

Abstract
Background
Alveolar bone grafting in unilateral cleft lip/palate (CLP) patients can improve nasal symmetry and facial esthetic. In some cases lateral piriform hypoplasia cannot be compensated by soft tissue thickness of the face, necessitating onlay bone grafting. This study was designed to estimate the proportion of patients among unilateral CLP patients requiring this procedure.
Materials and Methods
In a retrospective study, unilateral CLP patients with severe paranasal deficiency, who were managed by paranasal augmentation with cortico-cancellous bone graft during the alveolar cleft bone grafting, were included.
Results
From 85 unilateral CLP patients treated from 2005 to 2011 in the Oral and Maxillofacial Surgery Department, Mashhad University of Medical Sciences, fourteen patients were treated with lateral piriform augmentation technique. Mean age of the patients at the time of operation was 16 ± 4.8 years. Follow-up period was 2–6 years.
Conclusion
Concomitant alveolar bone grafting and lateral piriform augmentation is needed at least in 16.5 % of unilateral CLP patients.
Keywords: Alveolar bone grafting, Lateral piriform augmentation, Unilateral cleft lip and palate
Introduction
Alveolar bone grafting (ABG) is an important surgical step in the management of cleft lip/palate patients [1]. It has esthetic results apart from benefits obtained from closure of oronasal fistula in the alveolar cleft region [2, 3].
It provides a sound basis for further orthognathic surgery and rhinoplasty [4, 5]. Proper alveolar cleft bone grafting will reconstruct the nasal floor at the same level as unaffected side (in unilateral cases) and elevate nasal ala [6–8].
In unilateral cleft lip/palate patients, paranasal deformity on the side adjacent to the cleft margin is more pronounced in comparison to the unaffected side (Fig. 1). Correction of paranasal deformity can be made at the same time as the alveolar cleft bone grafting or during rhinoplasty. This study was designed to make an estimation of the percentage of patients among unilateral cleft lip/palate (CLP) patients needing paranasal onlay bone grafting concomitant with ABG.
Fig. 1.

The nasal ala and paranasal region depressed in the cleft side
Materials and Methods
In a retrospective study, unilateral CLP patients with severe paranasal deficiency, who were managed by paranasal augmentation with cortico-cancellous bone graft during the alveolar cleft bone grafting, were included. Bilateral CLP patients were excluded from the study. Post-operative panoramic views and at least 1-year of follow-up were considered to evaluate the possibility of root damage in maxillary canine adjacent to the cleft. Direct contact of the fixation appliance with canine root was considered a therapeutic error.
Surgical Technique
After closure of the oronasal fistula and alveolar cleft bone grafting, the periosteum overlying the piriform rim in the affected side was undermined. With placement of molded bone wax beneath the periosteum, the required bone for paranasal augmentation was estimated; then a block of cortico-cancellous bone graft harvested from the anterior iliac crest, was transferred to the paranasal region and fixed with a mini-screw by “lag screw” type technique (Fig. 2). Sharp edges were trimmed with a round surgical bur, followed by the soft tissue closure over the grafted bone by lateral sliding mucoperiosteal flap.
Fig. 2.

Fixation of onlay bone graft with miniscrew
Because of the added volume beneath the periosteum, wound closure was more difficult, necessitating more periosteal hatching; even in some cases distal soft tissue flap cut-back was required.
Results
Of 85 unilateral CLP patients treated from 2005 to 2011 in the Oral and Maxillofacial Surgery Department, Mashhad University of Medical Sciences, 14 patients were treated with lateral piriform augmentation technique. Demographic data of the patients are presented in Table 1. In two patients lip split approach was used for major lip repair, along with wide access for nasal floor reconstruction.In the others the intraoral incisions were used for this purpose.
Table 1.
Demographic information of fourteen unilateral alveolar cleft patients treated with lateral piriform augmentation technique concomitant with ABG
| Sex | Age at operation | Right or left | Follow up (years) | |
|---|---|---|---|---|
| 1 | M | 19 | Right | 6 |
| 2 | F | 17 | Left | 7 |
| 3 | M | 13 | Left | 6 |
| 4 | M | 19 | Left | 6 |
| 5 | F | 23 | Left | 5 |
| 6 | M | 9 | Left | 5 |
| 7 | M | 12 | Left | 5 |
| 8 | F | 22 | Left | 2 |
| 9 | F | 15 | Left | 5 |
| 10 | F | 16 | Left | 5 |
| 11 | M | 10 | Right | 5 |
| 12 | F | 13 | Left | 3 |
| 13 | F | 16 | Left | 2 |
| 14 | M | 25 | Right | 3 |
M male, F female
A total of 50 % of patients were females and 70 % of unilateral clefts were located on the left side. Post-operative radiographs showed no interference of the appliance used for internal fixation of paranasal bone block with tooth root except in one case (Fig. 3). There was a case of alveolar cleft bone graft failure while the onlay graft of the piriform rim survived (Fig. 4).
