is known about these pathways variables. We have been collecting a small amount of pilot data on selected variables in the context of the “Aristotle” and TRIP projects. TRIP will soon start to also gather follow-up data and it will then be able to study whether some of these parameters changed over time. Nonetheless, these pilot data will not suffice to make strong inferences and it is thus important to expand the measurement and include many other variables that will help us better understand the causal pathways to HIV transmission in the long term.
In the Greek situation, as discussed above, there is a large HIV outbreak among PWID. Little is known about the extent to which Greek PWID are parts of sexual networks with other (non-injecting) drug users (NIDU), but based on data from the United States (Des Jarlais, Arasteh, & Friedman, 2011; Rothenberg et al., 2000) and other countries (Li et al., 2011), it seems likely that such network connections are fairly extensive. In New York City, for instance, the stabilization of HIV incidence in injecting drug users was followed by a sexual transmission phase and equal prevalence rates between injecting and non-injecting groups (Des Jarlais et al., 2011). To the extent network ties do exist between injectors and non-injecting people who use drugs in Greece, changes in the size of the NIDU population may be one important determinant of the future of the HIV epidemic in Greece.
DISCUSSION
Based on what we have learned from the Greek HIV epidemic among people who inject drugs, we can suggest some improvements in the theory of Big Events and their epidemiological implications. We can also present ideas about what we do not know, and about research that would be useful for us to better understand how Big Events can and do affect drug use patterns, HIV epidemics, and public health more generally.
We can conceptualize how Big Events affect HIV epidemics in terms of the potential for short-term, medium-term, and long-term effects. In the short term, these events may affect those Key Populations such as PWID, sex workers, other high-risk heterosexuals or MSM among whom HIV is already present. If this leads to higher rates of risk behaviors, denser mixing patterns (including risk networks and group injection or sex events), and/or decreases in intervention programs that help reduce risk behaviors or help the infected to keep their viral loads low (and help maintain their health), an epidemic outbreak may occur in one or more Key Populations. In Athens, such an outbreak occurred among PWID.
Once such an outbreak occurs, it may remain concentrated in the given Key Population. On the other hand, depending on mixing patterns and risk behaviors in risk networks between members of the group in which the outbreak occurs and other population groups, and on the extent and nature of interventions to prevent further HIV transmission, HIV can spread to other Key Populations or perhaps become generalized. It is not yet clear what will happen in Athens. Figure 5 provides an overview of conditions that might affect this. It is important to note that the network and behavioral patterns in this figure are not constant, and may change as a result of the Big Events and their sequelae or in response to the HIV outbreak and programs to combat it.
Big Events may be able to spark HIV epidemics through a longer term path as well. This can occur if the Big Events lead to changes in the social, economic, and cultural situation in a city or other region. If such changes occur, and lead to the formation or enlargement of subpopulations of PWID, sex workers, or people who engage in high-risk sex with multiple partners, then conditions can be ripe for an HIV epidemic. This is maybe what happened in the former Soviet Union and in South Africa (Friedman & Reid, 2002). Figure 5 provides an overview of how this can happen. These same dynamics can of course occur in the same places where short-term and perhaps medium-term outbreaks have occurred, in which case some or all of the Key Populations that may have epidemics within them may grow considerably in size and/or epidemics that have been contained within one or more Key Populations may become generalized epidemics.
As is clear from our review of the HIV outbreak in Athens, very little is known about most of the pathways variables that are described in Figure 1 (Friedman et al., 2009) or in later figures. Little was known before the epidemic—and much remains unknown—about the normative pressures that influence the behaviors of Key Populations like people who inject drugs. Little is known about sexual network connections between Key Populations. Friedman and his colleagues have conducted one network study that presents an overview of such networks in one section of Brooklyn, New York (Friedman et al., 2007, 2008)—but far more research of this kind is needed in general, and particularly where Big Events occur. The authors of this paper are currently conducting intervention research (TRIP) in Athens that may provide more information about the sexual networks of PWID who have recently become infected with HIV (Friedman, Vasylyeva, & Smyrnov, 2012; Friedman, Downing, et al., 2013). For longer-term pathways, little or no research exists for Greece or other countries on most of the variables mentioned in the figures in this paper. This is because measures have not been developed to accurately assess many of these variables. Ongoing research (Friedman, Sandoval, et al., 2013) is attempting to develop and validate measures on many of the CHAT variables in Figure 5. The questionnaires of the “Aristotle” and TRIP projects also contain some of these scales, on a pilot basis, but certainly more research of this kind is needed.
