

Abstract
Prosthesis refers to artificial replacement of an absent part of the human body. These prostheses help in psychological support of the patients and enhance their social acceptance. Complete or partial finger amputations are some of most frequently encountered forms of partial hand loss. Micro vascular reconstruction is the first choice of rehabilitation but when it is contraindicated, unavailable, unsuccessful or unaffordable, the prosthetic rehabilitation is an alternative for improving the psychological status of an individual. Most of these artificial prostheses make use of silicone. The present paper tries to combine aesthetics with function. The authors have created functionally active finger prosthesis with the help of electromechanical controls. The prosthesis is battery-powered, light-weight, and allows the user to regain complete control of flexion and extension movements of an artificial finger.
Electronic supplementary material
The online version of this article (doi:10.1007/s13191-014-0388-5) contains supplementary material, which is available to authorized users.
Keywords: Finger prosthesis, Amputees, Functional prosthesis
Introduction
The human race has travelled a wonderful journey during the period of evolution right from amphibians, to reptiles, to apes and finally to human. The signal change in human evolution was due to the upright gait. When man lifted his hands from the ground they were freed from the purpose of locomotion and were put into the service of intelligence. A finger is a type of digit, an organ of manipulation and sensation found in the hands of humans and other primates. Normally, humans have five digits, termed phalanges on each hand. They enable us to interact with our environment and help in many day to day functions [1]. It has been stated that thumb is the most important digit from functional standpoint [2].
Apart from the face, the hand is a representation of one’s self-image that others can easily notice. The loss of body part, especially one as visible as a finger or hand, can be emotionally upsetting for a person. It can manifest itself in the form of anxiety, depression or a post traumatic stress disorder [3]. Hand may be affected by many conditions varying from congenital abnormalities to diseases, but greatest cause of functional impairment is trauma, traumatic amputation of the fingers represents a serious insult to the hand, resulting in dramatic impairment of hand function. In addition to immediate loss of grasp, strength and security, the absence of finger may cause marked psychological trauma [4].
Finger and partial finger amputations are encountered forms of partial hand losses. Amputation can be at the level of (a) digit involving partial or total distal, middle or proximal phalanx and partial or total amputation of thumb, (b) meta-carpal level, (c) through wrist, (d) forearm (e) upper arm. Various treatment options are available to restore finger amputation [2]. The most suitable approach for rehabilitation depends on the amount of tissue involved, the involvement of bone, the angles and levels of amputation and the involvement of other fingers [5].
Nowadays a severely injured and traumatically amputated finger can be saved by microsurgical reimplantation. However, in some patients surgical reconstruction is contraindicated, unsuccessful, unavailable and unaffordable [4]. Also, many of the prostheses that have been designed are aesthetic but have functional limitations. For such patients a high quality aesthetic prosthesis with passive and active function can be helpful. This can especially useful in cases where there is significant amount of amputation resulting in functional impairment. Technology is advancing nowadays with electronic components becoming more compact and powerful. So it’s only logical that this improvement in technology be tried for the betterment of physically disabled patients. Previous attempts have been made to design functionally active finger prostheses with mixed amount of success [6, 7]. Prostheses that rely on the nerve and muscle conduction to produce movements are also under development. As technology advances so does its cost. So, for a country like India where majority of the patients cannot afford expensive replacements, cost effective technology is the answer.
This paper presents a case of partial hand amputation with missing index, middle, ring finger and distal heads of respective metacarpals. The authors have designed a prosthesis which is battery-powered, light-weight, and allows user to regain complete control of flexion and extension movements of an artificial finger. This allows the patient to regain the functional aspect and that too at an affordable price. The prosthesis adopts an integrated design approach between mechanics and control. This means that the overall hand design is the result of a full integration of mechanics and control, where the hand dynamic modelization and the design and development of the control system contribute to the refinement and optimization process of the hand mechanical parameters.
Case Presentation
A 52 year old male patient reported to the Department of Prosthodontics, Tamil Nadu Government Dental College and Hospital, Chennai, India with a chief complaint of missing lower anterior teeth. He had a history of trauma to his left hand while working in factory one year back. On examination there was gross, soft tissue and hard tissue defect with missing left index, middle and ring finger also, some soft tissue defect of little finger was also seen (Fig. 1). On radiographic examination, there was loss of left index, middle and ring finger at the level of distal heads of respective meta-carpals (Fig. 2). The distal phalanx of the little finger was also missing. The amputated area showed normal surrounding area and no signs of any infection or inflammation.
Fig. 1.

Clinical photograph of patient’s hand
Fig. 2.