Fig. 3.
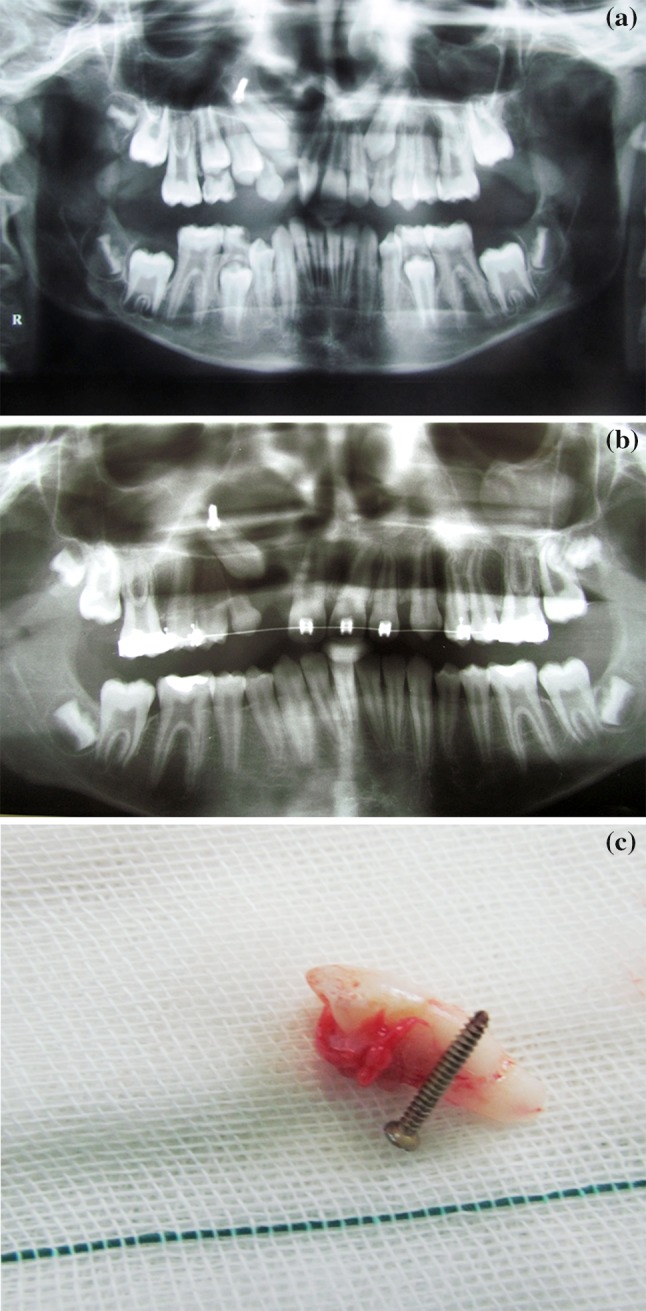
Interference with canine tooth eruption. a One month postoperation. b 2 years after surgery. Note that left canine is normally erupted while in the cleft side the permanent canine is retained. c Removed tooth and screw
Fig. 4.

Survived onlay grafted lateral piriform despite failed alveolar bone grafting
Mean age of the patients at the time of surgery was 16 ± 4.8 years. Follow-up period was 2–6 years. Donor site in all the patients was the anterior iliac crest.
In this study only 14 % of patients were under 10 years of age, which is an ideal age for ABG (Fig. 5). A complication involving a tooth root happened in a 10-year-old male patient.
Fig. 5.
