

Abstract
Purpose:
Gamma irradiated corneas in which the donor keratocytes and endothelial cells are eliminated are effective as corneal lamellar and glaucoma patch grafts. In addition, gamma irradiation causes collagen cross inking, which stiffens collagen fibrils. This study evaluated gamma irradiated corneas for use in corneal transplantations in a rabbit model comparing graft clarity, corneal neovascularization, and edema.
Methods:
Penetrating keratoplasty was performed on rabbits using four types of corneal grafts: Fresh cornea with endothelium, gamma irradiated cornea, cryopreserved cornea, and fresh cornea without endothelium. Slit lamp examination was performed at postoperative week (POW) one, two, and four. Corneal clarity, edema, and vascularization were graded. Confocal microscopy and histopathological evaluation were performed. A P < 0.05 was statistically significant.
Results:
For all postoperative examinations, the corneal clarity and edema were statistically significantly better in eyes that received fresh cornea with endothelium compared to the other three groups (P < 0.05). At POW 1, gamma irradiated cornea scored better than the cryopreserved and fresh cornea without endothelium groups in clarity (0.9 vs. 1.5 and 2.6, respectively), and edema (0.6 vs. 0.8 and 2.0, respectively). The gamma irradiated corneas, cryopreserved corneas and the fresh corneas without endothelium, developed haze and edema after POW 2. Gamma irradiated cornea remained statistically significantly clearer than cryopreserved and fresh cornea without endothelium during the observation period (P < 0.05). Histopathology indicated an absence of keratocytes in gamma irradiated cornea.
Conclusion:
Gamma irradiated corneas remained clearer and thinner than the cryopreserved cornea and fresh cornea without endothelium. However, this outcome is transient. Gamma irradiated corneas are useful for lamellar and patch grafts, but cannot be used for penetrating keratoplasty.
Keywords: Corneal Transplant, Gamma Irradiated Cornea, Sterile Cornea
INTRODUCTION
Corneal transplants are among the most commonly performed tissue transplants worldwide. Historically, penetrating keratoplasty (PK) was the most commonly used technique. PK is a well-established full thickness corneal transplant surgery. Recent advances in corneal transplant surgery allowed the development of additional lamellar corneal transplant techniques such as deep anterior lamellar keratoplasty and Descemets stripping automated endothelial keratoplasty. Unfortunately, the shortage of corneal tissue, coupled with the short shelf life (about 14 days) present serious limitations, especially in emergencies, rural areas, and developing countries. Furthermore, outside the United States, the demand for donor cornea is greater than the available supply.
Vision Graft Sterile Cornea®(VSC) (Tissue Banks International [TBI], Baltimore, Maryland), a gamma irradiated cornea, in which donor keratocytes and endothelial cells are removed, has been shown to be effective for corneal lamellar and glaucoma patch.1,2 Of the 108,000 donated corneas in the United States, approximately 40% are discarded for various reasons, including unhealthy endothelium.3 The tissues selected for gamma irradiation processing include grafts that are unsuitable for PK but have clear and uncompromised stroma. Hence, VSC can increase the supply of corneas suitable for transplantation in cases that do not require viable endothelium. In addition, irradiation prolongs the shelf life of the sterile cornea to more than a year at room temperature. Thus, it can be readily available for emergency procedures and in remote regions or developing countries. Finally, sterilization is beneficial in reducing the risk of transmission of bacterial or fungal infections from graft to host.4,5,6
Corneal collagen crosslinking (CXL) was introduced by Spoerl using a porcine eye.7 After promising basic science and animal studies, the technique was then performed as a treatment for keratoconus and corneal ectasia in humans.8,9 CXL treatment involves the use of ultraviolet A (UVA) light exposure after instillation of riboflavin onto the patient's cornea. CXL causes cross-linking of collagen fibrils, which strengthens the cornea and stabilizes the corneal shape.10,11 Recently, CXL has been attempted in cases of corneal infections and bullous keratopathy.12,13,14
In this study, we hypothesized that gamma irradiation to the donor cornea sterilizes and removes corneal keratocytes and endothelial cells and causes cross-linking of corneal collagen fibrils, which might keep the cornea more compact even without an endothelial pump. We performed PK in rabbit models using full thickness gamma irradiated corneas to evaluate the effect in vivo and to determine if it may serve as an alternative to fresh donor corneas.
