

Abstract
Purpose
The presence of the subacromial-subdeltoid (SASD) bursa inflammation has recently been proposed as a primary radiologic factor predicting persistent limitation and pain in operated patients. The aim of the study was to verify the hypothesis that pain, or increased shoulder pain, could be associated with SASD bursitis not only in operated patients but also in general population.
Methods
A consecutive series of 1940 shoulder ultrasound examinations were performed by our Department over a 5-year period using linear multi-frequency probes. All reports of examination executed for shoulder pain were reviewed. The video clips were independently reviewed by two radiologists: effusion in the SASD bursa and the presence of other pathological conditions were evaluated and confirmed.
Results
A total of 1147 shoulder video clips were re-evaluated, and 1587 pathologies were detected; 65.5 % of patients had only one pathology, 30.4 % had two and 4.1 % presented three pathologies. The difference between the group with and without effusion is statistically significant for acromioclavicular joint arthritis, supraspinatus tendon calcific tendinopathy, full-thickness and superficial tear of the supraspinatus, traumas and rheumatoid arthritis with a p value <0.01.
Conclusions
Our study shows that the effusion in the SASD bursa is frequently associated with shoulder pain often independently from the underlying pathology; further studies are needed to confirm the statistical significance of this relationship by clarifying possible confounding factors.
Electronic supplementary material
The online version of this article (doi:10.1007/s40477-015-0167-0) contains supplementary material, which is available to authorized users.
Keywords: Ultrasound, Subacromion-subdeltoid bursa, Bursal inflammation, Shoulder pain
Riassunto
Scopo del lavoro
La presenza di alterazioni flogistiche a livello della borsa subacromiondeltoidea (BSAD) è stata recentemente proposta come fattore principale per predire la comparsa di dolore e limitazione funzionale nei Pazienti operati a livello della spalla. Lo scopo del nostro studio è di verificare l’ipotesi che il dolore, o l’incremento dello stesso, sia associato con la flogosi della BSAD non solo nei Pazienti operati ma anche nella popolazione generale.
Materiali e Metodi
In 5 anni nel nostro dipartimento sono state eseguite, utilizzando esclusivamente sonde lineari multifrequenza, 1940 ecografie della spalla. Tutti gli esami aventi come indicazione il dolore sono stati selezionati. I videoclip degli esami selezionati sono stati rivalutati da due radiologi indipendentemente: è stata in tal modo confermata la presenza di versamento nella BSAD e di altri reperti patologici.
Risultati
Sono stati rivalutati i videoclip di 1147 ecografie di spalla. Sono state individuate 1587 alterazioni patologiche; il 65.5 % dei Pazienti presentava unicamente un riscontro patologico, il 30.4 % ne presentava due e il 4.1 % ne presentava 3. La differenza tra gruppo con e senza versamento è statisticamente significativa (p value <0.01) in caso di artrosi acromionclaveare, tendinopatia calcifica del sovraspinato, lesioni a tutto spessore e del versante bursale del tendine del sovraspinato, nei traumi e nell’artrite reumatoide.
Conclusioni
Il nostro studio mostra come il versamento nella BSAD sia frequentemente associato con il dolore di spalla spesso indipendentemente dalla patologia sottostante; ulteriori studi sono necessari per confermare tale relazione e chiarire l’influenza di possibili fattori confondenti.
Electronic supplementary material
The online version of this article (doi:10.1007/s40477-015-0167-0) contains supplementary material, which is available to authorized users.
Introduction
Painful shoulders are common: approximately 50 % of the population in the US experience at least one episode of shoulder pain every year [1]; the underlying pathologies are extremely varied and include tears of the rotator cuff, glenohumeral and acromioclavicular arthritis and bone marrow edema. Nonetheless, the presence of the subacromial-subdeltoid bursa (SASD) inflammation has recently been proposed as a primary radiologic factor predicting persistent limitation and pain in operated patients [2].
