

Abstract
AIM: To study the levels of 5-fluorouracail (5-FU) in plasma, liver and tumor in patients with hepatocellular carcinoma after oral administration of 5’-deoxy-5-fluorouridine (5’-DFUR).
METHODS: Thirty-nine patients with hepatocellular carcinoma were treated with oral 5’-DFUR for more than 4 d before operation. The contents of 5-FU in plasma, liver and tumor were measured by high performance liquid chromatography (HPLC) and apoptosis of tumor cells was evaluated by in-situ TUNEL after resection of tumor.
RESULTS: The concentrations of 5-FU were 1.1 μg/mL, 5.6, 5.9, and 10.5 μg/g in plasma, the liver tissue, the center of tumor and the periphery of tumor, respectively. 5-FU concentration was significantly higher in the periphery of tumor than that in the liver tissue and the center of tumor (10.5 ± 1.6 μg/g vs 5.6 ± 0.8 μg/g, t = 21.38, P < 0.05; 10.5 ± 1.6 μg/g vs 5.9 ± 0.9 μg/g, t = 20.07, P < 0.05). 5-FU level was significantly lower in plasma than that in the liver and the tumor (1.1 ± 0.3 μg/mL vs 5.6 ± 0.8 μg/g, t = 19.63, P < 0.05; 1.1 ± 0.3 μg/mL vs 10.5 ± 1.6 μg/g, t = 41.01, P < 0.05). Apoptosis of tumor cells was significantly increased after oral 5’-DFUR compared to the control group without 5’-DFUR treatment.
CONCLUSION: There is a higher concentration of 5-FU distributed in the tumor compared with liver tissue and apoptosis of tumor cells is increased following oral 5’-DFUR compared with the control group. The results indicate that 5’-DFUR is hopeful as neo-adjuvant chemotherapy to prevent recurrence after resection of hepatocellular carcinoma.
Keywords: Hepatocellular carcinoma, 5’-Deoxy-5-fluorouridine, 5-Fluorouracail, Apoptosis
INTRODUCTION
Hepatocellular carcinoma (HCC) remains one of the most common neoplasms in the world[1,2]. 5’-Deoxy-5-fluorouridine (5’-DFUR) is an oral fluoropyrimidine derivative and it is converted to 5-fluorouracil (5-FU) by Pyrimidine nucleoside phosphorylase (PyNPase) which is expressed with higher level in tumor tissues compared with normal tissues[3,4]. Oral 5-FU derivatives have shown comparable antitumor activity and long-term oral administration of low-dose has been considered as postoperative adjuvant chemotherapy after curative resection of the cancer to reduce recurrence and improve survival rate[5-9]. The selective antitumor activity of 5’DFUR is correlated with PyNPase activity in tumor[10]. Although the activity of 5-FU in tumor is well recognized, resistance to this agent is frequently observed and remains its major limitation. It was reported that doxifluridine still showed antitumor activity to tumor cells which were resistant to 5-FU[11].
The purpose of the present study was to investigate the impact of preoperative oral 5’-DFUR on distribution of 5-FU in plasma, liver and tumor and apoptosis of tumor cells in patients with hepatocellular carcinoma.
MATERIALS AND METHODS
Chemicals and reagents
5’-DFUR capsule (Furtulon) was produced by Shanghai Roche Pharmaceuticals Co. (Shanghai, China), and standard 5-FU was provided by Sigma Chemicals Co. (USA). Methyl-tert butyl ether, acetonitrile, methanol (HPLC grade) and potassium hydrogen phosphate (AR grade) were purchased from Peking Chemical Plant (Beijing, China).
Chromatographic conditions
HPLC system consisted of LC-10AT HPLC pump and SPD-10A Detector (SHIMADZU Co. Japan). The analytical column was Kromasil C18 (5 μm 200 mm × 4.6 mm ID). The mobile phase consisted of acetonitrile, methanol, and 0.25 mol/L potassium hydrogen phosphate (1:4:5). The flow rate was 1.0 mL/min and the wavelength was at 265 nm.