METHODS
The experiment was performed according to The Association for Research in Vision and Ophthalmology and Johns Hopkins University Animal Care and Use Committee guidelines. Our experiment consisted of four groups comprised of 17 male New Zealand white rabbits that underwent PK in the right eye. The first control group received freshly harvested allogenic corneal grafts (a fresh cornea with endothelium group; n = 5). The second group received gamma irradiated cornea (n = 6). The third received cryopreserved cornea (n = 2). The fourth group received fresh grafts with the endothelium removed (fresh cornea without endothelium; n = 4). Frozen cornea was used as the control group because gamma irradiation is performed after freezing the tissue for VSC. Postoperative care consisted of topical gentamicin sulfate and prednisolone acetate ointment. Intramuscular buprenorphine was used for pain relief.
Graft preparation
Rabbit scleral rims were frozen in Optisol GS®(Bausch and Lomb, Rochester, New York) until they were irradiated at TBI. They were then stored in albumin at room temperature; this procedure is the same as that used to prepare human irradiated sterile corneas. Rabbit cryopreserved corneas were kept frozen in Optisol GS® at −80°C until the time of surgery. Fresh rabbit corneas were obtained before performing PK. For the fresh cornea without endothelium group, Descemets membrane was removed before trephination of the corneal button.
Penetrating keratoplasty procedure
Rabbits were anesthetized with an intramuscular injection of ketamine (50 mg/kg) and xylazine (10 mg/kg). Lidocaine eye drops were used for local anesthesia. The pupils were dilated with tropicamide and phenylephrine eye drops. Intracameral heparin was injected through a stab incision, and the anterior chamber was filled with viscoelastic. Trephination was performed with an 8 mm diameter biopsy punch and completed with corneal scissors. Donor grafts were prepared by using 8.5 mm punches. The donor grafts were sutured to the host bed with 10–0 nylon sutures. The viscoelastic material in the anterior chamber was removed.
Postoperative evaluation
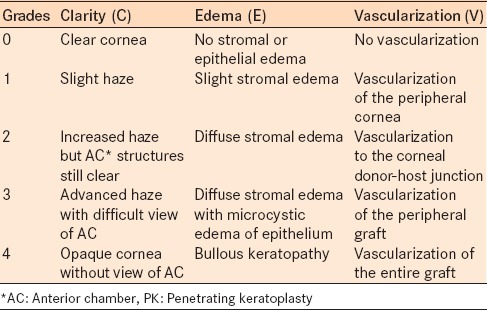
Slit lamp examination and photography was performed at postoperative week (POW) one, two, and four. Two examiners graded the transplanted cornea based on the modified Holland method at POW one, two, and four.15 Briefly, corneal clarity (C), edema (E), and vascularization (V) were scored on a 0–4 scale, in which smaller numbers indicated better results [Table 1]. The posterior surface of the graft was evaluated with confocal microscopy.
Table 1.
Slit lamp grading of corneal graft after PK in a rabbit model
Histological evaluation
Some rabbits were euthanized at POW 1 and POW 4 to evaluate the histology of the cornea. The enucleated eyes were fixed in 10% formalin. Hematoxylin and eosin staining was performed for evaluation of the stromal structure of each group.
Statistical analysis
Kruskal-Wallis rank tests were used to compare the baseline corneal clarity, edema, and vascularization among the four treatment groups. Generalized least squares models with an autoregressive correlation structure were used to compare clarity, edema, and vascularization collected over a 4-week period from the different treatment groups. The correlation structure is necessary to consider for correlation of repeated measures in the same eye. The models included time and indicator variables for the treatment effects as predictors. The models assumed the time effect to be the same in the four groups, and a linear relationship was assumed between the outcomes and time. Statistical significance in this study is reported as P values and 95% confidence intervals (CIs). A P < 0.05 was considered statistically significant. Analyses were performed using the SAS/STAT 9.2 (SAS Institute Inc. Cary, North Carolina).
RESULTS
Clinical observation
Clarity
Fresh grafts with endothelium remained clear throughout the observation period [Figures 1 and 2]. The fresh grafts with endothelium were statistically significantly clearer than gamma irradiated corneas (P = 0.0006), cryopreserved corneas (P < 0.0001), and the fresh corneas without endothelium (P < 0.0001) over the course of the 4 weeks.
Figure 1.

