

Abstract
To compare the surgery and conservative treatment of multiple fractured ribs, we designed a randomized controlled trial in the single center of thoracic surgery ward. After admission condition assessment (general clinical evaluation, operation condition assessment, the digital method of pain assessment), the selected multiple fractured rib patients were told to choose surgery or conservative treatment, according to the patient will undergo surgery or conservative treatment. In the acute phase, compared with conservative treatment, patients with mechanical ventilation in time (mechanical ventilation time MV) (3.7 ± 1.4 vs. 9.5 ± 4.3), ICU stay time (8.2 ± 4.3 vs. 14.6 ± 3.2), total hospitalization days (15.3 ± 6.4 vs. 26.5 ± 6.9), the incidence of pneumonia (6.7% vs. 19.1%), mortality (1.3% vs. 5.3%) and pain score on patients (3.3 vs. 5.8) of surgical treatment group were significant lower (P < 0.05). The number of tracheostomy in surgical patients with conservative treatment (4 vs. 7) was no statistically significant difference (P > 0.05). In chronic phase, the surgical patients compared with patients with conservative treatment in the chest wall pain (2.9 ± 1.2 vs. 5.6 ± 1.7), chest wall tension (13.3% vs. 57.3%), dyspnea (5.3% vs. 22.4%) and chest wall deformity rate (4% vs. 93.5%) were lower significantly (P < 0.05). In conclusion, the surgical treatment of multiple fractured ribs could ease the acute chest pain, reduce the mechanical ventilation time and incidence of pneumonia, shorten the hospitalization days and total hospitalization days in the ICU and alleviate the forward chest wall discomfort. The speedy recovery and long-term quality of patients’ life had improved significantly.
Keywords: Multiple rib fractured, randomized controlled trial, surgical treatment, conservative treatment
Introduction
Fractured ribs, a common performance after chest trauma, ever used conservative treatment, although have certain curative effect, but there are still shortcomings. In recent years, part of the rib fractures patients in our hospital were treated by surgical treatment, compared with the conservative treatment of patients with the clinical comparison and follow-up, now do a summary.
Materials and methods
Clinical data
From January 1, 2010 to December 31, 2012, in the thoracic surgery department of sixth people’s hospital affiliated to Shanghai Jiaotong university, the total number of patients with chest trauma of all kinds of trauma was 956, with 732 cases were male patients and 224 cases were women. Select male patients with pure chest trauma to assess the general clinical conditions, operation conditions and the degree of pain. To satisfy the operation conditions of the patients 1. the number of rib fracture was 3 or more, 2. frame fracture dislocation 50% or higher, 3. Serious chest wall deformity or chest cavity active bleeding, 4. The flail chest. Using random grouping, inform the patients with surgery or conservative treatment group after two treatments. If the patient is intend to agree with grouping situation in research, inconsistencies are excluded. Results a total of 164 cases of male patients with fracture of multiple ribs into the study. Ages from 24 to 72. Injury factors including traffic accident (84 cases), tumbling injury (18 cases), falling injury (47 cases) and others were 15 cases. 153 cases with pulmonary contusion, 148 cases with hemothorax, 61 cases with pneumothorax. Fractured ribs number 6~12 root, an average of 8.0. Hospitalization days 10~56 days, an average of 21.4 days. 75 cases with surgical group and 89 cases with conservative group.
Conservative treatment
Two groups of patients after admission for regular examination. Conservative groups of patients with chest strap are fixed, the semi recumbent position. According to the change of heart rate, blood pressure, the number of hemoglobin to decide whether to blood transfusion therapy. According to the patients’ temperature, nature of sputum, lung examination combined with imaging examination results determine presence of lung infection, and deciding whether antibiotic treatment is needed. According to the chest X-ray and chest CT examination to know the degree of pulmonary contusion and pleural effusion, and pleural puncture or chest closed drainage when necessary. Ladder use of analgesic drugs alleviate symptoms of patients with chest pain, giving the expectorant aerosolized medications, such as encourage and help patients with cough expectoration drainage to prevent lung infection. To encourage early ambulation in stable condition. If the paitents have low oxygen, give with nasal catheter or mask oxygen. If appear respiratory failure to give endotracheal intubation and mechanical ventilation. If need prolonged mechanical ventilation, the tracheostomy is processing.
