

Abstract
Traditional Chinese medicine (TCM) is one of the most common complementary and alternative medicines used in the treatment of patients with cancer worldwide. However, the clinical effect of TCM on patients with pancreatic cancer remains unclear. This study was aimed to explore the efficacy of TCM on selected patients with pancreatic cancer and to study the usefulness of multimodality treatment, including TCM and western medicine (WM), in pancreatic cancer.
From January 2009 to October 2013, 107 patients with pancreatic cancer were included in this study. Kaplan–Meier curves were used to assess the differences in survival time. Cox regression analysis was performed to determine survival trends adjusted for clinical and demographic factors.
Cox regression analysis suggested that elevated CA19-9 levels (P = 0.048), number of cycles of chemotherapy (P = 0.014), and TCM were independent prognostic factors (P < 0.001). The survival hazards ratio of TCM was 0.419 (95% confidence interval [CI], 0.261–0.671). The median overall survival (OS) was 19 months for patients with TCM treatment, while the median OS was 8 months for those without TCM treatment (P < 0.001). Patients who received multimodality treatment using TCM and WM had the best prognosis with a median OS of 19 months (P < 0.001). Patients with heat-clearing, diuresis-promoting and detoxification TCM treatment had a longer survival time (32.4 months) than those with blood-activating and stasis-dissolving (9.8 months) and tonifying qi and yang treatment (6.1 months; P = 0.008).
These results indicate that TCM has an important potential value for improving the prognosis of patients with pancreatic cancer, and multimodality treatment, including TCM and WM, leads to the best prognosis. More importantly, we suggest that heat-clearing, diuresis-promoting, and detoxification TCM treatment may improve the efficacy of TCM in pancreatic cancer.
INTRODUCTION
Pancreatic cancer is the fourth leading cause of cancer-related death in Europe and the United States.1,2 Early-stage pancreatic cancer is usually clinically silent, and disease only becomes apparent after the tumor invades surrounding tissues or metastasizes to distant organs.3 The overall survival (OS) of pancreatic cancer remains poor despite important improvements that have been made during the last decades among patients with early-stage disease.4 The 5-year survival for patients with pancreatic cancer is low, at approximately 5%.5
Conventional treatment approaches for pancreatic cancer include surgery, chemotherapy, and radiotherapy. Surgery is regarded as the only possible option to cure pancreatic cancer. However, less than 20% patients have a chance of operation, and postoperation survival is not satisfactory for most patients. In addition, pancreatic cancer responds poorly to most chemotherapeutic agents, and addition of radiation to adjuvant chemotherapy is unproven and controversial.6 The treatment and prognosis of pancreatic cancer is so poor that we should pay more attention to multidisciplinary treatment, which should include traditional Chinese medicine (TCM) treatment. In fact, multidisciplinary treatments for patients with pancreatic cancer have shown promise.7,8
TCM, as an ancient method against cancer, has been used in Asian countries for hundreds of years. Many clinical studies have shown that TCM is effective in the treatment of breast, gastric, and lung cancer.9–11 Our previous clinical study also indicated that TCM could improve the OS of patients with unresectable hepatocellular carcinoma.12 Moreover, many herb monomers and herb formulas could inhibit pancreatic cancer cell growth in vivo and in vitro.13,14 In addition, a clinical study showed that Chinese herbal medicine was a protective factor for patients with pancreatic cancer liver metastases.15 However, clinical studies on the survival benefit of TCM in pancreatic cancer are rare, and the efficacy of TCM in pancreatic cancer remains largely unknown.
According to TCM theories, herbal treatment is adapted according to the syndrome. The fundamental TCM treatment principle for pancreatic cancer involves clearing liver and resolving dampness, and 3 supporting TCM treatment principles are heat-clearing, diuresis-promoting and detoxification, blood-activating and stasis-dissolving, and tonifying qi and yang. The pancreas belongs to the hepatobiliary system in terms of TCM theories; thus, pancreatic cancer was mainly treated with herbs, with the effect of clearing liver and resolving dampness. In addition, it is well established that inflammation, hypercoagulability and the lack of an immune function are common in cancer, particularly in pancreatic cancer.16–18 Therefore, antiinflammation and improving the blood hypercoagulable state and the body's immune system are of significance for pancreatic cancer patients. Traditional Chinese herbs with activities of heat-clearing, diuresis-promoting and detoxification, blood-activating and stasis-dissolving, or tonifying qi and yang can improve these pathological conditions mentioned above and may subsequently improve the prognosis of patients.19 However, few reports regarding whether different TCM treatment principles can make a difference in the prognosis of patients with pancreatic cancer have been published in the last decades.
Therefore, we explored whether TCM herbal treatment has independent prognostic value for patients with pancreatic cancer and further evaluated the possible survival benefits of western medicine (WM) and TCM treatment for these patients. Moreover, we investigated whether different supporting TCM treatment principles influenced the survival of patients with pancreatic cancer.
MATERIALS AND METHODS
Patient Characteristics
We retrospectively studied 107 pancreatic cancer patients between January 2009 and October 2013 in Tianjin Medical University Cancer Hospital. We derived patient data from a review of inpatient and outpatient medical records and from direct patient follow-up visits. Major inclusion criteria were as follows: aged 18 years or older; histologic or cytologic diagnosis of pancreatic cancer or clinical and radiographic evidence of pancreatic cancer. Moreover, patients in the TCM group received TCM treatment for 2 months or more. Major exclusion criteria were as follows: serious complications (massive hemorrhage of the gastrointestinal tract, complete obstruction of the digestive tract, gastrointestinal perforation, severe cardiac or pulmonary diseases); concurrent cancer; pregnant or breast-feeding women; severe mental disorder; incomplete medical records; patients with molecular target therapy; and no accurate survival time or lost to follow-up. Finally, 51 patients who received TCM treatment alone or together with WM, including surgery, chemotherapy, radiotherapy, and biotherapy, were included in the TCM group.
