

Abstract
Background:
Geographic and doctor-to-doctor variations in care are a focus of quality and safety efforts in medicine. This study addresses factors associated with variation in the rate of operative treatment of de Quervain tendinopathy.
Methods:
We used a database including all patient encounters at 2 large medical centers, to study the experience of 10 hand surgeons and 1 physiatrist working in a hand surgery office in the treatment of 2,513 patients with de Quervain tendinopathy over a 12-year period. Survival analysis using the Kaplan-Meier method was used to compare surgery rates and time to surgery. Cox multivariable regression analysis was applied to identify factors associated with operative treatment.
Results:
One hundred ninety nine (7.9%) patients had surgery. The odds of operative treatment were 1.7 times greater after corticosteroid injection and varied more than 10-fold among providers. There was substantial variation in the overall rate of surgery by provider. Corticosteroid injection delayed surgery slightly, but was associated with a higher rate of surgery.
Conclusion:
Providers have substantial influence on treatment of de Quervain tendinopathy. The use of decision aids and other methods that help involve the patient in decision-making merit investigation as interventions to help reduce doctor-to-doctor variation.
Keywords: Cortisone injection, De Quervain tendinopathy, Decision aid, Operative treatment, Variation
Introduction
The prevalence of de Quervain tendinopathy is 1.3-2.1% in women and 0.5-0.6% in men (1, 2). Surgery is the only known disease-modifying treatment. There is insufficient evidence to determine if corticosteroid injection alters the natural history (3). All other treatments are palliative.
De Quervain tendinopathy may be a self-limited condition with no long-term consequences and surgery is discretionary. The substantial geographical variation in rate of surgery is generally higher for discretionary surgery (4-6). Unexplained variation in surgery rates suggests opportunities for improved quality and safety of care (7). A better understanding of the variation in surgery rate for common, benign hand illnesses such as de Quervain tendinopathy is a first step in developing interventions to improve the value of hand surgery.
This study addressed the primary null hypothesis that there are no factors associated with operative treatment of de Quervain tendinopathy. We also addressed the rate of surgery over time by provider.
Methods
Study population
In this institutional review board approved study, we used the institutional database from 2 large academic medical centers from January 2001 to June 2013 to retrospectively identify patients with an International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) diagnosis code of de Quervain tendinopathy (727.04). The first visit was set as the time of diagnosis without taking into account any prior care by the primary care doctor or specialists not at one of our hospitals. The date of first corticosteroid injection, the date of operation, and the time elapsed from the first visit to operation were recorded. We attributed injection to de Quervain given that injection was offered at or after diagnosis date and before operation date. Two hundred and seven patients with a history of prior surgery for de Quervain tendinopathy at the time of first visit were excluded, leaving 2,513 patients with de Quervain tendinopathy with treatment rendered by 11 different providers for analysis. We arbitrarily set provider 1 as a reference to be compared with the other providers. The physiatrist was set as provider 11. Patients under her care that had subsequent surgery were credited to her in the analysis.
Statistical analysis
We conducted a survival analysis starting at the time of diagnosis of de Quervain tendinopathy with operative treatment as an endpoint.
Continuous data were reported as means±standard deviation after testing the normality using a 1-sample Kolmogorov-Smirnov test. Categorical data were presented as absolute values and percentages. The clinical characteristics of the two groups (operative versus non-operative) were compared with the use of the independent samples t-test for continuous variables and the Chi-Square test for categorical variables if normally distributed and Kruskal-Wallis one-way ANOVA if the distribution was not normal. Survival analysis was performed using the Kaplan-Meier method and compared using the log-rank test for age, race, sex, cortisone injection and providers. Variables were inserted into a Cox multivariable regression analysis to identify factors associated with operative treatment.