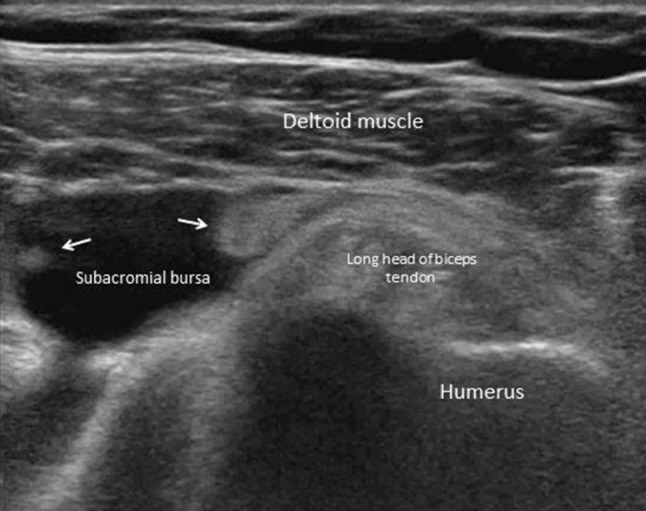
Bursae are synovial-line sacs overlying areas where structures, moving against each other, cause friction. The SASD bursa—an extra-articular synovial space—lies between the rotator cuff tendons and the undersurface of the acromion, the acromioclavicular joint and the deltoid muscle, overlying the bicipital groove [3]. It is a potential space, that appears as a hypoechoic tissue between highly reflective peribursal fat; in pathological conditions, the bursa is seen as a fluid-filled anechoic structure lined by an hyperechoic wall [4, 5]. Normally, no communication exists between the bursa and the joint; a communication is realized in full-thickness tears of the rotator cuff; SASD bursa may or may not communicate with the subcoracoid bursa.
Many pathological conditions may cause a SASD bursitis: disorders of the acromioclavicular joint, supraspinatus tendon tear, acute shoulder trauma, rheumatoid arthritis, infection, and pigmented villonodular synovitis. The aim of the study was to verify the hypothesis that pain, or increased shoulder pain, could be associated with SASD bursitis not only in operated patients [2] but also in general population.
Materials and methods
A consecutive series of 1940 shoulder ultrasound examinations were performed by our Department over a 5-year period using linear multi-frequency probes on an Acuson S2000 (Siemens, Erlangen, Germany), a Philips IU22 (Philips Medical System, The Netherlands), a GE Logic E9 (GE Healthcare, USA), and a Toshiba Aplio 500 system (Toshiba Corporation, Japan). This high number is due to the strong commitments on orthopedics and rheumatology of our institution and to a lack of trained specialists in nearby smaller centers. Attending radiologists back-scan almost all the examinations in our institution. The study has been approved by the institutional review board or comparable formal research ethics review committee. Informed consent was obtained from research subjects.
All patients were examined in the upright position, sat on the examination table. In order to observe the different shoulder structure with the optimal acoustic window and angle the position of the arm was changed during the different phases of the exam. The different positions allow the operator to obtain the right degree of tension of muscle and tendons maximizing the ultrasound diagnostic power. Different portions of the SASD bursa were examined with different arm positions: arm leaning on the tight with the palm up, and with the palm on the homolateral gluteus muscle, and arm laterally abducted with the palm up. SASD bursa was identified by using acromion, deltoid and supraspinatus muscle as landmarks. All the main components of the shoulder were separately examined. Every tendon was evaluated from the musculotendinous junction to the insertion with both transverse and longitudinal scans. Based on the anatomical situation, size, and echogenicity of the structures, the best compromise between resolution and signal penetration was empirically determined. Compound and harmonic imaging were used to improve image quality and contrast, particularly in the case of increased anisotropy.
All reports (1940) were reviewed for shoulder pain. Exclusion criteria included the presence of symptoms other than pain (e.g., instability or functional impairment) or reports with unrelated diagnoses (cutaneous or superficial soft tissue disease, e.g., sebaceous cyst). After screening, 1147 (1147/1940; 59.1 %) examinations were selected for further evaluation. The video clips were independently reviewed by two radiologists, both with 20 years of experience in ultrasound and musculoskeletal radiology. Effusion in the SASD bursa was evaluated by using a binary system (yes vs. no) and the presence of other pathological conditions was based not only on ultrasound evidence (e.g., calcific tendinopathy) but also on clinical information or other imaging techniques.
