

Abstract
Birth order has been associated with childhood obesity. The objective of this cross-sectional study was to examine maternal feeding and child eating behaviors as underlying processes for increased weight status of only children and youngest siblings. Participants included 274 low-income 4-8 year old children and their mothers. The dyads completed a videotaped laboratory mealtime observation. Mothers completed the Caregiver's Feeding Styles Questionnaire and the Children's Eating Behavior Questionnaire. Child weight and height were measured using standardized procedures. Path analysis was used to examine associations of birth order, maternal feeding behaviors, child eating behavior, and child overweight/obese status. The association between only child status and greater likelihood of overweight/obesity was fully mediated by higher maternal Verbal Discouragement to eat and lower maternal Praise (all p values < 0.05). The association between youngest sibling status and greater likelihood of overweight/obesity was partially mediated by lower maternal Praise and lower child Food Fussiness (all p values < 0.05). Results provide support for our hypothesis that maternal control and support and child food acceptance are underlying pathways for the association between birth order and weight status. Future findings can help inform family-based programs by guiding family counseling and tailoring of recommendations for family mealtime interactions.
Keywords: Birth order, Feeding behavior, Eating behavior, Overweight, Obesity
Introduction
Childhood obesity rates in the United States (US) continue to be excessively high (Ogden, Carroll, Kit, & Flegal, 2014). Although evidence for effective intervention strategies is scarce, family-based programs can be effective in achieving and maintaining weight loss among preschool and school-age children (Epstein, Valoski, Wing, & McCurley, 1994; Kaplan, Arnold, Irby, Boles, & Skelton, 2013; Quattrin et al., 2012). Understanding how family structure is associated with child weight status can help inform family-based programs and allow efficient tailoring of recommendations that involve interactions between family members. Such interventions are especially needed for low-income children who may live in chaotic and unstable homes (Evans, 2004), and who are at higher risk for obesity (Ogden et al., 2014).
Birth order has been found to be associated with child overweight and obesity (Haugaard, Ajslev, Zimmermann, Angquist, & Sorensen, 2013; Hesketh, Crawford, Salmon, Jackson, & Campbell, 2007; Hunsberger et al., 2012; Mosli et al.; Ochiai et al., 2012). Although findings are inconsistent, studies that examined only children, oldest siblings, and youngest siblings in separate birth order categories found that only children and youngest siblings have higher risk of obesity compared to oldest siblings (Haugaard et al., 2013; Hesketh et al., 2007; Hunsberger et al., 2012; Mosli et al.; Ochiai et al., 2012). The underlying process for increased obesity risk of only children and youngest siblings is not well established (Chen & Escarce, 2010; Haugaard et al., 2013; Hunsberger et al., 2012). This is primarily due to the use of less comprehensive behavioral measures in previous studies and/or less discrete categorization of birth order (i.e., combining only children and oldest siblings in the same comparison group) (Chen & Escarce, 2010; Drucker, Hammer, Agras, & Bryson, 1999; Duke, Bryson, Hammer, & Agras, 2004; Haugaard et al., 2013; Hesketh et al., 2007; Hunsberger et al., 2012; Ochiai et al., 2012). Evidence from social science research suggests that children within the same family can experience a non-shared home environment and dissimilar parenting behavior (Dunn & Plomin, 1991; Hotz & Pantano, 2013; Kidwell, 1981). Such behavioral variations might explain the association between birth order and weight status.
Parents often use different disciplinary strategies with first-born compared to later born children (Hotz & Pantano, 2013; Kidwell, 1981), and siblings may interact differently among each other depending on their sex and birth order (Kidwell, 1981). Only children experience a unique home environment, which may be characterized by greater parental attention (Trent & Spitze, 2011). Greater parental attention may be manifested in well-established rules and boundaries. On the other hand, the home environment of a youngest sibling might be characterized by less parental involvement and less stringent parenting practices compared to first-born children (Hotz & Pantano, 2013). The home environment of a youngest sibling also includes the presence of older siblings who can act as potent role models and secondary caretakers (Abramovitch, Corter, & Lando, 1979; Dunn, 1983). These distinctive behavioral interaction features of the home environment may also operate in the mealtime context and play a role in shaping child weight status.
Highly demanding and controlling parental feeding practices, such as restriction and pressure to eat, have been associated with maladaptive eating behaviors and higher weight status among children (Drucker et al., 1999; Fisher & Birch, 1999, 2002; Johnson & Birch, 1994). It has been suggested that such parenting practices may alter the child's ability to self-regulate and respond to internal satiety cues, leading to overeating and weight gain (Drucker et al., 1999; Faith, Scanlon, Birch, Francis, & Sherry, 2004; Fisher & Birch, 1999, 2002; Johnson & Birch, 1994). However, appropriate control that is exerted in a warm and supportive manner has been associated with a healthy weight status, such that adaptive parental involvement and praise may encourage internalized control and healthy eating behaviors (Patrick, Nicklas, Hughes, & Morales, 2005; Rhee, Lumeng, Appugliese, Kaciroti, & Bradley, 2006; Stanek, Abbott, & Cramer, 1990; Vereecken, Keukelier, & Maes, 2004).
