

Abstract
Background
Many countries continue to have high fertility rates and most of the predicted increase in the world’s population until 2100 comes from these countries. Among family planning methods, Long Acting and Permanent Methods are convenient for users and effectively prevent pregnancy. The objective of this study was to assess factors associated with unmet need of Long Acting and Permanent Methods of contraception among women in the reproductive age group (15-49) using contraception in health facilities of Shashemene town, Oromia Region, Ethiopia.
Methods
Facility based cross sectional quantitative study and stratified sampling technique was used. Total of 382 females in reproductive age group were enrolled in the study in January 2012. Pretested, structured and close-ended questionnaire was used to interview study participants. Collected data was entered by using EPI Info 17 and analyzed by SPSS version 20 statistical software.
Results
Utilization of Long Acting and Permanent Methods (LAPMs) of contraception in Shashemene town was found to be 28.4 % (104/366). From study participants, 71.6 % (262/366) used short acting methods and from these current short acting users, 127(41.5 %) desired to use LAPMs and unmet need of LAPMs was 122(33.3 %). Factors significantly associated with unmet need of LAMPs of contraception were: Education of women (< secondary level) AOR [3.8, 95 % CI: 2.9, 7.6; P < 0.001]; lack of discussion between partners AOR [2.9, 95 % CI: 1.8, 9.6; P = 0.01]; lack of proper counseling for women AOR [5.3, 95 % CI: 1.7, 11.2; P = 0.04]; and women’s occupation as a housewife AOR [4.7, 95 % CI: 3.1, 11.3; P = 0.02].
Conclusion
Unmet need of LAPMs of contraception in health facilities in Shashemene town was high. Women education, partner discussion and proper client counseling were found the main factors associated women LAPMs utilization.
Keywords: Long Acting and Permanent Methods (LAPMs), unmet need of LAPMs & Family planning
Background
Four contraceptive methods are categorized as long-acting and permanent (LAPMs): intrauterine contraceptive devices (IUCDs), implants, female sterilization, and vasectomy. IUCDs and implants are long acting temporary methods; when removed, return to fertility is prompt. Copper-containing IUCDs, the ones generally available in African Ministry of Health (MoH) family planning programs, is effective for at least 12 years, although it is labeled for 10 years. Implants, depending on the type, last for up to three to seven years. Female sterilization or tubal ligation and vasectomy are permanent methods [1].
Unmet need for family planning is defined as percentage of all fecund women who are married or living in union and thus presumed to be sexually active but are not using any method of contraception, either do not want to have more children or want to postpone their next birth for at least two more years or do not know when or if they want another child. The concept of unmet need points to the gap between women’s reproductive intentions and their contraceptive behavior [2, 3].
In developing countries, 20 to 30 % of women who use oral contraceptives or injectable stop within two years of starting because of side effects or other health concerns. Many of these women could benefit from switching to LAPMs [4]. Many countries continue to have high fertility rates and most of the predicted increase in the world’s population until 2100 comes from these high-fertility countries [5]. Ethiopia’s Reproductive Health Strategy (2006–2015) identifies priority areas to improve the reproductive health status of this country and fertility & family planning is one of the six strategies [6].
Ethiopia is a second populous country in Africa with a total population of 90,076,000 [7, 8]. The prevalence rates of contraceptives (CPRs) were 8.1 %, 14.7 % and 29 % in 2000, 2005 and 2011 respectively, while the unmet needs for family planning during the same periods were reported as 36 %, 34 % and 29 % respectively [9, 10]. Even though, LAPMs are effective and convenient method of pregnancy prevention for users, the prevalence of LAPMs remains relatively small with only accounts of 3.9 % (EDHS 2011) and sometimes missing component of national reproductive health and family planning programs [10, 11].
Evidence from studies in South East of and North West of Ethiopia shows unmet need for LAPMs was 9.4 % and 16.4 %, respectively [12, 13]. Data from Ethiopian demographic and health survey shows unmet need for married women to be 25 %, met need 29 % and the total demand 53.9 % and the prevalence of LAPMs of FP services in whole Ethiopia is about 3.9 %. But in Oromia, unmet need for modern FP 29.9 %, met need for modern FP 26.2 % and the total demand for modern FP 56.1 % and the prevalence of LAPMs of family planning services in Oromia Region is about 6 % [9]. According to Shashemene town health office report of 2011, the FP service coverage was 92 % but no clear data about the prevalence of LAPMs [14]. Therefore, this study intended to assess the extent of unmet need for LAPMs and contribute factors associated with unmet need of LAPMs of FP services in Shashemene town.