Treatment
Treatment with TCM formulas was granted according to the syndrome differentiation. The herbs used in our hospital were granulas. Herbal granulas are produced by Beijing Tcmages Pharmaceutical Co. Ltd (Niuhui street No.5, Niulanshan Industrial Zone, Shunyi District, Beijing, China), and the quantity of herbal granulas is guaranteed by this company. All patients received instructions to prepare the decoction, and the herbal granulas were taken after being dissolved in boiled water. The TCM was taken orally 3 times a day, 30 minutes after meals for 2 months (4 courses) or more in the TCM group. The core TCM formula remained in all treatments, and changes (herb modification) were only made based on the patients’ symptoms every 2 weeks. TCM formulas were recorded by an electronic prescription system in our hospital. Analysis of TCM formulas was performed using the prescriptions of 40 patients in the TCM group because the prescriptions of the other 11 patients were incomplete or missing in the electronic prescription system.
The traditional WM included surgery, chemotherapy, and radiotherapy for pancreatic cancer. Biotherapy therapy was rare among patients with pancreatic cancer in China. In this study, WM comprised the 4 types mentioned above.
Principles of TCM Treatment
In China, TCM herbs are given based on TCM theory and are prescribed by practitioners of TCM. Patients with the same disease may have different TCM syndromes. The TCM herbs are adjusted to the individual patient's syndromes to improve the prognosis. It was our intention to evaluate whether the patients with different TCM treatments were associated with a prolonged survival time.
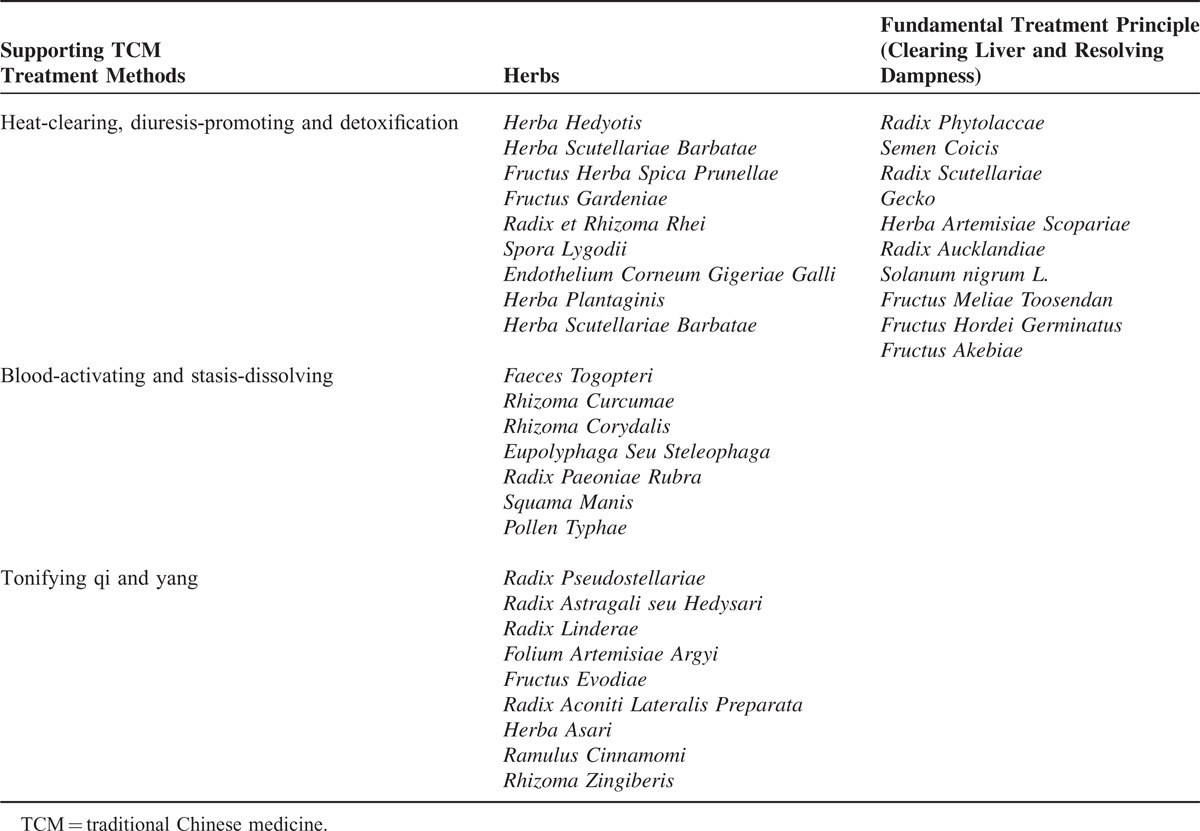
We analyzed the TCM formulas of 40 patients from the electronic prescription system of our hospital. In this study, for pancreatic cancer patients, the basic principles of TCM treatment were clearing liver and resolving dampness. According to the TCM theories and herb prescription features, we divided these patients into 3 groups: heat-clearing, diuresis-promoting and detoxification, blood-activating and stasis-dissolving, and tonifying qi and yang. The commonly used and typical herbs are shown in Table 1.
TABLE 1.
Three Kinds of Supporting TCM Treatment Methods on Pancreatic Cancer and Most Commonly Used Herbs of Each Method
Statistical Analysis
OS from the date of the definitive diagnosis of pancreatic cancer was estimated using the Kaplan–Meier method, and survival curves were compared using the log-rank test. The continuous variables were divided into categories using population quartiles, upper normal values, and published data to determine cutoff values. Multivariate Cox regression analysis was performed to determine survival trends adjusted for clinical and demographic factors. Baseline comparison was analyzed by the χ2 test. A P-value <0.05 was considered to indicate statistical significance.
All statistical analyses were performed using SPSS version 16.0.