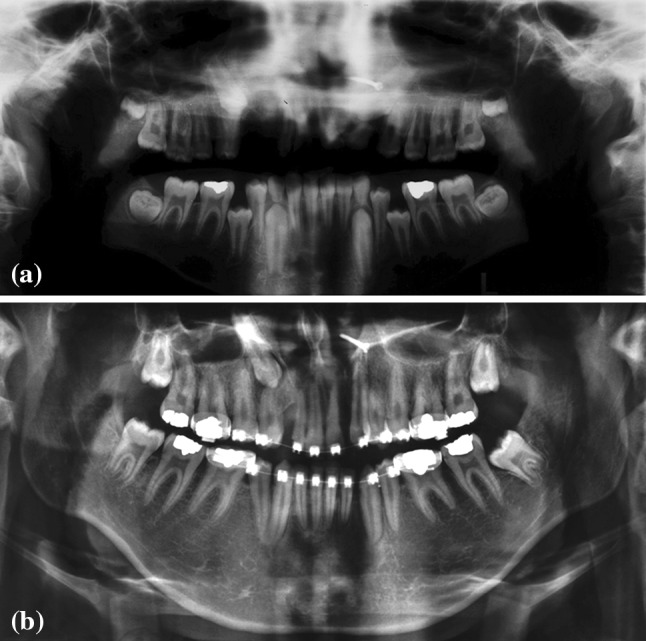
Lateral piriform augmentation in mixed dentition. a OPG 1 month after surgery. b Five year follow up graphy
Discussion
Alveolar cleft bone grafting has positive effects on facial esthetic [9]. In unilateral alveolar cleft patients, paranasal deficiency is more pronounced in comparison with bilateral alveolar cleft patients. The lateral piriform rim area needs special attention during bone grafting [10].
This procedure dramatically improves the esthetic results in unilateral alveolar cleft patients (Fig. 6) [11]. Not all the unilateral alveolar cleft patients need this operation; only 16.5 % of these patients in this study needed this operation. This is parallel with a study by Miyamoto, who showed that cleft side piriform margin depression does not necessarily lead to alar depression in all the cases [12].
Fig. 6.
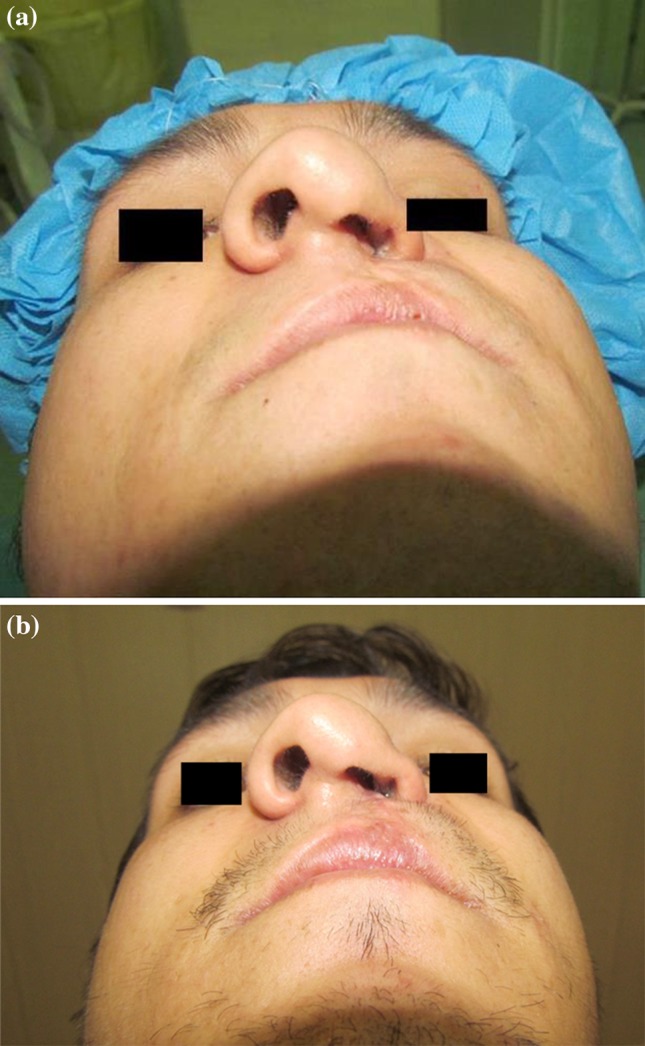
Improvement in facial esthetic after concomitant alveolar bone grafting and lateral piriform augmentation. a Pre-operative worms view of the patient. b 6 months after lateral piriform augmentation
Ordinarily alveolar cleft bone grafting will elevate the nasal floor and nasal ala but will not correct the paranasal deficiency. According to the study of Sander et al., mixed dentition alveolar bone grafting appears to have no significant long term effect on nasal morphology, symmetry or nasal shape so paranasal deficiency needs special attention during alveolar cleft bone grafting. Augmentation of the alar base with a bone block graft secured in place with titanium miniscrew can solve this problem [13, 14]. Concomitant ABG and lateral piriform augmentation was called “anterior maxillary bone grafting” by Li et al. [15].