In the context of general parenting, only children compared to youngest siblings experience different degrees of parent control and involvement (Conley & Glauber, 2006; Hotz & Pantano, 2013; Kidwell, 1981). Therefore, we hypothesized that feeding-specific parenting might show the same pattern. That is, excessive control and/or inadequate involvement during mealtimes may act as potential mediators in the association between only child or youngest sibling status and child overweight or obesity.
Another potential pathway involving mealtimes through which birth order might predict child weight status is the child's own eating behavior. The way a child behaves towards food (e.g., his/her response to satiety cues) can influence the quantity and quality of food consumed (Birch & Fisher, 1998; Wardle, Guthrie, Sanderson, & Rapoport, 2001), and child eating behavior is associated with weight status and obesity risk (Birch & Fisher, 1998; Johnson & Birch, 1994; Wardle et al., 2001). Children are known to alter their eating behavior in response to the presence of other children (Salvy, Vartanian, Coelho, Jarrin, & Pliner, 2008; Birch, 1980; Lumeng & Hillman, 2007). Since older siblings are known to exert powerful role-modeling influences on younger siblings (Abramovitch et al., 1979; Birch, 1980), and older children typically consume larger quantities of food than younger children (Piernas & Popkin, 2011), youngest siblings may be imitating the behavior of older siblings and eat larger quantities of food in the presence of their older siblings. Therefore, the eating behavior of youngest siblings might be characterized by high acceptance of food and increased food intake. Only children may also exhibit unique eating behaviors due to the absence of other children during home meals. For example, only children may be more likely to eat alone, and among school-aged children, eating alone has been associated with lower satiety responsiveness and increased food intake in the absence of hunger (Tanofsky-Kraff et al., 2007)(i.e., decreased use of internal signals of hunger and satiety as a basis for adjusting energy intake and responding with a desire to eat when a palatable food becomes freely available, even when not feeling physically hungry (Birch & Fisher, 1998; Fisher & Birch, 1999)). We therefore hypothesized that child eating behavior is a potential mediator in the association between birth order and child weight status.
In summary, the present study examined maternal feeding and child eating behaviors as underlying processes that may contribute to increased weight status of only children and youngest siblings.
Methods
Participants and Procedures
The study sample included 301 child-mother dyads recruited through Head Start programs in South-Central Michigan. Head Start is a federally funded preschool program for low-income, high-risk families in the US. Children were between the ages of 4 and 8 years old at the time of data collection. Inclusion criteria were: caregiver is fluent in English and has less than a college degree; and child is not in foster care, was born at ≥ 35 weeks gestation without significant perinatal or neonatal complications, and has no serious medical problems or history of food allergies. We limited the sample to participants living with their biological mothers with complete data on all variables (n = 277), as this represented the majority of the sample. Three children who only had same age siblings were also excluded, leaving a final analytic sample of 274, which did not differ from the sample not included (n = 27) with regard to child sex, child race/ethnicity, or maternal education. Mothers completed informed consents for themselves and for their children, and each mother was compensated $150 for participating in all study procedures. The University of Michigan Institutional Review Board approved this study.
Measures
Demographic Characteristics
Mothers reported the child's birthdate, sex and race/ethnicity as well as information. regarding individuals living in the household, including each individual's age and relationship to the index child. This information was used to categorize each index child into one of the birth order categories: only child, youngest sibling, middle sibling (defined as having at least 1 older sibling and at least 1 younger sibling), and oldest sibling. Mothers also reported their own birthdate and years of education.
Maternal Feeding Behaviors
Maternal feeding behaviors were coded during an observational eating protocol and assessed using a self-report questionnaire.
Observed Feeding Behavior
Each child-mother dyad participated in a structured eating protocol from which maternal feeding behavior was later coded. Dyads were seated at a table in a quiet room and video-recorded while sampling 4 different types of foods presented individually and sequentially in random order. The 4 types of food included a generic familiar and unfamiliar vegetable, and a generic familiar and unfamiliar dessert. This approach uniquely provides an opportunity to assess the mother's feeding practices with the target child in a standardized procedure that may elicit a range of feeding practices with different types of food. Bob and Tom's Method of Assessing Nutrition (BATMAN)(Klesges et al., 1983) was used to code maternal behavior during the meal. The BATMAN is an observational assessment that evaluates certain parent behaviors that may modify the child's eating behavior (Klesges et al., 1983). Verbal Encouragement and Verbal Discouragement are behaviors evaluated by the BATMAN that we included in this analysis. Other behaviors evaluated by the BATMAN, such as physical discouragement, were observed to be relatively rare and thus have been excluded from this analysis. Verbal Encouragement is operationalized as directing, suggesting, commanding, and making positive statements in order to get the child to eat. Verbal Discouragement is operationalized as forbidding, scolding, refusing, and making negative statements about, or verbally limiting the child from eating the food. Two coders rated each of these behaviors during the time periods when child-mother dyads were observed with each of the 4 foods and behaviors were summed across foods. Inter-rater reliability was calculated for 20% of tapes. Intraclass correlation coefficients (ICC) for both Verbal Encouragement and Verbal Discouragement were each 1.0, indicating perfect agreement (Cicchetti, 1994).
