

Abstract
The current research provides a framework for understanding how concealable stigmatized identities impact people's psychological well-being and health. The authors hypothesize that increased anticipated stigma, greater centrality of the stigmatized identity to the self, increased salience of the identity, and possession of a stigma that is more strongly culturally devalued all predict heightened psychological distress. In Study 1, the hypotheses were supported with a sample of 300 participants who possessed 13 different concealable stigmatized identities. Analyses comparing people with an associative stigma to those with a personal stigma showed that people with an associative stigma report less distress and that this difference is fully mediated by decreased anticipated stigma, centrality, and salience. Study 2 sought to replicate the findings of Study 1 with a sample of 235 participants possessing concealable stigmatized identities and to extend the model to predicting health outcomes. Structural equation modeling showed that anticipated stigma and cultural stigma were directly related to self-reported health outcomes. Discussion centers on understanding the implications of intraindividual processes (anticipated stigma, identity centrality, and identity salience) and an external process (cultural devaluation of stigmatized identities) for mental and physical health among people living with a concealable stigmatized identity.
Keywords: stigma, psychological distress, courtesy stigma, mental illness, identity
Recent reviews in psychology and sociology and from the Department of Health and Human Services have concluded that stigma has large and varied effects on people's life outcomes (e.g., Major & O'Brien, 2005; U.S. Department of Health and Human Services [DHHS], 1999; Williams, Neighbors, & Jackson, 2003). The goal of the current research is to propose and test a novel model for understanding how stigma impacts psychological and health well-being among people who live with a concealable stigmatized identity. Concealable stigmatized identities are vastly understudied in comparison to visible stigmatized identities. Despite the acknowledgment that stigma can have a variety of negative effects, there is currently no conceptual framework to understand how possessing a concealable stigmatized identity impacts psychological and physical distress. We seek to fill that gap.
Because stigma is socially constructed, we believe it is critical to examine both intraindividual and external stigma processes that can impact well-being. Whereas most psychological research has focused solely on the psychological processes internal to individuals that enable stigmatization to lead to psychological distress, here we focus on the impact of both intraindividual processes (i.e., anticipated stigma, centrality, and salience) and an external process (i.e., cultural stigma). In doing so, we adopt a broader approach to studying the impact of stigmatization than what has previously been attempted.
We propose that for people living with a concealable stigmatized identity, both psychological distress (as measured by levels of depression and anxiety) and health (as measured by self-report of illness symptoms) can be predicted by examining four important stigma-related components. First, at the intraindividual level, how much devaluation and prejudice does a person expect to occur if the identity is revealed? We predict that greater anticipated stigma will be related to increased distress. Next, how central is the concealable stigmatized identity to the self? Identities can be more or less self-definitional, and for concealable stigmatized identities we predict that greater centrality will be related to more distress. Last, how salient is the concealable stigmatized identity? Some people may rarely think about the identity, whereas others may think about it several times a day. We predict that increased salience will be related to increased distress. Finally, at the external, or cultural, level, different types of identities are culturally devalued to different degrees. We predict that possessing an identity with greater cultural stigma attached to it will be related to more psychological distress. Note that level of cultural stigma is determined by the community or culture in which a person is living, not by the individual him- or herself.
By simultaneously examining the relationships between these four constructs—anticipated stigma, centrality, salience, and cultural stigma—and psychological distress (in Study 1) and both psychological distress and health outcomes (in Study 2), we present a model that has both theoretical and practical implications. Although each of the four constructs has, individually, been theorized to affect people living with stigmatized identities, this research marks the first time they have been examined simultaneously, thereby allowing a fuller theoretical picture of how stigma operates in people's lives. More practically, this knowledge may help elucidate the pathways through which stigma can lead to health disparities (Muehrer, 2002), thereby leading to better interventions to reduce the negative impact of stigma.