Potential complications of paranasal augmentation in unilateral alveolar cleft patients include difficulty in wound closure and possibility of damage to the root of permanent unerupted maxillary canine.
The first situation can be managed by more periosteal hatching, distal cut-back and rounding of the bony edges of grafted bone with a surgical bur.
The second problem is not a concern in adult alveolar cleft patients but in early secondary bone grafting, which is the best time for alveolar cleft bone grafting, there is a real danger that can be prevented by careful selection of osteosynthesis site. Fortunately in this age group there is less need for this operation and only 14 % of the patients in this study were in this age group. If the estimated risk of the injury to the tooth germ is high, then monocortical fixation of the onlay graft and fixation with mini/micro-plate in more cephalic position, should be considered (Fig. 7). Experimental study in sheep has confirmed that graft fixation will decrease the risk of onlay bone graft movement and resorption [16]. One titanium screw is sufficient for this purpose [17].
Fig. 7.
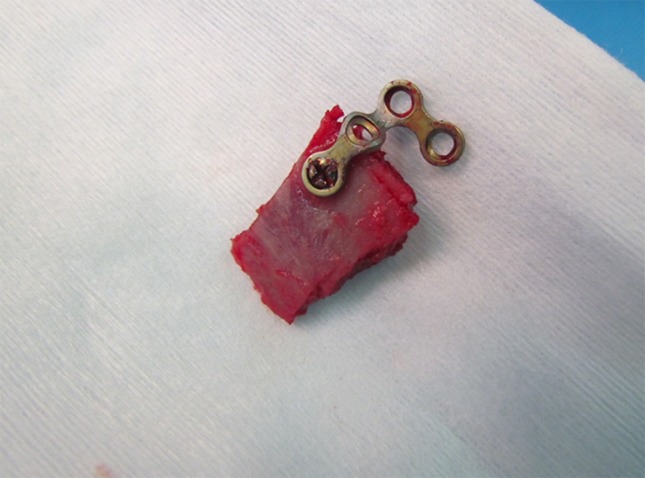
Suggested way for prevention of root damage in lateral piriform augmentation during mixed dentition is fixation of the onlay graft with mini/micro screw
This study showed that lateral piriform augmentation concomitant with alveolar cleft bone grafting is a much needed procedure in late alveolar cleft bone grafting. The need for ABG concomitant with lateral piriform augmentation should be carefully evaluated before ABG because it can influence the choice of donor site and achieve better results. Donor site in all the patients was the anterior iliac crest and no case of chin or tibia bone graft had been recorded as the donor site. This is attributed to the limited available volume of cortical bone in the chin and the fact that the tibia is a source of cancellous bone in ABG.
Conclusion
Concomitant alveolar bone grafting and lateral piriform augmentation is necessary in at least 16.5 % of unilateral CLP patients.
Acknowledgments
This study was supported by a Grant from the Vice Chancellor of Research of Mashhad University of Medical Sciences.
Conflict of interest
None declared.
Contributor Information
Amin Rahpeyma, Phone: +98(511)8829501, Email: rahpeymaa@mums.ac.ir.
Saeedeh Khajehahmadi, Phone: +98(511)8829501, Email: khajehahmadis@mums.ac.ir, Email: saeedeh.ahmady@yahoo.com.