Self-Reported Feeding Behavior
Mothers completed the Caregiver's Feeding Styles Questionnaire (CFSQ), an instrument specifically developed to assess feeding styles among low-income families (Hughes et al., 2005), with 5-point Likert response scales ranging from 1 = never to 5 = always. The scale is typically used to characterize mothers’ general feeding behaviors as more or less demanding and responsive. For the purposes of the current study, we sought to examine specific feeding behaviors in more detail. Thus, we conducted a factor analysis that generated three subscales reflecting specific dimensions of maternal feeding behavior: verbal direction, coercion, and praise. Scores were calculated as the mean of contributing items, with higher scores reflecting more of the given behavior. The Verbal Direction score consisted of 4 items (Cronbach's α= 0.74) concerning how often mothers verbally suggest or command the child to eat. The Coercion score consisted of 5 items (Cronbach's α= 0.82) concerning how often mothers use threats, bribes, and food as a reward in order to get the child to eat. Finally, the Praise score consisted of 2 items (Cronbach's α= 0.73) concerning how often mothers say something positive about the child or the food.
Child Eating Behavior
Mothers completed the Children's Eating Behavior Questionnaire (CEBQ); a 35-item questionnaire frequently used to assess eating styles in children through parental report (Wardle, Guthrie, Sanderson, & Rapoport, 2001), with 5-point Likert response scales ranging from 1 = never to 5 = always. The CEBQ generates subscales by calculating the mean of the contributing items, with higher scores reflecting more of the given behavior. In this analysis, we examined 3 subscales that evaluate behaviors that are salient in peer interactions, and which a child might modify in response to presence of an older sibling role model. For example, in the presence of older children, younger children may eat faster and eat a larger quantity of food (Lumeng & Hillman, 2007). Children may also alter their food preferences in response to observing foods consumed by older children role models (Birch, 1980). Therefore, the 3 subscales we examined were Slowness in Eating, which includes 4 items (Cronbach's α = 0.76) concerning the child's speed of eating; Satiety Responsiveness, which includes 5 items (Cronbach's α = .73) concerning how often the child finishes meals and maternal perceptions of the child's appetite; and Food Fussiness, which includes 6 items (Cronbach's α = .85) concerning the willingness of the child to eat different types of foods and novel foods.
Anthropometry
Trained staff members measured child weight and height following standardized procedures. Shoes and heavy clothing were removed. Each child was weighed twice and if the two readings were inconsistent by more than 0.1 kg, the individual was weighed two more times. Similarly, height was measured twice and if the measurements differed by more than 0.5 cm, two more measurements were taken. Body mass index (BMI) was calculated by dividing weight (kg) by height in meters, squared. To categorize children's weight status, percentiles were derived based on the US Centers for Disease Control and Prevention age and sex specific growth charts (Ogden & Flegal, 2010). A BMI ≥ the 85th percentile for age and sex was categorized as overweight/obese (OWOB). Mothers reported the child's birth weight, which was converted to z-scores based on National Centers for Health Statistics Natality Datasets (Oken, Kleinman, Rich-Edwards, & Gillman, 2003). Birth weight z-scores were missing and were imputed for 26 subjects using multiple imputations.
Statistical Analysis
Descriptive analyses were conducted using IBM SPSS Statistics 21.0 (Armonk, NY, USA). We examined characteristics of the full sample by calculating the distribution of demographic characteristics, birth weight z-score, birth order, and maternal feeding and child eating behavior variables. We tested differences in these variables by child OWOB status; by running t-tests for continuous variables and Chi-square tests for categorical variables. In addition, we used Analysis of Variance (ANOVA) to detect significant differences in maternal feeding and child eating behaviors by 4-category birth order.
We used path analysis to examine processes underlying the association between birth order and child OWOB. Specifically, we conducted path analysis in MPLUS version 7.2 (Muthen & Muthen, Los Angeles, CA, USA) to test both the direct and indirect associations between birth order, maternal feeding behaviors, child eating behavior, and child OWOB status. Significance level was set at 0.05. Birth order, the predictor in the model, was included as a categorical variable with “oldest sibling” as the reference category. We screened potential meditators by identifying maternal feeding behavior and child eating behavior variables that differed by both child OWOB status and child birth order (using a conservative p < 0.15) and included them in the path model. We used the Bayesian estimation technique to fit the path model, as it contained both binary and continuous variables. The model was adjusted for child race/ethnicity, child sex, and child birth weight z-score. Paths between variables and child OWOB status that were non-significant and did not improve goodness of fit were removed in order to obtain the most parsimonious model with better fit. We conducted Bayesian posterior predictive checks (PPC) using Chi-square statistics and the corresponding posterior predictive p-values to assess goodness of fit of the model (Gelman, 2004).
Results
The final sample size was 274. Mean child age was 5.4 years, and the prevalence of OWOB was 42.3%. Table 1 shows the distribution of demographic characteristics, birth weight z-score, birth order, maternal feeding and child eating behaviors for the total sample, as well as by OWOB status. In bivariate analyses, birth order, maternal feeding and child eating behaviors were associated with OWOB status (Table 1), and maternal feeding and child eating behaviors were associated with birth order (Table 2).