Concealable Stigmatized Identities
A concealable stigmatized identity1 is an identity that can be kept hidden from others but that carries with it social devaluation (Crocker, Major, & Steele, 1998). Specifically, an identity is stigmatized if it is considered a mark of failure or shame, tainting the self in the eyes of others (Goffman, 1963). The term covers a broad range of identities, including history of mental illness, rape, molestation, epilepsy, domestic violence, previous incarceration, HIV/AIDS, and substance abuse (see Pachankis, 2007, for a review). Although these attributes differ considerably in their etiology, course, and treatment, there are important similarities among all of these concealable stigmatized identities. Each is socially devalued and may render an individual vulnerable to prejudice and discrimination solely on the basis of this attribute (e.g., loss of status, employment discrimination, personal rejection). These identities also have negative stereotypes associated with them (e.g., mental illness's association with danger and instability; rape's association with promiscuity and moral impurity).
Associative Stigma
An additional distinction concerning concealable stigmatized identities is whether the identity is personal versus associative. A personal concealable stigma is an identity that the self possesses, such as one's own history of mental illness. In contrast, an associative stigma (also known as a courtesy stigma or affiliate stigma) is a stigma that a person possesses because of his or her close connection to a stigmatized other (Birenbaum, 1970; Goffman, 1963). Research has shown that parents of disabled children; spouses, siblings, and children of the mentally ill; and caregivers of people living with AIDS all report feeling stigmatized, including feelings of shame, the need to keep the identity concealed, and the belief that others avoid (or may avoid) them due to their associative stigma (Corrigan & Miller, 2004; Mickelson, 2001; Wight, Aneshensel, Murphy, Miller-Martinez, & Beals, 2006). In the current research we examined whether our model applies to both personal and associative concealable stigmatized identities.
Stigma and Psychological Distress
Stigma scholars have long linked stigmatized identities to increased psychological distress. Although early theorizing assumed uniformly negative outcomes for people in stigmatized groups (e.g., Allport, 1954; Erickson, 1956), current stigma research has recognized that there is immense variability in how people cope with and respond to stigmatized identities (see Major, 2006, for a review of this new perspective on stigma). Thus, for example, among visibly stigmatized racial minorities, African Americans routinely report higher self-esteem than do European Americans (Gray-Little & Hafdahl, 2000), but Hispanics, Asian Americans, and Native Americans report lower self-esteem than do European Americans (Twenge & Crocker, 2002). Research on the relationship between concealable stigmatized identities and psychological distress has been somewhat more consistent, with rape, childhood sexual abuse, and mental illness related to increased psychological distress (e.g., Brewin, Andrews, & Valentine, 2000; Link, Struening, Neese-Todd, Asmussen, & Phelan, 2001). However, even these relationships have been critiqued and questioned (Corrigan & Watson, 2002; Rind, Tromovitch, & Bauserman, 1998). The enormous variability of psychological distress within stigmatized groups has led stigma researchers across domains to assert that simply examining the link between a social identity and psychological distress is no longer useful in trying to explain who is vulnerable to distress (Friedman & Brownell, 1995; Twenge & Crocker, 2002). Instead, it is crucial to understand how the psychological meaning of the identity works in tandem with stigma to make a person more or less vulnerable to distress.
Although stigma can affect many different types of life outcomes (e.g., employment, housing, educational achievement), psychologists have primarily focused on psychological outcomes such as self-esteem, life satisfaction, happiness, depression, and anxiety. Because these measures tend to be highly correlated, they are often made into composites of “psychological well-being” or “psychological distress.” In the current research we focused on depression and anxiety as a composite measure of psychological distress. We chose these measures because they are often used in stigma research (see Mak, Poon, Pun, & Cheung, 2007, for a review), thereby making our work comparable with other research in the area. We also chose them because level of psychological distress is an important and powerful variable. Depression and anxiety are often comorbid with a variety of health conditions (e.g., cardiovascular disease, diabetes) and are related to exacerbation of medical symptoms and decreased healthy behaviors (Katon & Ciechanowski, 2002). Thus, in choosing psychological distress as our outcome variable, we were guided both by its overall importance to psychological and physical well-being and by its theorized link to stigma.