Methods
The study was conducted in Shashemene town of West Arsi zone, Oromia National Regional state, which is located around 240 Km from Addis Ababa (capital city) to the south of Ethiopia. Shashemene town has a total population of 140,717 of which 70,339 are women and women of childbearing age group expected to be 15,566 [8]. At the time of the study, there were 16 health institutions providing modern family planning to the community: 13 public health institution, 2 NGO clinics and one private medium clinic. The study area is selected due to the non exixtence of clear data on met and unmet need of LAPMs in the town.
Facility based cross sectional quantitative study was conducted in January and February, 2012, to determine the extent of unmet need of LAPMs of family planning services among women in the reproductive age group using modern family planning in the health facilities
The sample size was calculated for the unmet need of LAPMs (using single proportion formula) and factors associated with unmet need of LAPMs (double proportion formula). And the sample size of extent of unmet need of LAPMs was higher than factors associated with unmet need of LAPMs, we use sample size of extent of unmet need of LAPMs: n = 382.
Assumptions
Desired precision/margin of error (d) = 3.75 %, the prevalence of unmet needs of LAPMs in Oromia Region (p) was about 15 % and CI = 95 %, which means α set at 0.05 and Ζ α/2 = 1.96 (value of Ζ at α 0.05 or critical value for normal distribution at 95 % CI) by calculating with Epi Info 7 statcalc. Hence, the calculated sample size was found to be 348 + 10 % (non-response rate) = 382.
In Shashemene town there were 8 health facilities (by excluding 8 health posts because of non- fixed facility) providing modern FP services. A stratified sampling was used by dividing 8 health facilities in to strata: 4 health facilities with high client flow and 4 health facilities with low client flow. A separate sample was taken independently from each stratum by using simple random sampling. Thus, 3 health facilities out of 4 health facilities with high client flow and 3 health facilities out of 4 health facilities with low client flow were selected. Record review indicating how many clients received modern family planning services in the last 4 completed quarters (12 months) was made in each stratum, and then proportional allocation was used for each stratum to select study subjects.
Data was collected continuously by exit interview from study subjects who came for modern family planning within the study period in 6 selected health facilities until the required sample size was obtained according to their proportional size. The questionnaire was adapted from other studies developed for similar purposes [15, 16] and some adjustment was made to suit the local condition and study objective.
The study data were collected, checked, edited for consistency, processed and analyzed generally by means of a package computer program: statistical soft-wares: EPI Info 7 for data entry format designing, data entry, data cleaning and data processing/management; and SPSS 20 used for data analysis. The cut point that was used for statistical significance was the P- value 0.05.
Ethical considerations
Ethical clearance was obtained from Hawassa University and Addis Continental Institution of Public Health. Official permission was collected from Shashemene town Health Department, and both written informed consent and verbal was obtained from individual participants. All study participants in the survey were told about their participation was voluntary and confidential.
Operational definition of key words in unmet need of LAPMs is given below:
Unmet need for LAPMs of Contraceptive: - A condition of wanting to postpone or avoid pregnancy but not using any of the LAPMs of contraceptive or using short acting contraceptive but do not wants to use the method that they were using.
Short acting contraceptive: - Pills, injectable hormones and condoms.
Long acting contraceptive: - Intra-Uterine Contraceptive Device (IUCD) and Implants.
Permanent methods of contraceptive: - Tubal ligation and vasectomy. However, vasectomy not belongs to this operational definition since no male participated.
Unmet need for limiting: - When women who do not want any more children, but not using any of LAPMs of contraceptive.
Unmet need for spacing:- When a woman who does not want to have pregnancy soon after delivery or want to space for two years but not using any of LAPMs of contraceptive.