Table 1.
* Demographic, Birth Weight Z-Score, Birth Order, Maternal Feeding, and Child Eating Characteristics of the Full Sample and Differences by Overweight/Obese status
| Variables | Total n = 274 | BMI < 85th Percentile n = 158 | BMI ≥ 85th Percentile n = 116 | P-value |
|---|---|---|---|---|
| Child Sex, n (%) | ||||
| Male | 139 (50.7) | 88 (55.7) | 51 (44) | 0.06 |
| Female | 135 (49.3) | 70 (44.3) | 65 (56) | |
| Child Race/Ethnicity, n (%) | ||||
| Non-Hispanic white | 147 (53.6) | 91 (57.6) | 56 (48.3) | 0.13 |
| Hispanic or not white | 127 (46.4) | 67 (42.4) | 60 (51.7) | |
| Birth Order, n (%) | ||||
| Only child | 39 (14.2) | 16 (10.1) | 23 (19.8) | 0.02 |
| Youngest sibling | 100 (36.5) | 53 (33.5) | 46 (39.7) | |
| Middle sibling | 66 (24.1) | 41 (25.9) | 25 (21.6) | |
| Oldest sibling | 69 (25.2) | 48 (30.4) | 21 (18.1) | |
| Birth weight z score, M (SD) | −0.27 (1.02) | −0.44 (0.91) | −0.042 (1.12) | 0.00 |
| Maternal Age, M (SD) | 30.3 (5.8) | 30.5 (6.3) | 30.02 (5.2) | 0.47 |
| Maternal Education, n (%) | ||||
| ≤ High school education | 130 (47.4) | 99(62.7) | 51(44) | 0.27 |
| > High school education | 144 (52.6) | 59(37.3) | 65(56) | |
| Maternal feeding behaviors1, M (SD) Observed | ||||
| Verbal Encouragement | 10.24 (8.53) | 10.63 (8.94) | 9.74 (7.97) | 0.45 |
| Verbal Discouragement | 3.01 (4.30) | 2.52 (3.45) | 3.66(5.17) | 0.05 |
| Self-Reported (CFSQ) | ||||
| Verbal Direction | 2.79 (0.81) | 2.88 (0.78) | 2.66 (0.83) | 0.02 |
| Coercion | 2.12 (0.82) | 2.19 (0.82) | 2.03 (0.83) | 0.11 |
| Praise | 3.94 (0.91) | 4.03 (0.86) | 3.81 (0.97) | 0.06 |
| Child eating behavior (CEBQ)2, M (SD) | ||||
| Satiety Responsiveness | 2.80 (0.64) | 2.89 (0.63) | 2.67 (0.63) | 0.00 |
| Slowness in Eating | 2.83 (0.73) | 2.89 (0.74) | 2.74 (0.72) | 0.09 |
| Food Fussiness | 2.70 (0.76) | 2.80 (0.72) | 2.58 (0.79) | 0.02 |
Table showing means (M) and standard deviations (SD) or counts (n) and percentages (%). Differences by overweight/obese status tested using t-tests for continuous variables and Chi-square tests for categorical variables.
Observed maternal feeding behavior was coded from the structured eating protocol attended by each child-mother dyad.
Verbal Encouragement range= 46, Verbal Discouragement range= 27, Verbal Direction range=4, Coercion range=4, Praise range=4.
Satiety Responsiveness range=4, Slowness in Eating range=4, Food Fussiness range=4.
Table 2.
* Differences in Maternal Feeding and Child Eating Behaviors by Birth Order
| Variables | Only child | Youngest sibling | Middle sibling | Oldest sibling | P-value |
|---|---|---|---|---|---|
| Maternal feeding behavior, M (SD) Observed | |||||
| Verbal encouragement | 7.93 (5.88) a | 9.35 (7.62) | 9.98 (8.15) | 13.41 (10.78) b | 0.02 |
| Verbal discouragement | 5.03 (7.46) a | 2.68 (3.09) | 3.07 (4.42) | 2.27 (2.76) b | 0.03 |
| Self-Reported | |||||
| Verbal direction | 2.82 (0.72) | 2.76 (0.81) | 2.73 (0.88) | 2.86 (0.80) | 0.81 |
| Coercion | 2.04 (0.76) | 2.05 (0.79) | 2.14 (0.92) | 2.24 (0.81) | 0.48 |
| Praise | 3.73 (0.99) | 3.80 (0.82) | 4.14 (0.81) | 4.06 (1.03) | 0.03 |
| Child eating behavior, M (SD) | |||||
| Satiety responsiveness | 2.74 (0.57) | 2.89 (0.66) | 2.67 (0.65) | 2.82 (0.61) | 0.15 |
| Slowness in eating | 2.93 (0.65) | 2.90 (0.69) | 2.76 (0.81) | 2.74 (0.76) | 0.34 |
| Food fussiness | 2.83 (0.80) | 2.64 (0.80) | 2.52 (0.76) | 2.90 (0.62) | 0.02 |
Table showing means (M) and standard deviations (SD). Significance of differences between birth order groups tested by ANOVA.