Collection of samples
Thirty-nine patients of 27 male and 12 female with hepatocellular carcinoma were included in this study. Their average age was 49.1 years and the diamters of tumors were from 5 to 7 cm. 5’-DFUR was administered orally and preoperatively (1 200 daily for more than 4 d before operation and 400 mg on the day of operation). The mean total dosage was 6.4 g. Blood sample and specimens of the normal liver tissue and the tumor tissue were collected 3-5 h after final administration. The liver and tumor tissues were cleaned by distilled water and blotted by filter paper. One gram tissue was weighed accurately and 4 mL distilled water was added to the container to crush the tissue. The blood samples and the crushed tissues were centrifuged, and 1 mL plasma or aqueous layer sample was then stored under -20°C.
Extraction and determination of samples
Each 0.5 mL plasma or aqueous layer sample was added and mixed with 0.1 mL of potassium hydrogen phosphate (0.5 mol/L), followed by the addition of 5 mL methyl-tert butyl ether to each tube. The tube was then capped and shaken for 10 min on a shaker. The aqueous layer and the organic layer were separated by centrifugation at 3 000 r/min for 10 min. The aqueous layer was transferred to a clean test tube and evaporated to dryness under gentle stream of nitrogen at 50°C. The residue was dissolved with 0.1 mL of mobile phase and vortexed. Then the sample was transferred into a micro-spin filter tube and was centrifuged at 3 000 r/min for 10 min. The filtrate was collected and the injection volume was 20 μL and the content of 5-FU was measured by high performance liquid chromatography (HPLC)[12-14].
In vivo detection of apoptosis
TUNEL staining was used to detect DNA degradation in situ in the relatively late stage of apoptosis. Apoptotic cells were labeled by the TUNEL reaction using an in situ Cell Apoptosis Detection Kit. In situ Cell Apoptosis Detection Kits were purchased from Roche Diagnostics GmbH Co. in Germany. The detailed manipulation was conducted according to instructions for users. The procedure was performed following the instructions of the manufacturer and in reference of the previous observations[15,16].
The positive cells were identified and analyzed based on morphological characteristics of apoptotic cells as previously described. Under the fluorescence microscopy, apoptotic cells manifested as brownish staining in the nuclei. Non-necrotic zone was selected in the tissue section and images were randomly selected. The positive cells were determined in at least five areas at ×400 magnification and divided into three categories as follows: (+) only sporadic positive cells were detected; (++) a cluster of apoptotic cells were observed; (+++) positive cells in a large scale or multi-cluster apoptotic cells were seen in representative tissue sections of each individual case. Twenty patients of HCC without oral 5’-DFUR treatment were included as the control group.
Statistical analysis
The data were expressed as mean±SD. Student’s t-test was performed for statistical analysis. P value less than 0.05 was considered statistically significant.
RESULTS
Concentration of 5-FU in plasma, liver and tumor following oral administration of 5’-DFUR
The concentrations of 5-FU were 1.1 μg/mL, 5.6, 5.9, and 10.5 μg/g in plasma, the liver tissue, the center of tumor and the periphery of tumor, respectively. The 5-FU content was significantly higher in the periphery of tumor than that in the liver tissue and the center of tumor (P < 0.05). Moreover, the 5-FU concentration was significantly lower in plasma than liver and tumor (P < 0.05). However, the 5-FU level in the center of tumor was similar to that in the liver tissue (Table 1).
Table 1.
5-FU concentrations in blood, liver and tumor after oral 5’-DFUR
| Tissue | Level of 5-FU |
| Plasma (µg/mL) | 1.1 ± 0.3a |
| Liver tissue (µg/g) | 5.6 ± 0.8 |
| Central tissue of tumor (µg/g) | 5.9 ± 0.9 |
| Periphery tissue of tumor (µg/g) | 10.5 ± 1.6a |
P < 0.05 vs 5-FU concentration in liver tissue.