References
- 1.Rahpeyma A, Khajehahmadi S. Modified VIP-CT flap in late maxillary alveolar cleft surgery. J Craniomaxillofac Surg. 2014;42:432–437. doi: 10.1016/j.jcms.2013.05.036. [DOI] [PubMed] [Google Scholar]
- 2.Nakamura N, Okawachi T, Nishihara K, Hirahara N, Nozoe E. Surgical technique for secondary correction of unilateral cleft lip-nose deformity: clinical and 3-dimensional observations of preoperative and postoperative nasal forms. J Oral Maxillofac Surg. 2010;68:2248–2257. doi: 10.1016/j.joms.2009.06.012. [DOI] [PubMed] [Google Scholar]
- 3.Kau CH, Medina L, English JD, Xia J, Gateno J, Teichgraber J. A comparison between landmark and surface shape measurements in a sample of cleft lip and palate patients after secondary alveolar bone grafting. Orthodontics (Chic.) 2011;12:188–195. [PMC free article] [PubMed] [Google Scholar]
- 4.Albert TW. Oral and maxillofacial surgery: considerations in cleft nasal deformities. Facial Plast Surg. 2000;16:79–84. doi: 10.1055/s-2000-7329. [DOI] [PubMed] [Google Scholar]
- 5.Cutting CB. Secondary cleft lip nasal reconstruction: state of the art. Cleft Palate Craniofac J. 2000;37:538–541. doi: 10.1597/1545-1569(2000)037<0538:SCLNRS>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Zhang L, Lu L, Li ZJ, Liu Q, Yang ML, Wang XK, et al. Anthropometric analysis of the maxillary bone and the alar base in unilateral cleft lip with secondary nasal deformity: classification of a piriform margin bony depression. Cleft Palate Craniofac J. 2014;51:23–29. doi: 10.1597/11-205. [DOI] [PubMed] [Google Scholar]
- 7.Wu Y, Yang Y, Chen Y, Zhang Y, Wang G. Measurement and evaluation of the alar base in unilateral secondary lip nasal deformities by three-dimensional computed tomography. Cleft Palate Craniofac J. 2013;50:696–703. doi: 10.1597/11-144.1. [DOI] [PubMed] [Google Scholar]
- 8.Daskalogiannakis J, Mercado A, Russell K, Hathaway R, Dugas G, Long RE, Jr, et al. The Americleft study: an inter-center study of treatment outcomes for patients with unilateral cleft lip and palate part 3. Analysis of craniofacial form. Cleft Palate Craniofac J. 2011;48:252–258. doi: 10.1597/09-185.1. [DOI] [PubMed] [Google Scholar]
- 9.Nagasao T, Ogata H, Miyamoto J, Jiang H, Kaneko T, Isshiki Y, et al. Alveolar bone grafting for patients with unilateral complete alveolar and palatal clefts improves the bony structure of the nose. Cleft Palate Craniofac J. 2009;46:9–18. doi: 10.1597/07-169.1. [DOI] [PubMed] [Google Scholar]
- 10.Kokkinos PP, Ledoux WR, Kinnebrew MC, Weinberg R. Iliac apophyseal cartilage augmentation of the deficient piriform rim and maxilla in alveolar cleft grafting. Am J Orthod Dentofacial Orthop. 1997;112:145–153. doi: 10.1016/S0889-5406(97)70239-7. [DOI] [PubMed] [Google Scholar]
- 11.Baykul T, Aydin A, Nasir S, Türkkahraman H. Surgical rehabilitation of nasoalveolar complex in patients with alveolar clefts. J Craniofac Surg. 2010;21:1512–1515. doi: 10.1097/SCS.0b013e3181ebe646. [DOI] [PubMed] [Google Scholar]
- 12.Miyamoto J, Nagasao T, Nakajima T, Ogata H. Evaluation of cleft lip bony depression of piriform margin and nasal deformity with cone beam computed tomography: “retruded-like” appearance and anteroposterior position of the alar base. Plast Reconstr Surg. 2007;120:1612–1620. doi: 10.1097/01.prs.0000267421.69284.c7. [DOI] [PubMed] [Google Scholar]
- 13.Sander M, Daskalogiannakis J, Tompson B, Forrest C. Effect of alveolar bone grafting on nasal morphology, symmetry, and nostril shape of patients with unilateral cleft lip and palate. Cleft Palate Craniofac J. 2011;48:20–27. doi: 10.1597/09-007. [DOI] [PubMed] [Google Scholar]
- 14.Devlin MF, Ray A, Raine P, Bowman A, Ayoub AF. Facial symmetry in unilateral cleft lip and palate following alar base augmentation with bone graft: a three-dimensional assessment. Cleft Palate Craniofac J. 2007;44:391–395. doi: 10.1597/06-179.1. [DOI] [PubMed] [Google Scholar]
- 15.Li J, Shi B, Liu K, Zheng Q, Wang Y, Li S. A photogrammetric study of the effects of alveolar bone graft on nose symmetry among unilateral cleft patients. J Plast Reconstr Aesthet Surg. 2011;64:1436–1443. doi: 10.1016/j.bjps.2011.06.022. [DOI] [PubMed] [Google Scholar]
- 16.Phillips JH, Rahn BA. Fixation effects on membranous and endochondral onlay bone-graft resorption. Plast Reconstr Surg. 1988;82:872–877. doi: 10.1097/00006534-198811000-00023. [DOI] [PubMed] [Google Scholar]
- 17.Burger EA, Meshkini H, Lindeboom JA. One versus two titanium screw fixation of autologous onlay bone grafts in the anterior maxilla: a randomised histological pilot study. Eur J Oral Implantol. 2011;4:219–225. [PubMed] [Google Scholar]