

Abstract
Hypermagnesemia is a rare and under-recognized cause of paralytic ileus. We report a case of a 21-year-old primigravida who was managed aggressively for preeclampsia and presented with postpartum paralytic ileus. Detailed history was employed to consider hypermagnesemia-induced ileus as the working diagnosis, and the patient improved with correction of the electrolyte imbalance. Hypermagnesemia-induced lethargy, decreased reflexes, muscle weakness, flaccid paralysis, respiratory muscle paralysis, and cardiac arrest are well-described; however, intestinal smooth muscle dysfunction leading to paralytic ileus has never been reported in the setting of magnesium use for peripartum preeclampsia management.
Introduction
Well-established causes of paralytic ileus include electrolyte disturbances (commonly hypokalemia), pancreatitis, and medications including narcotics and anticholinergics. Hypermagnesemia a rare causes of ileus, with only 3 cases reported in literature.1,2 Clinically significant hypermagnesemia is uncommon in individuals with normal renal function, and it is usually attributed to iatrogenic causes including laxatives, antacids, and tocolytics.3-8 A wide range of cardiac and neurologic presentations are possible, with the hallmark being refractory hypotension, which may be subtle and resemble many other diseases.3-9
Case Report
A 21-year-old primigravida was admitted at week 37 of gestation to an outside hospital with lethargy, decreased urine output, and hypertension. She was managed aggressively for preeclampsia, underwent emergent Cesarean section for non-reassuring fetal heart tracing (NRFHT), and was later transferred to high-risk obstetric unit for continued low urine output (650 cc over 24 hours). She was ill-appearing with distended abdomen, hypoactive bowel sounds, diffuse mild tenderness with no rebound tenderness or guarding, lethargy, vision changes, and decreased reflexes. The laboratory work-up showed normal complete blood count, mild renal injury with creatinine 1.6 mg/dL, potassium 5.6 mEq/L, normal hepatic function, magnesium levels 7.1 mg/dL (down from maximum of 9 mg/dL), calcium 6.8 mg/dL, and ionized calcium 1.17 mmol/L. Abdominal x-ray showed multiple air-fluid levels concerning for small bowel obstruction (SBO; Figure 1), confirmed with abdominal computed tomography (CT) that showed partial SBO with transition point in the right lower quadrant and collapsed distal ileum (Figure 2).
Figure 1.

Abdominal x-ray showing multiple air-fluid levels concerning for small bowel obstruction.
Figure 2.
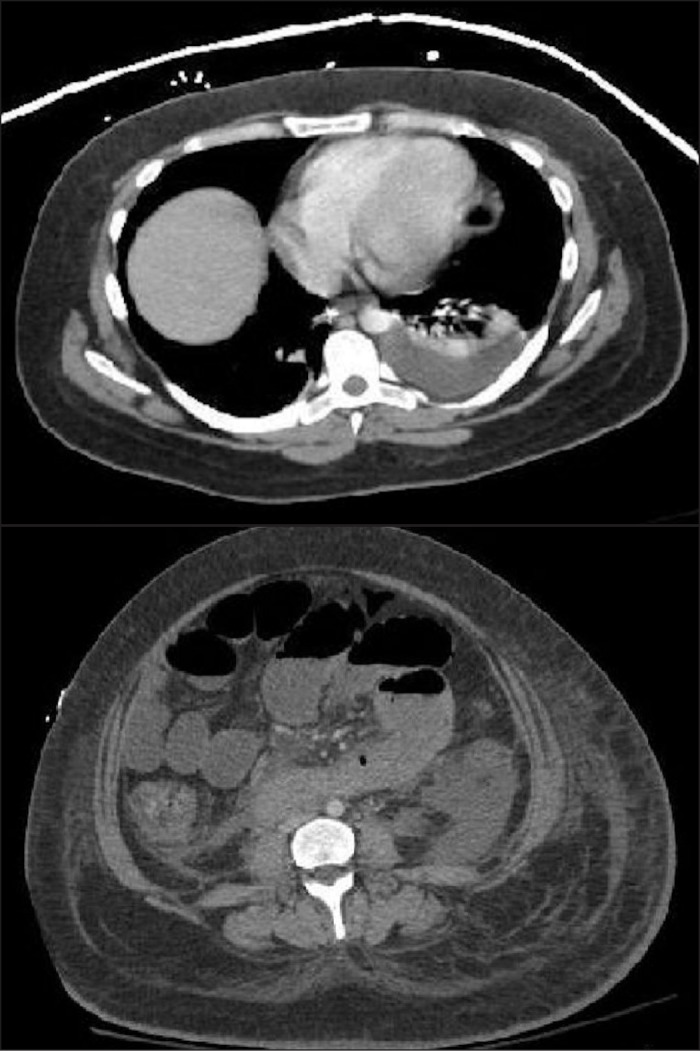
Abdominal CT showing multiple air-fluid levels with a transition point in the right lower quadrant and collapsed distal ileum concerning for partial small bowel obstruction.