Slit lamp grading scores at postoperative week one, two, and four of four groups (fresh graft with endothelium, gamma irradiated cornea, cryopreserved cornea, and fresh graft without endothelium)
Figure 2.
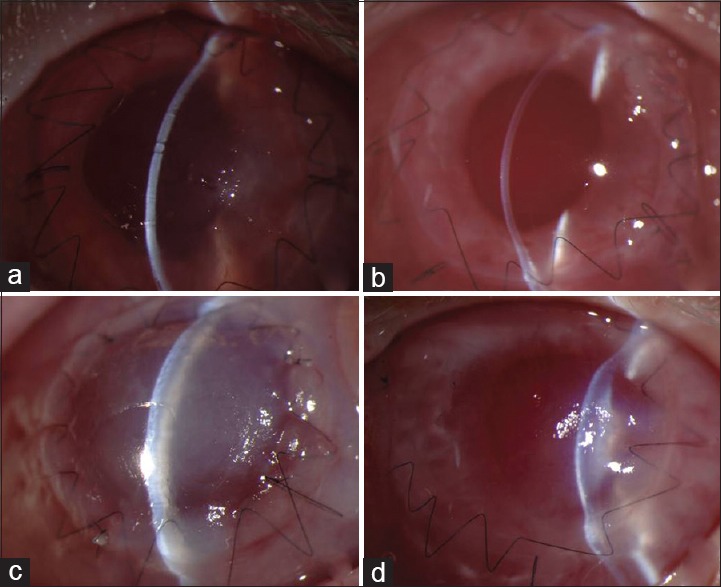
Postoperative week one slit lamp pictures of gamma irradiated cornea (a) fresh cornea with endothelium (b) fresh cornea without endothelium (c) and cryopreserved cornea (d) Note that while fresh graft with endothelium and gamma irradiated graft do not have edema, the other two without viable endothelium had corneal edema
Gamma irradiated corneas had mild haze at POW 1 which increased to moderate haze by POW 4. The other two groups (cryopreserved and fresh corneas without endothelium) showed moderate haze from the beginning, which progressed to significant haze by POW 4. The gamma irradiated corneas remained statistically significantly clearer than cryopreserved and fresh corneas without endothelium during the observation period (generalized least square model [P < 0.05]).
Edema
Fresh graft with endothelium did not have any significant edema during the 4-week observation period [Figure 1]. The fresh graft with endothelium was significantly thinner than the gamma irradiated cornea (P = 0.04), the cryopreserved (P = 0.005), and the fresh cornea without endothelium (P = 0.003) groups over the course of the 4 weeks.
Gamma irradiated corneas had minimal edema at POW 1 that increased to moderate stromal edema by POW 4. The cryopreserved cornea showed mild edema at POW 1 that progressed to severe edema by POW 4. The fresh cornea without endothelium had mild edema at POW 1 that progressed to moderate edema by POW 4. The gamma irradiated corneas were less edematous than cryopreserved and fresh corneas without endothelium, but this was not statistically significant (P = 0.08 and P = 0.15, respectively).
Neovascularization
All grafts had minimal neovascularization at POW 1. The neovascularization scores increased over time in all four groups [Figure 1]. The gamma irradiated corneas had less neovascularization than the fresh corneas with endothelium (P = 0.18), the cryopreserved cornea (P = 0.3), and the fresh cornea without endothelium (P = 0.2) for the duration this study.
Confocal microscopy
Confocal images indicated healthy, well-demarcated endothelial cells in the fresh cornea with endothelium group at POW 1 to POW 4. There were no hexagonal endothelial cells in the other groups including the irradiated corneas at any point in this study (data not shown). No regrowth of the endothelium was observed in these groups during the observation period.
Histological analysis
Hematoxylin and eosin staining of the grafts at POW 1 showed keratocytes in the fresh cornea with endothelium, the fresh cornea without endothelium and the cryopreserved cornea [Figure 3]. There were no keratocytes in the gamma irradiated corneas. The stromal structure of the fresh corneas with endothelium and gamma irradiated corneas were organized while the other two had vacuoles between the collagen layers indicating stromal edema. Endothelial cells were observed in the fresh cornea with endothelium, as well as the cryopreserved corneas, but not in the gamma irradiated or the fresh corneas without endothelium.
Figure 3.