Current Concepts and Models
Direct Effects of Stigma-Related Factors
Drawing on research conducted across a variety of different concealable stigmatized identities (e.g., mental illness, HIV/AIDS, childhood sexual abuse), we first define each of our four stigma identity–related factors—anticipated stigma, centrality, salience, and cultural stigma—and outline our predictions for how each of these separate factors can directly impact psychological distress when considered alone. In the sections that follow, we present a more complex framework that (a) examines how these factors can influence psychological distress when considered simultaneously and (b) accounts for both the direct and indirect (i.e., mediated) effects of these variables (see Figure 1). Finally, we extend this framework to consider how these factors influence both psychological distress and health (see Figure 2).
Figure 1.

Theorized mediated model predicting psychological distress.
Figure 2.

Theorized mediated model predicting psychological distress and health.
Anticipated Stigma
What do people think will happen if others learn of their concealable stigmatized identity? The concern that others will look down upon, shun, or discriminate against them is at the heart of anticipated stigma. Anticipated stigma refers to the degree to which individuals expect that others will stigmatize them if they know about the concealable stigmatized identity. Unlike people with visible stigmatized identities, who regularly interact with others who know of their stigmatized identity, people with concealable stigmatized identities may not know exactly how others will react if they reveal the identity. They do know, however, the negative stereotypes about their group. As Link and colleagues (Link, 1987; Link, Cullen, Struening, & Shrout, 1989) have discussed in regard to mental illness stigma, people often learn negative stereotypes before they acquire a stigmatized identity, and it is difficult to unlearn those stereotypes once one gains the identity. Thus, people with concealable stigmatized identities know the negative stereotypes about their groups and may even recall times when they themselves have discriminated against people with their identity. Moreover, because their identity is hidden, people with concealable stigmatized identities may often be in the position to directly witness disparagement of their stigmatized group (Wahl, 1999). It is not surprising, therefore, that people with concealable stigmatized identities are concerned about what will happen if they reveal their identity.
Previous research on anticipated stigma— often termed felt or perceived stigma— has consistently shown that the more people believe that others devalue their group, the worse their reported psychological well-being. This effect has been shown with several concealable stigmatized identities, including mental illness (e.g., Link, 1987; Link et al., 1989, Link & Phelan, 2001; Rosenfield, 1997), epilepsy (Westbrook, Bauman, & Shinnar, 1992), and HIV status (Katz & Nevid, 2005). Notably, for mental illness, the effect of perceived stigma on psychological distress occurs over and above any positive effects of mental illness treatment and continues long after the initial labeling of a mental illness disorder (Link, Struening, Rahav, Phelan, & Nuttbrock, 1997; Markowitz, 1998).
Measures of anticipated stigma in the literature, however, have often conflated several different types of beliefs (e.g., internalized shame, one's own beliefs about stereotypes, social rejection, and beliefs about others' possible attitudes and actions) into one measure termed perceived stigma. For example, Link's (1987) perceived Devaluation–Discrimination scale includes items such as “Most people believe that a man who has been hospitalized for a mental illness is dangerous” (Link, 1987; Link et al., 1997). Such items measure knowledge of stereotypes, but they do not directly measure whether the person with mental illness (or other concealed stigmatized identity) believes that others will devalue them if they reveal their concealed identity. It is this personal sense of anticipated stigma that we examined in the current research. Our measure of anticipated stigma explicitly asked people how likely they believed a variety of negative outcomes would occur if they revealed their stigmatized identities, making it a more direct and theoretically clear measure of anticipated stigma. We predicted that the more people anticipated negative consequences if they revealed their concealed stigmatized identities, the more distress they would report.