Radiograph of the patient’s hand
Treatment Planning
The objective of any prosthetic rehabilitation is to eliminate the psychological consequences of the amputation and restore passive function by fabrication of a prosthesis which has good retention, is comfortable to use and aesthetically acceptable to the patient. Since the area of amputation was quite large in this case, the patient was also functionally impaired. Fabrication of a passive prosthesis would not have served him a greater purpose. Hence it was decided to explore viable options for restoring the functionality of the lost fingers while maintaining the aesthetics. At the same time, the prostheses had to be affordable since the patient could not bear a high financial burden for the treatment.
After considering various options, it was planned to replace the missing fingers as a unit instead of replacing them individually. Accordingly, a light weight basic framework of metal was designed which provided enough rigidity. In order to induce functionality into the prostheses, an electro-mechanical type of prosthesis was planned. The treatment plan was discussed with the patient and an informed consent was signed to ensure his willingness for prosthetic rehabilitation before starting the procedure.
Technique for Fabrication of Electro-Mechanical Robotic Finger Prosthesis
Impression Making
A thin layer of petroleum jelly was applied on the patients hand with missing finger to prevent adherence of impression material to the skin and hair. The area around the hand was boxed and a thin layer of irreversible hydrocolloid impression material was poured over the hand covering both palmer and dorsal surface of hand.
Model Preparation
The impression was then poured in Type III dental stone (Kalabhai & Co., Mumbai, India) and a positive replica of hand was retrieved (Fig. 3).
Fig. 3.

Plaster model of the patient’s hand
Armamentarium Used
For making electro-mechanical robotic hand armamentarium chosen was ARDUINO-micro controller, servo motors, joy stick, lithium batteries.
Arduino-micro controller: This is a chip which acts as an main controller also called as Mini CPU/Open Source Hardware. It has memory, software programmes written in C-Language.
Servo Motors: The purpose of choosing this motor was the advantage of controlling angle and the speed of these motors. They are small and compatible (2.5 × 2.5) in size. Has greater range of movement from 0° to 180° as compared to other DC motors.
Joy Stick: Input to the micro-controller was given with the help of joy stick. It could generate from a minimum 0 to maximum 5 v (0–5).
Lithium Batteries: They were used for power supply.
As per the design, a soft metal which was moldable in any form was selected and a basic skeletal structure was made. Two motors were attached in such a way so that each one replaced the middle and proximal phalanx of all three fingers in a single unit. These motors were connected to the micro-chip. Joy stick was attached to lateral aspect of little finger so that when little finger moves, the joy stick will also move with it in same speed and angle. This joy-stick was also connected to the micro-chip. And lastly, the batteries were connected to provide the power supply. The whole assembly was first assembled on the stone model and checked for the function (Fig. 4). Then whole assembly was then transferred and fitted on the patient’s hand for testing the functioning of the prosthesis (Fig. 5).
Fig. 4.
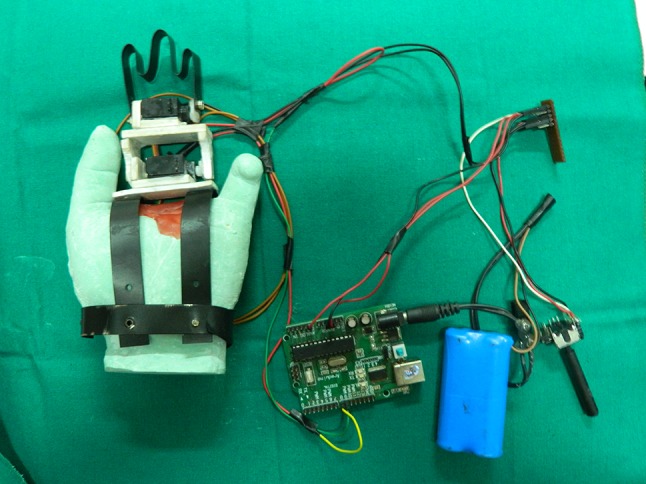
Prosthesis assembly mounted on the plaster model
Fig. 5.

Prosthesis assembly fitted on the patient’s hand
Mechanism
When the little finger moves, the joy stick attached to it also moves along with it and in this way it generates some voltage ranging from 0 to 5 v. Depending on movement of little finger, this voltage generated is detected by the micro-chip which in turn signals the motor to move with that speed and angle.
The prosthesis was tested for function by asking patient to grasp things like a bottle of water. A motor-bike glove cover was used to conceal the whole assembly and the fingers were sculpted with wax and were later fabricated into silicone. These were painted using acrylic colours and attached to the bike glove cover. Since the meta-carpal amputation involved the index, middle and little finger, the glove was modified and fitted in a way that the thumb and the little finger were free to move (Figs. 6, 7).
Fig. 6.

Functional movement of the prosthesis
Fig. 7.