Results
One hundred ninety nine of 2,513 (7.9%) patients with the mean age of 50±13 and the age range from 17 to 87 years had surgery within our hospitals during the study period. Only 8 of the 199 patients (4.0%) had surgery by a provider that did not make the initial diagnosis. The provider with the highest rate of surgery operated on 25% of patients. Two patients in the physiatrist’s service underwent surgery by another provider whereas both had prior corticosteroid injection. In bivariate analysis, the only factors associated with operative treatment were specific provider and corticosteroid injection [Table 1]. In the multivariable analysis, the odds of operative treatment were 1.7 times greater after corticosteroid injection and varied more than 10-fold among the nine providers who treated at least some of their patients with surgery [Table 2]. There was substantial variation in the time to surgery (P=0.035) and overall rate of surgery by provider (P<0.001) [Figures 1; 2]. There was significant variation amongst providers in regards to treatment with injection varied from 9% to 62% of patients (P<0.001). The rate of surgery over the years of the study was correlated with the number of patients diagnosed with de Quervain tendinopathy [Table 3]. Corticosteroid injection delayed surgery slightly, but was associated with a higher rate of surgery [Figure 3]. There was no correlation between the rate of injection and the rate of operation among providers [Figure 4].
Table 1.
Characteristics of patients with de Quervain’s tendinopathy between operated and non-operated groups (n=2,513)
| Characteristics | Total | Surgery | P-value¥ | |
|---|---|---|---|---|
| No (n=2314) | Yes (n=199) | |||
| Age, mean±SD, (Range) | 49±15 (14-93) | 49±15 (14-93) | 50±13 (17-87) | 0.37* |
| Sex, no. (%) | ||||
| Women | 2038 (81) | 1876 (92) | 162 (8.0) | 0.91^ |
| Men | 475 (19) | 438 (92) | 37 (8.0) | |
| Race, no. (%) | ||||
| White | 1730 (69) | 1583 (92) | 147 (8.0) | 0.11^ |
| Black | 271 (11) | 251 (93) | 20 (7.0) | |
| Asian | 144 (5.5) | 139 (97) | 5 (3) | |
| Hispanic | 200 (8.0) | 184 (92) | 16 (8.0) | |
| Other | 32 (1.0) | 29 (91) | 3 (9.0) | |
| Not recorded | 136 (5.5) | 128 (94) | 8 (6.0) | |
| Provider, no. (%) | ||||
| Provider 1 | 534 (21) | 482 (90.) | 52 (10.) | <0.001^ |
| Provider 2 | 92 (3.8) | 84 (91) | 8 (9.0) | |
| Provider 3 | 256 (10.) | 227 (89) | 29 (11) | |
| Provider 4 | 62 (2.6) | 62 (100) | 0 | |
| Provider 5 | 253 (10.) | 191 (75) | 62 (25) | |
| Provider 6 | 111 (4.6) | 105 (95) | 6 (5.0) | |
| Provider 7 | 129 (5.2) | 126 (98) | 3 (2.0) | |
| Provider 8 | 212 (8.6) | 212 (100) | 0 | |
| Provider 9 | 381 (15) | 368 (97) | 13 (3.0) | |
| Provider 10 | 356 (14) | 332 (93) | 24 (7.0) | |
| Provider 11 | 127 (5.2) | 125 (98) | 2 (2.0) | |
| Injection, no. (%) | ||||
| No | 1620 (65) | 1517 (94) | 103 (6.0) | <0.001^ |
| Yes | 893 (36) | 797 (89) | 96 (11) | |
¥ Comparing operated versus non-operated patients
* = Independent t-test, ^ = Pearson Chi-Square test
Table 2.
Cox regression analysis of predictors of operative treatment for de Quervain’s tendinopathy
| OR | 95% CI | P-value | |
|---|---|---|---|
| Age | 1.0 | 0.99-1.0 | 0.46 |
| Female sex | 1.1 | 0.76-1.5 | 0.67 |
| White race | 0.84 | 0.61-1.2 | 0.30 |
| Injection | 1.7 | 1.3-2.3 | <0.001 |
| Providers ^ | |||
| Provider 2 | 1.1 | 0.53-2.4 | 0.75 |
| Provider 3 | 1.3 | 0.83-2.1 | 0.26 |
| Provider 4 | * | * | 0.96 |
| Provider 5 | 2.9 | 2.0-4.3 | <0.001 |
| Provider 6 | 0.68 | 0.29-1.6 | 0.37 |
| Provider 7 | 0.24 | 0.074-0.76 | 0.016 |
| Provider 8 | * | * | 0.93 |
| Provider 9 | 0.40 | 0.21-0.73 | 0.0030 |
| Provider 10 | 0.77 | 0.47-1.2 | 0.28 |
| Provider 11 | 0.15 | 0.036-0.61 | 0.0080 |
OR=Odds ratio, CI= Confidence Interval
* = OR could not be calculated because the number of surgeries for this provider was zero
^ = Provider 1 is set as the reference
Figure 1.

