

Abstract
Cystic hygroma is a benign lymphatic malformation most commonly occurring in the cervico-facial region. It arises from sequestered lymphatic sacs that fail to communicate with the lymphatico-venous system. Although commonly presenting in paediatric age, cystic hygroma can occur at any age. Recurrent cystic hygroma is a known entity and can result from inadequate excision or specific tumour characteristics. We report such a case of giant recurrent cystic hygroma in the neck in a 14 years old female the surgical management of which was challenging due to the large size, previous adhesions and proximity to vital structures.
Keywords: Recurrent cystic hygroma, Large size, Surgical challenges, India
Case Report
A 14 years old female presented with swelling in right side of neck since birth. The swelling was gradually growing and painless with no compressive symptoms. Her only complaint of disfigurement made her visit a surgeon at the age of 10 years at a rural hospital, where it was diagnosed as cystic hygroma and subsequently operated. Four months following the surgery, the patient again developed swelling in the same region. The swelling gradually grew to attain the present size causing disfigurement without pain or compressive symptoms.
On examination, there was a cystic swelling of about 20 x 15 cm, situated in the right side of neck extending from mastoid process, along the ramus of mandible superiorly; to supraclavicular region inferiorly; anteriorly from the thyroid cartilage to midline posteriorly. The swelling was ill defined, smooth, cystic, fluctuant and transilluminant. The scar of previous incision and drain site was seen over the swelling. Trachea was deviated to opposite side. There were no signs of neurovascular deficit of the ipsilateral arm.
Routine blood investigations were normal. X-ray neck showed a soft tissue swelling on right side of the neck with tracheal deviation to the left. Contrast Enhanced Computed Tomography (CECT) of neck and chest was suggestive of ill-defined cystic lesion with multiple internal septations measuring 17.5 x 14 x 7.5 cm extending superiorly from level of right mastoid tip; inferiorly into the supraclavicular region; infero-medially small component into the pre-vertebral region from C7 to T2 level; anteriorly it was abutting the right angle of mandible and right submandibular gland; laterally it was extending through the intermuscular plane medial to right sternocleidomastoid muscle (SCM) and lateral to right paraspinal muscles. It was displacing the trachea and oesophagus to the left and indenting the apical pleura on the right. The mass displaced the right carotid artery antero-medially and right internal jugular vein (IJV) laterally causing its compression.
The neck was explored using a reverse ‘J’ shaped incision extending from right mastoid tip to middle one third of right SCM curving medially to cross the midline at the level of thyroid. After dividing the SCM for attaining wide exposure the cyst was found abutting the IJV and carotid artery which were carefully dissected away. The spinal accessory nerve and IJV were preserved. Complete excision of the cyst was done with combination of blunt and sharp dissection, shaving it off from the cervical nerve roots. The intra-operative findings corroborated with the CECT report. The cyst weighed 485gms. Postoperatively the patient recovered uneventfully, with minimal drain output which was removed on the 5th day; the patient was later discharged on 7th day after suture removal. Histopathology description of the mass is as follows: 18 x 15 cm multiloculated mass with multiple cysts draining serous fluid with gummous material seen at places. Section showed large lymphatic channels and dilated spaces (cysts) lined by flattened endothelium with abundant aggregates of lymphocytes in the stroma; consistent with benign cystic lymphangioma of the mixed type variety. The patient has been followed up for one year without symptoms or recurrence.
Discussion
Cystic hygroma is a benign lymphatic malformation also known as cystic lymphangioma. Lymphangiomas are classified as capillary, cavernous and cystic lymphangiomas of which cystic lymphangiomas are commonest. They are also classified based on the size of the cysts; microcystic measuring less than 2 cm in diameter, macrocystic measuring more than 2 cm, mixed lymphangioma is characterized by cysts of variable sizes. In 8th week of embryogenesis; six lymphatic sacs develop. These are two jugular sacs, two iliac, one at the base of root of mesentery and one dorsal to the abdominal aorta known as cysterna chyli. With the development of lymphatico-venous system these lymph sacs communicate with the lymphatic network and in 9th week of gestation, these sacs are invaded by connective tissue to form lymph nodes. Cystic hygroma develops from sequestered lymphatic sacs which fail to communicate with the lymphatic or venous system. Dilatation of these sequestered lymphatic tissues results in the cystic morphology of these lesions containing milky, serous, sero-sanguinous or straw-coloured fluid1.