Results
In our 1105 patients, mean age was 52 years (SD 14.27); 600 were males (54.3 %). A total of 1147 shoulders were evaluated: 698 right shoulders (63.17 %) and 449 left shoulders (40.63 %).
A total of 1587 pathologies were detected; 753 (65.5 %) had only one pathology, 348 (30.4 %) had two pathologies and 46 (4.1 %) presented three pathologies.
The results are summarized in Table 1.
Table 1.
Results
| Pain; no bursal effusion | Pain; bursal effusion | p value | ||
|---|---|---|---|---|
| Acromioclavicular joint arthritis | 626 (626/1587; 39.5 %) | 185 (185/626; 29.6 %) | 441 (441/626; 70.4 %) | <0.001 |
| Acromioclavicular joint instability | 8 (8/1587; 0.5 %) | 8 (8/8; 100 %) | 0 (0/8; 0 %) | NC |
| Acromioclavicular joint tumors | 7 (7/1587; 0.4 %) | 3 (3/7; 42.9 %) | 4 (4/7; 57.1 %) | 0.707 |
| Supraspinatus calcific tendinopathy | 594 (594/1587; 37.4 %) | 191 (191/594; 32.2 %) | 403 (403/594; 67.8 %) | <0.001 |
| Full-thickness tear of supraspinatus | 60 (60/1587; 3.8 %) | 2 (2/60; 3.3 %) | 58 (58/60; 96.7 %) | <0.001 |
| Superficial tear of supraspinatus | 163 (163/1587; 10.3 %) | 48 (48/163; 29.4 %) | 115 (115/163; 70.6 %) | <0.001 |
| Deep tear of supraspinatus | 32 (32/1587; 2.0 %) | 11 (11/32; 34.4 %) | 21 (21/32; 65.6 %) | 0.082 |
| Partial tear of supraspinatus | 22 (22/1587; 1.4 %) | 6 (6/22; 27.3 %) | 16 (16/22; 72.7 %) | 0.041 |
| Calcium-related bursitis | 20 (20/1587; 1.3 %) | 0 (0/20; 0 %) | 20 (20/20; 100 %) | NC |
| Traumas | 23 (23/1587; 1.4 %) | 1 (1/23; 4.4 %) | 22 (22/23; 95.6 %) | 0.003 |
| Rheumatoid arthritis | 19 (19/1587; 1.2 %) | 1 (1/19; 5.3 %) | 18 (18/19; 94.7 %) | 0.005 |
| Infection | 6 (6/1587; 0.4 %) | 0 (0/6; 0 %) | 6 (6/6; 100 %) | NC |
| Pigmented villonodular synovitis | 2 (2/1587; 0.1 %) | 0 (0/2; 0 %) | 2 (2/2; 100 %) | NC |
| Synovial osteochondromatosis | 5 (5/1587; 0.3 %) | 1 (1/5; 20 %) | 4 (1/5; 80 %) | 0.215 |
The most frequent pathologies in patients with shoulder pain were acromioclavicular joint arthritis (39.5 %) and supraspinatus tendon calcific tendinopathy (37.4 %). All together all type of partial-thickness tear of the supraspinatus tendon are present in about 13.7 % of patients with shoulder pain and full-thickness tear of the supraspinatus tendon accounts for approximately another 3.8 %. It is important to underline that acromioclavicular joint arthritis and supraspinatus calcific tendinopathy are often associated together or with other pathologies (patients with double or triple pathologies) such as supraspinatus tendon tear.
In almost all cases, the group with pain associated with bursal effusion outnumbers the group with only pain without effusion. Pain is present only in association with effusion in infection, calcium-related bursitis and pigmented villonodular synovitis (100 % of the cases in the group presenting pain and effusion vs. 0 % in the group presenting pain without effusion).
Pain is strongly associated with effusion in some groups: full-thickness tear of supraspinatus (pain with effusion 96.7 % vs. pain without effusion 3.3 %), traumas (95.6 vs. 4.4 %), rheumatoid arthritis (94.7 vs. 5.3 %) and synovial osteochondromatosis (80 vs. 20 %).