Centrality
A second factor that may allow a concealable stigmatized identity to impact psychological and health well-being is how central the identity is to the self. Just as people vary in the extent to which they anticipate stigmatizing reactions to their identity, they vary in whether the identity is considered to be critical to their self-definition. Although some previous research has examined the role of centrality of concealable stigmatized identities, it has focused predominantly on centrality's effects on disclosure decisions among people who are concealing sexual minority status (Griffith & Hebl, 2002; Ragins, 2008). To our knowledge, all other previous research on the role of centrality in psychological distress has focused on visible identities (primarily race). In both cross-sectional and longitudinal studies, greater centrality of ethnic identity has been related to lower levels of psychological distress among African Americans (e.g., Sellers, Caldwell, Schmeelk-Cone, & Zimmerman, 2003; Sellers, Smith, Shelton, Rowley, & Chavous, 1998; Yip, Seaton, & Sellers, 2006). On the contrary, work examining other stigmatized identities, including women and Latinos, as well as some additional work done with African Americans, has shown either a negative or null relationship between centrality—also called identity importance or group identification—and psychological well-being (e.g., Eccleston & Major, 2006; Major, Quinton, & Schmader, 2003; McCoy & Major, 2003).
In the current research we predicted that greater centrality of the identity would be related to increased psychological distress. While previous research has suggested that identities that are more central to the self may have benefits for psychological well-being because they offer people a source of social support and can provide external attributions for negative events (e.g., Bourguignon, Seron, Yzerbyt, & Herman, 2006; Crocker & Major, 1989; Cross, 1991), we predicted that this is not the case for those whose identity is concealable. Given that people with concealable stigmatized identities are less likely to spend time with similar others (Frable, Platt, & Hoey, 1998), the buffering effects of identity centrality on psychological well-being are not often open to those with concealable stigmatized identities. Thus, we hypothesized that higher levels of identity centrality would predict higher rates of psychological distress among people with concealable stigmatized identities.2
Salience
Stigmatized identities also vary in the extent to which they are salient to the holders of the identities. For some people, the identity will cross their minds only once a year, and few situations will make the identity salient (Quinn, Kahng, & Crocker, 2004). For others, the identity may be chronically accessible and occupy their thoughts quite often. To the extent that people are frequently thinking about the concealed identity, the stigma is a more important and salient part of their lives. Thus, our measure of salience is a straightforward frequency measure asking how often people think about their concealable stigmatized identity. We did not ask what people were thinking about or how they were feeling when they were thinking about the identity. We were interested in sheer salience of the identity to the self. We predicted greater salience would be related to increased psychological distress.
There are no current measures of stigma salience for concealed identities, but there has been research on two related concepts. Both stigma consciousness (Pinel, 1999) and race-based rejection sensitivity (Mendoza-Denton, Downey, Purdie, Davis, & Pietrzak, 2002) highlight individual differences in people's thoughts and expectations about whether situations are related to their stigmatized identity. However, both of these measures capture constructs substantially different from mere salience of the identity. Stigma consciousness measures the extent to which people believe their group membership is being used to judge or evaluate them (e.g., women wondering if men interpret their actions in a gendered way because they are women). The race-based rejection sensitivity measure is designed to examine whether people in specific situations in which their identity is known to others expect and are concerned about stereotype-related treatment (e.g., African Americans wondering if store clerks think they will shoplift). This measure is more akin to our anticipated stigma measure but is dependent on assessing stereotype-relevant situations for visible identities. Neither of these measures are frequency measures per se, and both would be difficult to adapt for identities that remain concealed in most situations. A comparison of these measures directly highlights the differences in the day-to-day experiences of concealable versus visible stigmatized identities. As noted by Goffman (1963), people with visible stigmas are managing situations, whereas people with concealed stigmas are managing information about the self.
Cultural Stigma
Different stigmatized identities carry with them different levels of social devaluation. This level of devaluation is culturally constructed, in that it originates outside the self and is not connected to any idiosyncratic characteristics beyond the stigma label. Unlike the intraindividual identity–related variables discussed thus far— anticipated stigma, centrality, and salience—level of cultural stigma is determined externally from the person possessing the identity. Although social scientists have emphasized that stigma is constructed through social relationships, cultures, and institutions (Hebl & Dovidio, 2005; Link & Phelan, 2001), level of cultural stigma has rarely been examined as a predictor of psychological distress.