In order to understand Big Events and their sequelae better, it would be useful to have annual or biannual sociobehavioral surveillance surveys in a number of countries that would measure these pathways variables in Key Populations and among youth and others who might become recruited to high-risk behaviors if a Big Event occurs. These would provide baseline data that might be useful in planning how to mitigate Big Events’ effects in those countries, and that would also be useful in studies of what changed, and how, after the Big Events.
Interventions to mitigate the effects of Big Events are likely to interact with the interests, understandings, and values of powerful economic and political stakeholders as well as with those of urban planners, police agencies, drug user treatment agencies, and other institutions. Research is needed on how to mitigate Big Events’ effects successfully. Intervention failures, as opportunities for learning, and posited processes such as “failure blindness” have not been adequately considered in substance use(r) intervention generally or within Big Events theory more specifically (Einstein, 2012).
Finally, we need research on how to respond to Big Events both in short run terms and in the middle and long term to minimize their effects on HIV transmission and other health issues. In immediate terms, it is important to maintain or increase programs like syringe distribution/exchange and drug user treatment—even though the neoliberal response in times of economic crisis might be to reduce them. In Greece, in spite of budget cutbacks, NSP and OST programs were remarkably reinforced, but it is crucial to improve them further to meet current and future needs. It is also important to establish effective surveillance systems to monitor for HIV and other infectious outbreaks so as to enable early and ongoing interventions if they occur. In Greece, the presence of phylogenetic surveillance procedures allowed much faster detection and description of the outbreak among PWID than might otherwise have occurred (Paraskevis et al., 2011). Interventions to prevent transmission sexually from one Key Population to other people should be developed—and implemented. In addition, as we learn more about what pathways lead to the growth of high-risk populations after Big Events, interventions should be developed to minimize adverse consequences. Some of these might be politically controversial or difficult, such as efforts to reduce police violence or to reduce stigmatization or social subordination of women, foreign immigrants, drug users or gays. Nonetheless, as the examples of South Africa and Russia make clear (Friedman & Reid, 2002), the consequences of not acting in these ways can be public health catastrophes.
Acknowledgments
The authors acknowledge support from National Institute on Drug Abuse (NIDA) grants P30 DA11041 (Center for Drug Use and HIV Research); DP1 DA034989 (Preventing HIV Transmission by Recently-Infected Drug Users); grant R01DA031597 (Developing measures to study how structural interventions may affect HIV risk); and T32 DA007233; National Institutes of Health D43TW000233 funded by the Fogarty International Center. The International AIDS Society and the National Institute on Drug Abuse (NIDA) have supported the post-doc fellowship of the first author. Support for the Aristotle Project and several authors was provided by EU NSRF 2007–2013 that is co-funded by the European Social Fund and Greek national resources.
GLOSSARY
- Big Events
Transitions, Serious Economic Crises, Wars, and Ecological Disasters. The term refers to major events, natural, as well as man-made, which effect adaptation, functioning, and quality-of-life of individuals as well as social relationships and systems. Existential threat, instability, and chaos are major dimensions and loss of control over one’s life is experienced
Biographies

Georgios K. Nikolopoulos, Ph.D., has received a postdoctoral research fellowship from the International AIDS Society and the National Institute on Drug Abuse and is now leading the Transmission Reduction Intervention Project (Principal Investigator: Dr. Samuel Friedman) in Athens, Greece. He earned a PhD in the epidemiology of infectious diseases at the School of Medicine of the Athens University in Greece and has served at the Greek public health agency for almost one decade, focusing on HIV surveillance. Dr. Nikolopoulos also has expertise in the conduct of systematic reviews and meta-analyses with useful contributions to the evolving domain of genetic epidemiology.

Vana Sypsa, Ph.D., is Assistant Professor of Epidemiology and Preventive Medicine in the Department of Hygiene, Epidemiology and Medical Statistics of Athens University Medical School in Greece. She obtained her first Degree in Mathematics, an M.Sc. in Biometry, and a Doctoral Degree in Epidemiology. She has been involved in several projects on infectious diseases and was co-investigator in a large RDS program in injecting drug users during an HIV outbreak in Athens. She is the Secretary of the Executive Committee of the International Society for Clinical Biostatistics. She is the author or coauthor of 68 papers published in peer-reviewed international journals.

Stefanos Bonovas, MD, M.Sc., Ph.D., graduated from the Medical School, University of Athens, and completed a medical residency in General Practice. He earned his M.Sc. in Biostatistics and his Ph.D. in Pharmacoepidemiology from the Medical School, University of Athens, Greece. His research focuses in the areas of pharmacoepidemiology, drug safety, public health, infectious disease surveillance, outbreak investigation, and meta-analysis of clinical research.