In other cases, the trend is clearly in favor of the group with pain and effusion: acromioclavicular joint arthritis (pain with effusion 70.4 % vs. pain without effusion 29.6 %), acromioclavicular joint tumors (57.1 vs. 42.9 %), supraspinatus tendon calcific tendinopathy (67.8 vs. 32.2 %), superficial tear of the supraspinatus (70.6 vs. 29.4 %), deep tear of supraspinatus (65.6 vs. 34.4 %) and partial tear of supraspinatus (72.7 vs. 27.3 %).
Lastly, the group presenting acromioclavicular joint instability can be considered as unique because of the inversion of the ratio previously seen in the other groups. This group is characterized by the presence of pain without bursal effusion in all the cases (pain with effusion 0 % vs. pain without effusion 100 %).
The difference between the groups with and without effusion is always statistically significant for acromioclavicular joint arthritis, supraspinatus tendon calcific tendinopathy, full-thickness tear of the supraspinatus, superficial tear of the supraspinatus with a p value <0.001. The difference is also statistically significant for traumas and rheumatoid arthritis with a p value <0.01 (0.03 and 0.05, respectively). It is not significant for all the other groups.
Descriptive statistics were produced for characteristics of cases. Mean and standard deviation (SD) were presented for continuous variables, while number and percentages were presented for categorical variables. Since data represent two shoulders per patient and (potentially) multiple diagnosis per shoulder, panel data statistical models were used. In particular, logistic regression models with clustering per patient and shoulder were used to assess significance of prevalence of bursal effusion within each diagnosis.
Discussion and conclusion
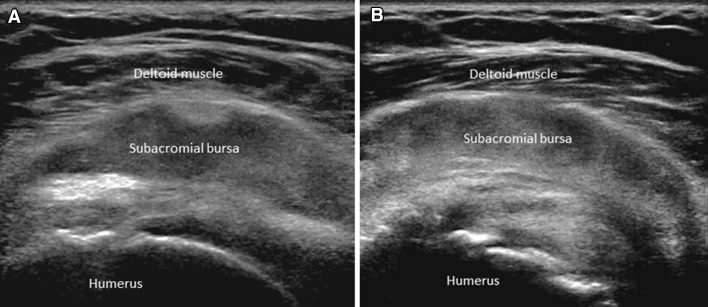
Disorders of the acromioclavicular joint including degenerative and inflammatory arthropathy, post-traumatic instability, and osteolysis, affect patients of all ages and are a common cause of shoulder pain. The clinical diagnosis of acromioclavicular pathology is difficult [6], and imaging is often necessary for the diagnosis. According to our experience, the most common cause of acromioclavicular joint pain is arthritis (Fig. 1a; ESM Video 1A). About 70 % of the patients with osteoarthritis had SASD bursitis (Fig. 1b; ESM Video 1B).
Fig. 1.

A 54-year-old women with acromioclavicular arthritis. Longitudinal sonograms demonstrates narrowing of joint space, cortical irregularity, synovial hypertrophy (a), involvement of the SASD bursa, depicted as a fluid-filled anechoic structure, and supraspinatus tendinitis (b)
Patients with acromioclavicular joint instability and tumors have frequently pain, but without any correlation with bursitis. The amount of patients representing the group is too low to draw statistically significant conclusions.
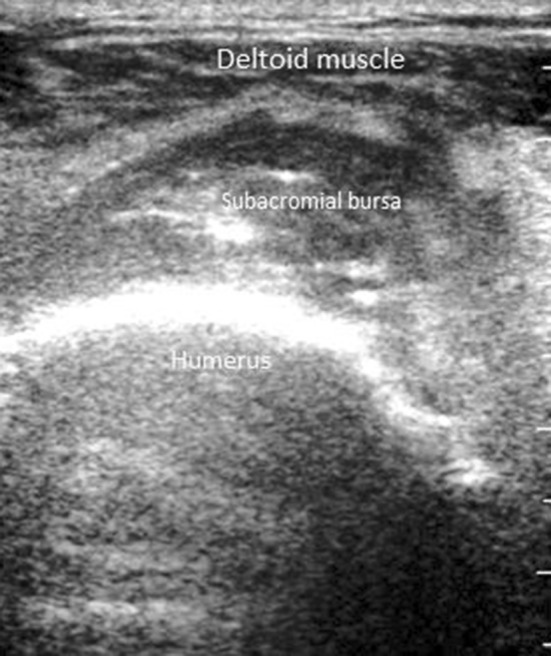
Shoulder involvement is particularly common in patients with rheumatoid arthritis. As a matter of fact, during the course of the disease 90 % of patients complain about shoulder pain at some time. In addition to the synovitis of the glenohumeral joint, involvement of more than one anatomical structure in rheumatoid arthritis is common and the most frequent causes identified in the US studies are joint effusion, rotator tendon tears—particularly the one of the subscapularis tendon—and SASD bursitis [7]. Ultrasound examination detected erosions, synovitis, tenosynovitis and bursitis (Fig. 2, ESM Video 2), thus being of great value for the diagnosis of shoulder pain in patients with rheumatoid arthritis. According to our experience, bursitis is present in more than 90 % of painful patients with rheumatoid arthritis.