The patient had received 4 doses of 4 mg magnesium sulfate intravenously over a 24-hour duration prior to delivery, but no narcotic analgesics. A strong suspicion of magnesium toxicity ileus was considered over postoperative ileus, which typically self-resolves within few days after surgery. She was conservatively managed with nil per os, intravenous fluids, and nasogastric tube decompression. Electrolytes (calcium and magnesium) were aggressively managed with calcium infusion, followed by diuresis to enhance urinary excretion of magnesium. The patient demonstrated remarkable improvement with correction of electrolyte imbalance over the following 5 days. Her bowel function returned, diet was advanced, and she was discharged. The patient continued to do well at all post-discharge outpatient follow-ups.
Discussion
Magnesium is the fourth most common cation in humans, with 1% of total body magnesium present in the extracellular fluid, and one-third bound to proteins.10-12 The kidneys are highly effective in regulating body magnesium levels. Thus, hypermagnesemia is much more likely in patients with impaired kidney function, especially if exposed to exogenous magnesium sources. Our patient developed hypermagnesemia after she received magnesium as a part of her severe preeclampsia treatment, which was complicated by renal insufficiency leading to hypermagnesemia. Hypermagnesemia has been reported in patients who ingest a large amount of Epsom salts and magnesium-containing cathartics.10,13
Hypermagnesemia usually manifests clinically at serum levels greater than 2 mmol/L (4.8 mg/dL).9 It affects a wide variety of body systems, with the most common systems affected being the cardiovascular and neuromuscular, resulting in lethargy, confusion, hypotension, and decrease in the deep tendon reflexes (due to the neuromuscular blockade effect).9 At serum levels <5 mmol/L, hypermagnesemia may lead to hypotension, delayed intraventricular conduction, and prolonged Q-T interval. It can progress to atrioventricular block and cardiac arrest at levels >5mmol/L, and to respiratory depression at levels >6.5 mmol/L.9
The effect of hypermagnesemia on intestinal smooth muscles has been well-studied in animals, with limited reports available in humans.14,15 Magnesium can block the peristaltic activity once applied to the mucosal surface of the guinea pig ileum, and this effect could be antagonized when anti-cholinergics are applied to the serosal surface.16 The paralytic effect of magnesium in humans has been reported only in a few cases, including a patient receiving parenteral magnesium sulfate for tocolysis, and in patients on magnesium laxatives and Epsom salts for chronic constipation; the effect was exacerbated in 2 cases secondary to calcium channel blocker use.1,2 There are 2 reported cases of newborn hypermagnesemia leading to intestinal hypomotility, subsequent meconium plug syndrome, abdominal distension, and respiratory depression that partially resolved after administration of calcium.15 The authors hypothesized that high calcium levels protected the patients from the hypermagnesemia-induced myoneural depression. Magnesium acts as a nonspecific calcium channel blocker, so its effect may be exacerbated by calcium channel blockers and hypocalcemia, and can be partially reversed with calcium infusion.15 Diuresis induced with intravenous fluids has also shown to be beneficial in the management of hypermagnesemia.9
