

Summary
Background
Unilateral invasion of the internal jugular vein (IJV) after subtotal thyroidectomy caused by local recurrence of papillary thyroid carcinoma is extremely rare. We report a case of papillary thyroid carcinoma which invades IJV with hypervascular tumor thrombus.
Case Report
We report a case of a 52-year-old woman with a history of previous thyroid operation who presented with a 2-month history of a painless, growing, hard, solitary mass on the left side of the neck. Clinical examination revealed also ipsilateral cervical lymphadenopathy. Radiological examination showed a necrotic and cystic mass arising from the operated area extending and invading the left jugular vein wall with hypervascular tumor thrombus. Cytological examination of the mass confirmed a papillary thyroid carcinoma (PTC) and enlarged metastatic lymph nodes. Therefore, total thyroidectomy with left neck dissection and segmental resection of the left internal jugular vein were performed, and the tumor thrombus was cleared successfully.
Conclusions
Invasion of IJV with hypervascular tumor thrombosis is an extremely rare condition in papillary thyroid carcinoma. Thrombosis of IJV is probably underdiagnosed. Early-stage diagnosis is important for long-term survival rates.
Keywords: Carcinoma, Papillary; Jugular Veins; Neoplasm Invasiveness; Thyroid Neoplasms
Background
Papillary thyroid carcinoma (PTC) is the most common histological subtype of thyroid carcinoma and it constitutes more than 85% of all cases [1]. The most common manifestation of thyroid cancers is a palpable thyroid nodule. Less frequently it can present as cervical cyst, distant metastasis, recurrent laryngeal nerve palsy, parapharyngeal mass, or isolated cervical lymphadenopathy [2]. Lymphatic spread is more common than hematogenous spread. Moreover, metastatic papillary thyroid carcinoma without any tumor focus in the thyroid gland has also been reported [3]. Local recurrence due to microscopic vascular invasion can be seen in papillary thyroid carcinoma after surgery; but invasion into great cervical veins or an artery from a local thyroid carcinoma recurrence is rare, but has a high mortality rate [4]. And most common are direct invasions from the outside wall of great vascular structures. Extraluminal vascular invasion by a locally spreading tumor is the most common in anaplastic thyroid cancers [5]. We describe a rare case of a 52-year-old woman with left internal jugular vein (IJV) spread of PTC.
Case Report
A case of a 52-year-old woman who underwent subtotal thyroidectomy 19 years ago and presented with a 2-month history of a painless, growing mass on the left side of the neck without any accompanying signs or symptoms. It is considered to be thyroid pathology due to a history of a previous thyroid operation. No distant metastases were confirmed. The patient was clinically and biochemically euthyroid. Serum thyroid function tests were within normal limits (TSH 0.4 Miu/L, free T3 3.5 pg/mL, free T4 1.4 ng/dL), but Anti-TPO level was high (567 iu/mL).
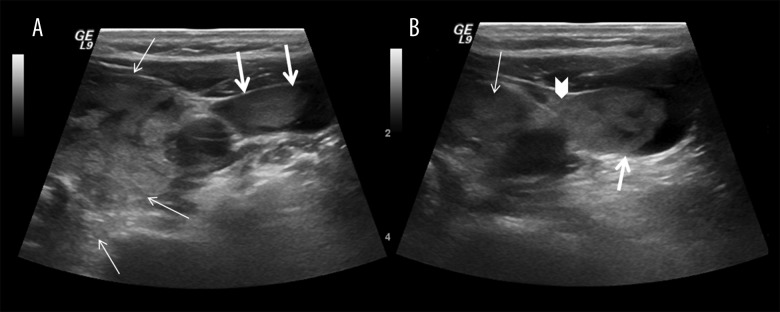
Ultrasonographic (US) examination revealed a 5.5×5.5 cm solitary mass with multiple areas of necrosis and cystic parts arising from the operated area, extending and invading the left jugular vein wall (Figure 1) displacing the left carotid artery posteriorly and laterally. It also showed multiple enlarged deep cervical lymph nodes. Color Doppler ultrasound revealed that the left internal jugular vein (IJV) was partially (approximately 80%) blocked with a tumor thrombus until the innominate vein (Figure 2), and the left common carotid artery was externally compressed by the mass. Moreover, the tumor thrombus was hypervascular in color Doppler ultrasound.
Figure 1.
Ultrasonographic (US) examination of neck, the solitary mass with multipl areas of necrosis and cystic parts (thin arrow) and the tumour thrombus of jugular vein (thick arrow) the invasion region of tumour to the jugular vein (arrow head).
