

Abstract
Infantile temporomandibular joint septic arthritis is an uncommon paediatric infection, but one which carries the potential for severe morbidity and mortality. Early diagnosis and aggressive medical and possibly surgical management is indicated for the best outcomes. The presenting clinical features are non-specific in a neonate and an infant; as such a high degree of clinical suspicion is required. We present the case of an eleven-month-old boy who has made a full recovery from an acute temporomandibular joint septic arthritis and review the relevant literature.
Key words: Temporomandibular joint, magnetic resonance imaging, septic arthritis
Introduction
Septic arthritis of the temporomandibular joint (TMJ) is an uncommon condition in children and it is rarely reported in the literature.1-4 The infection carries the risk of severe long term morbidity and mortality if effective diagnosis and treatment are not instituted. The clinical presenting features in neonates and young infants are non-specific requiring a high degree of clinician suspicion to elucidate the diagnosis. The most common clinical clues at presentation include trismus, pain, tenderness, swelling and erythema.2
The signs and symptoms may be similar to other conditions including cellulitis, rheumatological disease, dental abscess, pharyngitis, retropharyngeal abscess, peritonsillar abscess, acute otitis media, mastoiditis, parotitis, submandibular sialadenitis, and lymphadenopathy.2,3 Investigation of febrile children with facial swelling should consider TMJ infection as potential diagnosis.
We report an eleven-month-old infant whose clinical presentation of fever, mild facial swelling and trismus lead to the elucidation of right sided TMJ septic arthritis via magnetic resonance imaging (MRI).
Case Report
An eleven-month-old boy presented with 24 h history of right facial swelling and 48 h history of persistent fever, drooling and poor oral solid intake. He had had one week history of upper respiratory tract infection including coughing, rhinorrhoea and intermittent fever and had been treated with antipyretic and oral fluid. He was not on regular medications and was up-to-date with his immunization.
Physical examination revealed facial asymmetry due to mild-moderate pre-auricular swelling and tenderness including right zygomatic arch region and infratemporal fossa. His throat was erythematous with bilateral cervical lymphadenopathy. He had a fever of 39.1°C, a white cell count of 24.0x109/L, neutrophils 74% and a C-reactive protein concentration of 145 mg/L. He was admitted to the paediatric unit of the hospital and was commenced on intravenous antibiotics (ceftriaxone, gentamicin and metronidazole).
MRI on Day 3 of admission revealed an inflammatory and apparently infective process in the right temporal region and infratemporal fossa (Figures 1 and 2). The primary focus of the inflammation/infection was at the right temporomandibular joint with effusion and subtle marrow change. There was evidence of the thickening of the meninges through the right squamous temporal fossa and mild oedema within the right mastoid air cells and the other surrounding soft tissues. The radiological images suggested septic arthritis of right TMJ, supported by the clinical findings of guarding to contact, and apparent limitation of mandibular movement.
Figure 1.
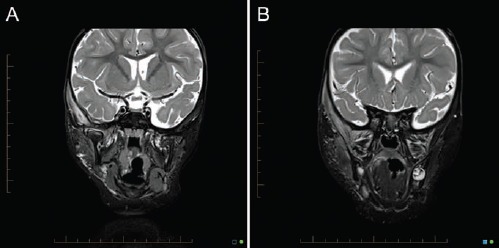
A and B) Coronal T2 (turbo inversion recovery) images demonstrates a right temporomandibular joint effusion with surrounding inflammation which extends through the temporalis and pterygoid muscles, as well as permeating through the right squamous temporal bone to cause a small temporal epidural inflammatory reaction, and reactive changes in the mastoid air cells, and reactive cervical adenopathy.
Figure 2.
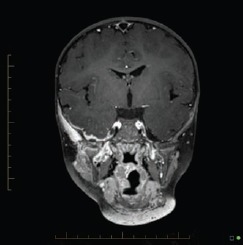
Coronal images reformatted T1 space post gadolinium.
Infective disease specialist, otorhinolaryngologist and maxillofacial surgeon were consulted and the recommendation was to continue conservative management with intravenous antibiotic treatment, which was switched to single agent of timentin (ticarcillin and clavulanate) from day 5 of admission. A central venous catheter was inserted to facilitate the administration of antibiotic. Blood culture collected before the commencement of antibiotic remained negative after five days.
The patient became afebrile from day 3 of admission. His facial swelling and tenderness were gradually settled over the following two weeks. His oral solid intake progressively returned to normal, after a week of nasogastric feeding, with no evidence of impairment of jaw movement. An ultrasound study of his right face and neck on day 8 of admission reviewed no focal fluid collection in the region. C-reactive protein returned to normal on day 10 of admission. In view of the unusual nature of severe infection of this young patient, immune function studies was performed to exclude X-linked chronic granulomatous disease. Immunoglobulin levels, neutrophil oxidative burst, and lymphocyte subsets all returned normal results.
A repeated MRI on day 13 of admission showed improvement in the extent of inflammatory response around the right TMJ with small persistent joint effusion. The overall shape of the joint was preserved although the size appeared slightly smaller (Figures 1 and 2). The patient was discharged home on day 16 of admission and continued on daily intravenous ceftriaxone for one more week as outpatient, followed by a further three months of oral cephalexin treatment. The patient received three months of oral antibiotic treatment and showed no signs of TMJ dysfunction or deformity. Twelve months after the acute event, our patient continued to demonstrate normal oromotor function.