Apoptosis of the tumor cell demonstrated by TUNEL
Under the fluorescence microscope, apoptotic cells manifested as brownish staining in the nuclei. The degree of apoptosis was shown + in tissue sections of the control group in which sporadic positive cells were detected, and ++ in cases with oral 5’-DFUR in which clusters of apoptotic cells were seen (Figures 1A and B).
Figure 1.
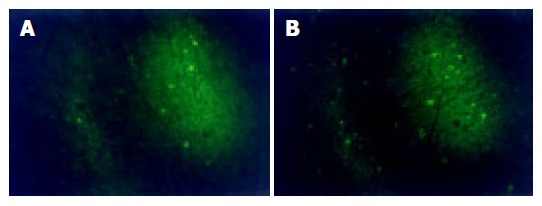
Apoptotic cancer cells detected by TUNEL method after oral administration of 5’-DFUR ×400. A: Sporadic apoptotic cells were detected; B: clusters of apoptotic cells were detected.
DISCUSSION
It is well known that hepatocellular carcinoma is one of the malignant tumors with poor chemosensitivity to anticancer agents[17,18]. 5-FU is still the first choice for the chemotherapy of hepatocellular carcinoma[19,20], because of its strong killing effects on the cancer cells. 5-FU can damage proliferating cells, reduce the tumor mass in size and prevent tumor cells from spreading and metastasis. However, its usage is limited due to the rapid development of acquired resistance. The effects of 5-FU are not so satisfactory because 5-FU has a lower concentration in tumor tissue and relatively higher concentrations in blood after intravenous administration of 5-FU. Moreover, its side effects are serious and many patients are unable to tolerate.
5’-DFUR is a prodrug of 5-FU and it is converted to 5-FU by Pyrimidine nucleoside phosphorylase (PyNPase). PyNPase exists in all kinds of tumor tissues and its expression and activity in tumor tissue are higher than that in normal tissue[3,4]. Nagata et al[21-24] reported that transfection of PyNPase gene into tumor cell can increase the sensitivity to 5’-DFUR, and thereby decreases the toxicity of the agent. In our study, it had been found that 5-FU level in tumor was 10 times higher than in plasma and 5-FU level was significantly higher in the periphery of tumor than in the liver tissue. The results suggested that more 5-FU was converted and accumulated within tumor tissue. This difference may be related to the higher PyNPase expression and activity in hepatocellular carcinoma. It had also been found that the 5-FU level was significantly higher in the periphery of tumor than the center of tumor. There was more 5-FU accumulated and converted in the periphery of tumor following oral 5’-DFUR administration. Oxygen, nutrition and growth factors were not equally distributed within the tumor tissue. Oxygen and nutrient of the central tumor tissue are supplied mainly by hepatic artery, and proliferation of the tumor in this region is slower and even partial necrosis appears. However, the periphery of tumor has effluent blood flow supplied by hepatic artery and portal vein, so the tumor cells can grow more rapidly. These results may indicate that large liver tumor is not sensitive to 5’-DFUR.
Oral 5’-DFUR is very convenient and its side effect is slight[6]. The drug arrives in the liver firstly after being absorbed by the intestine. So most of 5’-DFUR can be converted to 5-FU in the liver or the liver tumor and accumulated in these tissues with higher concentration than that administered by iv approach. In this study, the 5-FU level in peripheral vein was only one-tenth of that in tumor tissue. 5-FU can be maintained at a certain level within the tumor tissue but not accumulated in the peripheral vein after regular oral administration of 5’-DFUR.