Figure 2.

Color Doppler ultrasound of neck; (A) the longitudinal image of the left internal jugular vein (IJV) shows the hyperechoic filling defect and vascularization of tumour thrombus (thick arrow). (B) the transvers image of the vascularization of thyroid mass (thin arrow) and the invasion region (arrow head).
Subsequent Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) confirmed the angioinvasive solitary mass. MRI of the neck showed a heterogeneously-enhancing mass with a low signal intensity on T1-weighted images and a high signal intensity on T2-weighted images arising from the operated area, compressing and displacing the trachea to the right and invading the left IJV (Figure 3). A CT scan of the neck was performed and showed a large ill-defined heterogenous mass extending laterally to IJV and causing a filling defect (Figure 4).
Figure 3.
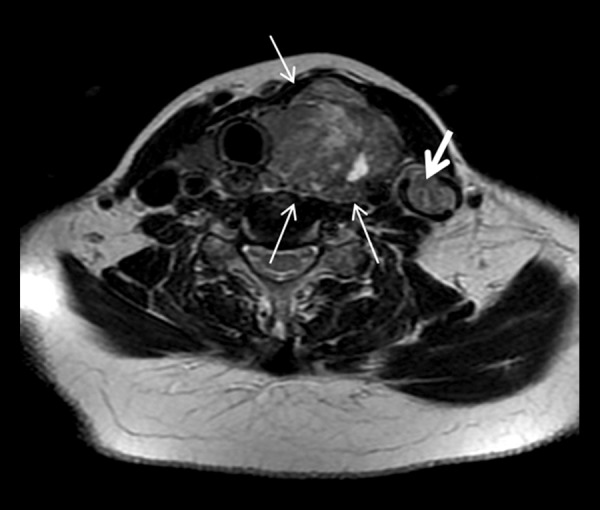
Transvers T2 weighted image of the neck shows a heterogeneous high signal intensity mass (thin arrow) which compresses and displaces the trachea to the right and similar signal intensity of the tumour thrombus (thick arrow) in the İJV and periferally luminal signal void area which shows the partially blood flow.
Figure 4.

Contrast enhanced CT scan of neck, sagittal (A) and transvers (B) images shows large ill defined heterogenous mass (thin arrow) and the extention of mass laterally into the IJV (arrow head) by causing filling defect (thick arrow).
Cytological examination of the mass confirmed the presence of papillary thyroid carcinoma (PTC) and papillary thyroid cells in the enlarged lymph node.
Surgery was considered for treatment. During surgery, surgeons found the mass and the lymph nodes deep in the left cervical regions, invading the left IJV. A left radical neck dissection with segmental resection of the left internal jugular vein that contained the tumor was carried out. Reconstruction of the left IJV with saphenous vein graft interposition was performed. The patient showed clinical improvement and the venous graft functioned normally. The postoperative pathologic examination revealed papillary carcinoma.
Discussion
Thyroid cancer can be a result of microscopic vascular invasion. However, macroscopic invasion and thrombus in the great cervical vascular structures is an extremely rare condition.
It is rare for thyroid carcinoma to result in occlusion of great vascular structures either by tumor invasion of the venous wall and thrombosis or extrinsic compression.
Invasion of IJV by thyroid cancer indicates a poor outcome [3]. Mortality is related to the degree of vascular invasion. Intravascular tumor extension usually starts at the thyroid veins with intraluminal invasion by malignant cells and deposition of fibrin, leading to continued growth [4]. Encapsulated tumor mass prevents the tumor cells from invading the adjacent vascular structures and making a total resection more possible [6]. Intravascular extension of tumor cells by direct intraluminal spread should be differentiated from extra luminal vascular invasion by a locally spreading tumor, more commonly encountered in anaplastic thyroid cancers; the management process may differ in both conditions [5]. On the other hand, PTC generally spreads via lymphatics and haematogenous spread leading to distant organ metastasis is rare. Direct extraluminal vascular invasion with PTC is extremely rare and can vary in extent from the thyroid vessels up to the right atrium [6].
Follicular and Hurthle cell carcinomas of the thyroid gland also have well-documented microscopic characteristics of microinvasion affecting the great cervical veins [5,6].
According to Graham, Kaufmann described the first case of thyroid cancer thrombi that occurred in a 58-year-old woman. An autopsy identified thyroid carcinoma with massive invasion into the superior vena cava and the right auricle, and into the internal jugular, subclavian, and innominate veins on both sides [7].
