

Abstract
The preservation of remaining root structure and alveolar bone covering them with denture has been used since many years. Tooth-retained overdentures transfer occlusal forces to the alveolar bone through the periodontal ligament of the retained tooth roots and thereby prevent bone resorption. Applications of magnets in overdenture technique has been widely used in dentistry in the field of prosthodontics, as they can be manufactured in small dimensions as retentive devices for complete denture, removable partial dentures, obturators and maxillofacial prosthesis. This article presents a simple and efficient method of fabrication of mandibular over denture retained by magnets in a patient whose mandibular residual ridge is severely resorbed with few remaining teeth and maxillary conventional removable partial denture. Mandibular over denture retained by magnets assembly consist of magnet and coping with keeper on remaining tooth structure to rehabilitate the patient since magnetic attachments can provide support, stability and retention.
Keywords: Magnet, Keeper, Overdenture, Micro laser welding
Introduction
The ultimate objective of prosthodontic service is to make the patient as nearly normal function as possible. The basic overdenture concept requires preservation of residual soft and hard tissues. Use of attachments and adherence to basic principles of complete denture design can improve both retention and stability of overdentures [1].Traditionally the vast majority of problems arise with a mandibular prosthesis, as due to the anatomy of the mandible often they fail to provide adequate support, retention and stability [2, 3]. In an attempt to help these patients, a variety of aids and materials have been tried such as springs, suction cups, adhesives, implants of various types, and magnets [4].
Dental magnetic attachment systems have been increasingly utilized in prosthodontics due to the development of hard magnetic substances such as samarium-cobalt [5–7] and iron–neodymium–boron magnets (Fe14Nd2B) [8–10]. Conventional overdenture placement involves embedding the magnetic assembly in the denture base and inserting its corresponding keeper into the abutment root. The magnetic assembly holds the keeper with a retentive force [11–14].
This clinical tip describes fabrication of mandibular over denture retained by magnets to highlights its benefits and maxillary conventional removable partial denture to rehabilitate the patient.
Clinical Report
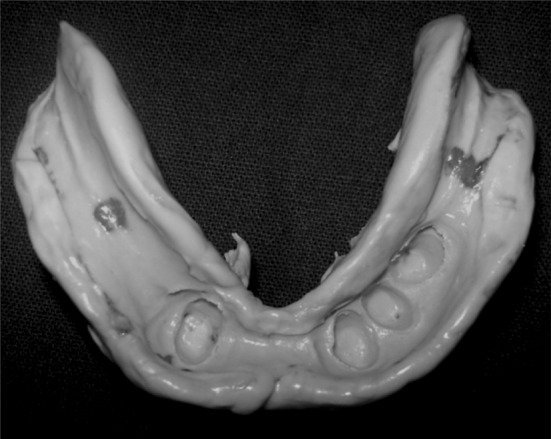
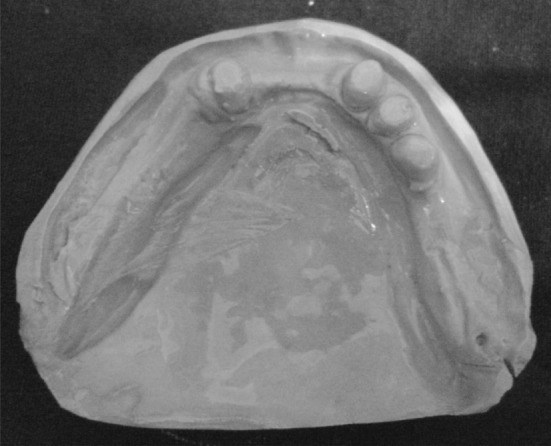
A 74-year-old man was referred to the department of prosthodontics at M.S. Ramaiah dental college, Bangalore. The medical history was non-contributory. Intraoral evaluation revealed partially edentulous maxillary and mandibular arch. Remaining teeth in mandibular arch were grade I mobile (Fig. 1). The patient was made aware of the situation and had expressed a desire to maintain the remaining teeth as long as possible. In mandibular arch remaining teeth were root canal treated, minimal vestibular depth and severe resorption in relation to bilateral mandibular posterior ridge. Others oral findings were unremarkable.
Fig. 1.