RESULTS
Patient Characteristics
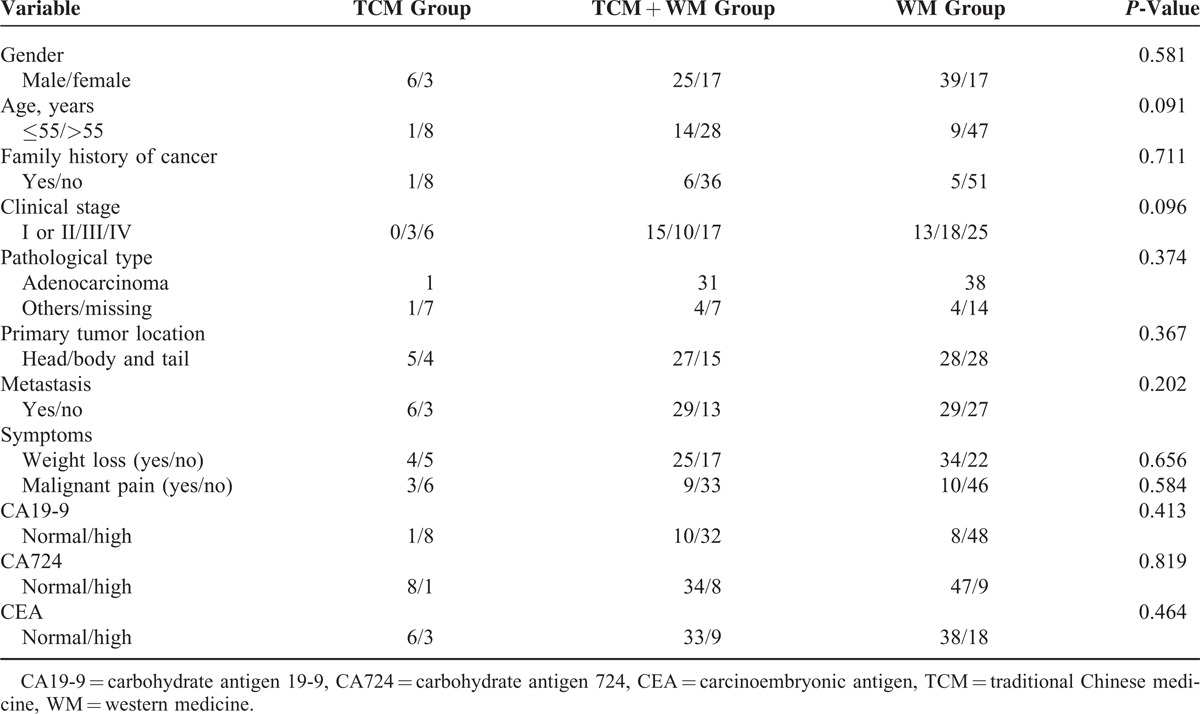
A total of 107 patients with pancreatic cancer were included in this study. The median age was 62 years (range, 41–85 years). Pancreatic cancer is predominately a disease of older individuals. In this study, 83 (77.6%) of 107 patients were diagnosed at age >55 years, and univariate analysis showed that age did not affect the survival outcome of pancreatic cancer (P = 0.340). There were more males than females (63.6% vs 36.4%, respectively), an observation that is in agreement with that in a study showing that the age-adjusted pancreatic cancer incidence in men was 30% higher than that in women.4 Of these patients, 79 (73.8%) had histological evidence of pancreatic cancer, among whom 70 (65.4%) had adenocarcinoma, and 28 (26.2%) were diagnosed through clinical and radiographic evidence. Stage I or II patients accounted for 26.2% (n = 28) of patients, and 73.8% (n = 79) of patients were diagnosed at stage III or IV. The demographic and clinical characteristics for these 107 patients are summarized in Table 2.
TABLE 2.
Univariate and Multivariate Analyses of Variables Influencing Survival of 107 Patients with Pancreatic Cancer
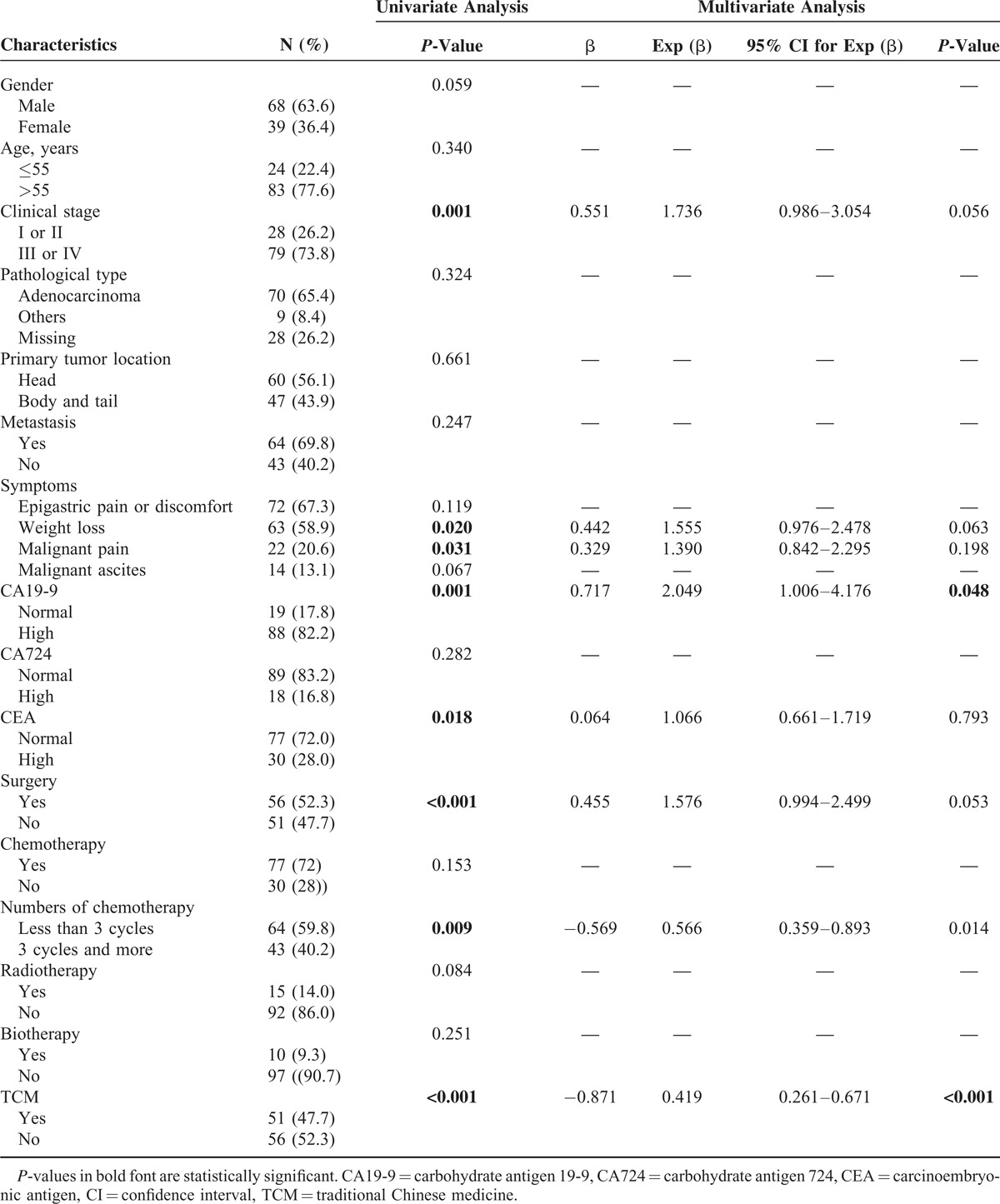
Univariate Analysis and Multivariate Analysis
Univariate analysis revealed that stage III or IV disease, weight loss (>10% within 6 months), malignant pain, elevated carbohydrate antigen (CA)19-9 levels (≥40 U/ml), and elevated carcinoembryonic antigen (CEA) levels (≥5 μg/L) were significantly associated with reduced median OS (Table 2). By contrast, surgery, 3 cycles and more of chemotherapy, and TCM were considered protective factors in univariate analysis (Table 2).