Discussion
Septic arthritis of the TMJ is an uncommon condition in children and it is rarely reported in the literature.1-4 Investigation of children with febrile illness with facial swelling should consider TMJ infection as potential diagnosis. The signs and symptoms may be similar to other conditions including cellulitis, rheumatological disease, dental abscess, pharyngitis, retropharyngeal abscess, peritonsillar abscess, acute otitis media, mastoiditis, parotitis, submandibular sialadenitis, and lymphadenopathy.2,3 A retrospective review shows septic arthritis of the TMJ is most often found in male adult with an average age of 36 years.5 The common presentations include trismus, pain and tenderness, swelling and erythema.2 Patient with this condition may not have the classic presentation of septic arthritis, i.e. febrile illness with unilateral swollen and tender TMJ.
Risk factors for septic arthritis of the TMJ include head and neck infection, systemic and autoimmune disease, iatrogenic causes, burn wounds, blunt trauma and sexual contact.3 Staphylococcus aureus and Staphylococcus saprophyticus, Streptococcus species, Neisseria and Haemophilus influenzae are the most commonly isolated pathogen.3,5,6 The causative organism may infect the joint by hematogenous spread, from a contiguous infection, by penetration injury of the joint space or following a blunt trauma of the joint.2,4 Severe complications may arise from septic arthritis of the TMJ including intracranial abscess, joint destruction, ankylosis and impaired growth of the condyle.3-7 A causative organism was not identified in our patient, we hypothesis that the preceding upper respiratory tract infection induced hematogenous spread of the offending organism. Surgical drainage of the joint was avoided in view of surgical induced joint ankylosis, and the patient was making an excellent clinical recovery.
Laboratory investigations include neutrophilia and elevated C-reactive protein concentration is supportive for the diagnosis. Blood cultures and joint fluid aspiration may assist the identification of the causative organism.3 MRI can demonstrate the joint effusion and allows the evaluation of the joint surfaces and adjacent soft tissues during the acute infection.2,5 The computed tomography is useful in the chronic stage of infection to demonstrate the bony changes related to cortical breakdown, osteomyelitis, and ankylosis of the TMJ.2,5 With such an unusual infection it is always prudent to exclude a primary immune deficiency especially X-linked chronic granulomatous disease.
There is no clear consensus regarding treatment for the septic arthritis of the TMJ.3,5 Intravenous broad-spectrum antibiotics should be commenced empirically once the septic arthritis is suspected as delayed treatment could result in severe complications. Even a small detriment to joint growth has profound and long-term effects on mandibular function and facial appearance. The antibiotic treatment regime can be modified if the culture and the sensitivity results are available. Aggressive intravenous antibiotic therapy, and possibly surgical drainage of the TMJ, are paramount in preventing both acute and chronic complications of the disease process.
Surgical drainage of the infected TMJ, such as needle aspiration, arthroscopy and arthrotomy,5,8,9 is indicated when abscess formation is developed, bony involvement is suspected, or poor response to antimicrobial treatment alone.3,10 The use of intra-articular antimicrobial irrigation is controversial and there is a concomitant risk of introducing new microbe into the infected joint.3,10 During the acute infection, nasogastric feed may help to minimize the TMJ movement in order to reduce discomfort. However, mouth movement should be encouraged once the joint pain subsides.3,5 These patients should be followed up to monitor the development of complication and the growth of the mandible.
Conclusions
In conclusion, septic arthritis of the TMJ is an uncommon condition in children, but one is a differential diagnosis for the child with facial swelling especially with concomitant trismus. Early diagnosis and prompt treatment are vital in prevention of serious complications.
References
- 1.Parmar J. Case Report: septic arthritis of the temporomandibular joint in a neonate. Br J Oral Maxillofac Surg 2008;46:505-6. [DOI] [PubMed] [Google Scholar]
- 2.Gayle EA, Young SM, McKenna SJ, et al. Septic arthritis of the temporomandibular joint: case reports and review of the literature. J Emerg Med 2013;45:674-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Leighty SM, Spach DH, Myall RW, et al. Septic arthritis of the temporomandibular joint: review of the literature and report of two cases in children. J Oral Maxillofac Surg 1993;22:292-7. [DOI] [PubMed] [Google Scholar]
- 4.Amos MJ, Patterson AR, Worrall SF. Septic arthritis of the temporomandibular joint in a 6-year-old child. J Oral Maxillofac Surg 2008;46:242-3. [DOI] [PubMed] [Google Scholar]
- 5.Cai XY, Yang C, Zhang ZY, et al. Septic arthritis of the temporomandibular joint: a retrospective review of 40 cases. J Oral Maxillofac Surg 2010;68:731-8. [DOI] [PubMed] [Google Scholar]
- 6.Chaves Netto HD, Nascimento FF, Chaves Md, et al. TMJ ankylosis after neonatal septic arthritis: literature review and two case reports. Oral Maxillofac Surg 2011;15:113-9. [DOI] [PubMed] [Google Scholar]
- 7.Regev E, Koplewitz BZ, Nitzan DW, et al. Ankylosis of the temporomandibular joint as a sequela of septic arthritis and neonatal sepsis. Pediatr Infect Dis J 2003;22:99-101. [DOI] [PubMed] [Google Scholar]
- 8.Cai XY, Yang C, Chen MJ, et al. Arthroscopic management of septic arthritis of temporomandibular joint. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:24-30. [DOI] [PubMed] [Google Scholar]
- 9.Sembronio S, Albiero AM, Robiony M, et al. Septic arthritis of the temporomandibular joint successfully treated with arthroscopic lysis and lavage: case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:e1-6. [DOI] [PubMed] [Google Scholar]
- 10.Hekkenberg RJ, Piedade L, Mock D, et al. Septic arthritis of the temporomandibular joint. Head Neck Surg 1999;120:780-2. [DOI] [PubMed] [Google Scholar]