Surgical treatment
The surgical patients except conservative treatment measures, using surgical treatment with open reduction and internal fixation of rib fractures. According to the chest X-ray, chest CT and ribs CT three-dimensional reconstruction of clear operation scheme. According to the condition is decided to surgery date. According to the concrete ribs fracture choose appropriate incision (posterolateral incision, straight axillary incision, etc.), try to use one incision to the fixed fractured ribs. In patients with preoperative doubt within the chest damaged, chest cavity detection and processed firstly, then fixed fractured ribs. In patients with preoperative no significant intrathoracic injury fixed fractured ribs directly. All fractured ribs fixed with the nickel titanium alloy by device. Note intercostals nerve and blood vessel protection, avoid the broken wall of the pleura. Routine postoperative drainage. According to the chest trauma choose whether postoperative ventilator support. After the operation, use drug treatments such as analgesia expectoranting atomization and conservative treatment of patients with the same, also encourage and assist patients cough expectoration drainage to prevent lung infection. To encourage early ambulation in stable condition, in order to promote recovery after surgery.
Acute indicators
1. The mechanical ventilation time and ICU stay days, 2. The total hospitalization days, 3. The incidence of pneumonia, 4. The number of tracheotomy, 5. The number of mortality.
Chronic indicators
1. Chest pain condition, 2. Difficulty in breathing, 3. The chest wall tension, 4. Chest wall deformity.
Pain
According to the numerical classification method (numerical rating scale, NRS) for pain after two groups of patients with traumatic. 0: painless; 1~3: mild pain; 4~7: moderate pain; 8~10: severe pain.
Follow-up
Two groups of patients were outpatient follow-up in two month from the date of damage. Through the patients’ subjective feeling, physical examination, chest X-ray, chest CT and ribs CT three dimensional reconstruction and to observe the effect after treatment of evaluation.
Statistical processing
Using SPSS 13.0 statistical software for statistical and measurement data with mean ± standard deviation, said between group by t test. Count data to rate, according to comparison between groups by chi-square test. With P < 0.05 for the difference was statistically significant.
Results
General clinical data of two groups of patients
Before treatment in two groups of patients age, Abbreviated Injury Scale (AIS), number of fractured ribs, the number of patients with flail chest, the number of patients with pulmonary contusion, the number of patients with hemathorax and pneumothorax, the number of patients with mechanical ventilation and chest wall deformity were all no statistically significant difference (P > 0.05), are shown in Table 1.
Table 1.
General clinical data of two groups of patients
| Surgical | Conservative | P value | |
|---|---|---|---|
| Age | 52 ± 4.5 | 51 ± 3.1 | NS |
| AIS | 4.5 ± 1.7 | 4.3 ± 1.3 | NS |
| Fracture number | 8.1 (6-12) | 7.9 (6-11) | NS |
| Flail Chest | 31 (41.3%) | 35 (39.3%) | NS |
| Lung contusion | 71 (94.5%) | 82 (92.1%) | NS |
| Hemathorax | 68 (90.7%) | 80 (89.9%) | NS |
| Pneumothorax | 23 (30.7%) | 28 (31.4% ) | NS |
| MV patients | 21 (28%) | 27 (30.3%) | NS |
| Chest wall deformity | 67 (89.3%) | 77 (86.7%) | NS |
The comparison of two groups of patients with acute phase
Except for the numbers of tracheotomy in two groups were no difference after treatment, the surgical treatment group of patients during mechanical ventilation, ICU stay time, the total number of days in hospital, the incidence of pneumonia and mortality were significantly lower than patients with conservative treatment, the differences between the two groups was statistically significant (P < 0.05), are shown in Table 2.
Table 2.
The comparison of two groups of patients with acute phase of index
| Surgical | Conservative | P value | |
|---|---|---|---|
| MV time (day) | 3.7 ± 1.4 | 9.5 ± 4.3 | 0.037 |
| ICU stay (day) | 8.2 ± 4.3 | 14.6 ± 3.2 | 0.041 |
| Hospital stay (day) | 15.3 ± 6.4 | 26.5 ± 6.9 | 0.039 |
| Tracheostomy (n) | 4 | 7 | NS |
| Pneumonia (n) | 5 (6.7%) | 17 (19.1%) | 0.036 |
| Mortality (n) | 1 (1.3%) | 4 (5.3%) | 0.045 |
The comparison of two groups after treatment in patients with pain
Pain score shows that at any point in time after treatment, the surgical patients experience pain feelings were significantly lower than the conservative group, the differences between the two groups have statistical significance (P < 0.05), as shown in Figure 1.
Figure 1.