Dimitrios Paraskevis, Ph.D., is Assistant Professor of Epidemiology and Preventive Medicine in the Department of Hygiene, Epidemiology and Medical Statistics at Athens University Medical School in Greece. Dr. Paraskevis has a master of science in Molecular Biology and a doctoral degree in Molecular Epidemiology of viruses. His research interests cover the epidemiology, molecular epidemiology, and evolution of viral infectious diseases, molecular diagnostics, as well as the resistance to antivirals. He is a panel member of the European HIV Drug Resistance and Tropism Guidelines.

Melpomeni Malliori-Minerva, DDS, MD, Ph.D., is Associate Professor of Psychiatry at Athens University Medical School in Greece. She is Member of the Management Board of the European Monitoring Centre for Drugs and Drug Addiction. Dr. Malliori-Minerva was President of the Greek Organization against Drugs and vice President of the Hellenic Centre for Disease Control and Prevention. She was Member of the European Parliament and has served as its representative to the European Centre for Disease Prevention and Control. She has 35 publications in international medical journals and books, and 70 publications in national medical journals and books.
Angelos Hatzakis, MD, M.Sc., Ph.D., is Professor of Epidemiology and Preventive Medicine, and former Director of the Department of Hygiene, Epidemiology and Medical Statistics at Athens University Medical School in Greece. He is founder and Head of the National Retrovirus Reference Center, and founder and Chair of the “Hepatitis B & C Public Policy Association.” Prof. Hatzakis has participated in many Executive Committees and was President of the Hellenic Center for Disease Control and Prevention. His research interests cover epidemiology and preventive medicine including virology, pathogenesis, prevention, and treatment of viral diseases and oncogenic viruses (human retroviruses, hepatitis viruses, herpes viruses).

Samuel R. Friedman, Ph.D., is Director of Infectious Disease Research at National Development and Research Institutes, Inc. and the Director of the Interdisciplinary Theoretical Synthesis Core in the Center for Drug Use and HIV Research, New York City. Dr. Friedman is an author of about 450 publications on HIV/hepatitis C/STIs, and drug use epidemiology and prevention. Honors include an NIDA Avant Garde Award (2012), the International Rolleston Award of the International Harm Reduction Association (2009), the first Sociology AIDS Network Award for Career Contributions to the Sociology of HIV/AIDS (2007), and a Lifetime Contribution Award, Association of Black Sociologists (2005).
Footnotes
Declaration of Interest:
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or other funding agencies.
The reader is referred to Hills’s criteria for causation, which were developed in order to assist researchers and clinicians determine if risk factors were causes of a particular disease or outcomes or merely associated. (Hill, A. B. (1965). The environment and disease: associations or causation? Proceedings of the Royal Society of Medicine 58:295–300.).
The reader is asked to consider that concepts and processes such as “risk,” “vulnerability,” and “protective” factors are often noted in the literature, without adequately delineating their dimensions (linear, nonlinear, rates of development, sustainability, cessation, etc.), their “demands,” the critical necessary conditions (endogenously as well as exogenously; micro to macro levels) which are necessary for them to operate (begin, continue, become anchored and integrate, change as de facto realities change, cease, etc.) or not to operate and whether their underpinnings are theory-driven, empirically based, individual and/or systemic stake holder-bound, historically bound, based upon “principles of faith” or what. This is necessary to clarify, if possible, if these terms are not to remain as yet additional shibboleths in a field of many stereotypes. Editor’s note.