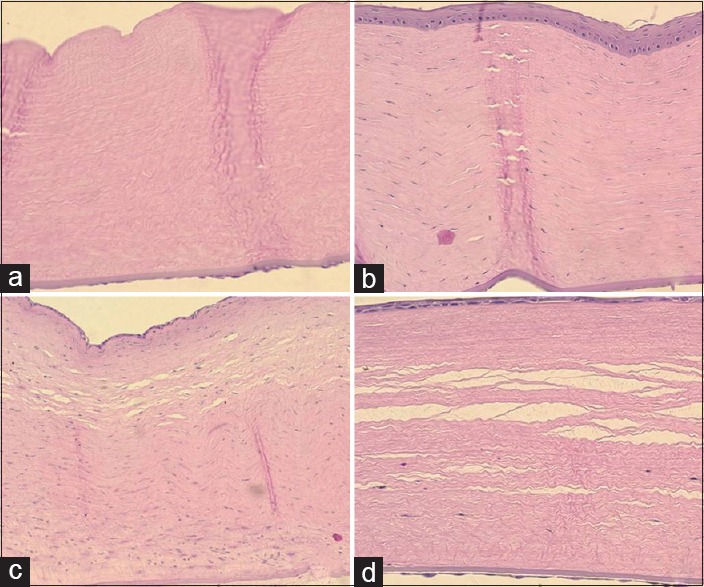
Hematoxylin and eosin staining of gamma irradiated cornea (a) fresh cornea with endothelium (b) fresh cornea without endothelium (c) and cryopreserved cornea (d) at postoperative week one
DISCUSSION
Gamma irradiated corneal grafts had reduced allogenicity,16 potentially supporting their use in procedures that do not require viable endothelium. VSC can have potential applications for procedures such as corneal patch grafts and anterior lamellar keratoplasty,1 donor corneal rims for the Boston II keratoprosthesis,17 and patch grafts for glaucoma drainage device.2 In addition, the cross-linking of collagen fibrils in gamma-irradiated corneas led us to postulate they will perform better than cryopreserved or fresh corneas without endothelium in PK.
We found that among the grafts without viable endothelium, gamma irradiated corneas remained clearer compared to the cryopreserved (P = 0.02) and the fresh graft without endothelium (P = 0.04). Although the gamma irradiated corneas remained thinner than the other two groups, this was not statistically significant (P > 0.05 all comparisons).
Rabbit endothelial cells proliferate in vivo.18 However, in our study, histopathology and confocal microscopy indicated no evidence of regrowth of endothelium in any of our grafts over 4 weeks follow-up. Despite the lack of endothelial cells, the gamma irradiated cornea stayed clear and thin suggesting the effect of gamma irradiation on stromal stiffening.
The evaluation of crosslinking due to gamma irradiation on the cornea is a nascent area of study. However, electron microscopy has demonstrated that the interfibrillar distance in the anterior stroma of irradiated cornea was significantly lower than non-irradiated controls.19 We know that oxidation is an underlying mechanism for cross-linking collagen.10 As radiation causes oxidation, collagen fibrils in the irradiated sterile cornea may be cross-linked as well. Thus, our findings may not be explained by cryopreservation or endothelial regeneration, but possibly, by the effect of gamma irradiation.
Previous studies found that CXL only transiently improved corneal thickness and transparency in eyes with bullous keratopathy.14 The transient strength of the stroma was improved upon in our study. However, we also found the stromal strength was limited, and over the course of a month, the anti-edematous effect was insufficient to keep the stroma thin, clear, and dehydrated. Hence, gamma irradiation may not be a replacement for viable endothelium.
The mechanism and the treatment of corneal neovascularization have been studied extensively.20,21,22 Neovascularization is a known risk factor in many cases of graft rejection after PK.23 In addition, to improving clarity and edema, the sterile cornea may have decreased angiogenesis properties. Maurice showed that corneal edema is necessary for the growth of vessels into the cornea.24 Our study demonstrated that gamma irradiation stiffened the corneal stroma. Thus, the irradiated graft's resistance to corneal edema theoretically blocks new vessel invasion into the corneal stroma, which could prevent secondary problems such as graft rejection and lipid deposition. In the current study, the new vessels in the cornea did not reach to the grafts while the gamma irradiated cornea was still thin. Hence, we cannot confirm this theory in this study.