Discrepant letters indicate that the difference between means is statistically significant (P-value < 0.05).
Discrepant letters indicate that the difference between means is statistically significant (P-value < 0.05).
Variables that met the first prerequisite for mediation, an association with birth order, included maternal Verbal Encouragement, maternal Verbal Discouragement, maternal Praise, and child Food Fussiness. However, only 3 of these variables also met the second prerequisite for mediation, an association with OWOB status. These variables were maternal Verbal Discouragement, maternal Praise, and child Food Fussiness. We thus proceeded with the 3 variables to build our path model. Results of the path analysis are shown in Figure 1. The path model showed good fit, with a posterior predictive p-value equal to 0.67, well within the 0.05-0.95 range.
Fig. 1.
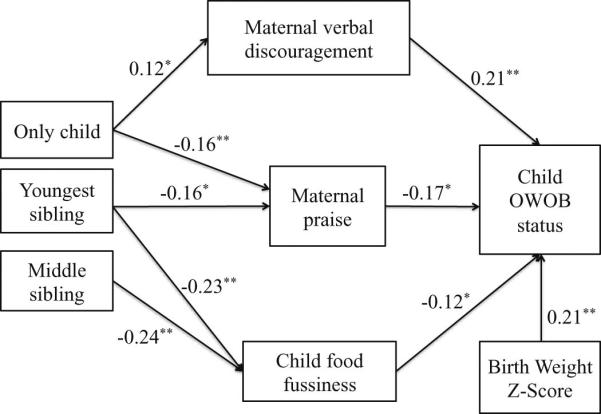
Path model showing standardized coefficients for associations between birth order, maternal feeding behavior, child eating behavior, and child overweigh/obese status.
* p ≤ 0.05
** p ≤ 0.01
As shown in Figure 1, only child status was associated with higher maternal Verbal Discouragement. Only child and youngest sibling status were associated with lower maternal Praise. In addition, youngest sibling and middle sibling status were associated with lower child Food Fussiness. Higher maternal Verbal Discouragement and lower maternal Praise and child Food Fussiness were associated with greater likelihood of child OWOB. There was a marginally significant direct association between youngest sibling status and child OWOB (Standardized β: 0.14, 95% confidence interval (CI): −0.024, 0.34, p-value: 0.08). The association between child sex and OWOB status was not significant (p-value: 0.26), and was therefore removed from the model. Child birth weight z-score was positively associated with OWOB (Standardized β: 0.21, 95% CI: 0.09-0.36, p < 0.001). Non-significant control variables were not in the final model (Figure 1).
In summary, the association between only child status and OWOB was eliminated once maternal Verbal Discouragement and Praise were entered into the model, suggesting that the association between only child status and greater likelihood of OWOB was fully mediated by higher maternal Verbal Discouragement and lower maternal Praise. Moreover, the association between youngest sibling status and OWOB was diminished after including maternal Praise and child Food Fussiness in the model, suggesting that the association between youngest sibling status and greater likelihood of OWOB was partially mediated by lower maternal Praise and lower child Food Fussiness.
Discussion
Results provided support for our hypothesis that the mealtime interaction features play a role in the association between birth order and child overweight/obesity. Specifically, we found that birth order was associated with maternal feeding behaviors and child eating behavior, which in turn were associated with child OWOB.
For only children, we found that maternal control and involvement were involved in the pathway of association between only child status and greater likelihood of OWOB. Mothers of only children were observed to use more verbal discouragement to eat during videotaped laboratory sessions. This type of maternal behavior is consistent with a previous study that found that only children were more likely to have parents supportive of food as a reward (as reported by parents via rating 8 statements pertaining to attitudes regarding using food as a reward) (Hunsberger et al., 2012). Others found that first-born children were observed to experience more verbal encouragement to eat from their mothers (Drucker et al., 1999; Duke et al., 2004), which can also represent increased maternal control. However, in these previous reports, only children and oldest siblings were both included in the definition of “first-born” children, and findings thus may not necessarily apply uniquely to only children. The present study thus elaborated on prior work in at least two ways, first by addressing methodological limitations by using observational and self-reported assessment of maternal behavior and second by examining only children separately from oldest siblings.
Although excessive control has been consistently associated with higher risk of child obesity (Drucker et al., 1999; Fisher & Birch, 1999, 2002; Johnson & Birch, 1994), maternal support and praise has been associated with a healthy diet and weight status among children (Rhee et al., 2006; Patrick et al., 2005; Stanek et al., 1990; Vereecken et al., 2004). Mothers of only children in this study reported praising their children less frequently compared to mothers of oldest siblings, and only children were in turn more likely to be OWOB. The measure of praise used in this study included mothers’ positive comments about healthy eating behavior and praise of healthy foods in front of the child. Thus, less-frequent praise of healthy eating behavior for only children may reflect less focus on these topics that may be important for the development of healthy eating behaviors (Patrick et al., 2005; Stanek et al., 1990; Vereecken et al., 2004).