Kaplan-Meier curves show substantial difference in the rate of operation for each provider over time.
Figure 2.
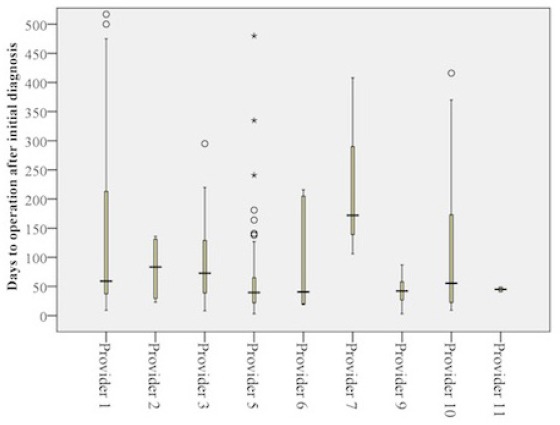
A box plot displays the substantial difference in distribution of time to operation among providers. Median and interquartile range (IQR) of the time elapsed from diagnosis to surgery is well demonstrated for each provider. Providers 4 and 8 with no subsequent surgery were excluded from the box plot.
Table 3.
Probability of having surgery after diagnosis with de Quervain
| Year | Total Diagnosed patients | Total Operation | Operated percentage |
|---|---|---|---|
| 2001 | 141 | 4 | 2.8 |
| 2002 | 151 | 5 | 3.3 |
| 2003 | 188 | 12 | 6.4 |
| 2004 | 171 | 24 | 14 |
| 2005 | 153 | 9 | 5.9 |
| 2006 | 181 | 14 | 7.7 |
| 2007 | 159 | 16 | 10 |
| 2008 | 182 | 14 | 7.7 |
| 2009 | 243 | 18 | 7.4 |
| 2010 | 224 | 14 | 6.3 |
| 2011 | 259 | 26 | 10 |
| 2012 | 299 | 28 | 9.4 |
| Mid 2013 | 162 | 15 | 9.3 |
| Total | 2513 | 199 | 7.9 |
There is a significant correlation between total number of diagnosed patients and operated patients (Adjusted R Sq=0.55, P value=0.0020)
Figure 3.
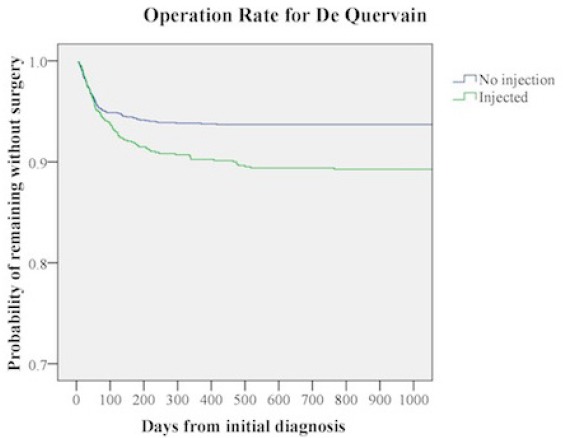
Kaplan-Meier curves demonstrate that patients with cortisone injection are more likely to have surgery for de Quervain tendinopathy.
Figure 4.
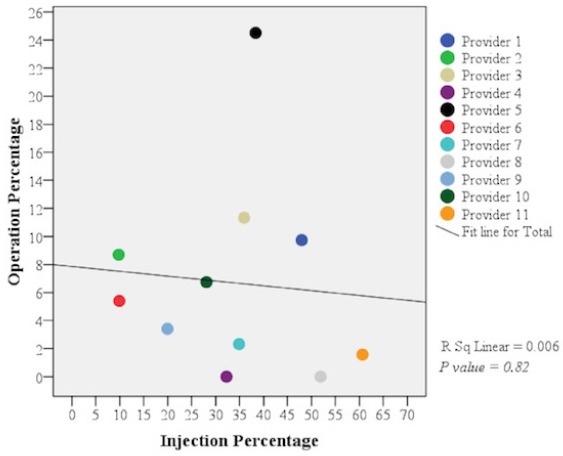
Scatter plot showing that there is no correlation between the rate of injection and the rate of surgery among providers.