Patient-, tumor-, and treatment-related variables that were found to be significantly associated with OS by univariate analysis were subsequently evaluated by Cox regression analysis to determine independent risk factors for the survival of pancreatic cancer patients. Elevated CA19-9 levels were found to be an independent predictor of poor survival; 3 cycles and more of chemotherapy and TCM were found to be independent protective factors (Table 2).
Survival Analysis of Different Treatment Groups
Cox regression univariate analysis suggested that TCM was an independent protective factor. We next accessed the difference in survival time between the TCM group (n = 51) and non-TCM group (n = 56) directly. As expected, there was a significant difference in the survival prognosis between patients with and without TCM treatment. Patients in the TCM group had a longer median OS (19 months) than those in the non-TCM group with a median OS of 8 months. The 1- and 2-year survival rate for the 2 groups were 54.9%, 38.2% and 30.4%, 6.6%, respectively (P < 0.001; Figure 1A). The 3-year survival rate of the TCM group was 24.4%. The details of the baseline characteristics are shown in Table 3.
FIGURE 1.
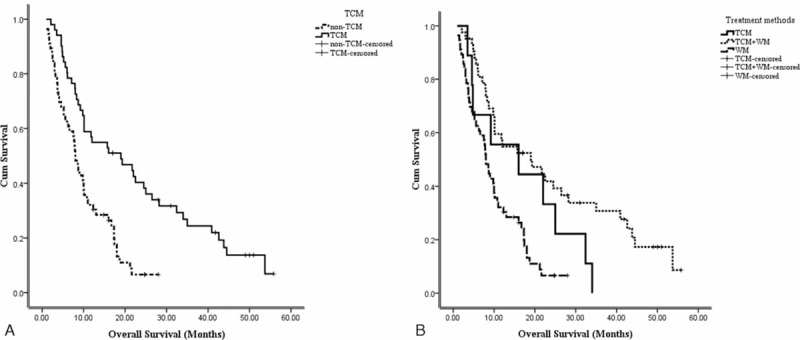
(A) Survival analysis between the TCM and non-TCM groups. The median OS in the TCM group was longer than that in the non-TCM group (19 vs 8 months, respectively; P < 0.001). (B) Survival analysis of patients with different treatment methods. The TCM + WM subgroup showed the best prognosis than that in TCM and WM groups; (P < 0.001). OS = overall survival, TCM = traditional Chinese medicine, WM = western medicine.