Similarly, among youngest siblings, maternal support and praise may play a role in the pathway of association between younger sibling status and higher weight status. As with only children, mothers of youngest siblings also reported praising their children less frequently compared to mothers of oldest siblings, and youngest siblings were in turn more likely to be OWOB. In addition, we found that child eating behavior might underlie the association between youngest sibling status and higher likelihood of OWOB. Mothers of youngest siblings reported that their children were less fussy about food and were more likely to consume unfamiliar foods than did mothers of oldest siblings. Although lower food fussiness can be associated with higher consumption of fruits and vegetables (Galloway, Yoonna, & Birch, 2003), it may also be associated with increased food intake in general and higher weight status (Galloway, Fiorito, Lee, & Birch, 2005). Lower food fussiness has been previously associated with higher BMI among preschoolers and school-age children (Dubois, Farmer, Girard, Peterson, & Tatone-Tokuda., 2007; Galloway et al., 2005; Webber, Hill, Jaarsveld, & Wardle, 2008). Although no prior study has examined food fussiness as a potential pathway for increased weight among youngest siblings, earlier studies have found that children tend to eat more when older children are present (Birch, 1980; Salvy et al., 2008). Therefore, lower food fussiness among youngest siblings may reflect youngest siblings modifying their eating behavior in response to their birth order status, for example by modeling what their older siblings do.
Our study has several limitations. First, this is a cross-sectional study that cannot test causality. There might also have been other potential mediators that were not examined in this analysis, and while our study only included maternal feeding behavior, the behavior of other family members (e.g., the father) might contribute to the underlying pathways. Future studies that measure additional possible mediating processes and use longitudinal designs are needed to further support our findings. Second, our study cohort only included low-income Head Start families who chose to respond to a flyer inviting them to participate in a research study about children's eating behavior. Thus, our findings may not be generalizable to families without these characteristics. Finally, our sample size is relatively small. Larger studies with higher power would be helpful in examining pathways in more detail.
Strengths of this study include our use of multiple methods and more accurate definitions of birth order categories in order to examine processes that could explain associations between child birth order and weight status. We have included both observational and self-report measures to examine maternal and child behaviors as pathways underlying the association between birth order and weight status. Finally, our low-income, racially diverse sample had a high prevalence of overweight/obesity.
Including multiple family members as part of obesity treatment programs can be associated with more positive child outcomes (Kaplan, Arnold, Irby, Boles, & Skelton, 2013). Since our findings suggest that mothers of only children may use more restrictive feeding practices, and that these only children are at higher risk of obesity, counseling mothers of only children about these associations may strengthen prevention and intervention programs. Although mothers may use restrictive feeding practices as a reaction to the child being already overweight (Faith et al., 2004), these types of feeding behaviors are believed to further promote obesogenic eating behaviors and result in additional weight gain over time (Fisher & Birch, 2002). Educating mothers of only children on how to adopt less demanding and more supportive feeding behaviors may be helpful. Furthermore, since our findings suggest that last-born children may be more willing to consume a variety of different types of foods, researchers and practitioners may recommend that mothers of last-born children be especially mindful of available food choices. In addition, since the child's eating behavior may drive maternal restriction (Gregory, Paxton, & Brozovic, 2010), discussing how to respond to the child's eating behavior (e.g., greater food intake) with mothers of last-born children is warranted.
Conclusion
The association between child birth order and weight status might operate through maternal control and support and child food fussiness during mealtime. Results of our study can provide a framework for researchers and practitioners to consider when designing family-based programs for overweight or obese children. Interventions that are sensitive to the relationship between family structure and mealtime behaviors of family members may be more successful and may contribute to efforts that aim to lower childhood obesity rates.
Highlights.
Association of birth order with weight status mediated by mealtime behaviors.
Only child status associated with higher maternal discouragement and lower praise.
Youngest sibling status associated with lower praise and child food fussiness.
Only children and youngest siblings are more likely to be overweight/obese.
Acknowledgments
RM designed the study, analyzed the data, and drafted the initial manuscript. JL, AM, and KR designed the data collection instruments, coordinated and supervised data collection, and critically reviewed the manuscript. NK, KP, and AB provided input on the analysis plan and critically reviewed the manuscript. All authors have approved the final manuscript as submitted. This study was supported by NIH grant 5R01HD061356.
Abbreviations
- BATMAN
Bob and Tom's Method of Assessing Nutrition
- CFSQ
Caregiver's Feeding Styles Questionnaire
- CEBQ
Children's Eating Behavior Questionnaire
- OWOB
overweight/obese
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of Interest
No conflict of interest was declared.