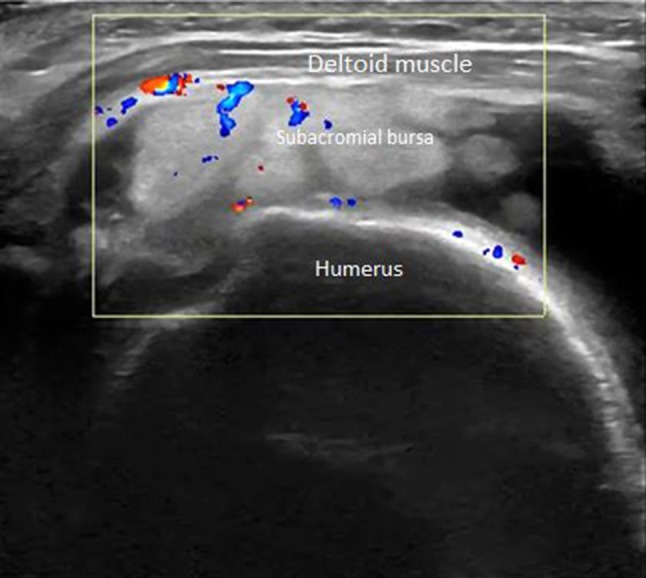
Fig. 2.
A 57-year-old women with rheumatoid arthritis. Ultrasonography shows effusion with synovial hypertrophy (arrows) in the SASD bursa
According to the literature, patients with only supraspinatus calcific tendinopathy were symptomatic in 6 % of the cases [8–10]. Patients with supraspinatus calcific tendinopathy and pain had bursitis [Fig. 1b] in 67 % of the cases. These data clearly support the hypothesis that calcification itself is frequently not painful.
A supraspinatus tendon tear may partially or totally involve tendon fibers and it is called full-thickness tear if it extends from the bursal (superficial) surface to the articular (deep) surface of the tendon. Partial-thickness tears of the supraspinatus tendon include lesions of only the superficial or deep surface and tendon central delamination [8]. The superficial or bursal surface tears are associated with bursitis (Fig. 3; ESM Video 3), when in contact with the glenohumeral joint the deep fibers tear with effusion. Full-thickness tears are associated with bursitis and glenohumeral joint effusion with communication between bursa and joint (Fig. 4; ESM Video 4) [9, 10]. Furthermore, bursitis is often a complication in the reconstruction of the supraspinatus tendon (Fig. 5; ESM Video 5).
Fig. 3.

A 43-year-old man with superficial partial tear of supraspinatus tendon. Long-axis ultrasound image of supraspinatus tendon shows bursal surface tear, filled with echoic material (arrows) and SASD bursal moderate effusion
Fig. 4.

A 55-year-old man with full-thickness tear of supraspinatus tendon. Coronal ultrasonographic view shows full-thickness tear with retraction of the fibers of the supraspinatus tendon and the communication between the SASD bursa and joint space
Fig. 5.

A 56-year-old man with reconstruction of the supraspinatus tendon. Ultrasonography shows continuity of the tendon, which is in the correct position, adequate thickness and correct tension and SASD bursitis
Occasionally in calcific tendinopathy, calcium may drain within the SASD bursa with calcium-related bursitis (Fig. 6; ESM Video 6). Calcium-related bursitis is more frequent in women, and it presents highly disabling, sharp, acute pain, usually scarcely responding to common painkillers. Our experience confirms the characteristics of this pathology as described in literature.