Pre-operative upper and lower arch (mandibular teeth were endodontically treated)
Clinical Procedure and Technique
Abutment Teeth Preparation for Mandibular Teeth
Abutment teeth (32,33,34 and 43) were prepared with diamond rotatory instruments (Shofu, Kyoto, Japan), producing a chamfer margin and decoronated slightly above the gingival margin followed by removal of two-third of the root canal filling material with a stainless rotary instrument (Peasow reamer; Dentsply, York, Pa) to prepare the post space to accommodate post along with keeper (Fig. 2). Cervical portion of all the abutment teeth were marginally bevelled to prevent any stress concentration eventually to prevent root fracture.
Fig. 2.

Post space preparations, gingival retraction and impressions of posts
Impression
Gingival retraction (Ultrapak cord#000, SKU:137, Ultradent; South Jordon, UT) followed by full arch impression with polysiloxane impression materials (Aquasil, Dentsply International Inc, USA) to record the margin area and root post was successfully made and definitive cast(Ultrarock, type IV dental stone; Kalabhai Karson Ltd, Vikhroli (W), Mumbai, India), was fabricated (Fig. 3, 4).
Fig. 3.

Polysiloxane impression of abutment teeth and posts
Fig. 4.

Definitive cast
Laboratory Fabrication
Wax-Up
Indirect inlay wax (Kerr co; USA) was used to make impression of root canal to fabricate the post and verified and 0.5 mm inlay wax was kept for the placement of keepers on root teeth (Fig. 6).
Fig. 6.

Keepers were placed and wax-up was done for casting along with posts
Keepers Setting
The cast bonded keeper method was used to firmly fix the keepers (Root keeper; Aichi Steel Co, Aichi, Japan) on the root teeth. The keeper has flat shape with an attractive face on one side and a dimple face on the other place. Attractive side was kept facing up on the wax-up. All the keepers were placed parallel to the occlusal plane ensured by surveying procedure (Fig. 5). Sprue wax attached to the wax-up unit (Fig. 6) and casting polishing and finishing was done to all root caps.
Fig. 5.
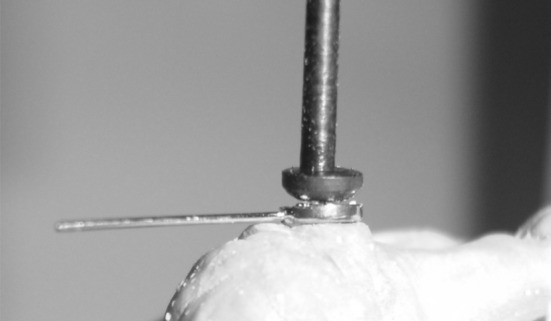
Surveying procedure
Try-In and Setting of Root Caps
All root caps were cemented on the roots teeth with glass ionomer cement (GC co; Tokyo, Japan). Excess cement was removed (Fig. 7) after cementing root caps, functional impression was made with polysiloxane impression materials (Reprosil, monophase; Dentsply International Inc, USA) under a proper pressure (Fig. 8) and definitive cast (Ultrarock, type IV dental stone; Kalabhai Karson Ltd, Vikhroli(W), Mumbai, India) was poured (Fig. 9). Now gypsum dummy (Ultrarock) was fabricated on the top of the keepers’ attractive surface of the cast so as coincided with both central axes to create space for magnetic assembly, larger than the magnetic assembly itself (Fig. 10). Now occlusal rims were fabricated on definitive upper and lower cast. Jaw relation, teeth arrangement and try- in was completed on waxed denture (Fig. 11) and processed. All interceptive occlusal contacts were eliminated before fixing the magnetic assembly in intaglio surface of overdenture.
Fig. 7.

Keepers along with post were cemented with resin cement
Fig. 8.
Border molding and functional impression
Fig. 9.
Definitive cast
Fig. 10.

Gypsum dummy (above dark line) was fabricated on the top of the keepers attractive surface of the cast
Fig. 11.