In the current research we take a novel approach to capture levels of cultural stigma. To obtain a truly external measure of cultural stigma, we asked a separate sample of participants—a sample that could be considered the cultural peers of our main sample of people with concealable stigmatized identities—to rate how negatively people with each of the concealable stigmatized identities are viewed. We then used these ratings of cultural stigma as a predictor of psychological distress. This process of using external aggregate ratings is similar to work done by Cutrona and colleagues (Cutrona et al., 2005; Cutrona, Wallace, & Wesner, 2006), in which aggregate ratings of neighborhood distress and census ratings of neighborhood poverty were used along with intraindividual-level risk factors (e.g., personality, socioeconomic status) to predict psychiatric disorders. We hypothesized that level of cultural stigma would affect psychological distress such that those with more socially stigmatized identities would report more distress, over and above the distress related to the internal factors of anticipated stigma, centrality, and salience. This is an important step to take stigma out of the individual and place it back into the larger culture, where it originated.
Summary
In the current work, we examine the direct and independent effect of each of our stigma-related variables on psychological distress for people with concealable stigmatized identities. There are varying levels of empirical and theoretical support for each of the intraindividual variables (anticipated stigma, centrality, and salience), but they have never been tested simultaneously. To our knowledge, utilizing an external measure of cultural stigma has not previously been examined. Also, because previous research has primarily focused on visible identities, several of the variables were modified (anticipated stigma, centrality) or specifically developed (salience, cultural stigma) for concealable stigmatized identities. The test of the direct effects model allows both a theoretical and practical advancement in the understanding of the experiences of people who live with concealable stigmatized identities.
Mediated Models Predicting Psychological Distress and Health Outcomes
We believe that in order to fully understand the negative effects of stigma, it is important to consider both the direct and indirect processes through which stigma results in deleterious psychological and health outcomes. That is, although it is important to understand the relative impact of each factor independently, these factors coexist within individuals and are likely to influence each other. Below we outline our framework for considering both the direct and indirect effects of these factors on psychological distress (see Figure 1) and both psychological distress and illness symptoms (see Figure 2).
Mediated Model Predicting Psychological Distress
In order to understand this complex process, we first started with the assumption that people who live with a concealable stigmatized identity contend with two basic types of stigma: anticipated stigma, which is an intraindividual process, and cultural stigma, which is an external process. Anticipated stigma has been consistently linked to deleterious psychological effects (see Mak et al., 2007, for a review), but the reasons why this occurs are not fully known. In the mediated model that we tested in the current work, we examined how anticipated stigma can affect well-being indirectly through both centrality and salience.
In Study 1, we predicted that greater levels of anticipated stigma would be related to greater centrality of the identity. Although there has been no research on this relationship for people with concealable stigmatized identities, there has been an ongoing debate on a similar topic within research on racial identity. Specifically, there are opposing viewpoints on whether greater centrality of racial identity leads to more perceived stigma and, ultimately, more distress or whether more perceived and experienced stigma leads to greater centrality (e.g., Branscombe, Schmitt, & Harvey, 1999; McCoy & Major, 2003). For concealable stigmatized identities, we hypothesized that because most people have little day to-day experience with discrimination because their identity is concealed, it makes more theoretical sense that it is their own anticipation of devaluation and rejection that will increase the importance of the identity for the self. That is, to the extent that people believe they will be rejected by others, the identity becomes more important in defining the self. In a similar vein, we hypothesized that greater anticipated stigma would be related to increased salience of the identity. Again, to the extent that people believe that greater rejection and devaluation will occur if others know about the identity, the identity will be on their minds more frequently. In summary, people who anticipate more stigma may also, in turn, find the identity to be of greater magnitude for the self—it will be more central and salient and may, therefore, lead to compromised well-being.
