

Abstract
Acute pancreatitis can be associated with a variety of complications caused by the interaction of the pancreatic fluids with the local structures, and may eventually form pseudocysts, ascites, etc. Nevertheless, scrotal swelling caused by severe acute pancreatitis was rarely reported due to low incidence or lack of recognition. We reported a rare phenomenon that left scrotal swelling caused by severe acute pancreatitis in a 38-year-old man.
Keywords: Pancreatitis, scrotum swell, complication, inguinal canal
Introduction
Pancreatitis associated with the extension of a pancreatic collection. According to Robert et al, 57% of patients were diagnosed to have fluid collections, 39% having 2 areas involved and 33% having 3 or more areas involved in an investigation of 137 patients hospitalized with acute pancreatitis [1]. The extension of a pancreatic collection, pseudocyst or abscess into the groin, involving the inguinal canal and scrotum is a rare complication of acute pancreatitis. In spite of low incidence of this complication, it does capture our attention as it may be misdiagnosed as other more common pathologies of scrotum swelling such as orchiepididymitis, testicular torsion, testicular hydrocele or testicular tumor, and may lead to unnecessary surgical treatment [2]. We report a case of left scrotal swelling caused by severe acute pancreatitis in a 38-year-old male.
Case report
A 38-year-old male from Anhui province in China was referred to our hospital for further examination and treatment with a 7-day-history of worsening abdominal pain and a 4-day-history after appendectomy in the local hospital. He began to complain of constant abdominal pain without any predisposing causes 7 days before his hospitalization in our hospital. The pain was tolerable and no fever, nausea or vomit accompanied. After visited the local hospital, an ultrasound examination was taken, revealing acute appendicitis. And blood routine test revealed an increase in leucocytes and neutrophils. Combining with the tests and his symptoms, he was diagnosed with acute appendicitis by doctors in the local hospital, and an open appendectomy was taken. It was a pity that his symptoms failed to improve and his inflammatory markers remained elevated after the operation. Furthermore, large area of ecchymosis was found in left abdomen and back. Therefore, a spiral Computerized Tomography (CT) scan of his abdomen and pelvis was performed. The scan revealed marked pancreatitis swelling, bilateral pleural effusion, portal vein and superior mesenteric vein thrombosis, consistent with acute pancreatitis.
Due to the fact that his clinical condition remained poor, he was transferred to our hospital for further management. On arrival, his vital signs were stable with blood pressure of 131/72 mmHg, heart rate of 102 per minute, and temperature of 37.2°C. But operative incision infection was found. He was managed carefully and over the following days his general clinical condition and inflammatory markers steadily improved.
Two days after his admission, he began to complain of left scrotal pain. His left scrotal swelling was noted and associated with a purple discoloration, with his left testicle being impalpable on examination (Figure 1). An ultrasound scan of the male’s scrotum was performed, revealing that a marked swelling of the left scrotal wall wrapped around the normal left testis and periorchium. And the swelling could be followed all the way up to the deep inguinal ring and into the abdomen (Figure 2). Subsequently, an abdominal and pelvic CT scan was performed which demonstrated multiple abdominal, retroperitoneal and pelvic fluid collections (Figure 3), and extending down to the root of the scrotum through the left inguinal canal and encased the spermatic vessels, testis and periorchium (Figure 4). Considering the impact of pancreatic fluid collection, a percutaneous drain was inserted guided by ultrasound into left retroperitoneum. Following this, his scrotal pain and oedema began to diminish slowly.
Figure 1.

Clinical photograph showing scrotal swelling with a purple discoloration.
Figure 2.
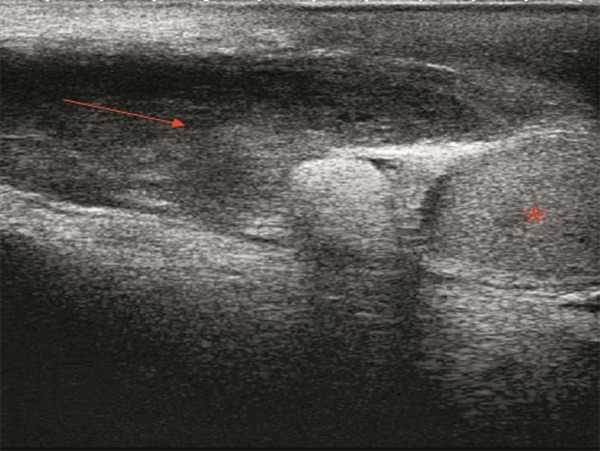
Ultrasound scan: a marked swelling of the left scrotal wall wrapped around the normal left testis and periorchium. And the swelling could be followed all the way up to the deep inguinal ring and into the abdomen. (The red * indicates the left testis, and the red arrow indicates swelling continuing through the abdomen).
Figure 3.