Complete wax-up trial
Setting the Magnetic Assembly into the Overdenture
All magnets (Magfit; Aichi Steel Corp, Aichi, Japan) were kept on the top of keeper so as to coincide with both central axes and autopolymerizing cure resin (DPI-RR; Wallace street, Mumbai, India) was filled into the space left for magnetic assembly in intaglio surface of mandibular overdenture, placed in oral cavity and asked the patient to occlude till curing of resin. Excess of resin removed and occlusion was checked to remove interceptive occlusal contacts and finished denture was delivered to the patient (Figs. 12, 13).
Fig. 12.

Magnets were attached in lower denture with the help of self-cure resin in patient’s mouth
Fig. 13.

Post-operative upper partial denture and lower magnet retained overdenture
Discussion
Magnet systems have been used as aids to denture retention for many years with some success [15]. These attachment systems, consisting of a magnet and a keeper, are used to retain removable partial dentures and maxillofacial prostheses. Magnetic system can also be used in an implant supported overdenture with magnets comprises magnets incorporated into the denture acting upon keepers attached to implant abutments [3]. Since these rare-earth magnets are vulnerable to corrosion, especially in the oral environment, they are covered and sealed with a yoke cap [16].
In this case the attachment system or magnetic assembly utilized a stainless steel casing hermetically sealed by micro-laser welding which provide assembly a corrosive resistant environment in oral cavity and magnets need not to be replaced after long time in use which is a major advantage over other magnet system and attractive force created by magnets were 400 gramforce (gf) to achieve adequate retention as multiple abutment teeth were used to retain denture.
Dental magnetic attachments of various types and sizes that have satisfactory retentive force and stability are now commercially available. An overdenture with a magnetic attachment is a useful choice for an abutment tooth with chronic periodontal disease, because the magnetic attachment dissipates the lateral stress component on the abutment teeth and improves poor clinical crown-to-root ratios [11–14, 17–20]. In this described article the MAGFIT DX (Magfit; Aichi Steel Corp, Aichi, Japan) type magnets were used. The heights of magnets were 1.0 mm and keepers’ height and diameter were 0.5 and 3.0 mm respectively, selected according to the cross-section of the retained root.
Most commercially available magnetic attachments composed of a magnet and yoke made from ferromagnetic material [11–14, 17–20]. In this article neodymium–boron–iron (NdBFe) magnets, stainless steel (AUM20) yoke, keeper, disc and stainless steel keeper holder (SUS316) assembly have been used.
The magnetic system used to retain dentures may be an open-field or closed-field system. Whether the open-field system causes any deleterious effect by the magnetic flux that scatters to the tissues has not been determined [18]. In closed-field systems the external magnetic flux fields were eliminated by placing the magnetic components in a series, called an assembly. When the two poles of a magnet are connected by any ferromagnetic material such as iron or stainless steel, the external magnetic flux field is shunted through the steel plate (keeper), because this is a path of least resistance. This procedure not only eliminated much of the external magnetic flux field, it also made the attachment more efficient by use of both the north and south poles [15, 21]. Therefore it was not surprising to find the greatest retention force occurred with closed-field magnets at both speeds of separation. Magnet system used in this case was close field and magnetic field leakage at the gingival margin is substantially below the accepted united state safety standard of 0.02 T. Its closed-field nature also makes this system more biocompatible then open-field system as open-field uncoated magnets exhibit significant cytotoxic effects which may be attributed due to the release of corrosion by products which required to replace them as early as signs of corrosion develop [22–24].