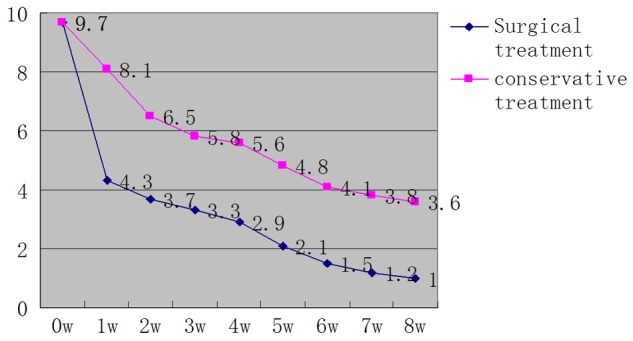
The comparison of two groups after treatment in patients with pain.
The comparison of two groups of patients with chronic phase
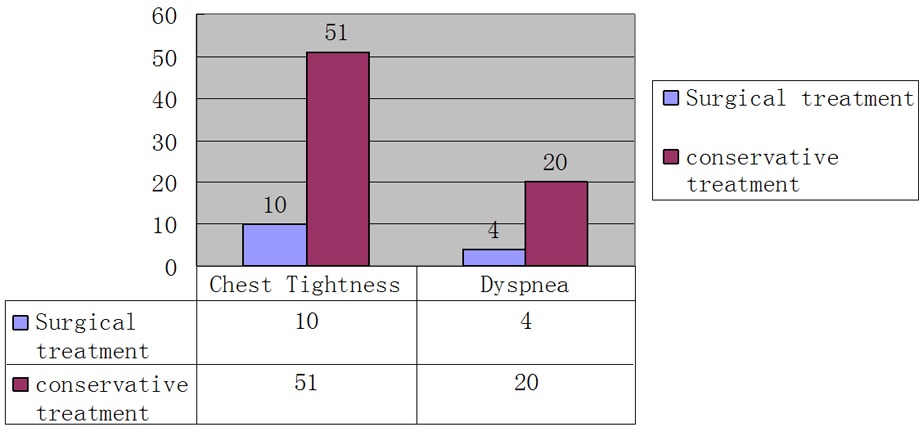
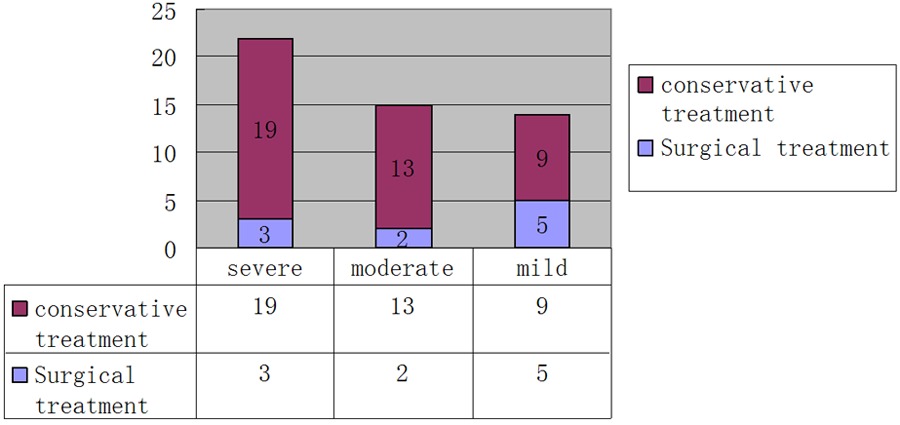
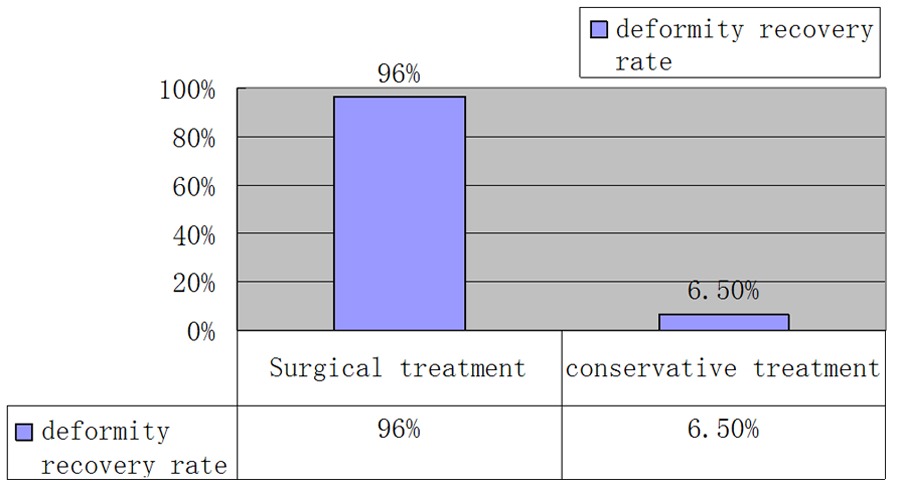
In chronic indicators after treatment of surgical patients with chronic chest pain, chest wall tension and dyspnea were significantly lower than patients with conservative, differences between the two groups was statistically significant (P < 0.05), see Tables 3, 4 and 5. And chest wall deformity correction surgery patients satisfaction rate higher than that of patients with conservative treatment, the differences between the two groups also have statistical significance (P < 0.05), as shown in Table 6.