We predicted that cultural stigma would directly affect psychological distress. We expected that cultural stigma would impact well-being due to the myriad subtle changes and slights that occur because one possesses a devalued identity. These faint—and for people with concealable stigmatized identities, fairly infrequent— degradations in treatment or relationships are hard for an individual to identify and do not necessarily consciously filter through individuals' psyches (see Link & Phelan, 2001, for a discussion of how stigma changes life outcomes). Thus, we predicted that levels of cultural stigma would have only direct effects on well-being, without working indirectly through centrality and salience.
Mediated Model Predicting Health
In Study 2, we extended the model tested in Study 1 to examine both psychological distress and health outcomes (see Figure 2). Members of stigmatized groups tend to have more negative health outcomes across a variety of indicators when compared with members of nonstigmatized groups (DHHS, 1999). Within research on racial stigma, there has been a consistent link between perceptions of discrimination and negative health outcomes, as well as reported experiences of discrimination and negative health outcomes (Williams, Neighbors, & Jackson, 2003). We predicted, on the basis of these findings, direct effects for both anticipated and cultural stigma on increased illness symptoms within our sample. That is, to the extent that people were worried about social rejection and discrimination (anticipated stigma) and were, indeed, devalued due to their identity (cultural stigma), they would report more illness symptomatology. In addition, increased psychological distress has been consistently and strongly comorbid with negative health indicators (Katon & Ciechanowski, 2002). Thus, in our current model we expected that psychological distress would be strongly related to increased illness symptomatology.
In summary, in Study 2 we tested a model predicting both psychological and health outcomes simultaneously. We expected that, in line with predictions from Study 1, anticipated stigma would be both directly related to psychological distress and indirectly related to it through its effect on centrality and salience. In addition, we predicted that both anticipated stigma and cultural stigma would be directly related to self-reported health outcomes. Finally, we predicted that in line with a large and consistent literature, psychological distress would be strongly related to more negative health outcomes.
Study 1
In Study 1, we measured the intraindividual constructs of anticipated stigma, centrality of the concealed identity to the self, and salience of the identity to self in a sample of 300 people living with concealable stigmatized identities. We also measured psychological distress, as indexed by depression and anxiety. In order to create an external measure of cultural stigma, we collected data from a second sample in which we had participants—who were not selected for having a concealable stigmatized identity—rate the level of devaluation associated with each of the identities reported in the first sample.
In our analyses, we first examine the independent, direct effects of each variable on psychological distress. Then, we consider both the direct and indirect effects of these variables on psychological distress within the model presented in Figure 1. Additionally, we provide tests of potential alternate models. Finally, we examine whether the model applied equally well to people with associative versus personal concealable stigmatized identities. Previous research has shown that although people with associative stigma reported feeling stigmatized, the level of distress was not as high as for people with a personal concealable stigmatized identity. In the current research we examine (a) whether there are differences in the reported distress level and (b) whether those differences are mediated by the lower levels of anticipated stigma, centrality, and salience that people with an associative stigma (compared with personal stigma) are likely to possess.
Method
Participants
People concealing a stigmatized identity are difficult to identify. In order to find participants potentially concealing a stigmatized identity, we included two questions in a mass prescreening session held during the 1st week of the semester during introductory psychology classes at the University of Connecticut. Participants were first asked if they possessed an identity that they regularly kept hidden from others. If they answered yes, they were further queried on whether they believed that if they revealed the identity to others, the reaction would be “mostly negative,” “mostly surprised,” or “mostly positive.” Over the course of two semesters, we screened a total of 2,057 students with these questions. Of these, 746 (36%), noted that they were concealing an identity that they believed others would react to negatively or with surprise. We deliberately used these broad criteria in order to obtain a variety of concealed identities. These 746 students were eligible to sign up for our study as one of many listed in our web-based participant pool system. There was no particular incentive for them to sign up for our study versus any other study occurring in the participant pool.
A total of 377 participants signed up and completed the survey. Of these, 300 participants indicated a codable stigmatized identity and were included in analyses. More information about the identities is given below. Participants completed the survey as partial fulfillment of a course requirement. Participants were predominantly female (73.3%) and Caucasian (85.4%), and the mean age was 18.59 years (SD = 1.08).