Cystic hygroma can occur in any region of the body, the common locations being cervico-facial region (75-80%), axilla, mediastinum and groin. Other regions are oral cavity, omentum, mesentery and rarer regions include limbs, chest wall, cheek, lumbar region, supra-sternal area and deltoid. Due to the infiltrative nature of cystic hygromas, they may extend to the soft tissue of neck, cross midline, reach axilla, mediastinum and cause neural encroachment. Most cystic hygromas present at the time of birth (60%) or before the age of 2 years (90%) and hence most of the literature on management considers paediatric patients2. Symptoms of cystic hygroma depend on the position and relationship to surrounding structures. The most common presentation in an adult is a painless asymptomatic lump. Cases of rapid enlargement over a short period of time have been reported frequently3-6 with compression and incorporation of major structures such as the larynx, trachea, oesophagus, brachial plexus and great vessels5 , with pain, hoarseness, dysphagia and breathlessness3,5,6 , causing a restriction of neck movement7. Other complications are infection, abscess, haemorrhage and rupture. Cystic hygromas can be staged as proposed by de Serres8.
Diagnostic investigations include ultrasonography (USG) and CECT scan. CECT scan can delineate the extent, relation to adjacent structures in a better way and it is recommended when surgery is contemplated.
Treatment options include surgery, sclerotherapy, simple drainage, radiation, laser excision, radio-frequency ablation and cauterization9. However surgery remains the preferred modality of treatment. Indications for treatment are recurrent infection, respiratory distress, dysphagia, haemorrhage within the cyst, sudden increase in the size, lymph discharging sinus and disfigurement.
The postoperative complications usually observed after surgical excision of cystic hygroma are wound infection, haemorrhage, hypertrophied scar and lymphatic discharge from the wound. Complex cystic hygromas recur in about 10-27% of cases, even after apparent complete excision and 50-100% in partial excision10. Recurrence is due to incomplete excision, is more common with the microcystic and mixed type as they have a tendency to interdigitate into tissue planes, enveloping neural and vascular tissues and complete excision is difficult and hazardous11 . Despite these possible complications, surgical excision of the cystic hygroma is still a preferred option.
Previously, sclerotherapy with boiling water, quinine, sodium morrhuate, urethane, iodine tenture, doxycycline and nitromin were used. However, the success rate with such agents have been low and with frequent associated complications12. At present sclerotherapy with bleomycin and OK-432 have shown good response, the latter showing more satisfactory response and lesser complications than bleomycin13, 14.
Unusual cases have been reported7,15-18. Ramachandran et al reported a recurrent cystic hygroma in a 17 years old female15 while Saxena and co-worker described a cystic hygroma in a 35 years female who was long treated as a case of tuberculosis16. Furthermore, Paladino et al reported a case of recurrent cystic hygroma 3 days after surgery17.
Cystic hygroma although known in paediatric age group can present at any age and should be considered as a differential diagnosis. Surgery is the best modality of treatment and the first operative intervention offers the best opportunity for complete excision. Surgery of a complex recurrent cystic hygroma, such as this case report, involving deep and vital structures, is challenging. Extreme care needs to be taken to avoid on table complications and incomplete excision in case of infiltration to the surrounding structures. What we found challenging in this patient are the size, weight, extent of the lesion, age at presentation and the operative complexity involved in order to ensure complete excision
Fig 1. Recurrent Cystic Hygroma on right side of neck.

Fig 2. X-rays of the neck and chest showing soft tissue swelling on right side of neck with tracheal deviation to left side.