Results
Socio-demographic characteristics of the respondents
A total of 382 study subjects were participated in the survey. The mean age of the respondents was 29.6 ± 7.8 S.D and the median age was 28 years ranging from 15-46 years. The highest proportion of the respondents 301/382 (78.8 %) were in the age group 15–34 years. Almost all 366 (95.8 %) of the respondents were married and living together. Majority of the respondents 376 (98.4 %) were residing in urban areas. About 91 (23.8 %) of respondents had no education at all; while the remaining 291 (76.2 %) attended school ranging from primary to secondary and above. The predominant ethnic group of the respondents was Oromo 49.2 % (188) followed by Amhara 42.4 % (162). The religion of most respondents was Orthodox, 39.8 % (152), followed by Muslim 32.5 % (124). The occupation of respondents was 33 % (126) house wife followed by government employee 19.7 % (75). The monthly income of the majority of the respondents 55.2 % (211) was 1,500-3,499 ETB followed by 31.9 % (122) was <1500 ETB (Table 1).
Table 1.
Socio-demographic characteristics among women in the reproductive age group (15-49) using contraception in health facilities in Shashemene town, West Arsi Zone, Oromia Region, 2012 (n = 382)
| Characteristics | Number | Percent |
|---|---|---|
| Age Group (years) | ||
| <25 | 154 | 40.3 |
| 25-34 | 147 | 38.5 |
| > = 35 | 81 | 21.2 |
| Mean ± SD for women15-49 years. =29.6 ± 7.8 and Median age for women15-49 years. =28 years. | ||
| Marital status | ||
| Single | 9 | 2.4 |
| Married | 366 | 95.8 |
| Separated | 6 | 1.6 |
| Divorced | 1 | 0.26 |
| Residence | ||
| Town | 376 | 98.4 |
| Rural | 6 | 1.6 |
| Education | ||
| Illiterate | 91 | 23.8 |
| Primary (1–8) | 110 | 28.8 |
| Secondary (9-10) and above | 181 | 47.4 |
| Ethnicity | ||
| Amhara | 162 | 42.4 |
| Oromo | 188 | 49.2 |
| Othersa | 32 | 8.4 |
| Religion | ||
| Orthodox | 152 | 39.8 |
| Muslim | 124 | 32.5 |
| Protestant | 106 | 27.7 |
| Occupation | ||
| House wife | 126 | 33 |
| Government employee | 75 | 19.7 |
| Daily laborer | 23 | 6 |
| Student | 52 | 13.6 |
| Merchant | 96 | 25.1 |
| Othersb | 10 | 2.6 |
| Income | ||
| <1500 | 122 | 31.9 |
| 1500-3499 | 211 | 55.2 |
| > = 3500 | 49 | 12 |
a = Wolaita, Kambata, Hadiya; b = Tella (local alcohol drink) Sellers/self-employee
The mean age of women at marriage and first delivery was 18.02 ± 2.4 SD and 19.6 ± 2.6 SD years respectively. The average number of pregnancies was 2.57 ± 0.8 SD, out of which, 59.9 % (217/362) experienced three and above pregnancy. Two hundred one (64.8 %) of the women aged 15-49 years responded that they want to have any more children in the future, of which one hundred thirty-one (65.2 %) seek 1-3 children in their life time. Most women one hundred seventy-two (85.6 %) want to have any more children after two years and above. Forty five (12.3 %) of the women aged 15-49 years had abortion, of which 10 (22.2 %) experienced more than one induced abortion in their life time. The average number of children in the household was 1.35 (SD = 0.7) (Table 2).
Table 2.
Reproductive History among women in the reproductive age group (15-49) using contraception in health facilities in Shashemene town, West Arsi Zone, Oromia Region, 2012
| Characteristics | Number | Percent |
|---|---|---|
| Age at marriage (n = 366) | ||
| <18 | 190 | 51.9 |
| ≥18 | 176 | 48.1 |
| Age at delivery (n = 317) | ||
| <18 | 44 | 13.9 |
| ≥18 | 273 | 86.1 |
| Number of pregnancy (n = 362) | ||
| One/two | 145 | 40.1 |
| Three/four | 112 | 30.9 |
| Five or more | 105 | 29.0 |
| Number of living children (n = 310) | ||
| One/two | 133 | 42.9 |
| Three/four | 95 | 30.6 |
| Four or more | 82 | 26.5 |
| Do you want to have any more children? (n = 310) | ||
| Yes | 201 | 64.8 |
| No | 109 | 35.2 |
| Ideal number of children you want (n = 201) | ||
| 1-3 | 131 | 65.2 |
| 4 or more | 45 | 22.4 |
| Depend on God | 2 | 1.0 |
| Depend on husband | 23 | 11.4 |
| When you want to have any more children? (n = 201) | ||
| Less than two years | 29 | 14.4 |
| Two years and above | 172 | 85.6 |
| Number of abortion (n = 45) | ||
| One | 35 | 77.8 |
| Two and above | 10 | 22.2 |
Unmet need of LAPMs
Further analysis carried out on the married respondents of 366 women. The current utilization rate of LAPMs of contraceptives in the town was 104 (28.4 %). Of these 88 (24 %) were using Implants, 15 (4.1 %) IUCD and 1 woman (0.3 %) were using Tubal ligation (Fig. 1). Two hundred sixty two (71.6 %) of the respondents were using short acting contraceptives mainly Depo-Provera 212 (57.9 %); and pills 50 (13.7 %). Out of these short acting contraceptive users 135 (51.5 %) were preferred to use the method and 127 (41.5 %) of these current short acting contraceptive users did not want to use the method that they were using (Table 4).