References
- Abramovitch R, Corter C, Lando B. Sibling interaction in the home. Child Development. 1979:997–1003. [Google Scholar]
- Birch LL. Effects of peer models' food choices and eating behaviors on preschoolers' food preferences. Child Development. 1980;51:489–496. [Google Scholar]
- Birch LL, Fisher JO. Development of eating behaviors among children and adolescents. Pediatrics. 1998;101(2):539–549. [PubMed] [Google Scholar]
- Chen AY, Escarce JJ. Family structure and childhood obesity, Early Childhood Longitudinal Study — Kindergarten Cohort. Preventing Chronic Disease. 2010;7(3) [PMC free article] [PubMed] [Google Scholar]
- Cicchetti DV. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychological Assessment. 1994;6(4):284–290. [Google Scholar]
- Conley D, Glauber R. Parental educational investment and children's academic risk estimates of the impact of sibship size and birth order from exogenous variation in fertility. Journal of Human Resources. 2006;41(4):722–737. [Google Scholar]
- Drucker RR, Hammer LD, Agras SW, Bryson S. Can mothers influence their child's eating behavior? Journal of Developmental and Behavioral Pediatrics. 1999;20(2):88–92. doi: 10.1097/00004703-199904000-00003. [DOI] [PubMed] [Google Scholar]
- Dubois L, Farmer A, Girard M, Peterson K, Tatone-Tokuda F. Problem eating behaviors related to social factors and body weight in preschool children: A longitudinal study. International Journal of Behavioral Nutrition and Physical Activity. 2007;4(1):9. doi: 10.1186/1479-5868-4-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duke RE, Bryson S, Hammer DL, Agras WS. The relationship between parental factors at infancy and parent-reported control over children's eating at age 7. Appetite. 2004;43(3):247–252. doi: 10.1016/j.appet.2004.05.006. [DOI] [PubMed] [Google Scholar]
- Dunn J. Sibling relationships in early childhood. Child Development. 1983:787–811. [Google Scholar]
- Dunn J, Plomin R. Why are siblings so different? the significance of differences in sibling experiences within the family. Family Process. 1991;30(3):271–283. doi: 10.1111/j.1545-5300.1991.00271.x. [DOI] [PubMed] [Google Scholar]
- Epstein LH, Valoski A, Wing RR, McCurley J. Ten-year outcomes of behavioral family-based treatment for childhood obesity. Health Psychology. 1994;13(5):373–383. doi: 10.1037//0278-6133.13.5.373. [DOI] [PubMed] [Google Scholar]
- Evans GW. The environment of childhood poverty. American Psychologist. 2004;59(2):77. doi: 10.1037/0003-066X.59.2.77. [DOI] [PubMed] [Google Scholar]
- Faith MS, Scanlon KS, Birch LL, Francis LA, Sherry B. Parent-child feeding strategies and their relationships to child eating and weight status. Obesity Research. 2004;12(11):1711–1722. doi: 10.1038/oby.2004.212. [DOI] [PubMed] [Google Scholar]
- Fisher J, Birch L. Restricting access to foods and children's eating. Appetite. 1999;32(3):405–419. doi: 10.1006/appe.1999.0231. [DOI] [PubMed] [Google Scholar]
- Fisher J, Birch L. Eating in the absence of hunger and overweight in girls from 5 to 7 y of age. The American Journal of Clinical Nutrition. 2002;76:226–231. doi: 10.1093/ajcn/76.1.226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galloway AT, Fiorito L, Lee Y, Birch LL. Parental pressure, dietary patterns, and weight status among girls who are “picky eaters”. Journal of the American Dietetic Association. 2005;105(4):541–548. doi: 10.1016/j.jada.2005.01.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galloway AT, Yoonna L, Birch LL. Predictors and consequences of food neophobia and pickiness in young girls. Journal of the American Dietetic Association. 2003;103(6):692–698. doi: 10.1053/jada.2003.50134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gelman A. Bayesian data analysis. Chapman & Hall/CRC; Boca Raton, Fla: 2004. [Google Scholar]
- Gregory JE, Paxton SJ, Brozovic AM. Pressure to eat and restriction are associated with child eating behaviours and maternal concern about child weight, but not child body mass index, in 2-to 4-year-old children. Appetite. 2010;54(3):550–556. doi: 10.1016/j.appet.2010.02.013. [DOI] [PubMed] [Google Scholar]
- Haugaard LK, Ajslev TA, Zimmermann E, Angquist L, Sorensen TI. Being an only or last-born child increases later risk of obesity. PloS One. 2013;8(2):e56357. doi: 10.1371/journal.pone.0056357. doi: 10.1371/journal.pone.0056357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hesketh K, Crawford D, Salmon J, Jackson M, Campbell K. Associations between family circumstance and weight status of Australian children. International Journal of Pediatric Obesity. 2007;2(2):86–96. doi: 10.1080/17477160601148554. [DOI] [PubMed] [Google Scholar]
- Hotz J, Pantano J. Strategic parenting, birth order and school performance: NBER Working Paper. The National Bureau of Economic Research; 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hughes SO, Power T, Fisher J. Revisiting a neglected construct: Parenting styles in a childfeeding context. Appetite. 2005;44:83–92. doi: 10.1016/j.appet.2004.08.007. [DOI] [PubMed] [Google Scholar]
