

Abstract
Background
Transverse sinus thrombosis can have nonspecific clinical and radiographic signs. We hypothesized that the novel “sigmoid notch sign” (on head CT) can help differentiate transverse sinus thrombosis from a congenitally atretic sinus among individuals with absent signal in one transverse sinus by magnetic resonance venography (MRV).
Methods
We retrospectively evaluated 53 subjects with a unilaterally absent transverse sinus signal on MRV. 11 had true transverse sinus thrombosis and 42 had an atretic transverse sinus. Reviewers were trained in the sigmoid notch sign: “positive” if one of the sigmoid notches was asymmetrically smaller than the other, consistent with a congenitally absent transverse sinus on that side. This sign was scored on CT scans by, two blinded reviewers to determine if signal dropout was clot or atretic sinus. A consensus rating was reached when the reviewers disagreed. Characteristics of the sigmoid notch sign as a diagnostic test were compared to a gold standard of full chart review by an independent reviewer.
Results
Each reviewer had a sensitivity of 91% (detecting 10/11 clots based on a negative sigmoid notch sign) and specificity of 71-81%; consensus specificity increased to 86% (36 of 42 individuals with an atretic sinus had a positive notch sign, detecting atretic sinuses based on presence of the sign).
Conclusion
Asymmetries of the sigmoid notches on non-contrast brain CT is a very sensitive and specific measure of differentiating transverse sinus thrombosis from an atretic transverse sinus when absence of transverse sinus flow is visualized on MRV.
Keywords: transverse sinus, venous sinus atresia, venous sinus occlusion, sigmoid notch sign
Thrombosis of the cerebral dural venous sinuses is an uncommon but potentially devastating cause of stroke, which has a predilection for women and the young. It occurs in 3-4 people per 1,000,000 population, and an estimated 86% of cases involve the transverse sinuses.1 The diagnosis of transverse sinus venous thrombosis, however, can be difficult to make given its nonspecific clinical signs and the lack of specificity of Magnetic Resonance Venograms (MRV) alone. 2 Autopsy and cerebral angiographic studies have consistently shown that a dominant transverse sinus is common, most commonly on the left.2,3,4 Only 37-50% of patients studied have equally sized transverse sinuses.2,3,4 In one study, 22% of normal subjects had one transverse sinus which did not opacify at all by conventional angiography.3 Therefore it is not uncommon to see dropout on MRV of one transverse sinus, suggesting occlusion due to thrombus, when congenital atresia may instead exist.
Standard non-contrast computed tomography (CT) of the brain can give a clue to whether a transverse sinus is occluded by clot. Narrowing of the sigmoid plate notch on CT can suggest congenital narrowing or sinus atresia, as opposed to clot as a cause of decreased flow.5 This asymmetry in sigmoid plate notches, however, has not been studied in any systematic way as a method to differentiate atretic from occluded sinuses. We hypothesized that, among individuals with absent signal of a transverse sinus on MRV, comparison of the sigmoid notches on non-contrast brain CT can differentiate transverse sinus clot from a congenitally atretic sinus.
METHODS
Patient Inclusion
The Johns Hopkins IRB approved this study. Subjects were selected based on either a sequential review of MRV scans from stroke inpatients or selection by ICD-9 codes after hospital discharge from Johns Hopkins Hospital or Johns Hopkins Bayview Medical Center from 2007-2010. The final data set consisted of individuals with absent signal on MRV in one of the transverse sinuses. We oversampled individuals with transverse sinus clot, so our sample does not represent the true prevalence of transverse sinus thrombosis.
A total of 53 patients were included in the study. A blinded investigator (RHL) reviewed all available historical, diagnostic, and imaging studies and then classified each subject as either having clot in the transverse sinus (n=11) or having an atretic sinus (n=43). This complete data review was considered the gold standard for adjudicating transverse sinus clot versus congenital sinus atresia.
