

Abstract
The gall bladder is least common intra-abdominal organ to be involved by tuberculosis. It is either part of systemic miliary tuberculosis or abdominal tuberculosis. Isolated gall bladder tuberculosis is even rarer, can presents either as calculus or acalculus cholecystitis. Gall bladder tuberculosis presenting as a localized perforation with a sinus formation into anterior abdominal wall is unreported complication in a non immuno-compromised person. A 48-year old female presented with a gradually increasing swelling in right hypochondrium. Abdominal ultrasound showed superficial collection over right hypochondrium with intraperitoneal extension. Computed tomography showed localized gall bladder perforation with extension to the abdominal wall. Patient underwent emergency exploration and cholecystectomy with excision of sinus tract and drainage of abdominal wall abscess. Histopathological examination showed granulomatous cholecystitis suggestive of tuberculosis of gall bladder with extension into the sinus tract. She had an uneventful recovery and was treated with 6-month antitubercular therapy after surgery.
Key words: Gall bladder tuberculosis, gall bladder perforation
Introduction
Abdominal tuberculosis is one of the most common types of extra-pulmonary tuberculosis (TB).1 Its prevalence in developing countries has been estimated to be high and increasing. In recent years, the increasing incidence of TB has been attributed to several causes, including the acquired immunodeficiency syndrome and intravenous drug abuse. Isolated tuberculosis of gall bladder is still extremely rare and the diagnosis of this disease is almost always overlooked unless there is a high index of suspicion. First case of gall bladder TB was reported in 1870 by Gaucher and till now less than 120 cases have been reported in the English medical literature.1 This infrequent involvement of the gall bladder has been attributed to the high concentration, high alkalinity of the bile and bile acids inhibiting the growth of tuberculosis bacillus. Previous damage to the gall bladder due to gallstones can be an initiating factor for the development of tuberculous-cholecystitis.2
It is even rarer to find tubercular gall bladder perforating and creating a subcutaneous sinus into anterior abdominal wall. We report such a case.
Case Report
A 48-year old female presented in the surgical emergency with a sudden history of increasing swelling over the right hypochondrium (Figure 1). Initially it was painless but gradually became painful and increased in size. Later it spontaneously busted and purulent discharge started coming from a pinhole like rent from the center of swelling followed by fever and non-projectile vomiting. Her personal and family history was unremarkable. Laboratory parameters depicted low hemoglobin (8.7 g/dL), leukocytosis (13,900/cc), had normal blood sugar levels and non-reactive HIV serology. Her chest x-ray was also within normal limits. Ultrasound abdomen revealed a large ill-defined hypo echoic collection in the right upper abdomen, which was extending to anterior abdominal wall. Contrast-enhanced computed tomography (CECT) of abdomen showed localized gall bladder perforation with intra-abdominal collection, which was extending to the right hypochodrium area (Figure 2). She underwent exploratory laparotomy where dense adhesions were found between abdominal wall, liver, gall bladder area and duodenum, which were walled off by omentum. After adhesiolysis the liver, intestines and peritoneum grossly looked normal. Gall bladder surrounded by a small collection near the fundus, was highly friable and edematous up to cystic duct where a stone was palpable at its neck. Common bile duct was normal on palpation. A sinus tract was extending to the anterior abdominal wall from the area near gall bladder fundus (Figure 3). Cholecystectomy and excision of the sinus tract with drainage of the superficial collection was performed. Histopathological examination showed granulomatous cholecystitis suggestive of gall bladder tuberculosis, with evidence of involvement into the sinus tract (Figures 4 and 5). The pus culture of the superficial collection was unremarkable. She recovered and developed mild discharge from wound which healed with repeated dressings and she left hospital on her 7th post operative day. Subsequently she was started on four-drug (isoniazide + rifampicin + ethambutol + pyrazinamide) anti-tubercular intensive treatment for two months and maintenance therapy with two drugs (isoniazide + rifampicin) for another four months. After completion of six months total therapy she is on follow up and is free from any symptoms.
Figure 1.

Clinical photograph showing the abscess over right hypochondrium (white arrow).
Figure 2.

Contrast-enhanced computed tomography image showing the contracted gall bladder (arrowhead) with the subcutaneous collection (asterix).
Figure 3.