References
- Arampatzi A, Nicholls WJ. The urban roots of anti-neoliberal social movements: The case of Athens, Greece. Environment and Planning A. 2012;44(11):2591–2610. Retrieved June 3, 2014, from http://www.envplan.com/abstract.cgi?id=a44416. [Google Scholar]
- Arie S. Has austerity brought Europe to the brink of a health disaster? BMJ (Clinical Research Ed) 2013;346(jun18_4):f3773. doi: 10.1136/bmj.f3773. [DOI] [PubMed] [Google Scholar]
- Bonovas S, Nikolopoulos G. High-burden epidemics in Greece in the era of economic crisis. Early signs of a public health tragedy. Journal of Preventive Medicine and Hygiene. 2012;53(3):169–171. Retrieved June 3, 2014 from http://www.ncbi.nlm.nih.gov/pubmed/23362624. [PubMed] [Google Scholar]
- Brand H, Rosenkötter N, Clemens T, Michelsen K. Austerity policies in Europe-bad for health. BMJ (Clinical Research Ed) 2013;346:f3716. doi: 10.1136/bmj.f3716. Retrieved June 3, 2014 from http://www.ncbi.nlm.nih.gov/pubmed/23766465. [DOI] [PubMed] [Google Scholar]
- Chang SS, Stuckler D, Yip P, Gunnell D. Impact of 2008 global economic crisis on suicide: Time trend study in 54 countries. BMJ (Clinical Research Ed) 2013;347:f5239. doi: 10.1136/bmj.f5239. Retrieved June 3, 2014 from http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3776046&tool=pmcentrez&rendertype=abstract. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Danis K, Baka A, Lenglet A, Van Bortel W, Terzaki I, Tseroni M, Kremastinou J. Autochthonous Plasmodium vivax malaria in Greece, 2011. Euro Surveillance: Bulletin Européen Sur Les Maladies Transmissibles = European Communicable Disease Bulletin. 2011;1642 Retrieved June 3, 2014, from http://www.ncbi.nlm.nih.gov/pubmed/22027375. [PubMed] [Google Scholar]
- Danis K, Lenglet A, Tseroni M, Baka A, Tsiodras S, Bonovas S. Malaria in Greece: Historical and current reflections on a re-emerging vector borne disease. Travel Medicine and Infectious Disease. 2013;11(1):8–14. doi: 10.1016/j.tmaid.2013.01.001. [DOI] [PubMed] [Google Scholar]
- Danis K, Papa A, Papanikolaou E, Dougas G, Terzaki I, Baka A, Kremastinou J. Ongoing outbreak of West Nile virus infection in humans, Greece, July to August 2011. Euro Surveillance: Bulletin Européen Sur Les Maladies Transmissibles = European Communicable Disease Bulletin. 2011;16(34) Retrieved June 3, 2014 from http://www.ncbi.nlm.nih.gov/pubmed/21903037. [PubMed] [Google Scholar]
- Danis K, Papa A, Theocharopoulos G, Dougas G, Athanasiou M, Detsis M, Panagiotopoulos T. Outbreak of West Nile virus infection in Greece, 2010. Emerging Infectious Diseases. 2011;17(10):1868–1872. doi: 10.3201/eid1710.110525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Des Jarlais DC, Arasteh K, Friedman SR. HIV among drug users at Beth Israel Medical Center, New York City, the first 25 years. Substance Use & Misuse. 2011;46(2–3):131–139. doi: 10.3109/10826084.2011.521456. [DOI] [PubMed] [Google Scholar]
- Des Jarlais DC, Braine N, Friedmann P. Unstable housing as a factor for increased injection risk behavior at US syringe exchange programs. AIDS and Behavior. 2007;11(6 Suppl):78–84. doi: 10.1007/s10461-007-9227-6. [DOI] [PubMed] [Google Scholar]
- Duong YT, Qiu M, De AK, Jackson K, Dobbs T, Kim AA, Parekh BS. Detection of recent HIV-1 infection using a new limiting-antigen avidity assay: Potential for HIV-1 incidence estimates and avidity maturation studies. PloS One. 2012;7(3):e33328. doi: 10.1371/journal.pone.0033328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Economou M, Madianos M, Peppou LE, Patelakis A, Stefanis CN. Major depression in the era of economic crisis: A replication of a cross-sectional study across Greece. Journal of Affective Disorders. 2013;145(3):308–314. doi: 10.1016/j.jad.2012.08.008. [DOI] [PubMed] [Google Scholar]
- Economou M, Madianos M, Peppou LE, Theleritis C, Patelakis A, Stefanis C. Suicidal ideation and reported suicide attempts in Greece during the economic crisis. World Psychiatry: Official Journal of the World Psychiatric Association (WPA) 2013;12(1):53–59. doi: 10.1002/wps.20016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Economou M, Madianos M, Peppou LE, Theleritis C, Stefanis CN. Suicidality and the economic crisis in Greece. Lancet. 2012;380:9839–337. doi: 10.1016/S0140-6736(12)61244-6. author reply 337–338. [DOI] [PubMed] [Google Scholar]
- Einstein S. Failure and psychoactive substances have been part of this living world and humankind since the Beginning. Introduction. Substance Use & Misuse. 2012;47(13–14):1360–1364. doi: 10.3109/10826084.2012.706152. [DOI] [PubMed] [Google Scholar]
- European Centre for Disease Prevention and Control. Risk Assessment on HIV in Greece. 2012 Retrieved June 3, 2014 from http://www.ecdc.europa.eu/en/publications/layouts/forms/Publication_DispForm.aspx?ID=730&List=4f55ad51-4aed-4d32-b960-af70113dbb90.