- Hughes SO, Shewchuk RM, Baskin ML, Nicklas TA, Qu H. Indulgent feeding style and children's weight status in preschool. Journal of Developmental and Behavioral Pediatrics. 2008;29(5):403. doi: 10.1097/DBP.0b013e318182a976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hunsberger M, Formisano A, Reisch LA, Bammann K, Moreno L, De Henauw S, Lissner L. Overweight in singletons compared to children with siblings: The IDEFICS study. Nutrition & Diabetes. 2012;2:e35. doi: 10.1038/nutd.2012.8. doi: 10.1038/nutd.2012.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson SL, Birch LL. Parents' and children's adiposity and eating style. Pediatrics. 1994;94(5):653–661. [PubMed] [Google Scholar]
- Kaplan SG, Arnold EM, Irby MB, Boles KA, Skelton JA. Family systems theory and obesity treatment applications for clinicians. Infant, Child, & Adolescent Nutrition. 2013 doi: 10.1177/1941406413516001. doi: 10.1177/1941406413516001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kidwell J. Number of siblings, sibling spacing, sex, and birth order: Their effects on perceived parent adolescent relationships. Journal of Marriage and the Family. 1981:315–332. [Google Scholar]
- Klesges RC, Coates TJ, Brown G, Sturgeon - Tillisch J, Moldenhauer - Klesges LM, Holzer B, Vollmer J. Parental influences on children's eating behavior and relative weight. Journal of Applied Behavior Analysis. 1983;16(4):371–378. doi: 10.1901/jaba.1983.16-371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lumeng JC, Hillman KH. Eating in larger groups increases food consumption. Archives of Disease in Childhood. 2007;92(5):384–387. doi: 10.1136/adc.2006.103259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mosli RH, Miller AL, Peterson KE, Kaciroti N, Rosenblum K, Baylin A, Lumeng JC. Birth order and sibship composition as predictors of overweight or obesity among low-income 4- to 8-year-old children. Pediatric Obesity. doi: 10.1111/ijpo.12018. doi: 10.1111/ijpo.12018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ochiai H, Shirasawa T, Ohtsu T, Nishimura R, Morimoto A, Obuchi R, Kokaze A. Number of siblings, birth order, and childhood overweight: a population-based cross-sectional study in Japan. BMC Public Health. 2012;12:766. doi: 10.1186/1471-2458-12-766. doi: 10.1186/1471-2458-12-766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA. 2014;311(8):806–814. doi: 10.1001/jama.2014.732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ogden CL, Flegal KM. Changes in terminology for childhood overweight and obesity. AGE. 2010;12(12) [PubMed] [Google Scholar]
- Oken E, Kleinman KP, Rich-Edwards J, Gillman MW. A nearly continuous measure of birth weight for gestational age using a United States national reference. BMC Pediatrics. 2003;3(6) doi: 10.1186/1471-2431-3-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patrick H, Nicklas TA, Hughes SO, Morales M. The benefits of authoritative feeding style: Caregiver feeding styles and children's food consumption patterns. Appetite. 2005;44(2):243–249. doi: 10.1016/j.appet.2002.07.001. [DOI] [PubMed] [Google Scholar]
- Piernas C, Popkin BM. Increased portion sizes from energy-dense foods affect total energy intake at eating occasions in US children and adolescents: patterns and trends by age group and sociodemographic characteristics, 1977–2006. The American Journal of Clinical Nutrition. 2011;94(5):1324–1332. doi: 10.3945/ajcn.110.008466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quattrin T, Roemmich JN, Paluch R, Yu J, Epstein LH, Ecker MA. Efficacy of family-based weight control program for preschool children in primary care. Pediatrics. 2012;130(4):660–666. doi: 10.1542/peds.2012-0701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rhee KE, Lumeng JC, Appugliese DP, Kaciroti N, Bradley RH. Parenting styles and overweight status in first grade. Pediatrics. 2006;117(6):2047–2054. doi: 10.1542/peds.2005-2259. [DOI] [PubMed] [Google Scholar]
- Salvy S-J, Vartanian LR, Coelho JS, Jarrin D, Pliner PP. The role of familiarity on modeling of eating and food consumption in children. Appetite. 2008;50(2):514–518. doi: 10.1016/j.appet.2007.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanek K, Abbott D, Cramer S. Diet quality and the eating environment of preschool children. Journal of the American Dietetic Association. 1990;90(11) [PubMed] [Google Scholar]
- Tanofsky-Kraff M, Goossens L, Eddy KT, Ringham R, Goldschmidt A, Yanovski SZ, Yanovski JA. A multisite investigation of binge eating behaviors in children and adolescents. Journal of Consulting and Clinical Psychology. 2007;75(6):901. doi: 10.1037/0022-006X.75.6.901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trent K, Spitze G. Growing up without Siblings and Adult Sociability Behaviors. Journal of Family Issues. 2011;32(9):1178–1204. doi: 10.1177/0192513X11398945. doi: 10.1177/0192513X11398945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vereecken CA, Keukelier E, Maes L. Influence of mother's educational level on food parenting practices and food habits of young children. Appetite. 2004;43(1):93–103. doi: 10.1016/j.appet.2004.04.002. [DOI] [PubMed] [Google Scholar]
- Wardle J, Guthrie CA, Sanderson S, Rapoport L. Development of the children's eating behaviour questionnaire. Journal of Child Psychology and Psychiatry. 2001;42(7):963–970. doi: 10.1111/1469-7610.00792. [DOI] [PubMed] [Google Scholar]
- Webber LC, Hill JS, Jaarsveld CHMV, Wardle J. Eating behaviour and weight in children. International Journal of Obesity. 2008;33(1):21–28. doi: 10.1038/ijo.2008.219. [DOI] [PMC free article] [PubMed] [Google Scholar]