The expression and activity of PyNPase is higher in the tumor with vascular permeation and lymph node metastasis[4,25,26]. Akao et al[27] reported that PyNPase activity was significantly higher in metastatic lymph node. Tazawa et al[28] found that 5’-DFUR could inhibit hepatic metastasis of tumor, which would be effective for the prophylactic treatment of metastatic disease. These indicate that PyNPase activity appears to be a new useful parameter for identifying both a poor prognosis and a highly malignant potential of tumor and 5’-DFUR is preferably sensitive in cancer patients with lymph node metastasis and vascular infiltration. 5-DFUR is still effective to the tumor which is resistant to 5-FU therapy[11]. Monden et al[29] found that vessel density and stage of tumor were correlated with expression of PyNPase which showed prognosis. 5-DFUR not only is effective on primary tumor and metastatic lesion but also suitable to postoperative prevention of tumor. Apoptosis of the tumor was enhanced after oral administration of 5’-DFUR. In this study, it was found that there were more apoptosis cells in the tumor after oral administration of 5’-DFUR.
In summary, our results showed that there was a higher concentration of 5-FU accumulated in the tumor tissue compared with liver tissue and apoptosis of the tumor cells was increased after oral administration of 5’-DFUR. 5’-DFUR is a hopeful agent for neo-adjuvant chemotherapy to prevent recurrence after resection of hepatocellular carcinoma.
Footnotes
Science Editor Guo SY Language Editor Elsevier HK
References
- 1.Yu MC, Yuan JM, Govindarajan S, Ross RK. Epidemiology of hepatocellular carcinoma. Can J Gastroenterol. 2000;14:703–709. doi: 10.1155/2000/371801. [DOI] [PubMed] [Google Scholar]
- 2.El-Serag HB. Hepatocellular carcinoma: an epidemiologic view. J Clin Gastroenterol. 2002;35:S72–S78. doi: 10.1097/00004836-200211002-00002. [DOI] [PubMed] [Google Scholar]
- 3.Kobayashi N, Kubota T, Watanabe M, Otani Y, Teramoto T, Kitajima M. Pyrimidine nucleoside phosphorylase and dihydropyrimidine dehydrogenase indicate chemosensitivity of human colon cancer specimens to doxifluridine and 5-fluorouracil, respectively. J Infect Chemother. 1999;5:144–148. doi: 10.1007/s101560050024. [DOI] [PubMed] [Google Scholar]
- 4.Hiroyasu S, Shiraishi M, Samura H, Tokashiki H, Shimoji H, Isa T, Muto Y. Clinical relevance of the concentrations of both pyrimidine nucleoside phosphorylase (PyNPase) and dihydropyrimidine dehydrogenase (DPD) in colorectal cancer. Jpn J Clin Oncol. 2001;31:65–68. doi: 10.1093/jjco/hye014. [DOI] [PubMed] [Google Scholar]
- 5.Ito K, Okushiba S, Morikawa T, Kondo S, Katoh H. [Appropriate duration of postoperative oral adjuvant chemotherapy with HCFU for colorectal cancer] Gan To Kagaku Ryoho. 2004;31:55–59. [PubMed] [Google Scholar]
- 6.Min JS, Kim NK, Park JK, Yun SH, Noh JK. A prospective randomized trial comparing intravenous 5-fluorouracil and oral doxifluridine as postoperative adjuvant treatment for advanced rectal cancer. Ann Surg Oncol. 2000;7:674–679. doi: 10.1007/s10434-000-0674-9. [DOI] [PubMed] [Google Scholar]
- 7.André T, Boni C, Mounedji-Boudiaf L, Navarro M, Tabernero J, Hickish T, Topham C, Zaninelli M, Clingan P, Bridgewater J, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med. 2004;350:2343–2351. doi: 10.1056/NEJMoa032709. [DOI] [PubMed] [Google Scholar]