- European Monitoring Centre for Drugs and Drug Addiction. HIV outbreak among injecting drug users in Greece. 2012 Retrieved June 3, 2014 from http://www.emcdda.europa.eu/publications/ad-hoc/2012/greece-hiv-update.
- European Monitoring Centre for Drugs and Drug Addiction. Country overview: Greece. 2014 Retrieved June 4, 2014 from http://www.emcdda.europa.eu/publications/country-overviews/el#harm.
- Eurostat. General government deficit. 2014a Retrieved June 3, 2014 from http://epp.eurostat.ec.europa.eu/tgm/table.do?tab=table&init=1&language=en&pcode=tec00127&plugin==1.
- Eurostat. General government gross debt. 2014b Retrieved June 3, 2014 from http://epp.eurostat.ec.europa.eu/tgm/refreshTableAction.do?tab=table&plugin=1&pcode=teina225&language=en.
- Eurostat. Infant mortality. 2014c Retrieved June 3, 2014 from http://epp.eurostat.ec.europa.eu/tgm/table.do?tab=table&init=1&language=en&pcode=tps00027.
- Eurostat. Real GDP growth rate. 2014d Retrieved June 3, 2014 from http://epp.eurostat.ec.europa.eu/tgm/table.do?tab=table&init=1&plugin=1&language=en&pcode=tec00115.
- Eurostat. Unemployment rate. 2014e Retrieved June 3, 2014 from http://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=une_rt_a&lang=en.
- Friedman SR. Teamster rank and file Power, bureaucracy and rebellion at work and in a union. New York: Columbia University Press; 1982. [Google Scholar]
- Friedman SR, Bolyard M, Khan M, Maslow C, Sandoval M, Mateu-Gelabert P, Aral SO. Group sex events and HIV/STI risk in an urban network. Journal of Acquired Immune Deficiency Syndromes (1999) 2008;49(4):440–446. doi: 10.1097/qai.0b013e3181893f31. Retrieved June 3, 2014 from http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3410442&tool=pmcentrez&rendertype=abstract. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman SR, Bolyard M, Mateu-Gelabert P, Goltzman P, Pawlowicz MP, Singh DZ, Flom PL. Some data-driven reflections on priorities in AIDS network research. AIDS and Behavior. 2007;11(5):641–651. doi: 10.1007/s10461-006-9166-7. [DOI] [PubMed] [Google Scholar]
- Friedman SR, Curtis R, Neaigus A, Jose B, Des Jarlais DC. Social networks, drug injectors’ lives and HIV/AIDS. New York: Kluwer Academic Publishers; 2002. [Google Scholar]
- Friedman SR, Downing MJ, Smyrnov P, Nikolopoulos G, Schneider JA, Livak B, Hatzakis A. Sociallyintegrated transdisciplinary HIV prevention. AIDS and Behavior. 2013 doi: 10.1007/s10461-013-0643-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman SR, Kottiri BJ, Neaigus A, Curtis R, Vermund SH, Des Jarlais DC. Networkrelated mechanisms may help explain long-term HIV-1 seroprevalence levels that remain high but do not approach population-group saturation. American Journal of Epidemiology. 2000;152(10):913–922. doi: 10.1093/aje/152.10.913. Retrieved June 3, 2014 from http://www.ncbi.nlm.nih.gov/pubmed/11092433. [DOI] [PubMed] [Google Scholar]
- Friedman SR, Mateu-Gelabert P, Sandoval M. Group sex events amongst non-gay drug users: An understudied risk environment. The International Journal on Drug Policy. 2011;22(1):1–8. doi: 10.1016/j.drugpo.2010.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman SR, Neaigus A, Jose B, Curtis R, Goldstein M, Ildefonso G, Des Jarlais DC. Sociometric risk networks and risk for HIV infection. American Journal of Public Health. 1997;87(8):1289–1296. doi: 10.2105/ajph.87.8.1289. Retrieved June 3, 2014 from http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1381088&tool=pmcentrez&rendertype=abstract. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman SR, Reid G. The need for dialectical models as shown in the response to the HIV/AIDS epidemic. International Journal of Sociology and Social Policy. 2002;22:177–200. [Google Scholar]
- Friedman SR, Rossi D, Braine N. Theorizing “Big Events” as a potential risk environment for drug use, drug-related harm and HIV epidemic outbreaks. The International Journal on Drug Policy. 2009;20(3):283–291. doi: 10.1016/j.drugpo.2008.10.006. [DOI] [PubMed] [Google Scholar]
- Friedman SR, Rossi D, Flom PL. “Big Events” and Networks. Connections (Toronto, Ont) 2006;27(1):9–14. Retrieved June 3, 2014 from http://www.pubmedcentral.nih.gov/articlerender.fcgi?artidd=3143004&tool=pmcentrez&rendertype=abstract. [PMC free article] [PubMed] [Google Scholar]
- Friedman SR, Sandoval M, Mateu-Gelabert P, Rossi D, Gwadz M, Dombrowski K, Perlman D. Theory, measurement and hard times: Some issues for HIV/AIDS research. AIDS and Behavior. 2013;17(6):1915–1925. doi: 10.1007/s10461-013-0475-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman SR, Vasylyeva T, Smyrnov P. Recentlyfunded transdisciplinary integrated HIV prevention project: Overview and challenges. Somatosphere. 2012 Retrieved June 3, 2014 from http://somatosphere.net/2012/10/recently-fundedtransdisciplinary-integrated-hiv-prevention-project-overviewand-challenges.html.