A word of caution needs to be mentioned while fixing denture magnets with autopolymerizing acrylic resin. The force needed to separate magnets was designated as breakaway load expressed in terms of grams [25, 26]. Patient was instructed to apply minimal occlusal or bite force while fixing denture magnet as more pressure would displace magnets inwards which in turn decrease the breakaway force when the denture was later on inserted in patient’s mouth.
In this case magnet retained mandibular overdenture was constructed primarily on remaining anterior abutment which is quiet similar to the other reported cases of implant supported mandibular overdenture where implant are usually placed bilaterally in the anterior atrophic mandible in the canine regions, avoiding mental foramina to provide retention and soft tissue support. In both clinical situations retention and soft tissue support is gained by anterior abutment and posterior segments of mandible respectively [27–30].
Conclusion
This clinical tip on overdenture retained by magnetic assembly provided predictable retention, stability, support and was successfully rehabilitated when compared to overdenture with implants, teeth retained had better proprioception and satisfaction because of patients own teeth and also advantageous when cost and time factors were considered.
References
- 1.Mensor NC., Jr Attachment fixation for overdentures, Part I. J Prosthet Dent. 1977;37:366–373. doi: 10.1016/0022-3913(77)90137-8. [DOI] [PubMed] [Google Scholar]
- 2.Rutkunas V, Mizutani H (2004) Retentive and stabilizing properties of stud and magnetic attachments retaining mandibular overdenture. An in vitro study. Stomatol Baltic Dent Maxillofac J 6:85–90
- 3.Saha S, Ray-Chaudhuri A. Mandibular implant-retained complete overdenture using retentive abutments: a case report. Dent Update (England) 2009;36:154–158. doi: 10.12968/denu.2009.36.3.154. [DOI] [PubMed] [Google Scholar]
- 4.Moghadam BK, Scandrett FR. Magnetic retention for overdentures. J Prosthet Dent. 1979;41:26–29. doi: 10.1016/0022-3913(79)90351-2. [DOI] [PubMed] [Google Scholar]
- 5.Becker J. Permanent magnets. J Appl Phys. 1970;233:92–100. [Google Scholar]
- 6.Strnat KJ. The hard magnetic properties of rare earth-transition metal alloys. IEEE Trans Magn. 1972;8:511–516. doi: 10.1109/TMAG.1972.1067368. [DOI] [Google Scholar]
- 7.Tawara Y, Strnat KJ. Rare earth-cobalt permanent magnets near the 2–17 composition. IEEE Trans Magn. 1976;12:954–958. doi: 10.1109/TMAG.1976.1059138. [DOI] [Google Scholar]
- 8.Sagawa M, Fujimura S, Yamamoto H, Matsuura Y, Hiraga K. Permanent magnet materials based on the rare earth-iron-boron tetragonal compounds. IEEE Trans Magn. 1984;20:1584–1589. doi: 10.1109/TMAG.1984.1063214. [DOI] [Google Scholar]
- 9.Sagawa M, Fujimura S, Togawa N, Yamamoto H, Matsuura Y. New material for permanent magnets on a base of Nd and Fe. J Appl Phys. 1984;55:2083–2087. doi: 10.1063/1.333572. [DOI] [Google Scholar]
- 10.Croat JJ, Herbst JF, Lee RW, Pinkerton FE. Pr-Fe and Nd-Fe-based materials: a new class of high-performance permanent magnets. J Appl Phys. 1984;55:2078–2082. doi: 10.1063/1.333571. [DOI] [Google Scholar]
- 11.Maeda Y, Nakao K, Yagi K, Matsuda S. Composite resin root coping with a keeper for magnetic attachment for replacing the missing coronal portion of a removable partial denture abutment. J Prosthet Dent. 2006;96:139–142. doi: 10.1016/j.prosdent.2006.04.011. [DOI] [PubMed] [Google Scholar]