Table 3.
The two groups of patients in January after the comparison of chronic index
| Surgical | Conservative | P value | |
|---|---|---|---|
| Thoracic pain | 2.9 ± 1.2 | 5.6 ± 1.7 | 0.043 |
| Chest tightness | 10 (13.3%) | 51 (57.3%) | 0.014 |
| Dyspnea | 4 (5.3%) | 20 (22.4%) | 0.029 |
| Chest wall deformity | 3 (4.0%) | 72 (93.5%) | 0.017 |
Table 4.
The two groups after treatment in patients with chest wall tension, and the comparison of degree of difficulty in breathing
|
Table 5.
The two groups after treatment in patients with different degree of chest wall tension
|
Table 6.
The two groups after treatment in patients with chest wall deformity recovery rate
|
Discussion
Multiple fractured ribs is a common clinical manifestations of chest trauma, there are statistics show that the chest trauma incidence is rising, accounts for 10-15% trauma, including fractured ribs accounted for 85% of chest trauma [1]. Rib fractures in patients with early most feel severe chest pain, dare not to breathe, cough, body posture change also is limited by a certain [2]. Even some serious multiple fractured ribs with because of flail chest and merge pulmonary contusion will appear acute respiratory function failure, which threaten life [3]. In the past for such patients can only adopt bed rest, use of analgesic drugs to relieve the symptom [4]. Or give a wide tape or chest wall fixed, fixed even towel clips in for acute respiratory failure patients need improve hypoxia by mechanical ventilation. Although these methods have certain curative effect, but patients thoracic activity is restricted because of still stay in bed longer and cannot effectively cough phlegm and induce pulmonary complications, or because of long time of intubation with mechanical ventilation associated pneumonia [5]. Even through the lung infection, the persistence of chest painful sensation and chest wall deformity result in impaired respiratory function in long term are still difficult problems, and affect the quality of life of patients [6].
In the early 16th century Ambroise Pare proposed the surgical treatment to the fractured ribs in first time. 40-50 s of the 20th century to promote the development of surgical treatment of fractured ribs because of the second world war. The mechanical ventilation technology development in the 70 s of this century, was once reduced people’s expectations of the surgical treatment, and think that multiple fractured ribs respiratory function of patients with flail chest in failure and only for breathing machine internal fixation treatment. And since the 20th century, with the study of chest trauma, which is not flail chest caused patients appearing respiratory failure, but the degree of pulmonary contustion [7]. Acute lung injury induce lung ventilation flow ratio imbalance cause the patients breathing difficulties and appearing hypoxemia. So the purpose of using respiratiory machine is to improve the oxygen supply and oxygenation in patients with pulmonary contusion, while the chest wall fixed flail chest is beneficial to early mechanical ventilation patients out of the machine, contribute to the recovery of the lung function in patients with mechanical ventilation and avoid the occurrence of pulmonary complications. At present, with the study of fractured ribs, the sequelae after fractured ribs and all kinds of new fixed material, surgical treatment is recommended by more and more surgeons. So we choose part of rib fracture patients treated with open surgical internal fixation, and compared with the conservative treatment of fractured ribs.
In order to avoid the chest trauma caused by outside interference and gender differences on pain tolerance, we just choose the men pure chest trauma patients. In age, trauma score before treatment in both groups, the number of fractured ribs, and pulmonary contusion, number of hemothorax, number of pneumothorax, number of mechanical ventilation, lung infections and chest wall deformity rate were indiscriminate. When compared to patients with conservative treatment, the surgical treatment of rib fractures in patients with acute injury was significantly reduced. In addition to the number of the trachea cutting was no significant difference, the patients with surgical treatment of multiple fractured ribs are less days of mechanical ventilation, ICU stay time, total hospitalization days, the incidence of pneumonia and mortality were significantly lower than patients with conservative treatment, with similar results of Meta analysis [8,9]. Prompt surgical treatment for patients out of the body early recovery, can make patients with fracture of multiple ribs obvious benefit.