Fig. 6.

A 40-year-old woman with calcium-related bursitis. Ultrasonography shows hyperechoic material (calcium) within the effusion in the SASD bursa (a). Axial PD magnetic resonance image confirm the presence of calcium within the effusion (b)
Acute shoulder trauma is frequent and bursal injuries with bursitis (Figs. 7, 8, 9; ESM Videos 7, 8, 9), or even bursal rupture (Fig. 10; ESM Video 10) are common [1]. Since our hospital hosts an emergency radiology, our experience in shoulder trauma is limited to a few cases; nevertheless, in all the cases of dislocation [Figs. 9, 10] or trauma without dislocation [Figs. 7, 8], a bursitis was present and associated with painful shoulder.
Fig. 7.
A 21-year-old man with acute shoulder trauma. Keeping the patient in the upright position, sat on the examination table for several minutes, it is possible to distinguish two layers, serum (a) and blood (b) in the SASD bursa, axial plane
Fig. 8.

A 21-year-old man with acute shoulder trauma. Same case as in Fig. 7. After a week from the trauma the hematoma of the bursa appears organized
Fig. 9.

A 24-year-old man with dislocation. Hill-Sachs lesion manifested by an abrupt change in the humeral head contour at the inferior aspect of the image (arrows), associated with SASD bursitis
Fig. 10.
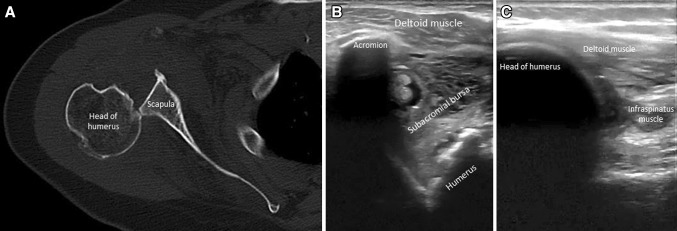
A 33-year-old women with bursal rupture. Computed tomography of posterior shoulder dislocation (a). Ultrasonography shows ruptured of distended SASD bursa (b), with posterior dislocation of humeral head (c)
Septic bursitis is commonly located in superficial bursae [11]—such as the olecranon or the bursae around the knee; infection of the SASD bursa is uncommon, with only a few cases in the literature [12]. Infections into the SASD bursa are generally associated with injection into the bursa (typically for rotator cuff tendonitis and impingement syndrome), and with trauma, while hematogenous spread is rare (immunocompromised individuals, intravenous drug abuse, tuberculosis). In our case, series septic bursitis was associated with joint effusion and pain, the liquid is particulate in 6 out of 6 cases (Fig. 11; ESM Video 11).
Fig. 11.
A 78-year-old men with septic bursitis. Ultrasound demonstrate localized particulate fluid collection within an enlarged SASD bursa
Pigmented villonodular synovitis is a rare benign tissue proliferation in synovial structures [13]. The peak of incidence is between 30 and 50 years, and both genders are affected equally. It is usually monoarticular, involving the knee in about 80 % of cases, while it has been rarely reported (in medical literature less than 40 cases, of those only two exclusively extra-articular) in other joints, including shoulder [14]. In our case series, two patients presented SASD bursa involvement (Fig. 12; ESM Video 12 A, B), but the group is too small to draw statistically significant conclusion.
Fig. 12.
A 35-year-old man with pigmented villonodular synovitis. Sonography reveals SASD bursitis with exuberant, circumscribed, hypervascularized, synovial proliferations
Synovial osteochondromatosis is an idiopathic benign metaplasia of the synovia which is rarely found in an extra-articular bursa. Its exact etiology remains unknown. The clinical manifestations include pain, tenderness and limited joint motion, all of which are nonspecific. Ultrasound examination may exclude the calcific tendinopathy of the rotator cuff and it makes the diagnosis of synovial osteochondromatosis possible [15]. The ultrasound features of synovial osteochondromatosis include well-circumscribed intra-bursal hyperechoic mass or masses (Fig. 13; ESM Video 13). Surgical removal of nodules with bursal resection is recommended if after a conservative treatment symptoms do not improve. Our study underlines that pain in patients with synovial osteochondromatosis is almost always associated with bursal effusion (80 % of the cases) which is probably the cause of the pain (the osteochondromatous nodules themselves are not the cause of the pain).