Fig. 1.
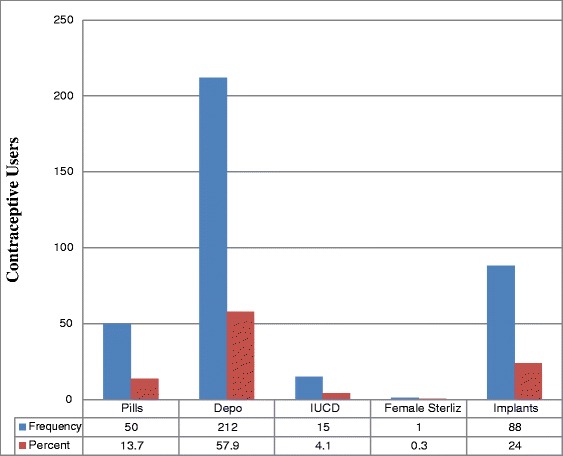
Contraceptive Methods Currently in Use among Women in Reproductive Age Group (15-49) in Health Facilities in Shashemene Town, West Arsi Zone, Oromia Region, 2012
Table 4.
Percentage of methods preferred & reasons for not using LAPMs among women in the reproductive age group (15-49) in Shashemene town, West Arsi Zone, Oromia Region, 2012
| Characteristics | Number | Percent |
|---|---|---|
| Currently used Short Acting Method preferred n = 262 | ||
| Yes | 135 | 51.5 |
| No | 127 | 48.5 |
| What LAPM was wanted? n = 127 | ||
| IUD | 27 | 21.3 |
| Implants | 95 | 74.8 |
| Tubal ligation | 5 | 3.9 |
| Reason for not using IUD n = 27 | ||
| Previously used methods inconvenient | 4 | 14.8 |
| Proven health problem | 2 | 7.4 |
| Fear of complication | 15 | 55.6 |
| Partner/husband opposed | 6 | 22.2 |
| Reason for not using Implant = 95 | ||
| Previously used methods inconvenient | 10 | 10.5 |
| proven health problem | 4 | 4.2 |
| Fear of complications | 51 | 53.7 |
| Partner/husband opposed | 30 | 31.6 |
| Reason for not tubal ligation n = 5 | ||
| Proven health problem | 1 | 20.0 |
| Fear of complications | 3 | 60.0 |
| Partner/husband opposed | 1 | 20.0 |
The total unmet need of LAPMs of contraceptives in health facilities in the town was found to be 122 (33.3 %) of which seventy-nine (21.6 %) for spacing and forty-three (11.7 %) for limiting (Fig. 2).
Fig. 2.