- Georgakas D. Greece nearing the breaking point. Solidarity. 2013 Retrieved June 3, 2014 from http://www.solidarityus.org/node/3851.
- Hellenic Centre for Disease Control and Prevention. HIV/AIDS surveillance report in Greece. 2013 Retrieved June 3, 2014 from http://www.keelpno.gr.
- Hellenic Statistical Authority. Greece in figures. 2014 Retrieved June 3, 2014 from http://eu2014presidency.statistics.gr/eu2014/index.php/en/greece-in-figures.
- International Monetary Fund. World economic outlook. Hopes, realities, and risks. 2013 Retrieved June 3, 2014 from http://www.imf.org/external/pubs/ft/weo/2013/01/
- Kang JS, Shambaugh JC. The evolution of current account deficits in the Euro Area periphery and the Baltics: Many paths to the same endpoint. 2013 Retrieved June 3, 2014, from http://www.imf.org/external/pubs/cat/longres.aspx?sk=40792.
- Karanikolos M, Mladovsky P, Cylus J, Thomson S, Basu S, Stuckler D, McKee M. Financial crisis, austerity, and health in Europe. Lancet. 2013;381(9874)(13):1323–1331. 60102–6. doi: 10.1016/S0140-6736. [DOI] [PubMed] [Google Scholar]
- Kentikelenis A, Karanikolos M, Papanicolas I, Basu S, Mc-Kee M, Stuckler D. Health effects of financial crisis: Omens of a Greek tragedy. Lancet. 2011;378(9801):1457–1458. doi: 10.1016/S0140-6736(11)61556-0. [DOI] [PubMed] [Google Scholar]
- Kentikelenis A, Papanicolas I. Economic crisis, austerity and the Greek public health system. European Journal of Public Health. 2012;22(1):4–5. doi: 10.1093/eurpub/ckr190. [DOI] [PubMed] [Google Scholar]
- Kondilis E, Gavana M, Giannakopoulos S, Smyrnakis E, Dombros N, Benos A. Payments and quality of care in private for-profit and public hospitals in Greece. BMC Health Services Research. 2011;11:234. doi: 10.1186/1472-6963-11-234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kondilis E, Giannakopoulos S, Gavana M, Ierodiakonou I, Waitzkin H, Benos A. Economic crisis, restrictive policies, and the population’s health and health care: The Greek case. American Journal of Public Health. 2013;103(6):973–979. doi: 10.2105/AJPH.2012.301126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kondilis E, Smyrnakis E, Gavana M, Giannakopoulos S, Zdoukos T, Iliffe S, Benos A. Economic crisis and primary care reform in Greece: Driving the wrong way? The British Journal of General Practice: The Journal of the Royal College of General Practitioners. 2012;62(598):264–265. doi: 10.3399/bjgp12x641546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kousoulis AA, Chatzigeorgiou KS, Danis K, Tsoucalas G, Vakalis N, Bonovas S, Tsiodras S. Malaria in Laconia, Greece, then and now: A 2500-year-old pattern. International Journal of Infectious Diseases: IJID: Official Publication of the International Society for Infectious Diseases. 2013;17(1):e8–e11. doi: 10.1016/j.ijid.2012.09.013. [DOI] [PubMed] [Google Scholar]