Histopathological examination of gamma irradiated cornea demonstrated the absence of keratocytes. This is consistent with previous studies with electron microscopy.19 In addition, to the effect of reduced edema, decellularization of the cornea itself can prevent an immunogenic reaction1 and thus, neovascularization as well.
The major limitation of this study is the small sample size. Although our study, showed encouraging results with gamma-irradiated corneas compared to other preserved corneas, the statistical power was weak. Perhaps a larger sample size is required. In addition, the reduced antigenicity of irradiated corneas requires further study.
In conclusion, gamma irradiated corneas were superior to other preserved corneas in vivo for an animal model in terms of resisting corneal haze. However, the gamma irradiated cornea is an unsuitable alternative to fresh donor cornea for a PK graft. Gamma irradiated corneas may be better candidates for patch grafts and anterior lamellar transplants.
ACKNOWLEDGMENT
Tissue Banks International.
Footnotes
Financial support and sponsorship Tissue Banks International.
Conflicts of interest There are no conflicts of interest.
REFERENCES
- 1.Utine CA, Tzu JH, Akpek EK. Lamellar keratoplasty using gamma-irradiated corneal lenticules. Am J Ophthalmol. 2011;151:170–4e.1. doi: 10.1016/j.ajo.2010.08.007. [DOI] [PubMed] [Google Scholar]
- 2.Daoud YJ, Smith R, Smith T, Akpek EK, Ward DE, Stark WJ. The intraoperative impression and postoperative outcomes of gamma-irradiated corneas in corneal and glaucoma patch surgery. Cornea. 2011;30:1387–91. doi: 10.1097/ICO.0b013e31821c9c09. [DOI] [PubMed] [Google Scholar]
- 3.Eye Bank Association of America. 2009 Eye Banking Statistical Report 2009 Eye Banking Statistical Report. [Last accessed on 2012 Dec 03; Last updated on 2015 Jun 01]. Available from: http://www.corneas.org/repository/images/pressimages/EBAA%202009%20Statistical%20Report%20.%20Final.pdf .
- 4.Jambulingam M, Parameswaran SK, Lysa S, Selvaraj M, Madhavan HN. A study on the incidence, microbiological analysis and investigations on the source of infection of postoperative infectious endophthalmitis in a tertiary care ophthalmic hospital: An 8-year study. Indian J Ophthalmol. 2010;58:297–302. doi: 10.4103/0301-4738.64132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Keyhani K, Seedor JA, Shah MK, Terraciano AJ, Ritterband DC. The incidence of fungal keratitis and endophthalmitis following penetrating keratoplasty. Cornea. 2005;24:288–91. doi: 10.1097/01.ico..0000138832.3486.70. [DOI] [PubMed] [Google Scholar]
- 6.Kloess PM, Stulting RD, Waring GO, 3rd, Wilson LA. Bacterial and fungal endophthalmitis after penetrating keratoplasty. Am J Ophthalmol. 1993;115:309–16. doi: 10.1016/s0002-9394(14)73580-9. [DOI] [PubMed] [Google Scholar]
- 7.Spoerl E, Huhle M, Seiler T. Induction of cross-links in corneal tissue. Exp Eye Res. 1998;66:97–103. doi: 10.1006/exer.1997.0410. [DOI] [PubMed] [Google Scholar]
- 8.Wollensak G. Crosslinking treatment of progressive keratoconus: New hope. Curr Opin Ophthalmol. 2006;17:356–60. doi: 10.1097/01.icu.0000233954.86723.25. [DOI] [PubMed] [Google Scholar]
- 9.Caporossi A, Baiocchi S, Mazzotta C, Traversi C, Caporossi T. Parasurgical therapy for keratoconus by riboflavin-ultraviolet type A rays induced cross-linking of corneal collagen: Preliminary refractive results in an Italian study. J Cataract Refract Surg. 2006;32:837–45. doi: 10.1016/j.jcrs.2006.01.091. [DOI] [PubMed] [Google Scholar]