- 12.Van Waas MA, Kalk W, van Zetten BL, van Os JH. Treatment results with immediate overdentures: an evaluation of 4.5 years. J Prosthet Dent. 1996;76:153–157. doi: 10.1016/S0022-3913(96)90299-1. [DOI] [PubMed] [Google Scholar]
- 13.Obatake RM, Collard SM, Martin J, Ladd GD. The effects of sodium fluoride and stannous fluoride on the surface roughness of intraoral magnet systems. J Prosthet Dent. 1991;66:553–558. doi: 10.1016/0022-3913(91)90522-X. [DOI] [PubMed] [Google Scholar]
- 14.Boeckler AF, Morton D, Ehring C, Setz JM. Mechanical properties of magnetic attachments for removable prostheses on teeth and implants. J Prosthodont. 2008;17:608–615. doi: 10.1111/j.1532-849X.2008.00356.x. [DOI] [PubMed] [Google Scholar]
- 15.Gillings BRD. Magnetic retention for complete and partial overdentures, Part I. J Prosthet Dent. 1981;45:484–491. doi: 10.1016/0022-3913(81)90032-9. [DOI] [PubMed] [Google Scholar]
- 16.Okuno O, Ishikawa S, Imuro FT, Kinouchi Y, Yamada H, Nakano T, et al. Development of sealed cup yoke type dental magnetic attachment. Dent Mater J. 1991;10:172–174. doi: 10.4012/dmj.10.172. [DOI] [PubMed] [Google Scholar]
- 17.Sasaki H, Kinouchi Y, Tsutsui H, Yoshida Y, Karv M, Ushita T. Sectional prostheses connected by samarium–cobalt magnets. J Prosthet Dent. 1984;52:556–558. doi: 10.1016/0022-3913(84)90345-7. [DOI] [PubMed] [Google Scholar]
- 18.Akaltan F, Can G. Retentive characteristics of different dental magnetic systems. J Prosthet Dent. 1995;74:422–427. doi: 10.1016/S0022-3913(05)80386-5. [DOI] [PubMed] [Google Scholar]
- 19.Matsumura H, Kawasaki K. Magnetically connected removable sectional denture for a maxillary defect with severe undercut: a clinical report. J Prosthet Dent. 2000;84:22–26. doi: 10.1067/mpr.2000.107916. [DOI] [PubMed] [Google Scholar]
- 20.Riley MA, Walmsley AD, Harris IR. Magnets in prosthetic dentistry. J Prosthet Dent. 2001;86:137–142. doi: 10.1067/mpr.2001.115533. [DOI] [PubMed] [Google Scholar]
- 21.Gillings BR. Magnetic denture retention systems. In: Prieskel HW, editor. Precision attachments in prosthodontics. Chicago: Quintessence; 1985. pp. 19–24. [Google Scholar]
- 22.Barnothy MF. Biological effects of magnetic fields. New York: Plenum; 1964. pp. 29–306. [Google Scholar]
- 23.Drago CJ. Tarnish and corrosion with the use of intra oral magnets. J Prosthet Dent. 1991;66:536–540. doi: 10.1016/0022-3913(91)90519-3. [DOI] [PubMed] [Google Scholar]
- 24.Evans RD, Mc Donald F. Effect of corrosion products (Neodymium Iron Boron) on oral fibroblast proliferation. J Appl Biomater. 1995;6:199–202. doi: 10.1002/jab.770060309. [DOI] [PubMed] [Google Scholar]
- 25.Gillings BR (1976) Magnetic retention systems for overdentures. Aust Soc Prosthet Bull. 6–9
- 26.Gillings BR. Magnetic retention for overdentures, part II. J Prosthet Dent. 1983;49:607–618. doi: 10.1016/0022-3913(83)90382-7. [DOI] [PubMed] [Google Scholar]
- 27.Ohkubo C, Kobayashi M, Okamoto N, et al. Implant overdenture using Konus telescope on one-piece implant: a case report. Eur J Prosthodont Restor Dent. 2009;17:188–191. [PubMed] [Google Scholar]
- 28.Gallego L, Junquera L, Llorente S. Oral carcinoma associated with implant-supported overdenture trauma: a case report. Dent Traumatol. 2009;25:3–4. doi: 10.1111/j.1600-9657.2008.00721.x. [DOI] [PubMed] [Google Scholar]
- 29.Schneider GB, Synan WJ. Use of a single implant to retain a mandibular complete overdenture on the compromised atrophic alveolar ridge: a case report. Spec Care Dentist. 2011;31:138–142. doi: 10.1111/j.1754-4505.2011.00196.x. [DOI] [PubMed] [Google Scholar]
- 30.Flanagan D. An implant-retained maxillary overdenture to obturate a patent oronasal communication: a case report. J Oral Implantol. 2009;35:12–17. doi: 10.1563/1548-1336-35.1.12. [DOI] [PubMed] [Google Scholar]