- 8.Takiguchi N, Fujimoto S, Koda K, Oda K, Okui K, Nakajima N, Miyazaki M. Postoperative adjuvant chemotherapy is effective in gastric cancer with serosal invasion: significance in patients chosen for multivariate analysis. Oncol Rep. 2002;9:801–806. [PubMed] [Google Scholar]
- 9.Zhou J, Tang ZY, Fan J, Wu ZQ, Ji Y, Xiao YS, Shi YH, Li XM, Sun QM, Liu YK, et al. Capecitabine inhibits postoperative recurrence and metastasis after liver cancer resection in nude mice with relation to the expression of platelet-derived endothelial cell growth factor. Clin Cancer Res. 2003;9:6030–6037. [PubMed] [Google Scholar]
- 10.Hata Y, Takahashi H, Sasaki F, Ogita M, Uchino J, Yoshimoto M, Akasaka Y, Nakanishi Y, Sawada Y. Intratumoral pyrimidine nucleoside phosphorylase (PyNPase) activity predicts a selective effect of adjuvant 5'-deoxy-5-fluorouridine (5'DFUR) on breast cancer. Breast Cancer. 2000;7:37–41. doi: 10.1007/BF02967186. [DOI] [PubMed] [Google Scholar]
- 11.Bajetta E, Di Bartolomeo M, Somma L, Del Vecchio M, Artale S, Zunino F, Bignami P, Magnani E, Buzzoni R. Doxifluridine in colorectal cancer patients resistant to 5-fluorouracil (5-FU) containing regimens. Eur J Cancer. 1997;33:687–690. doi: 10.1016/s0959-8049(96)00491-1. [DOI] [PubMed] [Google Scholar]
- 12.Zufía L, Aldaz A, Castellanos C, Giráldez J. Determination of 5-fluorouracil and its prodrug tegafur in plasma and tissue by high-performance liquid chromatography in a single injection: validation for application in clinical pharmacokinetic studies. Ther Drug Monit. 2003;25:221–228. doi: 10.1097/00007691-200304000-00013. [DOI] [PubMed] [Google Scholar]
- 13.Nassim MA, Shirazi FH, Cripps CM, Veerasinghan S, Molepo MJ, Obrocea M, Redmond D, Bates S, Fry D, Stewart DJ, et al. An HPLC method for the measurement of 5-fluorouracil in human plasma with a low detection limit and a high extraction yield. Int J Mol Med. 2002;10:513–516. [PubMed] [Google Scholar]
- 14.Ozawa S, Hamada M, Murayama N, Nakajima Y, Kaniwa N, Matsumoto Y, Fukuoka M, Sawada J, Ohno Y. Cytosolic and microsomal activation of doxifluridine and tegafur to produce 5-fluorouracil in human liver. Cancer Chemother Pharmacol. 2002;50:454–458. doi: 10.1007/s00280-002-0528-1. [DOI] [PubMed] [Google Scholar]
- 15.Xu Y, Kajimoto S, Nakajo S, Nakaya K. Beta-hydroxyisovalerylshikonin and cisplatin act synergistically to inhibit growth and to induce apoptosis of human lung cancer DMS114 cells via a tyrosine kinase-dependent pathway. Oncology. 2004;66:67–75. doi: 10.1159/000076337. [DOI] [PubMed] [Google Scholar]
- 16.Barnett KT, Fokum FD, Malafa MP. Vitamin E succinate inhibits colon cancer liver metastases. J Surg Res. 2002;106:292–298. doi: 10.1006/jsre.2002.6466. [DOI] [PubMed] [Google Scholar]
- 17.Huesker M, Folmer Y, Schneider M, Fulda C, Blum HE, Hafkemeyer P. Reversal of drug resistance of hepatocellular carcinoma cells by adenoviral delivery of anti-MDR1 ribozymes. Hepatology. 2002;36:874–884. doi: 10.1053/jhep.2002.35619. [DOI] [PubMed] [Google Scholar]
- 18.Warmann S, Göhring G, Teichmann B, Geerlings H, Pietsch T, Fuchs J. P-glycoprotein modulation improves in vitro chemosensitivity in malignant pediatric liver tumors. Anticancer Res. 2003;23:4607–4611. [PubMed] [Google Scholar]