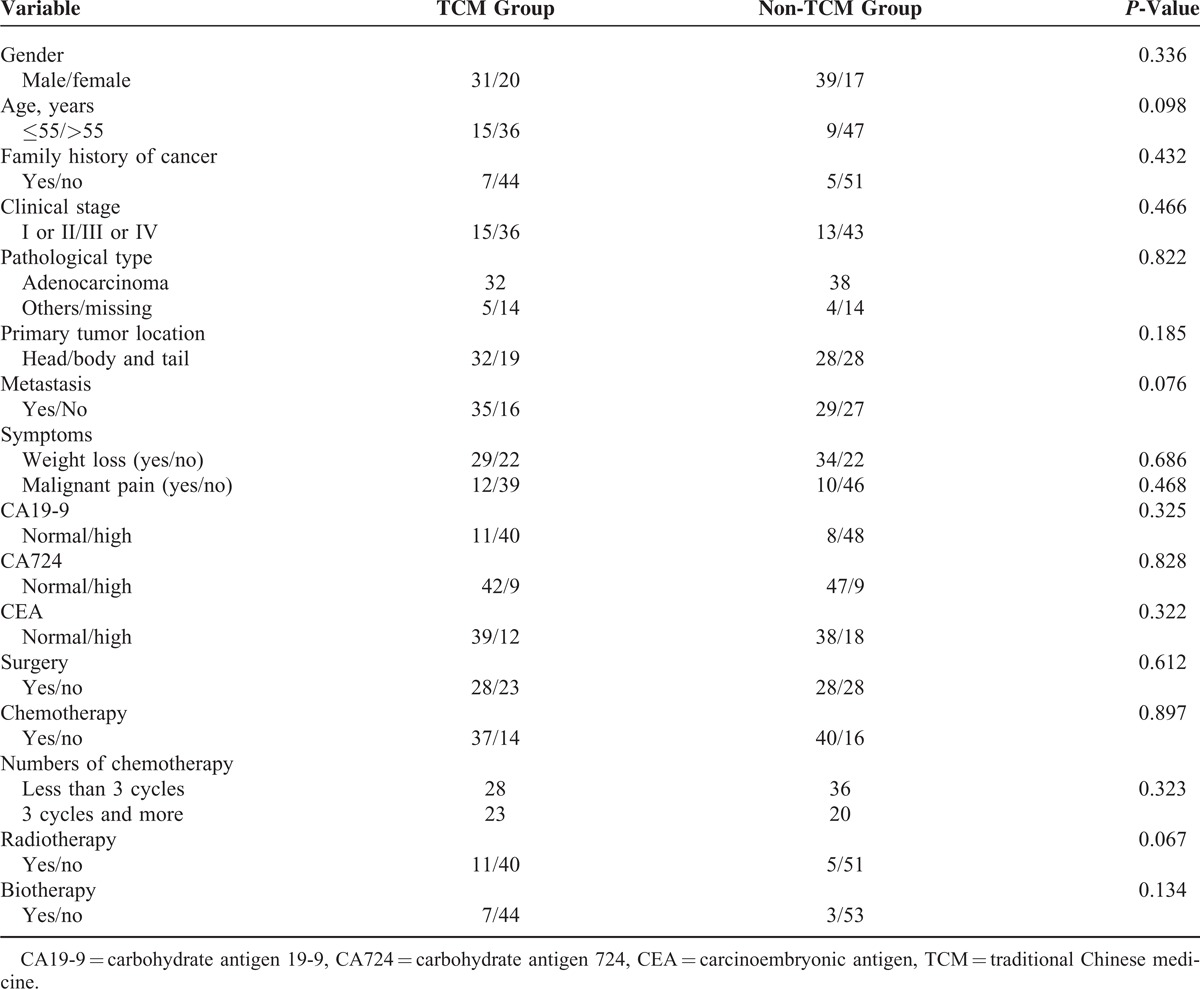
TABLE 3.
Details of Baseline Characteristics of Patients with Pancreatic Cancer
There were 9 patients receiving only TCM treatment; thus, according to therapeutic methods, we divided these patients into 3 subgroups: the TCM subgroup (n = 9), TCM + WM subgroup (n = 42), and WM subgroup (n = 56). The median survival times were 16, 19, and 8 months, respectively (P < 0.001; Figure 1B). The 1- and 2-year survival rates for the 3 groups were 44.4%, 54.8%, and 30.4% (1 year) and 22.4%, 39.3%, and 6.6% (2 years), respectively. The 3-year survival rate of the TCM + WM group was 30.8%. The details of the baseline characteristics are presented in Table 4.
TABLE 4.
Details of Baseline Characteristics of Patients with Different Combination Treatment Strategies
TCM Group Analysis
Patients with the same disease may have different TCM syndromes. Here, we wanted to analyze whether different principles of TCM treatment were associated with the prognosis of patients with pancreatic cancer. We analyzed the TCM formulas of 40 patients, who received 7701 days of TCM treatment and 165 types of herbs in total. The frequency of single-herb treatment was balanced by dividing the average treatment days and patient numbers. The frequency of single herbs over 10% is shown in Figure 2.
FIGURE 2.
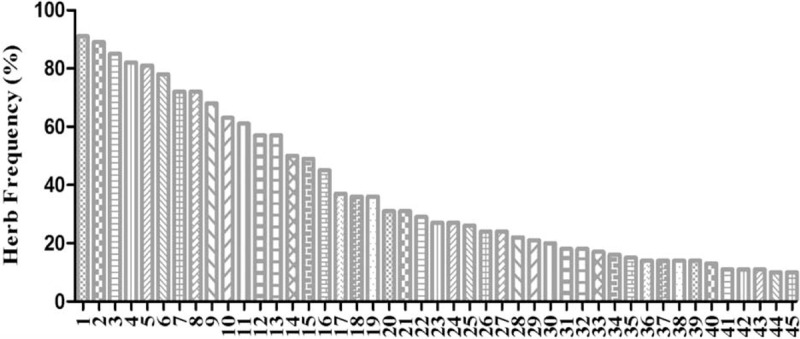
Forty-five types of herbs with a frequency >10.0%. (1) Radix Phytolaccae, (2) Semen Coicis, (3) Radix Scutellariae, (4) Gecko, (5) Herba Artemisiae Scopariae, (6) Radix Aucklandiae, (7) Radix Notoginseng, (8) Solanum nigrum L. (9) Fructus Meliae Toosendan, (10) Fructus Hordei Germinatus, (11) Fructus Akebiae, (12) Radix Curcumae, (13) Herba Pogostemonis, (14) Rhizoma Bolbostemmatis, (15) Rhizoma Pinelliae Preparatum, (16) Fructus Ammomi Rotundus, (17) Fructus Lycii, (18) Alumen, (19) Carapax Trionycis, (20) Rhizoma Arisaematis Cum Bile, (21) Endothelium Corneum Gigeriae Galli, (22) Radix Paeoniae Alba, (23) Sarcandra glabra (Thunb.) Nakai, (24) Cortex Magnoliae Officinalis, (25) Pericarpium Arecae, (26) Radix Glycyrrhizae, (27) Faeces Togopteri, (28) Radix Bupleuri, (29) Salvia chinensis Benth, (30) Bulbus Fritillariae Thunbergii, (31) Radix Trichosanthis, (32) Rhizoma Corydalis, (33) Talcum, (34) Rhizoma Cyperi, (35) Spora Lygodii, (36) Bulbus Lilii, (37) Herba Hedyotis, (38) Herba Taraxaci, (39) Radix Cynanchi Paniculati, (40) Radix Angelicae Sinensis, (41) Fructus Amomi Villosi, (42) Radix Scrophulariae, (43) Rhizoma Curcumae Longae, (44) Rhizoma Arisaematis, and (45) Actinidia valvata Dunn.