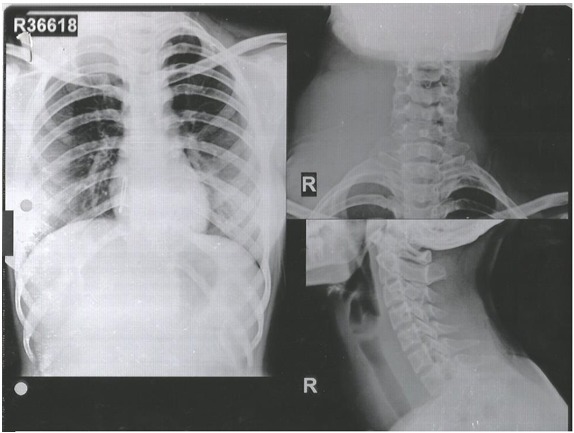
Fig 3. Contrast Enhanced CT showing recurrent cystic hygroma.
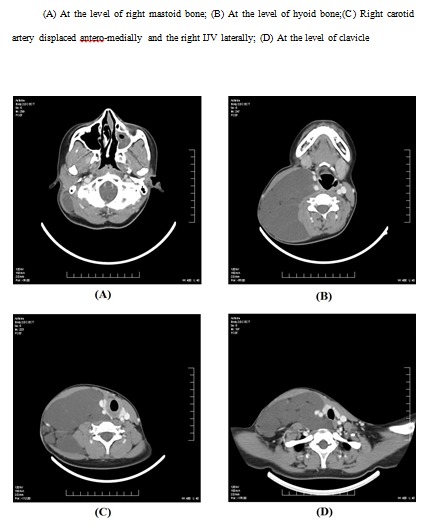
Fig 4. Intra-operative image showing the cystic hygroma with the cut edges of SCM muscle .
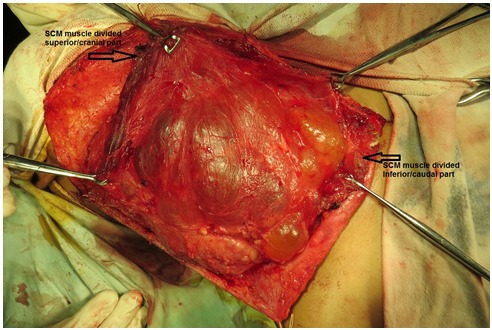
Fig 5. Intra-operative image showing the cystic hygroma dissected away from IJV .
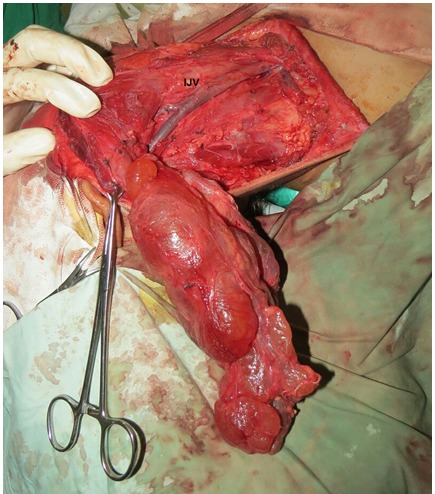
Fig 6. Specimen of the recurrent cystic hygroma .

Footnotes
Competing Interests: The authors have declared that no competing interests exist.