A “positive” sigmoid notch sign was defined as an asymmetrically smaller sigmoid notch on the side of MRV loss of transverse sinus signal (Figure 1). A single slice of each subject’s brain CT scan at the level of the sigmoid plate with clear visualization of the bilateral sigmoid notches through which the transverse sinus runs (Figure 1) was selected and marked with the side of abnormal transverse sinus on MRV. The blinded neurologists adjudicated each CT as having a negative (consistent with transverse sinus thrombosis) or positive sigmoid notch sign (sigmoid sinus congenital atresia) on the side of MRV signal dropout. The blinded reviewers were not given access to any other imaging studies, and their assessment was entirely due to visual estimation from the image, but they could ask for an additional CT slice from the same scan if needed. In the case of disagreement, a consensus rating was made by the reviewers.
Figure 1. Sigmoid notch sign suggesting right transverse sinus clot.
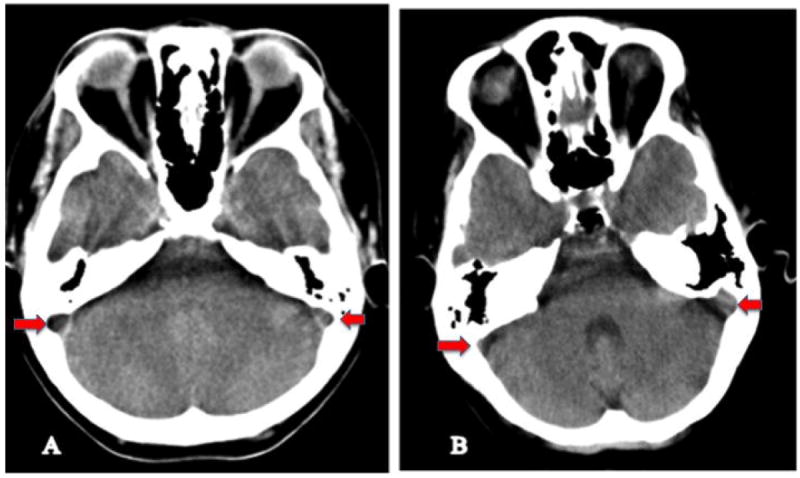
Both subjects A and B had right transverse sinus MRV dropout. Subject A has a negative sigmoid notch sign suggesting right transverse sinus clot. Subject B has a positive sigmoid notch sign (the right notch is smaller than the left) suggesting right atretic sinus. Arrows identify the sigmoid notches.
Inter-rater reliability was calculated using a kappa statistic. Sensitivity and specificity were calculated relative to the gold standard, as were false positive and negative rates. Secondary analyses repeated analyses for right versus left signal dropout.
RESULTS
Of the 53 subjects, 11 had venous clot and 42 had an atretic sinus by gold standard. Of the 11 subjects with clot, 1 subject had a right-sided clot and an atretic left transverse sinus. Another subject had both atresia and clot on the left. Seven of the 11 subjects with clot had right-sided clot. Overall MRV signal dropout was identified on the right for 19 (35.9%) of the 53 patients and the majority of atretic sinuses occurred on the left.
Each blinded neurologist had a sensitivity of 91% (detecting 10/11 clots based on a negative sigmoid notch sign). Specificity was 71% for one reviewer (identifying a positive sign in 30 of 42 atretic sinus cases) and 81% for the other (a positive sign in 34 of 42 cases). Cohen’s kappa was 0.60. The consensus sensitivity was 91% and specificity was 86%. The false positive rate was 14.3% (proportion of individuals with atretic sinus who had a negative sigmoid notch sign, suggesting presence of a thrombus), and the false negative rate was 9.1%.(Table 1). Sensitivity and specificity improved to 100% and 92%, respectively, in the 19 cases where MRV dropout was on the right side. (Table 2)
Table 1. Presence or absence of sigmoid notch sign on CT.
Distribution of films read as positive or negative sigmoid notch sign by gold standard diagnosis of transverse sinus thrombosis or congenitally atretic sinus.
| “Positive” sigmoid notch sign | “Negative” sigmoid notch sign | Total | Percent with “Positive” sign | 95% CI | Percent with “Negative” sign | 95% CI | |
|---|---|---|---|---|---|---|---|
| Transverse sinus thrombosis | 1 | 10 | 11 | 9.1% (FALSE NEGATIVE RATE) | -9.2%, 27.3% | 90.9% (SENSITIVITY) | 72.7%, 109.2% |
| Congenitally atretic sinus | 36 | 6 | 42 | 85.7% (SPECIFICITY) | 74.7%, 96.7% | 14.3% (FALSE POSITIVE RATE) | 3.3%, 25.3% |
Table 2. Sensitivity and specificity of absence of the sigmoid notch sign as predictor.