Intra-operative image showing the gall bladder area (black arrow) with the sinus tract in the anterior abdominal wall (white arrow).
Figure 4.
High power photomicrograph showing epitheloid cell granuloma, giant cells and surrounding lymphocytes (hematoxylin & eosin; 100X).
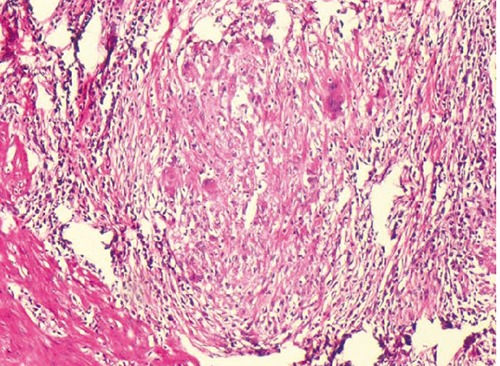
Figure 5.

Low power photomicrograph showing part of mucosal epithelium and presence of epitheloid cell granuloma in the serosa (hematoxylin & eosin; 100X).
Discussion
Abdominal tuberculosis constitutes about 1% of all tuberculosis.3 The infection usually spreads via the hematogenous route, from adjacent caseating lymph nodes or peritoneal tubercles. The gall bladder is infected by mycobacterium tuberculosis as a part of four distinct clinical varieties: i) as a component of military tuberculosis in children and in adults; ii) as a component of disseminated abdominal tuberculosis; iii) isolated gall bladder tuberculosis without overt tubercular foci elsewhere in the body; and iv) Involvement of gall bladder in anergic states due to uraemia, cancer or immunodeficiency.3 Presentation of gall bladder tuberculosis with spontaneous rupture into abdominal wall is unknown and extremely rare.
As gall bladder TB is rare and no pathognomonic imaging feature is known. Trans abdominal ultrasound findings are nonspecific for gall bladder tuberculosis.2 CECT abdomen findings of localized gall bladder perforation with abdominal wall collection are also not specific for tuberculosis. Concomitant presence of tuberculosis with gall bladder malignancy is reported along with all gall bladder tuberculosis masquerading as malignancy.4 The diagnosis is usually made on histological examination of the gall bladder specimen after cholecystectomy.5 Sensitivity of acid-fast stain and culture result is low, histopathological diagnosis of gall bladder tuberculosis can be very demanding. TB-polymerase chain reaction can also be performed on the resected specimen, which has high sensitivity and specificity.5 Gall bladder TB should be considered in the differential diagnosis of diseases with an irregular, hypodense thickened gall bladder wall with pericholecystic edematous changes and abdominal wall abscess.
Cholelithiasis and cystic duct obstruction are considered as important factors in the development of complication after gall bladder tuberculosis.2,3 It has been suggested that cystic duct obstruction leads to disappearance of bile acids and decreasing the alkalinity from the gall bladder, lowers the resistance to this infection. As tuberculous cholecystitis is difficult to diagnose, all resected cholecystectomy specimens should be sent for histopathological examination for evidence of tuberculosis along with ruling out co existing malignancy.4,6
Conclusions
Gall bladder TB is a rare finding that is diagnosed post operatively on histopathology. Due to paucity of cases, establishing preoperative diagnostic criteria is difficult.
References
- 1.Xu XF, Yu RS, Qiu LL, et al. Gallbladder tuberculosis: CT findings with histopathologic correlation. Korean J Radiol 2011;12:196-202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rejab H, Guirat A, Ellouze S, et al. Primitive gallbladder tuberculosis: a case report with review of the literature. Ann Ital Chir 2013;84:1-3. [PubMed] [Google Scholar]
- 3.Kumar K, Ayub M, Kumar M, et al. Tuberculosis of the gallbladder. HPB Surg 2000;11:401-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sharma S, Bansal R, Agrawal N, et al. Tuberculosis of the gall bladder clinically mimicking carcinoma - a case report. J Indian Med Assoc 2012;110:402-3. [PubMed] [Google Scholar]
- 5.Ryu MJ, Jeon TJ, Park JY, et al. A case of gallbladder tuberculosis diagnosed by positive tuberculosis-polymerase chain reaction. Korean J Gastroenterol 2014;63:51-5. [DOI] [PubMed] [Google Scholar]
- 6.Javed A, Arora A, Kalayarasan R, et al. Gallbladder cancer management impacted by coexistent tuberculosis. Trop Gastroenterol 2013;34:87-90. [DOI] [PubMed] [Google Scholar]