Discussion
We are interested in the doctor-to-doctor variation in operative rates for various upper extremity conditions; diseases for which surgery is discretionary in particular. This study addressed the factors associated with operative treatment of de Quervain tendinopathy in a large database of patients treated at two hospitals. A better understanding of variation might lead to interventions to improve the quality and safety of care.
In spite of the large number of patients in our series, there are some limitations to consider when interpreting the results. This study depends on the accuracy of billing data. We have audited the database in prior studies and found an acceptable rate of errors. Using codes alone we cannot tell if the initial diagnosis, the injection, and the surgery were on the same side, but we believe it is safe to assume this was nearly always the case. We can only comment on treatment within the two hospitals included in the database. A small percentage of patients may have had surgery or corticosteroid injection prior to seeing one of the providers within our hospitals. A small percentage may have had surgery outside our system after diagnosis in our hospitals. Based on prior studies, we believe the rates of both occurrences are likely to be very low. There may be differences between the patients in each provider’s practice that cannot be captured by the data in this database.
The observation that only 7.9% of patients had surgery within our hospitals during the study period suggests that most patients get better without surgery. The observation that corticosteroid injection was associated with a higher rate of surgery suggests that it was not an injection that resolved the disease. An alternative explanation is that injections were offered to patients with more severe pathology (patients more likely to have surgery); however, our findings suggest injections are more of a practice idiosyncrasy than a consistent treatment algorithm. Furthermore, other studies have found that there is strong and consistent evidence that illness severity (pain intensity and disability) correlates most strongly with mood and mindset (8).
It seems safe to conclude that de Quervain tendinopathy is a self-limited disease. It certainly has the epidemiology of a self-limited disease; it does not accumulate with age like arthritis or rotator cuff pathology. A postal survey of patients with de Quervain tendinopathy found all but 3 patients (5%) were free of symptoms more than a year after diagnosis (4). Among patients in a recent randomized trial comparing two splint regimens called an average of 4 years after enrollment, only 3% had surgery and 5% reported continued symptoms (although they were not examined to be sure it was from de Quervain rather than thumb arthritis or another problem). (Data in peer review)
It is not clear that cortisone injection is a disease-modifying treatment in de Quervain tendinopathy. Treatment of de Quervain tendinopathy with corticosteroid injection is based on provider experience and a few case series, but there is insufficient data to know whether corticosteroid injection alters the natural history of the disease, or if it outperforms regression to the mean or the placebo effect. We are aware of two prospective, randomized placebo injection controlled trials of corticosteroid injection for de Quervain tendinopathy, both small and low quality with conflicting findings. A randomized trial involving 21 subjects by Peters-Veluthamaningal et al. published in an online open access journal found relief of pain but not disability one week after injection of triamcinolone rather than saline—an oddly short follow-up time to study (9). Another very small and incomplete trial by Makarawung et al that combined subjects with trapeziometacarpal arthrosis and de Quervain tendinopathy found little difference between placebo and dexamethasone injection (8). Both studies were methodologically weak and neither study could meaningfully conclude that steroid injection alters the natural history of the condition.
In our study patients who had a corticosteroid injection were more likely to have surgery in the 2 hospitals studied. There are several possible explanations for this association. Perhaps providers who offer injection are also more likely to offer surgery. Or it might be that a subset of patients prefer to intervene and if injections don’t work, they and their providers will decide to progress to surgery. But an important alternative explanation is that the steroid injection might medicalize the problem--where the evidence suggests that de Quervain tendinopathy is a self-limited condition, giving a patient an injection might reinforce a false belief that the problem will not resolve without intervention. When the injection doesn’t resolve the problem, patients with this mindset will be more likely to proceed to the next step of surgery.