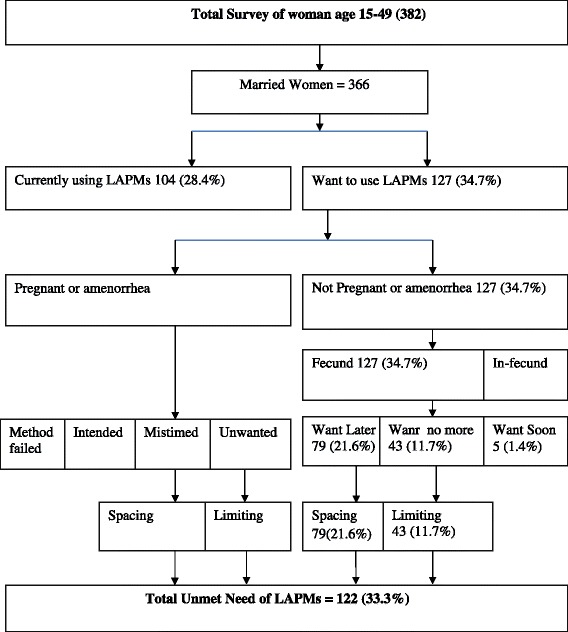
Unmet Need of LAPMs among Women in The Reproductive Age Group (15-49) Using Contraception in Health Facilities in Shashemene Town, West Arsi Zone, Oromia Region, 2012 (Westoff Model)
Associated factors and unmet need of LAPMs
Most of the respondents (85 %) heard about LAPMs of contraceptives at least once. From which 362 (98.9 %) heard about implants as LAPMs of contraceptive and the least ever heard LAPMs of contraception was Tubal-ligation 220 (60.1 %). Less than one-fourth 82 (22.4 %) of the respondents were counseled about LAPMs of contraception by health professionals. Nearly all 355 (97 %) reported, knew the source of LAPMs of contraceptives were found in health facilities in the town. Three hundred twenty four (88.6 %) have heard of LAPMs from Hospital sources. Media (radio and television) was the major sources of information 322 (88 %). In the past few months only 146 (39.9 %) respondents discussed about LAPMs once/twice and 41 (11.2 %) respondents discussed about LAPMs more often with their husband/partner. One hundred seventy nine (48.9 %) of the respondents had never discussed about LAPMs of contraceptives with their husband/partner. One hundred ninety eight (54.1 %) of the respondents responded that their husband/partner opposes using LAPMs, while 192 (41.8 %) of the respondents responded their husband/partner approves using LAPMs. The decision of using LAPMs of contraceptive was made by both partners together for 235 (64.2 %) of the respondents (Table 3).
Table 3.
Percentage of ever heard, LAPMs counseling, Knowledge of source, discussion with husband and source of information of LAPMs among women in the reproductive age group (15-49) in Shashemene town, West Arsi Zone, Oromia Region, 2012 (n = 366)
| Characteristics | Number | Percent |
|---|---|---|
| Ever heard at least LAPMs | ||
| IUCD | 355 | 97.0 |
| Implants | 362 | 98.9 |
| Tubal-ligation | 220 | 60.1 |
| Women’s reports of whether counseled or not | ||
| Yes | 82 | 22.4 |
| No | 284 | 77.6 |
| Knows source of LAPMs | ||
| Yes | 355 | 97.0 |
| No | 11 | 3.0 |
| Mentioned sources LAPMs | ||
| Hospital | 324 | 88.6 |
| Health Center | 18 | 4.9 |
| Clinic | 14 | 3.8 |
| Private Health facilities | 10 | 2.7 |
| Heard information of LAPMs | ||
| Yes | 361 | 98.6 |
| No | 5 | 1.4 |
| Source of information of LAPMs | ||
| Radio | 170 | 46.5 |
| Television | 152 | 41.5 |
| News Paper | 18 | 4.9 |
| Pamphlet | 20 | 5.5 |
| Health personnel | 6 | 1.6 |
| Discussed with husband on LAPMs | ||
| Not at all | 179 | 48.9 |
| Once/twice | 146 | 39.9 |
| More often | 41 | 11.2 |
| Husband attitude to LAPMs | ||
| Approves | 153 | 41.8 |
| Opposes | 198 | 54.1 |
| Don’t know | 15 | 4.1 |
| Main decider on using LAPMs | ||
| Self- | 111 | 30.3 |
| Husband | 20 | 5.5 |
| Both decide together | 235 | 64.2 |
Among current short acting contraceptive users, 127 (34.7 %) desired to use LAPMs of contraceptives. From those who desired to use LAPMs 95 (74.6 %) desired to use Implants. For more than half, 51 (53.7 %) of the non-users of Implants the reason for not using Implant was fear of complications. Fear of complications was not only the reason for not using Implant but also for IUCD’s and Tubal ligation. For those who desired to use LAPMs of contraception, but are not using the methods, their reasons for husband/partner opposition, previous method inconvenient and proven health problems (Table 4).