Fig. 13.

A 81-year-old women with synovial osteochondromatosis. Sonograms show arc-shaped bright interface with acoustic shadowing and effusion in the SASD bursa
Our study has several limitations: it spans over a long period of time, and several equipments were utilized. This sometimes has created “technology bias” such as the visibility of a physiologic amount of fluid into the SASD bursa with more recent US scanner. No quantitative cutoff values for normal/abnormal fluid were set, but only semi quantitative evaluations were performed (with consensus among readers for the most challenging cases). Nevertheless, the main limitation is probably the absence of a suitable control group. If we take into account the fact that this is a retrospective study and that in our country, only symptomatic patients generally undergo US examinations, we can conclude that the identification of a control group is quite impossible. The best option would be having a group without pain to evaluate the presence of SASD bursal effusion, but this case is extremely rare since pain is almost the only indicator to shoulder ultrasound examination (besides post-surgical controls). To overcome this bias, we are working to create a prospective study protocol which includes for every patients the analysis of the other (non-painful) shoulder. This data are nonetheless in an extremely early phase.
Our clinical study shows that the effusion in the SASD bursa is frequently associated with shoulder pain, often independently from the underlying pathology; further studies are needed to confirm the statistical significance of this relationship by clarifying possible confounding factors.
Electronic supplementary material
Supplementary material 11: Video 10 Bursal rupture (after dislocation) (MPG 1092 kb)
Supplementary material 12: Video 11 Septic bursitis (MPG 2846 kb)
Supplementary material 14: Video 12B Pigmented villonodular synovitis—Color Doppler (MPG 2494 kb)
Supplementary material 13: Video 12A Pigmented villonodular synovitis—B-Mode (MPG 2276 kb)
Supplementary material 1: Video 1A Acromioclavicular joint arthritis (MPG 1772 kb)
Supplementary material 2: Video 1B Osteoarthritis and SASD bursitis (MPG 1782 kb)
Supplementary material 3: Video 2 Rheumatoid arthritis (MPG 1312 kb)
Supplementary material 4: Video 3 Partial supraspinatus tendon tear (MPG 2118 kb)
Supplementary material 5: Video 4 Complete supraspinatus tendon tear (MPG 864 kb)
Supplementary material 6: Video 5 Bursitis as a complication in the reconstruction of the supraspinatus tendon (MPG 664 kb)
Supplementary material 7: Video 6 Calcium-related bursitis (MPG 858 kb)
Supplementary material 8: Video 7 Acute shoulder trauma (MPG 4670 kb)
Supplementary material 9: Video 8 Acute shoulder trauma (MPG 598 kb)
Supplementary material 10: Video 9 Acute shoulder trauma (Hill-Sachs lesion) (MPG 998 kb)
Conflict of interest
The authors have nothing to disclose.
Ethical standards
Studies have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
References
- 1.Chalian M, Soldatos T, Faridian-Aragh N, et al. MR evaluation of synovial injury in shoulder trauma. Emerg Radiol. 2011;18(5):395–402. doi: 10.1007/s10140-011-0973-4. [DOI] [PubMed] [Google Scholar]
- 2.Collin P, Abdullah A, Kherad O, Gain S, Denard PJ, Lädermann A. Prospective evaluation of clinical and radiologic factors predicting return to activity within 6 months after arthroscopic rotator cuff repair. J Shoulder Elbow Surg. 2014 doi: 10.1016/j.jse.2014.08.014. [DOI] [PubMed] [Google Scholar]
- 3.Hirji Z, Hunjun JS, Choudur HN. Imaging of the bursae. J Clin Imaging Sci. 2011;1:22. doi: 10.4103/2156-7514.80374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jacobson JA. Shoulder US: anatomy, technique, and scanning pitfalls. Radiology. 2011;260(1):6–16. doi: 10.1148/radiol.11101082. [DOI] [PubMed] [Google Scholar]