- 10.Ashwin PT, McDonnell PJ. Collagen cross-linkage: A comprehensive review and directions for future research. Br J Ophthalmol. 2010;94:965–70. doi: 10.1136/bjo.2009.164228. [DOI] [PubMed] [Google Scholar]
- 11.Snibson GR. Collagen cross-linking: A new treatment paradigm in corneal disease-a review. Clin Experiment Ophthalmol. 2010;38:141–53. doi: 10.1111/j.1442-9071.2010.02228.x. [DOI] [PubMed] [Google Scholar]
- 12.Wollensak G, Aurich H, Wirbelauer C, Pham DT. Potential use of riboflavin/UVA cross-linking in bullous keratopathy. Ophthalmic Res. 2009;41:114–7. doi: 10.1159/000187630. [DOI] [PubMed] [Google Scholar]
- 13.Ehlers N, Hjortdal J, Nielsen K, Søndergaard A. Riboflavin-UVA treatment in the management of edema and nonhealing ulcers of the cornea. J Refract Surg. 2009;25:S803–6. doi: 10.3928/1081597X-20090813-08. [DOI] [PubMed] [Google Scholar]
- 14.Ghanem RC, Santhiago MR, Berti TB, Thomaz S, Netto MV. Collagen crosslinking with riboflavin and ultraviolet-A in eyes with pseudophakic bullous keratopathy. J Cataract Refract Surg. 2010;36:273–6. doi: 10.1016/j.jcrs.2009.07.041. [DOI] [PubMed] [Google Scholar]
- 15.Holland EJ, Chan CC, Wetzig RP, Palestine AG, Nussenblatt RB. Clinical and immunohistologic studies of corneal rejection in the rat penetrating keratoplasty model. Cornea. 1991;10:374–80. doi: 10.1097/00003226-199109000-00003. [DOI] [PubMed] [Google Scholar]
- 16.Stevenson W, Cheng SF, Emami-Naeini P, Hua J, Paschalis EI, Dana R, et al. Gamma-irradiation reduces the allogenicity of donor corneas. Invest Ophthalmol Vis Sci. 2012;53:7151–8. doi: 10.1167/iovs.12-9609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Akpek EK, Aldave AJ, Aquavella JV. The use of precut, γ-irradiated corneal lenticules in Boston type 1 keratoprosthesis implantation. Am J Ophthalmol. 2012;154:495–4981. doi: 10.1016/j.ajo.2012.03.022. [DOI] [PubMed] [Google Scholar]
- 18.Van Horn DL, Sendele DD, Seideman S, Buco PJ. Regenerative capacity of the corneal endothelium in rabbit and cat. Invest Ophthalmol Vis Sci. 1977;16:597–613. [PubMed] [Google Scholar]
- 19.Sikder S, McCally RL, Engler C, Ward D, Jun A. Evaluation of irradiated corneas using scatterometry and light and electron microscopy. Cornea. 2011;30:503–7. doi: 10.1097/ICO.0b013e3181eadd0f. [DOI] [PubMed] [Google Scholar]
- 20.Joussen AM, Poulaki V, Mitsiades N, Stechschulte SU, Kirchhof B, Dartt DA, et al. VEGF-dependent conjunctivalization of the corneal surface. Invest Ophthalmol Vis Sci. 2003;44:117–23. doi: 10.1167/iovs.01-1277. [DOI] [PubMed] [Google Scholar]
- 21.Usui T, Ishida S, Yamashiro K, Kaji Y, Poulaki V, Moore J, et al. VEGF164 (165) as the pathological isoform: Differential leukocyte and endothelial responses through VEGFR1 and VEGFR2. Invest Ophthalmol Vis Sci. 2004;45:368–74. doi: 10.1167/iovs.03-0106. [DOI] [PubMed] [Google Scholar]
- 22.Chen WL, Lin CT, Lin NT, Tu IH, Li JW, Chow LP, et al. Subconjunctival injection of bevacizumab (avastin) on corneal neovascularization in different rabbit models of corneal angiogenesis. Invest Ophthalmol Vis Sci. 2009;50:1659–65. doi: 10.1167/iovs.08-1997. [DOI] [PubMed] [Google Scholar]
- 23.Bachmann B, Taylor RS, Cursiefen C. Corneal neovascularization as a risk factor for graft failure and rejection after keratoplasty: An evidence-based meta-analysis. Ophthalmology. 2010;117:1300–5.e7. doi: 10.1016/j.ophtha.2010.01.039. [DOI] [PubMed] [Google Scholar]
- 24.Maurice DM, Zauberman H, Michaelson IC. The stimulus to neovascularization in the cornea. Exp Eye Res. 1966;5:168–84. doi: 10.1016/s0014-4835(66)80004-0. [DOI] [PubMed] [Google Scholar]