Education of women was found to be an associated factors of unmet need of LAPMs of contraception, respondents who had less than secondary levels of education were found about four times more likely to have had unmet need of LAPMs of contraception than those respondents who had secondary and above levels of education AOR [3.8, 95 % CI: 2.9, 7.6; P < 0.001]. Women’s discussion with their partners was found to be an associated factor of unmet need of LAPMs of contraception, respondents who don’t discuss with their partners were found about three times more likely to have had unmet need of LAPMs of contraception than those respondents who discuss with their partner at least one times and more AOR [2.9, 95 % CI: 1.8, 9.6; P = 0.01]. Furthermore women’s reports of whether they were counseled or not to use LAPMs of contraceptives was found to be an associated factors of unmet need of LAPMs of contraception, respondents who were not properly counseled by health professionals to use LAPMs of contraception were found to be more than five times more likely to have had unmet need of LAPMs of contraception than those respondents who were properly counseled by health professionals to use LAPMs of contraception AOR [5.3, 95 % CI: 1.7, 11.2; P = 0.04]. The other important association found was women’s occupation, respondents who were categorized as housewives were found to be about five times more likely to have had unmet need of LAPMs of contraception than those respondents who had other occupation AOR [4.7, 95 % CI:3.1, 11.3; P = 0.02]. In logistic regression model, age, parity, residence, religion, knowledge of places, monthly income and the number of children were not associated with unmet need of LAMPs of contraception (Table 5).
Table 5.
Association of unmet need for LAPMs and its correlates among women in the reproductive age group (15-49) using contraception in health facilities in Shashemene town, West Arsi Zone, Oromia Region, 2012 (Multivariate table)
| Determinants | Unmet need of LAPMs | Crude | Adjusted* |
|---|---|---|---|
| Yes (%) | OR(95 % CI) | OR(95 % CI) | |
| Educational status | |||
| Illiterate/Primary (1-8) | 82(42.1) | 4.10(1.64, 8.11) | 3.80(2.90,7.60) |
| Secondary (9-10) & above | 40(23.4) | 1.00 | 1.00 |
| Number of pregnancy | |||
| Zero | 10(35.7) | 1.00 | 1.00 |
| One/two | 46(33.1) | 1.56(0.54,3.35) | 1.42(0.24,5.94) |
| Three/four | 27(27.8) | 1.16(0.48,4.69) | 3.70(0.41,8.14) |
| Five or more | 39(38.2) | 1.74(1.86,7.88) | 1.50(0.34,5.80) |
| Discussed with husband on LAPMs | |||
| Not at all | 69(38.1) | 3.77(2.51,7.73) | 2.90(1.80,9.60) |
| Once/twice | 39(27.3) | 3.79(0.85,8.17) | 2.45(0.62, 5.43) |
| More often | 14(33.3) | 1.00 | 1.00 |
| Main decider on using LAPMs | |||
| Self/Husband | 51(38.3) | 1.35(1.62,6.33) | 0.34(0.26,5.47) |
| Both decide together | 71(30.5) | 1.00 | 1.00 |
| Women’s reports counseled or not | |||
| Yes | 26(29.9) | 1.00 | 1.00 |
| No | 96(34.4) | 5.60(2.44,12.67) | 5.30(1.70,11.20) |
| Number of living children | |||
| Zero | 18(29.5) | 1.00 | 1.00 |
| One/two | 42(31.8) | 0.32(0.58,4.55) | 0.66(0.38,6.71) |
| Three/four | 29(32.2) | 3.81(0.43,6.41) | 2.84(0.63,5.42) |
| Five or more | 33(39.8) | 3.11(2.75,8.19) | 4.16(0.54,8.11) |
| Occupational status | |||
| House wife | 54(43.5) | 6.30(2.20,15.10) | 4.70(3.10,11.30) |
| Government employee | 19(27.5) | 3.18 (0.16,1.36) | 3.70(0.31,3.09) |
| Daily laborer | 10(47.6) | 1.15(0.56,4.07) | 1.55(0.65,3.11) |
| Student | 17(34.7) | 3.11(0.26,5.35) | 1.19(0.12,3.35) |
| Merchant | 22(21.4) | 1.00 | 1.00 |
| Husband attitude to LAPMs | |||
| Approves | 44(22.7) | 0.29(0.45,3.74) | 1.36(0.28,7.78) |
| Opposes | 73(46.5) | 2.17(2.94,10.33) | 0.16(0.33,25.33) |
| Don’t know | 5(33.3) | 1.00 | 1.00 |
*Adjusted for: Number of pregnancy, Main decider on using LAPMs, Number of living children and Husband attitude to LAPMs
Discussion
In this study the women education was found to be one of associated factors of unmet need of LAPMs of contraception. This finding is similar to a study done in Ethiopia and Sri Lanka [17, 18, 19]. So, effort should be on empowering every woman for education as stated in Millennium Development Goal 2.