Neck US, MRI and CT can be performed for the diagnosis, and radiologists should attempt to detect signs of tumor thrombi in all patients with thyroid masses. CT can be useful to show a dilated vein with an intraluminal filling defect and adjacent mass. Absence of normal flow void on MR images can be very significant in showing venous thrombosis [8]. Color Doppler is able to demonstrate an absent flow in veins or even detect partial thrombosis. Preoperative US plays an important role in the diagnosis, and operators should take into account the presence of tumor thrombi in all patients with thyroid carcinoma [9].
IJV thrombosis without central venous catheterization may be the first manifestation of an occult malignancy [10] and it must be ruled out. There is a good correlation between malignancy and coagulation, 50% of the patients with malignancy and 90% of those with metastatic tumors have coagulation abnormalities while only 15% have any symptoms [11].
Cervical and arm edema and pain are the most common presentations of IJV thrombosis, which may also be completely asymptomatic, so the history and examination may be indeterminate [10].
The most effective treatment method of aggressive thyroid cancers is total surgical resection of the thyroid gland followed by TSH-suppression therapy and radioactive iodine ablation. Surgery with vascular repair has offered an increased survival rate and recovery rate in comparison with nonsurgical management and a minimum risk of mortal complications of intraluminal masses. The reported survival of patients with invasion of IJV or other great cervical veins by thyroid cancer is between 2 and 5 years [10]. Intraluminal extension is not a contraindication to aggressive surgical treatment in well-differentiated thyroid cancers due to the relatively good prognosis of PTC as well as to a decreased risk of superior vena cava obstruction, sudden death from airway occlusion, tumor embolism or fatal right atrial obstruction [5].
Conclusions
In conclusion, invasion of IJV is a rare condition and associated with poor prognosis. Ultrasonography is highly significant to show vascular invasion in patients with thyroid carcinoma. Radiologists should be attentive to a potential invasion of great vascular structures. Long-term survival rate can be increased by diagnosis at an early stage by radiologists.
References
- 1.Liang K, He L, Dong W, Zhang H. Risk factors of central lymph node metastasis in cN0 papillary thyroid carcinoma: a study of 529 patients. Med Sci Monit. 2014;20:807–11. doi: 10.12659/MSM.890182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Anil S, Radu B, Ricardo L. Metastatic papillary thyroid carcinoma with absence of tumor focus in thyroid gland. Am J Case Rep. 2013;14:73–75. doi: 10.12659/AJCR.883834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kebebew E, Clark OH. Locally advanced differentiated thyroid cancer. Surg Oncol. 2003;12:91–99. doi: 10.1016/s0960-7404(03)00032-x. [DOI] [PubMed] [Google Scholar]
- 4.Niederle B, Hausmaninger C, Kretschmer G, et al. Intraatrial extension of thyroid cancer: technique and results of a radical surgical approach. Surgery. 1990;108:951–56. [PubMed] [Google Scholar]
- 5.Gross M, Mintz Y, Maly B, et al. Internal jugular vein tumour thrombus associated with thyroid carcinoma. Ann Otol Rhinol Laryngol. 2004;113:738–40. doi: 10.1177/000348940411300912. [DOI] [PubMed] [Google Scholar]
- 6.Sugimoto S, Doihara H, Ogasawara Y, et al. Intraatrial extension of thyroid cancer: a case report. Acta Med Okayama. 2006;60:135–40. doi: 10.18926/AMO/30734. [DOI] [PubMed] [Google Scholar]
- 7.Graham A. Malignant epithelial tumours of the thyroid with special reference to invasion of blood vessels. Surg Gynecol Obstet. 1924;39:781–801. [Google Scholar]
- 8.Holt WL. Extension of malignant tumours of thyroid into great veins and heart. JAMA. 1934;102:1921–24. [Google Scholar]
- 9.Kobayashi K, Hirokawa M, Yabuta T, et al. Tumour thrombus of thyroid malignancies in veins: Importance of detection by ultrasonography. Thyroid. 2011;21:527–31. doi: 10.1089/thy.2010.0099. [DOI] [PubMed] [Google Scholar]
- 10.Boedeker CC, Ridder GJ, Weerda N, et al. Etiology and therapy of the internal jugular vein thrombosis. Laryngorhinootologie. 2004;83:743–49. doi: 10.1055/s-2004-825749. [in German] [DOI] [PubMed] [Google Scholar]
- 11.Carrington BM, Adams JE. Jugular vein thrombosis associated with distant malignancy. Postgrad Med J. 1988;64:455–58. doi: 10.1136/pgmj.64.752.455. [DOI] [PMC free article] [PubMed] [Google Scholar]