Grant support: None
References
- 1.Fonkalsrud EW, Grosfeld, JL; O'Neill, JA Jr; Coran, JA; Fonkalsrud, EW; Caldamone, AA; Pediatric surgery. 6th edition. Chicagor: Mosby Elsevie; 2006. Lymphatic disorders. pp. 2137–2145. [Google Scholar]
- 2.Kaur N, Gupta A, Amratash, Singh N. Giant cystic hygroma of the neck with spontaneous rupture. J Indian Assoc Pediatr Surg. 2007;12:154–155. [Google Scholar]
- 3.Kraus J, Plzak J, Bruschini R. Cystic lymphangioma of the neck in adults: a report of three cases. Wiener Klin Wochenschr. 2008;120:242–245. doi: 10.1007/s00508-008-0950-4. [DOI] [PubMed] [Google Scholar]
- 4.de Casso Moxo C, Lewis NJ, Rapado F. Lymphangioma presenting as a neck mass in the adult. Int J Clin Pract . 2001;55:337–338. [PubMed] [Google Scholar]
- 5.Cheng LHH, Wells FC. A multidisciplinary approach to recurrent cervicothoracic cystic hygroma in an adult. Br J Oral Maxillofacial Surg. 2004;42:66–68. doi: 10.1016/S0266-4356(03)00173-6. [DOI] [PubMed] [Google Scholar]
- 6.Vaid L, Gupta M, Gupta N, Singh P. Bleomycin sclerotherapy in a rare case of adult-onset cervical lymphangioma. Ear Nose Throat J. 2010;89:E23–E26. [PubMed] [Google Scholar]
- 7.Gow L, Gulati R, Khan A, Mihaimeed F. Adult-onset cystic hygroma: a case report and review of management. Grand Rounds. 2011;11:5–11. [Google Scholar]
- 8.de Casso Moxo C, Lewis NJ, Rapado F. Lymphangioma presenting as a neck mass in the adult. Int J Clin Pract . 2011;55:337–338. [PubMed] [Google Scholar]
- 9.Sheila S, Nazarian-Mobin, Simms K, Urata MM, Tarczy-Hornoch K, Jeffrey A. Misleading presentation of an orbital lymphangioma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:82–85. doi: 10.1016/j.tripleo.2009.08.042. [DOI] [PubMed] [Google Scholar]
- 10.Oldham, KT; Colombani, PM; Foglia, RP; Dillon P. Surgery of Infants and Children: Scientific Principles and Practice. Philadelphia: Lippincott-Raven; 1997. Lymphatic and venous disorders. pp. 1727–1743. [Google Scholar]
- 11.Seashore JH, Gardiner LJ, Ariyan S. Management of giant cystic hygromas in infants. Am J Surg. 1985;149:459–465. doi: 10.1016/s0002-9610(85)80040-4. [DOI] [PubMed] [Google Scholar]
- 12.Ibrahim AH, Kandeel A, Bazeed MF. Successful non surgical management of a huge life threatening cervicomediastinal cystic hygroma case report and review of the literature. . J Pediatr Surg Specialt. 2009;3:48–50. [Google Scholar]
- 13.Niramis R, Watanatittan S, Rattanasuwan T. Treatment of cystic hygroma by intralesional bleomycin injection: experience in 70 patients. Eur J Pediatr Surg. 2010 May;20(3):178–182. doi: 10.1055/s-0030-1247548. [DOI] [PubMed] [Google Scholar]
- 14.Peters DA, Courtemanche DJ, Heran MK. Treatment of cystic lymphatic vascular malformations with OK-432 sclerotherapy. Plast Reconstr Surg. 2006 Nov;118(6):1441–1446. doi: 10.1097/01.prs.0000239503.10964.11. [DOI] [PubMed] [Google Scholar]
- 15.Ramachandran V, Rajan P. Recurrent Cystic Hygroma. The Internet Journal of Surgery. 2001;3(1) [Google Scholar]
- 16.Saxena P, Chandra D. Cystic Hygroma of neck in an adult female: Case report and literature review. The Internet Journal of Surgery. 2009;22(2) [Google Scholar]
- 17.Paladino NC, Scerrino G, Chianetta D, Di Paola V, Gulotta G, Bonventre S. Recurrent cystic lymphangioma of the neck. Case report. Ann Ital Chir. 2014 01 - 03;85(1):69–74. [PubMed] [Google Scholar]
- 18.Bihani Ameya, Lodha Jaini, Dokhe Yogesh, Hardikar Priyanka, Sharma Arpit, Dabholkar Jyoti. A Giant Cystic Hygroma in Adult – A Surgical Challenge. BMR Medicine. 2014;1(2):1–5. [Google Scholar]