Procedure
The first page of the survey gave a neutral explanation of a concealed identity (“Almost all people have parts of their history or personal identity that they regularly keep concealed from other people. In the questions that follow, we are interested in learning more about the experience of both concealing and revealing ‘hidden’ experiences or identities”), followed by examples of positive, negative, and neutral identities.3 We reminded them that they were selected because they had indicated in the prescreening that they had something about themselves that they regularly kept hidden. The participants were then asked to describe their concealed identity in their own words and were told that this identity would be referred to as their “concealed identity” in the survey. They were also told that if they had multiple concealed identities, they should choose only one on which to report.
Participants then completed a battery of measures related to both concealed identity and psychological distress (described below). Two presentation orders of these materials were created such that half of the participants completed the questions about the concealed identity first followed by the psychological distress measures, and the other half completed the measures in the reverse order. All participants were assured of their anonymity, and each participant completed the survey alone in a small cubicle.
Measures
Nature of the concealed identity
Two raters coded the open-ended responses describing the concealed identity into one of the following categories: (a) mental illness (e.g., depression, obsessive compulsive disorder), (b) weight/appearance concerns (e.g., eating disorder), (c) sexually related activity (e.g., fetishes, affairs), (d) medical conditions (e.g., diabetes, epilepsy), (e) history of rape, (f) history of childhood sexual abuse, (i) sexual orientation, (j) family member with medical or psychological issues (e.g., cancer, mental illness), (k) family member with addiction (e.g., alcoholism, gambling), (l) abusive family (e.g., domestic violence), (m) drug use, (n) criminal actions (e.g., stealing), (o) abortion, (p) lies about background or personal information, (q) death of a family member, (r) adoption, and (s) uncodable (e.g., question was not answered or did not include enough information for the coders to categorize it). Interrater reliability was high (κ = .93), and discrepancies were resolved through discussion. Because the last four categories above— concerning lying (n = 10), family member death (n = 19), adoption (n = 4), and being uncodable (n = 44)—were not clearly stigmatized identities (i.e., they do not taint the whole person in the eyes of others or carry with them consensual negative stereotypes), we did not include these participants' data in the analyses.
Anticipated stigma
To measure the extent to which people thought they would be socially stigmatized if they revealed their identity, we presented a 15-item scale with the following directions: “If others knew your concealed identity, how likely do you think the following would be to occur?” Answers were rated on a 1 (not at all likely) to 7 (very likely) Likert scale. The scale contained the nine-item “day-to-day” discrimination scale from Kessler, Mickelson, and Williams (1999, p. 214), with items such as “Getting poorer service than others do at restaurants or stores” and “People threatening or harassing you,” as well as six additional items we thought would be likely to capture the type of social devaluation about which college students would be concerned: “People not wanting to date you,” “Current friends stop hanging out with you,” “Friends avoiding you,” “Roommates wanting to move out of apartment or dorm room,” “People not wanting to get to know you better,” and “People not wanting to get involved in an intimate relationship with you” (α = .95).
Identity centrality
We used the Importance to Identity sub-scale of the Collective Self-Esteem scale (Luhtanen & Crocker, 1992) to examine the centrality of the concealed identities to self. This four-item scale has been widely used across different types of identities (Luhtanen & Crocker, 1992; Sellers et al., 1998) and was modified to pertain to concealed identity (e.g., “My concealed identity is an important reflection of who I am”). Each item was answered on a 7-point response scale that ranged from 1 (strongly disagree) to 7 (strongly agree). Questions were coded so that higher scores reflected greater centrality (α = .76).