Women’s discussion with their partners was also found to be an associated factor of unmet need of LAPMs of contraception, respondents who don’t discuss with their partners were found about four times more likely to have had unmet need of LAPMs of contraception than those respondents who discuss with their partner at least ones or more. This is similar to studies done in Jimma and Uganda [20, 21]. This tells us the importance of partner discussion and support on family planning.
A study done in Jimma (Ethiopia) shows women’s being counseled by health professionals was one of associated factors for unmet need for LAPMs [20]. This study also reveals the same result that women who were not properly counseled by health professionals to use LAPMs of contraception were found more than six times more likely to have had unmet need of LAPMs of contraception than those women with proper consultation. This implies that FP service providers should recognize their big responsibility and accountability on providing women who were using modern FP with appropriate counseling about LAPMs.
The other important association with unmet need of LAPMs was the woman’s occupation, respondents who were categorized as housewife were found about six times more likely to have had unmet need of LAPMs of contraception than those respondents with other occupation similar to other studies done in developing countries [22]. Substantial increase in the use of maternal health services can be achieved by accelerating socioeconomic development and effectively addressing basic human needs of schooling, economic welfare, and gender-based discrimination [22].
The study suffers from the usual limitation of cross sectional study. The study could not discover any information from the service providing side of LAPMs. Furthermore, this study was not triangulated by qualitative study. Since the study was institutional based, that might undermine generalizing the result to the general population, and only female contraceptive users were selected, so it was not comprehensive enough to represent all males and females who are desire to use but not using LAPMs.
Conclusion
Unmet need of LAPMs of contraception in health facilities in Shashemene town was high. Factors significantly associated with unmet need of LAMPs of contraception were women’s education, spouse discussion and women counseling. Hence we recommend policy makers and different stakeholders to focus on these major factors associated with LAPMs to increase the service.
Acknowledgements
We would like to express our thanks to the School of Graduate Studies of Joint MPH program Hawassa University and Addis Continental Institute of Public Health for giving us the chance to conduct this research. Also our deepest gratitude goes to Mr. Asressie Molla, Head of the School of Public & Environmental Health at Hawassa University, Mr. Ayalew Astatkie, lecturer at Hawassa University, and others for giving us their constructive idea and comments.
Abbreviations
- AOR
Adjusted Odds Ratio
- CPR
Contraceptive Prevalence Rate
- E.C.
Ethiopian Calendar
- EDHS
Ethiopian Demographic Health Survey
- ETB
Ethiopian Birr
- FP
Family Planning
- IUCD
Intra Uterine Contraceptive Device
- LAPMs
Long Acting and Permanent Methods
- NGO
Non Governmental Organization
- RH
Reproductive Health
Footnotes
Competing interests
We declare that we have no competing interests.
Authors’ contributions
KM conceived the study, developed the proposal, carried out data collection, and conducted the analysis and reviewing the manuscript. SR participated in reviewing the proposal, reviewing the analysis and participated in final study document development. BG provided general guidance in overall study progress and participated in drafting and reviewing the manuscript. All authors read and approved the final manuscript.
Contributor Information
Kuma Mota, Email: kuma1969@yahoo.com.
Surender Reddy, Email: dr.surenderreddy@yahoo.com.
Biniam Getachew, Email: biniongech@gmail.com.
References
- 1.USAID: Long-Acting and Permanent Methods of Contraception: Meeting clients’ needs. http://pdf.usaid.gov/pdf_docs/pnadi070.pdf. Accessed on: February 5, 2015
- 2.Ali, Okud Factors affecting unmet need for family planning in Eastern Sudan. BMC Public Health. 2013;13:102. doi: 10.1186/1471-2458-13-102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.http://www.who.int/reproductivehealth/topics/family_planning/unmet_need_fp/en/)
- 4.Ali M, Cleland J. Determinants of contraceptive discontinuation in six developing countries. J Biosoc Sci. 1999;31:343–60. doi: 10.1017/S0021932099003430. [DOI] [PubMed] [Google Scholar]
- 5.Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat. World Population Prospects. The 2010 Revision, available at http://esa.un.org/unpd/wpp/index.htm.