Disclosures
Author contributions: M. Al-Shoha and JS Klair drafted and revised the manuscript. M. Girotra and M. Garcia-Saenzde-Sicilia, conceptualized, designed, and revised the manuscript. M. Garcia-Saenz-de-Sicilia is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
References
- 1. Hill WC, Gill PJ, Katz M. Maternal paralytic ileus as a complication of magnesium sulfate tocolysis. Am J Perinatol. 1985;2(1):47–8. [DOI] [PubMed] [Google Scholar]
- 2. Golzarian J, Scott HW, Richards WO. Hypermagnesemia-induced paralytic ileus. Dig Dis Sci. 1994;39(5):1138–42. [DOI] [PubMed] [Google Scholar]
- 3. Qureshi TI, Melonakos TK. Acute hypermagnesemia after laxative use. Ann Emerg Med. 1996;28(5):552–5. [DOI] [PubMed] [Google Scholar]
- 4. Nordt SP, Williams SR, Turchen S, et al. Hypermagnesemia following acute ingestion of Epsom salt in a patient with normal renal function. J Toxicol Clin Toxicol. 1996;34(6):735–9. [DOI] [PubMed] [Google Scholar]
- 5. Byron FE. Fatal results following administration of magnesium sulfate. J Malaya Branch Med Assn. 1939;3:100–1. [Google Scholar]
- 6. Garcia-Webb P, Bhagat C, Oh T, et al. Hypermagnesemia and hypophosphatemia after ingestion of magnesium sulphate. B Med J (Clin Res Ed). 1995;288(6419):759–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Fung MC, Weintraub M, Bowen DL. Hypermagnesemia. Arch Fam Med. 1995;4(8):718–23. [DOI] [PubMed] [Google Scholar]
- 8. Ferdinandus J, Pederson JA, Whang R. Hypermagnesemia as a cause of refractory hypotension, respiratory depression and coma. Arch Intern Med. 1981;141(5):669–70. [PubMed] [Google Scholar]
- 9. Van Hook JW. Hypermagnesemia. Crit Care Clin. 1991;7(1):215–23. [PubMed] [Google Scholar]
- 10. Birrer R, Shallash A, Totten V. Hypermagnesemia-induced fatality following Epsom salt gargles. J Emerg Med. 2002;22(2):185–188. [DOI] [PubMed] [Google Scholar]
- 11. Graber TW, Yee AS, Baker FJ. Magnesium: Physiology, clinical disorders and therapy. Ann Emerg Med. 1981;10(1):49–57. [DOI] [PubMed] [Google Scholar]
- 12. Whang R. Clinical disorders of magnesium metabolism. Comp Ther. 1997;23(3):168–73. [PubMed] [Google Scholar]
- 13. Gerard SK, Hernandez C, Khayam-Bashi H. Extreme hypermagnesemia caused by an overdose of magnesium-containing cathartics. Ann Emerg Med. 1988;17(7):728–31. [DOI] [PubMed] [Google Scholar]
- 14. Iseri LT, French JH. Magnesium: Nature's physiologic calcium blocker. Am Heart J. 1984;108(1):188–189. [DOI] [PubMed] [Google Scholar]
- 15. Sokal M, Koenigsberger M, Rose J. Neonatal hypermagnesemia and the meconium plug syndrome. N Engl J Med. 1972;286(15):823–826. [DOI] [PubMed] [Google Scholar]
- 16. Beleslin D, Samardizic R. Pharmacological analysis of the peristalsis block induced by magnesium applied at the serosal and mucosal surfaces of the isolated guinea-pig ileum. CR Soc Biol Fil. 1977;171(4):750–754. [PubMed] [Google Scholar]