Using scatter diagrams of the death distribution in the TCM and non-TCM groups (Figure 3A and B), the efficacy of TCM treatment could be evaluated as follows: low-efficacy group (survival time ≤25 months, n = 34) and high-efficacy group (survival time >25 months, n = 17). Unfortunately, there was no one in the non-TCM group who survived 25 months or longer.
FIGURE 3.
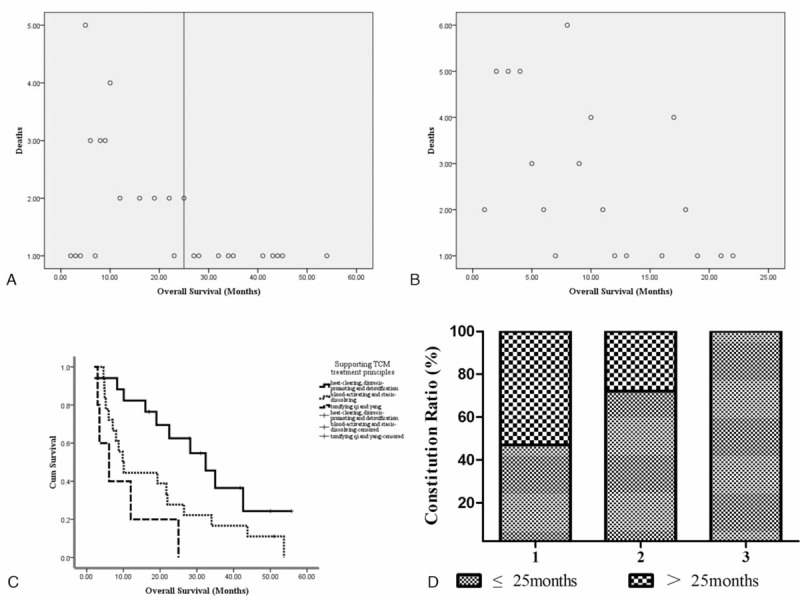
(A and B) Death distribution scatter diagram of patients in the TCM group (A) and non-TCM group (B). (C) Survival analysis of patients with different supporting TCM treatment principles. The median OS of patients who received heat-clearing diuresis-promoting and detoxification was longer than that for patients who received blood-activating and stasis-dissolving, and tonifying qi and yang TCM treatment (P = 0.008). (D) Constitution rates of survival time in different supporting TCM treatment principles. It was significantly different in patients who survived more than 25 months between heat-clearing, diuresis-promoting and detoxification adjuvant therapy subgroup and other adjuvant therapy subgroups (P < 0.001). 1 = heat-clearing, diuresis-promoting and detoxification, 2 = blood-activating and stasis-dissolving, 3 = tonifying qi and yang. OS = overall survival, TCM = traditional Chinese medicine.
According to the TCM formulas of the 40 patients, we created 3 groups according to TCM theory: heat-clearing, diuresis-promoting and detoxification (n = 17), blood-activating and stasis-dissolving (n = 18), and tonifying qi and yang (n = 5). The median OS values were 32.4, 9.8, and 6.1 months, respectively (P = 0.008; Figure 3C). These results suggested that patients receiving heat-clearing, diuresis-promoting and detoxification treatment had prolonged survival. This indicates that patients in the high-efficacy TCM treatment group (survival time >25 months) tended to receive heat-clearing, diuresis-promoting and detoxification treatment. Next, we calculated the survival constitution rates of the different TCM treatment groups. Among the patients receiving heat-clearing, diuresis-promoting and detoxification and blood-activating and stasis-dissolving, the constitution rates in the highly effective group (survival time ≥25 months) were 53% and 28%, respectively. All patients with tonifying qi and yang TCM treatment survived <25 months (P < 0.001; Figure 3D).
DISCUSSION AND CONCLUSIONS
Pancreatic cancer is one of the most aggressive cancers, with almost equivalent incidence and mortality rates. The OS of pancreatic cancer remains poor, and the 5-year OS for patients with pancreatic cancer is <5%.5 In the present study, we retrospectively analyzed 107 patients with pancreatic cancer and observed the efficacy of TCM in pancreatic cancer.
Cox regression analysis showed that an elevated CA19-9 level (P = 0.048), 3 cycles and more of chemotherapy (P = 0.014), and TCM treatment (P < 0.001) were independent prognostic factors. The HR of TCM was 0.419 (95% CI, 0.261–0.671). No TCM-related adverse events were observed, with a median TCM intervention time of 6 months.
A previous clinical study showed that Chinese herbal medicine was an independent protective factor in patients with pancreatic cancer liver metastases. The OS was 5.4 months, and the 1-year survival rate was 21.9% for the TCM group, compared with a median survival of 3.9 months and 1-year survival rate of 4.8% for the non-TCM group.15 In our study, TCM herbal treatment did improve the prognosis of patients with pancreatic cancer. The patients in the TCM group had a longer median OS (19 months) than those in the non-TCM group (8 months; P < 0.001). In addition, the 1- and 2-year survival rates for the 2 groups were 54.9%, 38.2% and 30.4%, 6.6%, respectively. Remarkably, the 3-year survival rate of the TCM group was 24.4%, while no one in the non-TCM group survived over 3 years. These results suggested the survival benefit of TCM treatment in patients with pancreatic cancer.