We also found compared to the conservative treatment, the patients after surgery can leave bed earlier, so it can restore the damaged lung function with great help. This avoids pulmonary complications because of staying in bed and restricted position at a long time, patients after surgery can recover earlier.
Research shows that after treatment the pain of chest wall gradually decreased with prolonged , and the pains of surgical patients were obviously decline compare to conservative treatment group (4.3 vs. 8.1) in the first day after surgery. During the next at any point in time, compared with conservative treatment group, the surgical patients with showed a lower pain, highlighted the advantages of surgical treatment. Khandelwal G [10] showed that after surgery, the surgical pain score higher than the conservative group after 5 days of the surgery, but 15 days and 30 days postoperative pain score is significantly lower than the conservative groups. Early surgical pain score plateau for consideration of the surgical patients are not receiving treatment after injury immediately, but with the conservative group patients received conservative treatment after 10 days together only under still not obvious pain relief, and the pain score is included in the incision wounds.
Pain of the chest wall in rib fractures patients is a primary and strong subjective feeling, this kind of feeling is unpleasant, fractured ribs broken the dislocation stimulation, the release of pain factor, extrusion of intercostals nerve of rib fracture, caused by the comprehensive factors such as friction and pull. Pain often limit the chest movement, reduces the breathing rate, reduce the swing of trachea cilia, also cause pain in patients with systemic stress reaction. Under the local and systemic factors, patients self expectoration drainage function is reduced, and the vast majority of merging different rib fracture patients degree of pulmonary contusion, thus increased the probability of patients with pneumonia after trauma, some patients with severe pneumonia may occur and even life-threatening. So pain control can not only relieve the discomfort of fractured ribs itself, also can prevent the occurrence of complications [11].
Because of significantly reduce the patients pain, as a result of the surgery for patients with respiratory with great help, so can reduce the incidence of pneumonia, reduced the time of mechanical ventilation, shortening the days of ICU stay and hospitalization, and also significantly reduce mortality. We find the pain significantly reduced on the first day after the surgery, and most of incision pain can be well tolerated by patients. Actually review past all sorts of conservative treatment, in view of multiple rib fractures in patients with the first and important principles is to alleviate symptoms of patients with chest pain, in order to prevent and respiratory complications such as pneumonia, atelectasis [12]. Patients tend to the worries of the analgesic effects and reducing the intake of drugs, tape or chest strap limit the thoracic movement and can not help reduce respiratory complications. After treatment with surgery, due to multiple rib fracture fixation of fracture end, avoid the dislocation movement, ease of fracture end of intercostals nerve conformity and stimulation, significantly reduced in patients with chest pain feeling. Multiple studies have shown that surgery can not only significantly improve pain and respiratory function, improve the quality of life, reduce the loss of social work ability has a great help. According to surgical treatment can improve patients with symptoms of short-term and long-term, quickly reduce disability, improve recovery, improve the cure results [13,14].
Through the comparison of chronic injury index including chest wall chronic pain, chest wall tension, difficulty breathing and degree of chest wall deformity we found surgery patients were significantly lower than patients with conservative treatment. Chronic pain is due to the chest wall intercostals nerve injury or to continuous stimulation by dislocation ribs. Chest wall tension is a kind of tightening feeling caused by multiple fractured ribs dislocation healing. It will appear in mild patients with walking quickly or upstairs, moderate patients can appear when walking on the ground, whereas severe patients will have this feeling in the resting state. Surgical patients with rib fractures in various degree of chest wall tension were significantly lower than that of patients with conservative treatment, because of multiple fractured ribs dislocation shortening healing in patients with thoracic narrow or collapse caused by chest wall deformity in conservative group. Chest wall tension caused by chest wall deformity limits the range of the patient’s breathing, the onset of dyspnea in patients with feeling, reduce the patient’s lung function, influence the patient’s quality of life. After surgical treatment of patients with recovery continuity and stability, and eliminates the shortening dislocation deformity, makes the thoracic was restored to normal anatomic structures and eliminates the due to the adverse consequences of dislocation deformity, so in all sorts of chronic index up are significantly lower than the conservative treatment of patients, improve the prognosis and the quality of life of fractured rib patients ultimate [6].