- 6.Federal Democratic Republic of Ethiopia Ministry of Health . National reproductive health strategy. Addis Ababa, Ethiopia: Federal Democratic Republic of Ethiopia Ministry of Health; 2006. [Google Scholar]
- 7.Wikipidia. List of African Countries by population. Accessed on February, 2015 http://en.wikipedia.org/wiki/Ethiopia.
- 8.Federal Democratic Republic of Ethiopia Central Statistical Agency . Population projection of Ethiopia for all regions at Wereda level from 2014 – 2017. Addis Ababa, Ethiopia: Federal Democratic Republic of Ethiopia Central Statistical Agency; 2013. [Google Scholar]
- 9.Central Statistical Agency - Ethiopia, ORC, Macro . Demographic and health survey - 2005. Addis Ababa, Ethiopia: Central Statistical Agency - Ethiopia, ORC, Macro; 2006. [Google Scholar]
- 10.Central Statistical Agency - Ethiopia, ICF International . Ethiopia Demographic and Health Survey (EDHS) 2011. Addis Ababa, Ethiopia: Central Statistical Agency - Ethiopia, ICF International; 2011. [Google Scholar]
- 11.Family Health International . Long acting and permanent methods: addressing unmet need for family planning in Africa. FHI, 2007. NC: Research Triangle Park; 2007. [Google Scholar]
- 12.Abulie T, Getu D, Mezgebu Y. Demand for long acting and permanent methods of contraceptives and factors for non-use among married women of Goba Town, Bale Zone, South East Ethiopia. Reprod Health. 2012;9:26. doi: 10.1186/1742-4755-9-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Getachew A, Tatek A, Teresa K. Demand for long acting and permanent contraceptive methods and associated factors among married women of reproductive age group in Debre Markos Town, North West Ethiopia. BMC Women’s Health. 2014;14:46. doi: 10.1186/1472-6874-14-46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shashemene town health office . Shashemene town health office annual report. Shashemene, Ethiopia: Shashemene town health office; 2011. [Google Scholar]
- 15.Korra A. Attitudes toward family planning, and reasons for nonuse among women with unmet need for family planning in Ethiopia. Calverton, Maryland USA: ORC Macro; 2002. [Google Scholar]
- 16.Alemayehu M, Belachew T, Tilahun T. Factors associated with utilization of long acting and permanent contraceptive methods among married women of reproductive age in Mekelle town, Tigray region, northEthiopia. BMC Pregnancy and Childbirth 2012; 12:6. [DOI] [PMC free article] [PubMed]
- 17.Gordon C, Sabates R, Bond R, Wubshet T. Women’s education and modern contraceptive use in Ethiopia. International Journal of Education. 2011;13(1):18. [Google Scholar]
- 18.Malwenna L, Jayawardana P, Balasuriya A. Effectiveness of a community based health educational intervention in reducing unmet for modern methods of family planning among ever married reproductive age women in the Kalutara district Sri Lanka. Int J Collabarative Res Intern Med Public Health. 2012;4(6):1097–114.
- 19.Eliason S, Awoonor-Williams J, Eliason C, Novignon J, Nonvignon J, Aikins M. Determinants of modern family planning use among women of reproductive age in the Nkwanta district of Ghana: a case–control study. Reprod Health. 2014;11:65. doi: 10.1186/1742-4755-11-65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Eskindir L, Mekonnen A, Chali J, FasilTessema Assessment of quality of care in family planning service in Jimma zone, Ethiop. JHealth Dev. 2003;18(1):8–18. [Google Scholar]
- 21.Kasedde S. Long-term and permanent family planning methods in Uganda: a literature review. Baltimore, MD: Johns Hopkins Bloomberg School of Public Health/Center for Communication Programs; 2000. [Google Scholar]
- 22.Ahmed S, Creanga A, Gillespie D, Tsui A. Economic status, education and empowerment: implications for maternal health services utilization in developing countries. PLoS ONE. 2010;5(6) doi: 10.1371/journal.pone.0011190. [DOI] [PMC free article] [PubMed] [Google Scholar]