Moreover, subgroup analysis showed that patients in the TCM + WM group had the best prognostic outcome with a median OS of 19 months (P < 0.001). The median OS in the TCM and WM groups were 16 and 8 months, respectively. Although there was no statistically significance between the TCM and WM groups (P = 0.075), for patients who could not receive WM therapy, TCM treatment may be a good alternative choice. These findings indicated that multimodality treatment, including TCM and WM, was promising for patients with pancreatic cancer, and this result was in accordance with that in a previous study showing that multimodality treatment was effective in prolonging the survival of patients with liver metastases of pancreatic cancer.15
We then analyzed the characteristics of the TCM group to further explore the effectiveness of TCM. Initially, the top 3 herbs used in our TCM prescriptions for patients with pancreatic cancer were Radix Phytolaccae, Semen Coicis, and Radix Scutellariae (Figure 2). All 3 herbs have been used as effective antitumor drugs for over a thousand years,20–22 and Semen Coicis is an important herb used in TCM formulas for the treatment of pancreatic cancer. Semen Coicis, belonging to the family Gramineae, is a potential cancer chemopreventive agent toward multistage carcinogenesis processes.21 Many traditional Chinese herb formulas against pancreatic cancer contain Semen Coicis, such as the Qingyihuaji formula.23,24 In addition, Kang-Lai-Te (KLT) injections, extracted from Semen Coicis, is a new biphase extended-spectrum anticancer medicine,25 and the Food and Drug Administration (FDA) of the United States also approved a phase II trial to investigate the therapeutic efficacy of KLT in combination with gemcitabine in pancreatic cancer patients (http://www.clinicaltrial.gov). The mechanisms contributing to the antitumor effect of Semen Coicis, at least in part, included cell-cycle arrest and apoptosis induction involving the upregulation of the cyclin-dependent kinase inhibitor p21 and inhibition of antiapoptotic protein Bcl-2 expression.26
Second, we further evaluated whether different supporting TCM treatment methods were associated with a different survival time. Based on the symptoms and characteristics of patients and guided by the theories of TCM, a formula was designed to contain a combination of different types of plants or minerals to improve clinical efficacy. In our study, for pancreatic cancer patients, the basic principle of TCM treatment was clearing liver and resolving dampness. According to different supporting TCM therapeutic methods, we divided these patients into 3 groups: heat-clearing, diuresis-promoting and detoxification, blood-activating and stasis-dissolving, and tonifying qi and yang. We found that the median OS values were 32.4, 9.8, and 6.1 months, respectively (P = 0.008). These results indicate that heat-clearing, diuresis-promoting and detoxification TCM treatment showed a longer OS than the other 2 groups, and patients with tonifying qi and yang therapy had the worst prognosis. Although tonifying qi and yang treatment can strengthen the patients’ physical health,27–29 patients who receive tonifying qi and yang treatment are in poor physical condition, which may explain why this group is insensitive to TCM therapy.
Certainly, there are potential limitations in the present study. First, the number of patients in this study is relatively small, and the study is retrospective. A large number of multicenter prospective randomized trials should be undertaken comparing traditional WM and TCM treatment. Second, we did not classify patients in terms of clinical stage. The cause may be due to the following: the number of cases was too small to group them into subgroups according to clinical stage; in this study, clinical stage was not an independent prognostic factor (P = 0.056); the baseline characteristics of each subgroup were equal; and the prognosis of each stage of pancreatic cancer is poor. However, there are several strengths in this study. First, we suggest that TCM treatment can bring survival benefit for patients with pancreatic cancer. In fact, there are rare clinical studies focusing on TCM therapy for patients with pancreatic cancer. In addition, we indicate that different supporting TCM treatment principles affect survival time, providing prescription medication advice in clinical practice.
We conclude, from this small retrospective study, that TCM treatment was associated with a survival benefit in patients with pancreatic cancer. In addition, TCM in combination with WM would be a better optimal treatment for patients with pancreatic cancer to improve survival time. More importantly, we provide TCM practitioners with a proposal that heat-clearing, diuresis-promoting and detoxification TCM treatment may improve the efficacy of TCM in patients with pancreatic cancer.
Footnotes
Abbreviations: CA19-9 = carbohydrate antigen 19-9, CEA = carcinoembryonic antigen, OS = overall survival, TCM = traditional Chinese medicine, WM = western medicine.
This work was supported by the National Science Foundation of China (nos. 81173376 and 81473441).
The authors have no conflicts of interest to disclose.