- Ladbury GAF, Gavana M, Danis K, Papa A, Papamichail D, Mourelatos S, Panagiotopoulos T. Population seroprevalence study after a West Nile virus lineage 2 epidemic, Greece, 2010. PloS One. 2013;8(11):e80432. doi: 10.1371/journal.pone.0080432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li J, Liu H, Li J, Luo J, Des Jarlais D, Koram N. Role of sexual transmission of HIV among young noninjection and injection opiate users: A respondent-driven sampling study. Sexually Transmitted Diseases. 2011;38(12):1161–1166. doi: 10.1097/OLQ.0b013e3182315772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Linton SL, Celentano DD, Kirk GD, Mehta SH. The longitudinal association between homelessness, injection drug use, and injection-related risk behavior among persons with a history of injection drug use in Baltimore, MD. Drug and Alcohol Dependence. 2013;132(3):457–465. doi: 10.1016/j.drugalcdep.2013.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madianos M, Economou M, Alexiou T, Stefanis C. Depression and economic hardship across Greece in 2008 and 2009: Two cross-sectional surveys nationwide. Social Psychiatry and Psychiatric Epidemiology. 2011;46(10):943–952. doi: 10.1007/s00127-010-0265-4. [DOI] [PubMed] [Google Scholar]
- Malliori M, Golna C, Souliotis K, Hatzakis A. Financial crisis, austerity, and health in Europe. Lancet. 2013;382(9890)(13):392. 61664–5. doi: 10.1016/S0140-6736. [DOI] [PubMed] [Google Scholar]
- Mungiu-Pippidi A. The good, the bad and the ugly: Controlling corruption in the European union. 2013 Retrieved June 3, 2014 from http://www.againstcorruption.eu/reports/the-goodthe-bad-and-the-ugly-controlling-corruption-in-the-europeanunion/
- Nikolopoulos G, Paraskevis D, Hatzakis A. HIV epidemiology in Greece. Future Microbiology. 2008;3(5):507–516. doi: 10.2217/17460913.3.5.507. [DOI] [PubMed] [Google Scholar]
- Paraskevis D, Nikolopoulos G, Fotiou A, Tsiara C, Paraskeva D, Sypsa V, Hatzakis A. Economic recession and emergence of an HIV-1 outbreak among drug injectors in Athens metropolitan area: A longitudinal study. PloS One. 2013;8(11):e78941. doi: 10.1371/journal.pone.0078941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paraskevis D, Nikolopoulos G, Tsiara C, Paraskeva D, Antoniadou A, Lazanas M, Hatzakis A. HIV-1 outbreak among injecting drug users in Greece, 2011: A preliminary report. Euro Surveillance : Bulletin Européen Sur Les Maladies Transmissibles=European Communicable Disease Bulletin. 2011;16(36) doi: 10.2807/ese.16.36.19962-en. Retrieved June 3, 2014 from http://www.ncbi.nlm.nih.gov/pubmed/21924120. [DOI] [PubMed] [Google Scholar]
- Pharris A, Wiessing L, Sfetcu O, Hedrich D, Botescu A, Fotiou A, van de Laar MJ. Human immunodeficiency virus in injecting drug users in Europe following a reported increase of cases in Greece and Romania, 2011. Euro Surveillance: Bulletin Européen Sur Les Maladies Transmissibles = European Communicable Disease Bulletin. 2011;16(48) Retrieved June 3, 2014 from http://www.ncbi.nlm.nih.gov/pubmed/22172301. [PubMed] [Google Scholar]
- Potterat JJ, Phillips-Plummer L, Muth SQ, Rothenberg RB, Woodhouse DE, Maldonado-Long TS, Muth JB. Risk network structure in the early epidemic phase of HIV transmission in Colorado Springs. Sexually Transmitted Infections. 2002;78(Suppl 1):i159–i163. doi: 10.1136/sti.78.suppl_1.i159. Retrieved June 3, 2014 from http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1765823&tool=pmcentrez&rendertype=abstract. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reinhart CM, Rogoff KS. This time is different: A panoramic view of eight centuries of financial crises. 2008 Retrieved June 3, 2014 from http://www.nber.org/papers/w13882.