Sensitivity and specificity of sigmoid notch sign by side of MRV signal dropout.
| Sensitivity | Specificity | |
|---|---|---|
| MRV dropout left side (N=34) | 75% | 83% |
| MRV dropout right side(N=19) | 100% | 92% |
DISCUSSION
The diagnosis of cerebral sinus thrombosis can be difficult given its nonspecific clinical presentation. Due to the potential seriousness of this diagnosis, a screening tool that is both rapid and highly sensitive to the presence of venous clot is needed. MRV flow studies often overcall occlusion, and a congenitally atretic transverse sinus may appear identical in appearance to a transverse sinus thrombosis. Four-vessel cerebral angiography, the current gold standard in diagnosing thrombosis, can be time-consuming and carries potential risk.
The sigmoid notch sign, as described in this study, is a highly sensitive and specific measure of differentiating clot from atretic sinus when dropout of the transverse sinus is visualized on MRV. With the addition of the sigmoid notch sign on CT (which was likely already obtained, so is cost-effective) to the rest of the clinical presentation, an immediate decision can be made as to whether this is likely a clot requiring anticoagulation, or simply an atretic sinus. This technique can be used by specialist or nonspecialist neurologists.
This study is limited by our relatively small sample size, as true transverse clot thrombosis is a relatively rare finding. In addition, our gold standard was based on review of all available records, but in the majority of cases did not include cerebral angiography. However, we are confident that our final gold standard classifications were accurate since they were based on the entire set of brain MRI images and medical records available. In addition, although the number of patients with thrombosis was especially low, the sample used to calculate specificity is larger, with a narrower confidence interval. This allows a clinician to “rule out” a clot with fairly high confidence, if there is an asymmetrically smaller sigmoid notch on the same side as absent signal on an MRV.
The sigmoid notch sign, a simple and quick tool, is highly sensitive and specific. This makes it potentially useful to neurologists, in conjunction with clinical judgment, for diagnosis of transverse sinus venous thrombosis when dropout of flow is seen on MRV. Further studies are needed to evaluate its utility prospectively and in comparison with conventional angiography.
Acknowledgments
none
Sources of Funding
Dr. Gottesman is supported by the NIH (NINDS) RO1 AG040282-01.
Footnotes
Conflicts of Interest/Disclosures
None.
References
- 1.Stam J. Thombosis of the Cerebral Veins and Sinuses. NEJM. 2005;352:1791–1798. doi: 10.1056/NEJMra042354. [DOI] [PubMed] [Google Scholar]
- 2.Leach JL, Fortuna RB, Jones BV, Shipley G. Imaging of Cerebral Venous Thrombosis. Current Techniques, Spectrum of Findings, and Diagnostic Pitfalls RadioGraphics. 2006;26:S19–S43. doi: 10.1148/rg.26si055174. [DOI] [PubMed] [Google Scholar]
- 3.Morris L. Angiography of the superior sagittal and transverse sinuses. British Journal of Radiology. 1960;33:606–613. doi: 10.1259/0007-1285-33-394-606. [DOI] [PubMed] [Google Scholar]
- 4.Oka K, Rhonton LA, Barry M, Rodrequez R. Microsurgical anatomy of the Superficial veins of the Cerebrum. Neurosurgery. 1985;17(5):711–48. doi: 10.1227/00006123-198511000-00003. [DOI] [PubMed] [Google Scholar]
- 5.Connor EJ, Siddiqui MA, Stewart VR, O’Flynn EAM. The relationship of transverse sinus stenosis to bony groove dimensions provides an insight into the aetiology of idiopathic intracranial hypertension. Neuroradiology. 2008;50:999–1004. doi: 10.1007/s00234-008-0431-5. [DOI] [PubMed] [Google Scholar]