Patient testing the functionality
Discussion
The amputation of one or more fingers of the hand, as the consequence of trauma or congenital absence of one or more phalanges, carries a serious reduction of hand function and social dysfunction for the patient. Nowadays many injuries and traumatic amputations of fingers can be treated by microsurgery through re-implantation. However, prosthesis can be provided in cases where surgery may not be advisable or possible which may offer great psychological aid [5].
Several reconstruction techniques have been described, such as toe-to-finger transfers, pollicisation, lengthening procedures and osteo-cutaneous flaps [8]. Reconstruction of an amputated finger may be achieved by surgical procedures but the cosmetic results may not be satisfactory. Weak retention, instability, and lack of sensibility are some of the drawbacks of traditionally used silicones [5].
The human hand represents a wonderful example of a natural biomechatronic system, which still represents a benchmark for robotic designers aimed at replicating its complex functionality. In the literature, several examples of robotic hands can be traced, ranging from simple grippers for industrial applications up to more sophisticated artefacts trying to mimic human mechanics.
Prosthetics was one of the first application fields envisaged for artificial anthropomorphic hands. Prosthetic applications of robotic technologies impose a series of challenging requirements regarding the cosmetic appearance, the size and the weight of the hand, and its embeddable control system, which is crucial for obtaining reliable and robust hand acceptable for end users [6]. Most of robotic fingers that have been designed have independent joint actuators for independent articulation. Inspite of the greater flexibility, the increased bulk makes it difficult for practical use as prosthesis. The motion of the fingers is not independent but has a certain linked relation. Limited space to install actuators is one of the most difficult problems in the design of prosthetic hands [7].
In the present case, the area of amputation was quite large with the absence of the residual stumps in the index, middle and ring fingers which would have made retention of a simple silicone prosthesis difficult. Also, the space was enough for the installation of a single actuator. Joints were minimized so that the entire prosthesis acted as a single unit. Due to the limited number of components used, it was possible to ensure that the size of the prosthesis was the same as that of the fingers. The framework was designed keeping in mind the motion of the human hand. The joystick controlling the motion of the prosthesis is connected to the little finger which ensures a smooth and synchronous motion.
The main advantage of this prosthesis over the conventional ones is the functionality which can be imparted to the amputated hand which goes a long way in boosting the psychological morale and social acceptance of the patient. This type of prosthesis can especially be useful in cases of large defects. With advancements in technology, the size of the components required may be reduced which may make the prosthesis suitable for single finger defects also. Advanced prostheses are being designed for entire arms which rely on electro-myographic signals from the muscles for carrying out motion. Developing an intelligent human—prosthesis interface remains a future work [7].
Conclusion
A simple robotic finger for a prosthetic fit has been introduced. The three fingers are controlled by a single actuator with synchronous motion. The driving force is given by the servo motors fitted to the framework. The position control command is initiated with the joy stick which is attached to the little finger. The designed robotic finger has a limited workspace due to the simple mechanism. However, it is very promising as a prosthetic finger.
Electronic supplementary material
References
- 1.James CH. Campbell’s operative orthopaedics. 10. St. Louis: Mosby Inc.; 2003. Amputations of hand; pp. 611–622. [Google Scholar]
- 2.Shanmuganathan N, et al. Aesthetic finger prosthesis. J Indian Prosthodont Soc. 2011;11(4):232–237. doi: 10.1007/s13191-011-0074-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lundborg G, Branemark PI, Rosen B. Osseointegrated thumb prostheses: a concept for fixation of digit prosthetic devices. J Hand Surg [Am] 1996;21:216–221. doi: 10.1016/S0363-5023(96)80103-1. [DOI] [PubMed] [Google Scholar]
- 4.Kamble VB, Desai RG, Arabbi KC, Mahajan K, Patil S (2013) Finger prostheses for multiple finger amputations: two case reports. Natl J Med Dent Res 1(2):38–42
- 5.Ozkan A, Senel B, Durmaz CE, Uyar HA, Evinc R. Use of dental implants to retain finger prostheses: a case report. OHDM. 2012;11(1):11–15. [PubMed] [Google Scholar]
- 6.Zollo L, Roccella S, Guglielmelli E, Carrozza MC, Dario P. Biomechatronic design and control of an anthropomorphic artificial hand for prosthetic and robotic applications. IEEE ASME Trans Mechatron. 2007;12(4):418–429. doi: 10.1109/TMECH.2007.901936. [DOI] [Google Scholar]
- 7.Baek SE, Lee SH, Chang JH (1999) Design and control of a robotic for prosthetic hands. In: Proceedings of the 1999 IEEE/RSJ. International conference on intelligent robots and systems
- 8.Doppen P, Solomons M, Kritzinger S. Osseointegrated Finger Prostheses. J Hand Surg Eur. 2009;34:29–34. doi: 10.1177/1753193408093807. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.