- Reyes JC, Robles RR, Colón HM, Matos TD, Finlinson HA, Marrero CA, Shepard EW. Homelessness and HIV risk behaviors among drug injectors in Puerto Rico. Journal of Urban Health: Bulletin of the New York Academy of Medicine. 2005;82(3):446–455. doi: 10.1093/jurban/jti073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rhodes T, Simic M. Transition and the HIV risk environment. BMJ (Clinical Research Ed) 2005;331(7510):220–223. doi: 10.1136/bmj.331.7510.220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rhodes T, Stimson GV, Crofts N, Ball A, Dehne K, Khodakevich L. Drug injecting, rapid HIV spread, and the risk environment: Implications for assessment and response. AIDS. 1999;13(Suppl A):S259–S269. Retrieved June 3, 2014 from http://www.ncbi.nlm.nih.gov/pubmed/10885783. [PubMed] [Google Scholar]
- Rothenberg RB, Long DM, Sterk CE, Pach A, Potterat JJ, Muth S, Trotter RT. The Atlanta urban networks study: A blueprint for endemic transmission. AIDS. 2000;14(14):2191–2200. doi: 10.1097/00002030-200009290-00016. Retrieved June 3, 2014 from http://www.ncbi.nlm.nih.gov/pubmed/11061661. [DOI] [PubMed] [Google Scholar]
- Rothenberg RB, Potterat JJ, Woodhouse DE, Muth SQ, Darrow WW, Klovdahl AS. Social network dynamics and HIV transmission. AIDS. 1998;12(12):1529–1536. doi: 10.1097/00002030-199812000-00016. Retrieved June 3, 2014 from http://www.ncbi.nlm.nih.gov/pubmed/9727575. [DOI] [PubMed] [Google Scholar]
- Seymour R. Golden Dawn’s rise signals breakdown of the Greek state’s authority. 2013 Retrieved June 3, 2014 from http://www.theguardian.com/commentisfree/2013/sep/24/goldendawn-greece-state-authority.
- Strathdee SA, Stachowiak JA, Todd CS, Al-Delaimy WK, Wiebel W, Hankins C, Patterson TL. Complex emergencies, HIV, and substance use: No “big easy” solution. Substance Use & Misuse. 2006;41(10–12):1637–1651. doi: 10.1080/10826080600848116. [DOI] [PubMed] [Google Scholar]
- Stuckler D, Basu S. The InternationalMonetary Fund’s effects on global health: Before and after the 2008 financial crisis. International Journal of Health Services: Planning, Administration, Evaluation. 2009;39(4):771–781. doi: 10.2190/HS.39.4.j. Retrieved June 3, 2014 from http://www.ncbi.nlm.nih.gov/pubmed/19927414. [DOI] [PubMed] [Google Scholar]
- Stuckler D, Basu S, Suhrcke M, Coutts A, McKee M. The public health effect of economic crises and alternative policy responses in Europe: An empirical analysis. Lancet. 2009;374(9686):315–323. doi: 10.1016/S0140-6736(09)61124-7. [DOI] [PubMed] [Google Scholar]
- Stuckler D, Basu S, Suhrcke M, McKee M. The health implications of financial crisis: A review of the evidence. The Ulster Medical Journal. 2009;78(3):142–145. Retrieved June 3, 2014 from http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2773609&tool=pmcentrez&rendertype=abstract. [PMC free article] [PubMed] [Google Scholar]
- Sypsa V, Paraskevis D, Malliori M, Nikolopoulos GK, Panopoulos A, Kantzanou M, Hatzakis A. Homelessness and other risk factors for HIV infection in the current outbreak among injection drug users in Athens, Greece. American Journal of Public Health. 2014 doi: 10.2105/AJPH.2013.301656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Economist. Greece’s default: The wait is over. 2012 Retrieved June 3, 2014 from http://www.economist.com/node/21550271.
- The Organization for Economic Co-operation and Development. Better Life Index, Greece. 2013 Retrieved June 3, 2014 from http://www.oecdbetterlifeindex.org/countries/greece.
- Vlachadis N, Kornarou E. Increase in stillbirths in Greece is linked to the economic crisis. BMJ (Clinical Research Ed) 2013;346:f1061. doi: 10.1136/bmj.f1061. Retrieved June 3, 2014 from http://www.ncbi.nlm.nih.gov/pubmed/23423369. [DOI] [PubMed] [Google Scholar]
- World Health Organization – Regional Office for Europe. Health, health systems and economic crisis in Europe: Impact and policy implications. World Health Organization; Copenhagen, Denmark: 2013. Retrieved June 3, 2014 from http://www.euro.who.int/en/media-centre/events/events/2013/04/oslo-conference-on-health-systems-and-theeconomic-crisis/documentation/working-documents/health,-health-systems-and-economic-crisis-in-europe-impact-andpolicy-implications. [Google Scholar]