- 19.Tono T, Hasuike Y, Ohzato H, Takatsuka Y, Kikkawa N. Limited but definite efficacy of prophylactic hepatic arterial infusion chemotherapy after curative resection of colorectal liver metastases: A randomized study. Cancer. 2000;88:1549–1556. [PubMed] [Google Scholar]
- 20.Guo WJ, Yu EX. Evaluation of combined therapy with chemoembolization and irradiation for large hepatocellular carcinoma. Br J Radiol. 2000;73:1091–1097. doi: 10.1259/bjr.73.874.11271902. [DOI] [PubMed] [Google Scholar]
- 21.Nagata T, Nakamori M, Iwahashi M, Yamaue H. Overexpression of pyrimidine nucleoside phosphorylase enhances the sensitivity to 5'-deoxy-5-fluorouridine in tumour cells in vitro and in vivo. Eur J Cancer. 2002;38:712–717. doi: 10.1016/s0959-8049(01)00469-5. [DOI] [PubMed] [Google Scholar]
- 22.Evrard A, Cuq P, Ciccolini J, Vian L, Cano JP. Increased cytotoxicity and bystander effect of 5-fluorouracil and 5-deoxy-5-fluorouridine in human colorectal cancer cells transfected with thymidine phosphorylase. Br J Cancer. 1999;80:1726–1733. doi: 10.1038/sj.bjc.6690589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kanyama H, Tomita N, Yamano T, Miyoshi Y, Ohue M, Fujiwara Y, Sekimoto M, Sakita I, Tamaki Y, Monden M. Enhancement of the anti-tumor effect of 5'-deoxy-5-fluorouridine by transfection of thymidine phosphorylase gene into human colon cancer cells. Jpn J Cancer Res. 1999;90:454–459. doi: 10.1111/j.1349-7006.1999.tb00769.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Evrard A, Cuq P, Robert B, Vian L, Pèlegrin A, Cano JP. Enhancement of 5-fluorouracil cytotoxicity by human thymidine-phosphorylase expression in cancer cells: in vitro and in vivo study. Int J Cancer. 1999;80:465–470. doi: 10.1002/(sici)1097-0215(19990129)80:3<465::aid-ijc21>3.0.co;2-6. [DOI] [PubMed] [Google Scholar]
- 25.Yamagata M, Mori M, Mimori K, Mafune KI, Tanaka Y, Ueo H, Akiyoshi T. Expression of pyrimidine nucleoside phosphorylase mRNA plays an important role in the prognosis of patients with oesophageal cancer. Br J Cancer. 1999;79:565–569. doi: 10.1038/sj.bjc.6690089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mimori K, Ueo H, Shirasaka C, Shiraishi T, Yamagata M, Haraguchi M, Mori M. Up-regulated pyrimidine nucleoside phosphorylase in breast carcinoma correlates with lymph node metastasis. Ann Oncol. 1999;10:111–113. doi: 10.1023/a:1008399306583. [DOI] [PubMed] [Google Scholar]
- 27.Akao S, Inoue K. [PyNPase and DPD expression potentially predict response to 5'-DFUR treatment for node-positive breast cancer patients] Gan To Kagaku Ryoho. 2003;30:1361–1364. [PubMed] [Google Scholar]
- 28.Tazawa K, Sakamoto T, Kuroki Y, Yamashita I, Okamoto M, Katuyama S, Fujimaki M. Inhibitory effects of fluorinated pyrimidines, 5'-DFUR, UFT and T-506, in a model of hepatic metastasis of mouse colon 26 adenocarcinoma-assessment of inhibitory activity and adverse reactions at the maximum tolerated dose. Clin Exp Metastasis. 1997;15:266–271. doi: 10.1023/a:1018425532296. [DOI] [PubMed] [Google Scholar]
- 29.Monden T, Haba A, Amano M, Kanoh T, Tsujie M, Ikeda K, Izawa H, Ohnishi T, Sekimoro M, Tomita N, et al. [PyNPase expression and cancer progression in the colorectum] Nihon Geka Gakkai Zasshi. 1998;99:446–451. [PubMed] [Google Scholar]