- 5.Precerutti M, Garioni E, Madonia L, Draghi F. US anatomy of the shoulder: pictorial essay. J Ultrasound. 2010;13(4):179–187. doi: 10.1016/j.jus.2010.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cadogan A, McNair P, Laslett M, Hing W. Shoulder pain in primary care: diagnostic accuracy of clinical examination tests for non-traumatic acromioclavicular joint pain. BMC Musculoskelet Disord. 2013;14:156. doi: 10.1186/1471-2474-14-156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kim HA, Kim SH, Seo YI. Ultrasonographic findings of the shoulder in patients with rheumatoid arthritis and comparison with physical examination. J Korean Med Sci. 2007;22(4):660–666. doi: 10.3346/jkms.2007.22.4.660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Guerini H, Fermand M, Godefroy D et al (2012) US appearance of partial-thickness supraspinatus tendon tears: application of the string theory. Pictorial essay. J Ultrasound 15(1):7–15 [DOI] [PMC free article] [PubMed]
- 9.Arslan G, Apaydin A, Kabaalioglu A, Sindel T, Lüleci E (1999) Sonographically detected subacromial/subdeltoid bursal effusion and biceps tendon sheath fluid: reliable signs of rotator cuff tear? J Clin Ultrasound 27(6):335–339 [DOI] [PubMed]
- 10.Hodgson RJ, O’Connor PJ, Hensor EM, Barron D, Robinson P. Contrast-enhanced MRI of the subdeltoid, subacromial bursa in painful and painless rotator cuff tears. Br J Radiol. 2012;85(1019):1482–1487. doi: 10.1259/bjr/45423226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Costantino TG, Roemer B, Leber EH. Septic arthritis and bursitis: emergency ultrasound can facilitate diagnosis. J Emerg Med. 2007;32(3):295–297. doi: 10.1016/j.jemermed.2006.08.012. [DOI] [PubMed] [Google Scholar]
- 12.Khan H, Al-Tawil K. Spontaneous isolated infection of the subacromial bursa. Case Rep Orthop. 2013 doi: 10.1155/2013/564690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chiang ER, Ma HL, Wang ST, Hung SC, Chen TH. Arthroscopic treatment for pigmented villonodular synovitis of the shoulder associated with massive rotator cuff tear. Arthroscopy. 2009;25(7):716–721. doi: 10.1016/j.arthro.2009.01.007. [DOI] [PubMed] [Google Scholar]
- 14.Madruga Dias J, Costa MM, Duarte A, Pereira da Silva JA (2013) Localized pigmented villonodular synovitis of the shoulder: a rare presentation of an uncommon pathology. Acta Med Port 26(4):459–462 [PubMed]
- 15.Kim TK, Lee DH, Park JH, Kim CH, Jeong WK. Synovial osteochondromatosis in the subacromial bursa mimicking calcific tendinitis: sonographic diagnosis. J Clin Ultrasound. 2014;42(4):237–240. doi: 10.1002/jcu.22097. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary material 11: Video 10 Bursal rupture (after dislocation) (MPG 1092 kb)
Supplementary material 12: Video 11 Septic bursitis (MPG 2846 kb)
Supplementary material 14: Video 12B Pigmented villonodular synovitis—Color Doppler (MPG 2494 kb)
Supplementary material 13: Video 12A Pigmented villonodular synovitis—B-Mode (MPG 2276 kb)
Supplementary material 1: Video 1A Acromioclavicular joint arthritis (MPG 1772 kb)
Supplementary material 2: Video 1B Osteoarthritis and SASD bursitis (MPG 1782 kb)
Supplementary material 3: Video 2 Rheumatoid arthritis (MPG 1312 kb)
Supplementary material 4: Video 3 Partial supraspinatus tendon tear (MPG 2118 kb)
Supplementary material 5: Video 4 Complete supraspinatus tendon tear (MPG 864 kb)
Supplementary material 6: Video 5 Bursitis as a complication in the reconstruction of the supraspinatus tendon (MPG 664 kb)
Supplementary material 7: Video 6 Calcium-related bursitis (MPG 858 kb)
Supplementary material 8: Video 7 Acute shoulder trauma (MPG 4670 kb)
Supplementary material 9: Video 8 Acute shoulder trauma (MPG 598 kb)
Supplementary material 10: Video 9 Acute shoulder trauma (Hill-Sachs lesion) (MPG 998 kb)