Above all, patients with multiple fractured ribs after surgical treatment in the acute phase of trauma recovery and forward on the improvement of chronic injuries have advantage, so for some patients with multiple fractured ribs for the surgical treatment is a good choice.
Disclosure of conflict of interest
None.
References
- 1.Altunkaya A, Aktunc E, Kutluk AC, Buyukates M, Demircan N, Demir AS. Analysis of 282 patients with thoracic trauma. Turk J Thorac Cardiovasc Surg. 2007;15:127–132. [Google Scholar]
- 2.Topcu I, Ekici Z, Sakarya M. Comparison of clinical effectiveness of thoracic epidural and intravenous patient-controlled analgesia for the treatment of rib fractures pain in intensive care unit. Ulus Travma Acil Cerrahi Derg. 2007;13:205–210. [PubMed] [Google Scholar]
- 3.Dehghan N, De Mstral C, Mckee MD, Schemitsch EH, Nathens A. Flail chest injuries: a review of outcomes and treatment practices from the National Trauma Data Bank. J Trauma Acute Care Surg. 2014;76:462–468. doi: 10.1097/TA.0000000000000086. [DOI] [PubMed] [Google Scholar]
- 4.Karmakar MK, Ho AM. Acute pain management of patients with multiple fractured ribs. J Trauma. 2003;54:615–625. doi: 10.1097/01.TA.0000053197.40145.62. [DOI] [PubMed] [Google Scholar]
- 5.Brasel KJ, Guse CE, Layde P, Weigelt JA. Rib fractures: relationship with pneumonia and mortality. Crit Care Med. 2006;34:1642–1646. doi: 10.1097/01.CCM.0000217926.40975.4B. [DOI] [PubMed] [Google Scholar]
- 6.Marasco S, Lee G, Summerhayes R, Summerhayes R, Fitzgerald M, Bailey M. Quality of life after major trauma with multiple rib fractures. Injury. 2014;1383:1–5. doi: 10.1016/j.injury.2014.06.014. [DOI] [PubMed] [Google Scholar]
- 7.Dongel I, Coskun A, Ozbay S, Bayram M, Atli B. Management of thoracic trauma in emergency service: Analysis of 1139 cases. Pak J Med Sci. 2013;29:58–63. doi: 10.12669/pjms.291.2704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Leinicke JA, Elmore L, Freeman BD, Colditz GA, Operative M. Operative Management of rib fractures in the setting of Flail Chest: a systematic review and meta-analysis. Ann Surg. 2013;258:914–921. doi: 10.1097/SLA.0b013e3182895bb0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Marasco SF, Davies AR, Cooper J, Varma D, Bennett V, Nevill R, Lee G, Bailey M, and Fitzgerald M. Prospective randomized controlled trial of operative rib fixation in traumatic flail chest. J Am Coll Surg. 2013;216:924–932. doi: 10.1016/j.jamcollsurg.2012.12.024. [DOI] [PubMed] [Google Scholar]
- 10.Khandelwal G, Maehur RK, Shukla S, Maheshwari A. A prospective single center study to assess the impact of surgical stabilization in patients with rib fracture. Int J Surg. 2011;9:478–481. doi: 10.1016/j.ijsu.2011.06.003. [DOI] [PubMed] [Google Scholar]
- 11.Hwang EG, Lee Y. Effectiveness of intercostal nerve block for management of pain in rib fracture patients. J Exerc Rehabil. 2014;10:241–244. doi: 10.12965/jer.140137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Solak O, Oz G, Kokulu S, Solak O, Doğan G, Esme H, Ocalan K, Baki ED. The effectiveness of transdermal opioid in the management multiple rib fractures: randomized clinical trial. Balkan Med J. 2013;30:277–281. doi: 10.5152/balkanmedj.2013.8191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Girsowicz E, Falcoz PE, Santelmo N, Massard G. Does surgical stabilization improve outcomes in patients with isolated multiple distracted and painful non-flail rib fractures? Interact Cardiovas Thorac Surg. 2012;14:312–315. doi: 10.1093/icvts/ivr028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Moreno De La Santa Barajas P, Polo Otero MD, Delgado Sánchez-Gracián C, Lozano Gómez M, Toscano Novella A, Calatayud Moscoso Del Prado J, Leal Ruiloba S, Choren Durán ML. Surgical fixation of rib fractures with clips and titanium bars (STRATOSTM System) Preliminary Experience Cir Esp. 2010;88:180–186. doi: 10.1016/j.ciresp.2010.06.004. [DOI] [PubMed] [Google Scholar]