

Abstract
A frontotemporal craniotomy is usually performed using a “keyhole,” made at the union of the zygomatic arch and frontal bone. Consequently, skull depression may occur postoperatively, leading to temporal area deformities and poor cosmetic results. To prevent these complications, we describe our technique for frontotemporal craniotomy using an osteotome to prevent cosmetic deformities. After the temporal muscle is dissected and reflected with the scalp flap, a total of 3 burr holes are made in the frontal and temporal bones. In the lateral greater wing of the sphenoid, where a keyhole is usually made, a bone incision is made anteriorly-posteriorly with an osteotome. The bone flap is lifted upward, and the osteotome is inserted from behind to continue the incision. At craniotomy closure, the bone flap is fixed using a cranial bone flap fixation clamp. This procedure involves almost no removal of frontal or inferior temporal bone, resulting in virtually no bone defect. The absence of skull depression or deformity in the temples postoperatively leads to excellent cosmetic results. Our technique for frontotemporal craniotomy using an osteotome does not create bone defects, and use of titanium clamps for bone flap fixation provides normal skull bone alignment. This procedure provides excellent postoperative cosmetic results.
Keywords: frontotemporal craniotomy, keyhole, osteotome
Introduction
A frontotemporal craniotomy is usually performed using a MacCarty “keyhole.”4) This keyhole is made at the union of the zygomatic arch and frontal bone. Consequently, skull depression may occur postoperatively, leading to temporal area deformities and poor cosmetic results. To prevent these complications, bone cement, ceramic burr hole buttons, or titanium plates must be used. In this article, we describe our technique for frontotemporal craniotomy using an osteotome to prevent cosmetic deformities, without making a keyhole.
Methods
From January 1998 to December 2011, we performed frontotemporal craniotomy for tumor and aneurysm surgery in 1,393 patients (283 men and 1,110 women), ranging from 26 to 84 years of age. Among these patients, 18 had a sphenoid ridge meningioma or high position basilar top aneurysm, and a two-piece frontotemporal orbitozygomatic craniotomy was performed.
Surgical technique
The patient is placed in a supine position, and the head is rotated about 30° contralaterally. The neck is slightly extended such that the malar eminence is in the highest position, and the head is placed in pin fixation. A curvilinear skin incision is made along the zygomatic arch, advanced superoanteriorly within the hairline, and extended to the midline. The temporal muscle is dissected at the posterior margin of the incision and reflected with the scalp flap. No attempt is made to dissect between the scalp flap and temporal fascia. The scalp flap and temporal muscle are reflected back using a fishhook attached to a rubber band. This allows adequate exposure of the frontal bone where it joins with the zygomatic bone. Using an 11-mm perforator, a total of 3 burr holes are made in the frontal and temporal bones (Fig. 1). A craniotomy is performed to include the inferior part of the temporal bone. Then, in the lateral greater wing of the sphenoid, where a keyhole is usually made, a bone incision is made anteriorly-posteriorly with an osteotome. The bone flap is lifted upward, and the osteotome is inserted from behind to continue the incision (Fig. 2). The sphenoid wing is resected as extensively as possible using a Luer rongeur. At craniotomy closure, the bone flap is fixed using a cranial bone flap fixation clamp (CranioFix, Aesculap AG, Tuttlingen, Germany). There is no need to use cement, ceramic buttons, or titanium plates for repair of the temples.
Fig. 1.
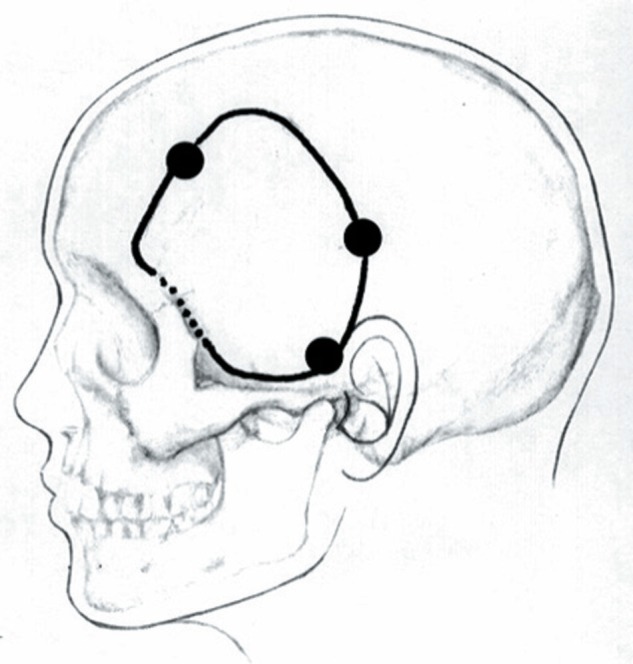
Position of burr holes for cosmetic frontotemporal craniotomy. Dotted line indicates the line of bone incision using an osteotome.
Fig. 2.

Operative photographs showing steps of left frontotemporal craniotomy using an osteotome and bone flap fixation using titanium clamps (CranioFix). In the lateral greater wing of the sphenoid, where a keyhole is usually made, a bone incision is made posteriorly (a) and anteriorly (b) with an osteotome. The bone flap is lifted upward, and the osteotome is inserted from behind to continue the incision (c). After the fixation using titanium clamps (d), there is no need to use cement, ceramic buttons or titanium plates for repair of the temples. There is very little removal of inferior temporal bone, and thus virtually no bone defect.