REFERENCES
- 1.Siegel R, Ma J, Zou Z, et al. Cancer statistics, 2014. CA Cancer J Clin 2014; 64:9–29. [DOI] [PubMed] [Google Scholar]
- 2.Malvezzi M, Bertuccio P, Levi F, et al. European cancer mortality predictions for the year 2013. Ann Oncol 2013; 24:792–800. [DOI] [PubMed] [Google Scholar]
- 3.Kelsen DP, Portenoy R, Thaler H, et al. Pain as a predictor of outcome in patients with operable pancreatic carcinoma. Surgery 1997; 122:53–59. [DOI] [PubMed] [Google Scholar]
- 4.Shaib YH, Davila JA, El-Serag HB. The epidemiology of pancreatic cancer in the United States: changes below the surface. Aliment Pharmacol Ther 2006; 24:87–94. [DOI] [PubMed] [Google Scholar]
- 5.Sener SF, Fremgen A, Menck HR, et al. Pancreatic cancer: a report of treatment and survival trends for 100,313 patients diagnosed from 1985–1995, using the National Cancer Database. J Am Coll Surg 1999; 189:1–7. [DOI] [PubMed] [Google Scholar]
- 6.Vincent A, Herman J, Schulick R, et al. Pancreatic cancer. Lancet 2011; 378:607–620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pawlik TM, Laheru D, Hruban RH, et al. Evaluating the impact of a single-day multidisciplinary clinic on the management of pancreatic cancer. Ann Surg Oncol 2008; 15:2081–2088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yang GY, Wagner TD, Fuss M, et al. Multimodality approaches for pancreatic cancer. CA Cancer J Clin 2005; 55:352–367. [DOI] [PubMed] [Google Scholar]
- 9.Lee YW, Chen TL, Shih YR, et al. Adjunctive traditional Chinese medicine therapy improves survival in patients with advanced breast cancer: a population-based study. Cancer 2014; 120:1338–1344. [DOI] [PubMed] [Google Scholar]
- 10.Xu Y, Zhao AG, Li ZY, et al. Survival benefit of traditional Chinese herbal medicine (a herbal formula for invigorating spleen) for patients with advanced gastric cancer. Integr Cancer Ther 2013; 12:414–422. [DOI] [PubMed] [Google Scholar]
- 11.Guo H, Liu JX, Xu L, et al. Traditional Chinese medicine herbal treatment may have a relevant impact on the prognosis of patients with stage IV adenocarcinoma of the lung treated with platinum-based chemotherapy or combined targeted therapy and chemotherapy. Integr Cancer Ther 2011; 10:127–137. [DOI] [PubMed] [Google Scholar]
- 12.Man Y-N, Liu X-H, Wu X-Z. Chinese medicine herbal treatment based on syndrome differentiation improves the overall survival of patients with unresectable hepatocellular carcinoma. Chin J Integr Med 2015; 21:49–57. [DOI] [PubMed] [Google Scholar]
- 13.Liszka L, Pajak J, Mrowiec S, et al. Age distribution patterns of patients with conventional ductal adenocarcinoma of the pancreas. A single-institution study of 580 cases re-evaluated using current histopathological diagnostic criteria. Pol J Pathol 2010; 61:65–77. [PubMed] [Google Scholar]
- 14.Li Y, Ellis K-L, Ali S, et al. Apoptosis-inducing effect of chemotherapeutic agents is potentiated by soy isoflavone genistein, a natural inhibitor of NF-kappaB in BxPC-3 pancreatic cancer cell line. Pancreas 2004; 28:e90–e95. [DOI] [PubMed] [Google Scholar]
- 15.Ouyang H, Wang P, Meng Z, et al. Multimodality treatment of pancreatic cancer with liver metastases using chemotherapy, radiation therapy, and/or Chinese herbal medicine. Pancreas 2011; 40:120–125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell 2010; 140:883–899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sorensen HT, Mellemkjaer L, Olsen JH, et al. Prognosis of cancers associated with venous thromboembolism. N Engl J Med 2000; 343:1846–1850. [DOI] [PubMed] [Google Scholar]
- 18.Yang L, Yamagata N, Yadav R, et al. Cancer-associated immunodeficiency and dendritic cell abnormalities mediated by the prostaglandin EP2 receptor. J Clin Invest 2003; 111:727–735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.World Scientific, Yu R, Hong H. Cancer Management with Chinese Medicine [M]. 2012. [Google Scholar]
- 20.Ravikiran G, Raju A, Venugopal Y. Phytolacca americana: a review. Int J Res Pharm Biomed Sci 2011; 2:942–946. [Google Scholar]
- 21.Kuo CC, Chen HH, Chiang W. Adlay (yi yi; “soft-shelled job's tears”; the seeds of Coix lachryma-jobi L. var. ma-yuen Stapf) is a potential cancer chemopreventive agent toward multistage carcinogenesis processes. J Tradit Complement Med 2012; 2:267–275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Donald G, Hertzer K, Eibl G. Baicalein—an intriguing therapeutic phytochemical in pancreatic cancer. Curr Drug targets 2012; 13:1772–1776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Yin J-H, Shi W-D, Zhu X-Y, et al. Qingyihuaji formula inhibits progress of liver metastases from advanced pancreatic cancer xenograft by targeting to decrease expression of Cyr61 and VEGF. Integr Cancer Ther 2012; 11:37–47. [DOI] [PubMed] [Google Scholar]
- 24.Wang P, Chen Z, Meng Z-Q, et al. Ski acts as therapeutic target of qingyihuaji formula in the treatment of SW1990 pancreatic cancer. Integr Cancer Ther 2010; 9:50–58. [DOI] [PubMed] [Google Scholar]
- 25.Lu Y, Wu LQ, Dong Q, et al. Experimental study on the effect of Kang-Lai-Te induced apoptosis of human hepatoma carcinoma cell HepG2. Hepatobiliary Pancreat Dis Int 2009; 8:267–272. [PubMed] [Google Scholar]
- 26.Bao Y, Yuan Y, Xia L, et al. Neutral lipid isolated from endosperm of Job's tears inhibits the growth of pancreatic cancer cells via apoptosis, G2/M arrest, and regulation of gene expression. J Gastroenterol Hepatol 2005; 20:1046–1053. [DOI] [PubMed] [Google Scholar]
- 27.Tatsumi K, Shinozuka N, Nakayama K, et al. Hochuekkito improves systemic inflammation and nutritional status in elderly patients with chronic obstructive pulmonary disease. J Am Geriatr Soc 2009; 57:169–170. [DOI] [PubMed] [Google Scholar]
- 28.Ko K-M, Leon T, Mak D, et al. A characteristic pharmacological action of ‘Yang-invigorating’ Chinese tonifying herbs: enhancement of myocardial ATP-generation capacity. Phytomedicine 2006; 13:636–642. [DOI] [PubMed] [Google Scholar]
- 29.Ko KM, Leung HY. Enhancement of ATP generation capacity, antioxidant activity and immunomodulatory activities by Chinese Yang and Yin tonifying herbs. Chin Med 2007; 2:3. [DOI] [PMC free article] [PubMed] [Google Scholar]