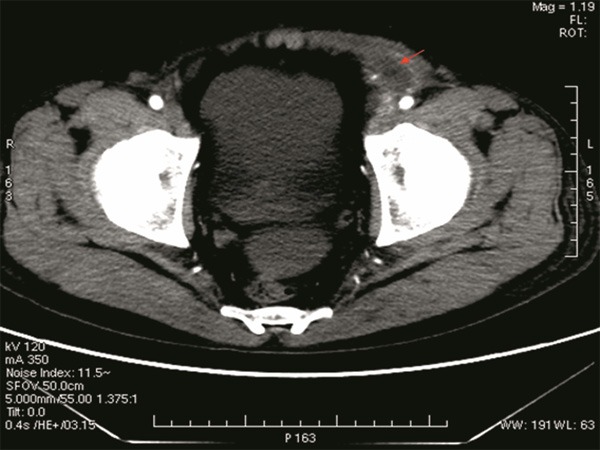
CT scan: swelling in the left inguinal canal.
Figure 4.
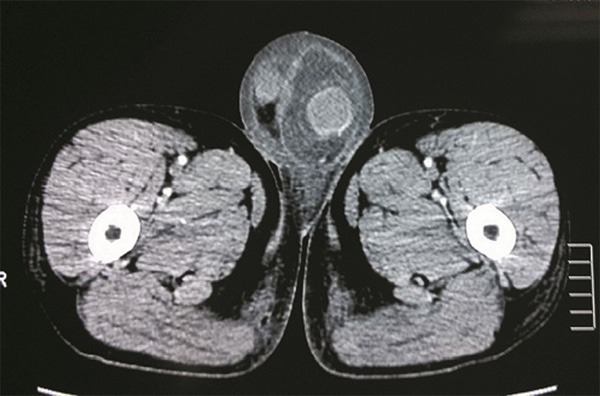
CT scan of the pelvis: extension of the pancreatic collection into the left scrotum with scrotal oedema.
He was kept fasting for 14 days and was treated conservatively by parenteral and enteral nutrition, trypsin inhibitor and antibiotic for 21 days. He was discharged until his general condition improved, and oral intake resumed. At the same time, the scrotal pain disappeared and swelling significantly diminished.
Discussion
Scrotal swelling is a rare complication of acute pancreatitis, with only a few cases reported in literature up to present [2-4]. As it may be misdiagnosed as other scrotal or testicular pathologies, mainly because the clinical presentation of this condition is indistinguishable from other more common causes of an acute scrotum. So early diagnosis and prompt treatment are vital to avoid unnecessary management.
In this case, the pathogenesis of this clinical entity was presumed to have two reasons. Firstly, ascites with pancreatic fluid in the retroperitoneal and pelvic space was assumed to extend down through inguinal canal into the scrotum along processus vaginalis [5]. We were informed the patient ever feeling that the left scrotum was little larger than the right by further questions about his medical history. So we surmised a potential hernia might be present in the left groin, although without other evidences. It might make it easy for ascites extending into the scrotum. Secondly, ascites with pancreatic fluid in the left retroperitoneal space might lead to local lymphangitis and vasculitis, which impacted lymphatic and venous return of the left scrotum. In the CT scan of this patient, we also found the left venae spermatic narrows. It could account for scrotal swelling in this patient to some extent.
We gained some experiences from this case that scrotal swelling might be caused by pancreatic fluid collections in patients with acute pancreatitis. Ultrasound and CT scan were useful in differential diagnosis for other scrotal or testicular pathologies, and could help to avoid unnecessary surgical management. Expectant treatment or local percutaneous drainage of the pancreatic collection may be the treatment of choice in these cases.
Disclosure of conflict of interest
None.
References
- 1.Robert JH, Frossard JL, Mermillod B. Early prediction of acute pancreatitis: prospective study comparing computed tomography scans, Ranson, Glascow, Acute Physiology and Chronic Health Evaluation II scores, and various serum markers. World J Surg. 2002;26:612–9. doi: 10.1007/s00268-001-0278-y. [DOI] [PubMed] [Google Scholar]
- 2.Kim SB, Je BK, Lee SH. Scrotal swelling caused by acute necrotizing pancreatitis: CT diagnosis. Abdom Imaging. 2011;36:218–21. doi: 10.1007/s00261-010-9638-0. [DOI] [PubMed] [Google Scholar]
- 3.Atiq M, Budhani I, Snyder R, Safdar K, Khan A, Chauhan S. Pancreatic hydrocele: an unusual manifestation of severe acute pancreatitis. Gastrointest Endosc. 2008;68:393–5. doi: 10.1016/j.gie.2007.11.030. [DOI] [PubMed] [Google Scholar]
- 4.Lee AD, Abraham DT, Agarwal S. The scrotum in pancreatitis: a case report and literature review. J Pancreas. 2004;5:337–59. [PubMed] [Google Scholar]
- 5.Skouras C, Skouras T, Pai M. Inguinoscrotal extension of a pancreatic collection: a rare complication of pancreatitis-case report andreview of the literature. Updates Surg. 2013;65:153–9. doi: 10.1007/s13304-012-0138-3. [DOI] [PubMed] [Google Scholar]