Results
As our technique provides flat exposure of the anterior skull base, use of a rongeur for bone resection is almost unnecessary. There is almost no removal of the inferior temporal bone, and thus virtually no bone defect. The absence of skull depression or deformity in the temples postoperatively leads to excellent cosmetic results. Using CranioFix, there are no differences in bone alignment after fixation (Fig. 3). In the first 5 patients who underwent this craniotomy procedure, there was a very small dural injury, but no brain injury. Subsequent use of a dissector to achieve adequate dural dissection has been successful in preventing injury to the dura. Among the 18 patients who underwent two-piece frontotemporal orbitozygomatic craniotomy, temporal muscle atrophy caused slight differences between the left and right temples in 4 patients. However, no cosmetic deformities have resulted from bone defects or flap depression, and no additional cosmetic surgery has been required.
Fig. 3.
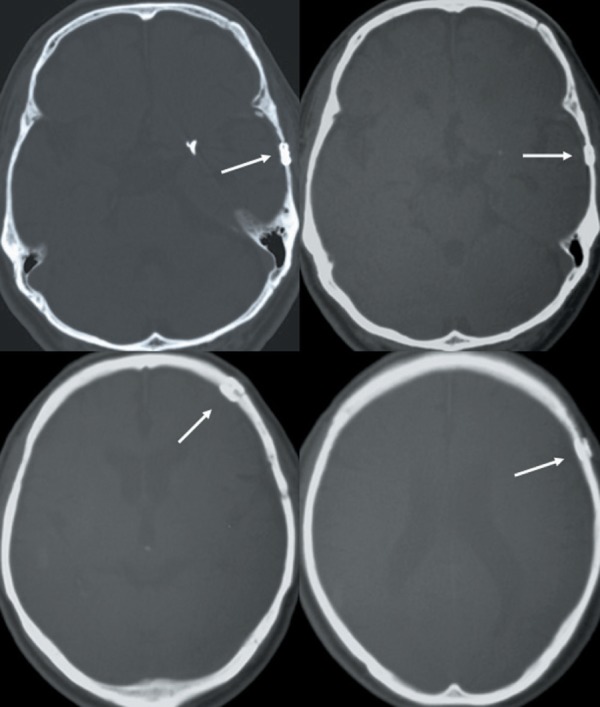
Postoperative computed tomographic (CT) scans with bone windows. Note the excellent skull bone alignment after fixation. Arrows indicate titanium clamps (CranioFix).
Discussion
The present craniotomy procedure is designed to prevent bone defects of the skull near the temples. A frontotemporal craniotomy is usually performed using a MacCarty “keyhole” for exposure just under the frontal dura.2,4) This is used to expose the epidural space and avoid dural injury due to the craniotomy. However, unless reinforcement is used at craniotomy closure, the bone defect can result in postoperative skin depression and poor cosmetic results. This often leads to noticeable skin depression in the temples and patient dissatisfaction. Cements, titanium plates, and ceramic buttons have been developed to prevent these problems.1,5) Although the surgical procedure is relatively straightforward, these foreign materials are often less than satisfactory as reinforcement. The present technique has the advantage that no burr hole is made at this site. A recently developed titanium bone flap fixation clamp system (CranioFix) offers higher reproducibility of fixation strength and excellent skull bone alignment after fixation. This fixation system does not impair the quality of postoperative CT or MRI, because the titanium alloy produces minimum susceptibility artifact.3,6) In the present procedure using this fixation system, the technique for craniotomy closure is not time-consuming, and foreign material is not required as reinforcement for repair of the temples.
Conclusion
Our technique for frontotemporal craniotomy using an osteotome does not create bone defects, and use of titanium clamps for bone flap fixation provides normal skull bone alignment. This procedure provides excellent postoperative cosmetic results.
References
- 1). Badie B: Cosmetic reconstruction of temporal defect following pterional [corrected] craniotomy. Surg Neurol 45: 383– 384, 1996. [DOI] [PubMed] [Google Scholar]
- 2). Hakuba A, Tanaka K, Suzuki T, Nishimura S: A combined orbitozygomatic infratemporal epidural and subdural approach for lesions involving the entire cavernous sinus. J Neurosurg 71: 699– 704, 1989. [DOI] [PubMed] [Google Scholar]
- 3). Lerch KD: Reliability of cranial bone flap fixation techniques: comparative experimental evaluation of suturing, titanium miniplates, and a new rivet-like titanium clamp (CranioFix): technical note. Neurosurgery 44: 902– 905, 1999. [DOI] [PubMed] [Google Scholar]
- 4). MacCarty CS: Meningiomas of the sphenoidal ridge. J Neurosurg 36: 114– 120, 1972. [DOI] [PubMed] [Google Scholar]
- 5). McDermott MW, Durity FA, Rootman J, Woodhurst WB: Combined frontotemporal-orbitozygomatic approach for tumors of the sphenoid wing and orbit. Neurosurgery 26: 107– 116, 1990. [DOI] [PubMed] [Google Scholar]
- 6). Shellock FG, Shellock VJ: Cranial bone flap fixation clamps: compatibility at MR imaging. Radiology 207: 822– 825, 1998. [DOI] [PubMed] [Google Scholar]