The variations in surgery rate (0 to 25%) and time to surgery between providers are striking. Clearly the provider is having a substantial influence on treatment. We saw no pattern in practice of old versus young providers in that two most likely to operate were one of the oldest and one of the youngest providers. Only 8 (0.32%) of all 2,513 patients (and fewer than 4% of the patients that had surgery) switched provider to have surgery, indicating that patients generally accept the influence of the first provider they see. Differences between providers are a known source of variation in care. Particularly for discretionary conditions, fully informed patients should exhibit less variation by caregiver. Decision aids (videos, websites, pamphlets, etc. that help patients understand their options and determine their preferences) can decrease decisional conflict and limit variation by provider (10, 11). There is also some evidence that they might reduce overall use of resources (12-14). The use of decision aids for discretionary hand surgery merits additional study.
References
- 1.Walker-Bone K, Palmer KT, Reading I, Reading I, Coggon D, Cooper C. Prevalence and impact of musculoskeletal disorders of the upper limb in the general population. Arthritis Rheum. 2004;51(4):642–51. doi: 10.1002/art.20535. [DOI] [PubMed] [Google Scholar]
- 2.Petit Le Manac'h A, Roquelaure Y, Ha C, Bodin J, Meyer G, Bigot F, et al. Risk factors for de Quervain's disease in a French working population. Scand J Work Environ Health. 2011;37(5):394–401. doi: 10.5271/sjweh.3160. [DOI] [PubMed] [Google Scholar]
- 3.Peters-Veluthamaningal C, van der Windt DA, Winters JC, Meyboom-de Jong B. Cochrane Database Syst Rev. Cochrane Database Syst Rev. 2009;3:CD005616. doi: 10.1002/14651858.CD005616.pub2. [DOI] [PubMed] [Google Scholar]
- 4.Ring D, Schnellen A. Patient-centered care of de Quervain's disease. J Hand Microsurg. 2009;1(2):68–71. doi: 10.1007/s12593-009-0018-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dartmouth Atlas: overtreatment still common. Capitation Rates Data. 2008;13(8):8–10. [PubMed] [Google Scholar]
- 6.Weinstein JN, Lurie JD, Olson PR, Bronner KK, Fisher ES. United States' trends and regional variations in lumbar spine surgery 1992-2003. Spine (Phila Pa 1976) 2006;31(23):2707–14. doi: 10.1097/01.brs.0000248132.15231.fe. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Waits SA, Reames BN, Krell RW, Bryner B, Shih T, Obi AT, et al. Development of Team Action Projects in Surgery (TAPS): A Multilevel Team-Based Approach to Teaching Quality Improvement. J Surg Educ. 2014;71(2):166–8. doi: 10.1016/j.jsurg.2014.01.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Makarawung DJ, Becker SJ, Bekkers S, Ring D. Disability and pain after cortisone versus placebo injection for trapeziometacarpal arthrosis and de Quervain syndrome. Hand (N Y) 2013;8(4):375–81. doi: 10.1007/s11552-013-9529-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Peters-Veluthamaningal C, Winters JC, Groenier KH, Meyboom-DeJong B. Randomised controlled trial of local corticosteroid injections for de Quervain's tenosynovitis in general practice. BMC Musculoskelet Disord. 2009;10(1):131. doi: 10.1186/1471-2474-10-131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rashidian H, Nedjat S, Majdzadeh R, Gholami J, Haghjou L, Abdollahi BS, et al. The perspectives of iranian physicians and patients towards patient decision aids: a qualitative study. BMC Res Notes. 2013;6(1):379. doi: 10.1186/1756-0500-6-379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lee YK, Low WY, Ng CJ. Exploring patient values in medical decision making: a qualitative study. PLoS One. 2013;8(11):80051. doi: 10.1371/journal.pone.0080051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Reames BN, Shubeck SP, Birkmeyer JD. Strategies for reducing regional variation in the use of surgery: a systematic review. Ann Surg. 2014;259(4):616–27. doi: 10.1097/SLA.0000000000000248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rivlin M, Kachooei AR. Benefits of either operative or non-operative treatment for perilunate dislocation and fracture dislocations. Arch Bone Jt Surg. 2014;2(1):84–5. [PMC free article] [PubMed] [Google Scholar]
- 14.Moradi A, Ebrahimzadeh MH, Ring D. Nonspecific arm pain. Arch Bone Jt Surg. 2013;1(2):53–8. [PMC free article] [PubMed] [Google Scholar]