Identity salience
A one-item measure asked participants to indicate the extent to which they generally think about their concealed identity. Response options were almost never, several times a year, once a month, once a week, a few times a week, once a day, and many times each day. Participants checked the frequency level that best described their situation. We then converted this categorical measure into a continuous measure representing number of thoughts per day. Specifically, “almost never” = 0 times per day; “several times a year” = 3/365; “once a month” = 12/365; “once a week” = 52/365; “a few times a week” = (4 × 52)/365; “once a day” = 1; “many times a day” = 5.
Psychological distress
In line with previous work on stigma and psychological distress, we defined distress as a combination of depression and anxiety (e.g., Kessler et al., 1999; Major & Gramzow, 1999; Sellers et al., 2003). Items from the State–Trait Anxiety Inventory–Trait (STAI-T) scale and the Center for Epidemiological Studies–Depression scale (CES-D) were standardized and combined to create a composite measure of psychological distress. The CES-D is a 20-item self-report measure of depressive symptomatology (Radloff, 1977). It is one of the most used and validated measures of depression (Shafer, 2006). Participants indicated the extent to which they felt each symptom during the past week on a 4-point scale ranging from 0 (Rarely or none of the time) to 3 (Most or all of the time). Scale reliability for this sample was high (α = .91). The STAI-T is a 20-item self-report measure of trait levels of anxiety that has also been widely used and validated (Spielberger, Vagg, Barker, Donham, & Westberry, 1980). Each item was rated on a 1 (not at all) to 5 (very much) scale, and scale reliability for this sample was high (α= .92). The two scales were correlated at r = .79, and the reliability of the composite measure was α = .95.
Cultural stigma
In order to collect an external measure of cultural stigma, we had a separate group of 114 participants complete a survey about their beliefs and views of different stigmatized groups. Participants were predominantly female (72.8%), Caucasian (79.8%), and 19.4 years of age (SD = 1.9). Undergraduate students were recruited from several large classes at the University of Connecticut to complete the survey. Thus, this sample constituted a sample of peers for the concealed identity sample.
We collected ratings from this separate group of participants in order to determine the relative level of devaluation of each type of concealable stigmatized identity in our main sample. Participants were first asked to think about a particular group (e.g., “People who have a history of mental illness,” “People who have had an abortion,” “People who have been raped”). Then they were asked to respond to the question “How do you think people with this identity are generally viewed by others?” on a 1 (very positive) to 7 (very negative) scale in reference to each of the 13 concealed identities in the main sample plus 1 visible identity (African American ethnicity) for comparison. Note that the rating always focused on the people rather than an event or experience.
All participants rated all of the identities, and presentation of the identities was randomized across participants. We specifically phrased this question to downplay socially desirable responding and to capture consensual ratings of stigma. Participants in this study could be considered “raters” or “judges” of identity negativity (i.e., we had 114 judges of 13 different targets). We computed an intraclass correlation (ICC) to examine rater reliability (Shrout & Fleiss, 1979) and found the ratings reliable (ICC = .99). We used the mean rating of each identity as our measure of cultural stigma. Notably, all of the concealed identities were judged to be as negative or more negative than possessing an African American racial identity, and all were above the midpoint of the scale, with means ranging between 4.10 (for people with a hidden medical condition) to 6.40 (for people with a history of criminal activity).
Additional measures
The survey contained, in addition to the main variables of interest, several additional measures. We adapted the Ruminative Responses Scale (Treynor, Gonzalez, & Nolen-Hoeksema, 2003) to ask participants how often they tended to ruminate about their concealed identity (10 items; α = .89). Rumination is a maladaptive coping strategy whereby people have a tendency to focus on their own negative thoughts and feelings, resulting in increased depression (Nolen-Hoeksema, 1991; Nolen-Hoeksema & Morrow, 1991). In the current study, we examined whether our measures of anticipated stigma, centrality, and salience predicted depression, controlling for the tendency to ruminate on the self. Participants were also asked to indicate the length of time they had possessed their concealed identity, which ranged from less than a year (5.6%) to their entire lifetime (11.8%), with a mean of approximately 5 years. Finally, we also asked a variety of questions, primarily open-ended, around beliefs about disclosure, which are not discussed here.
Results
We examined whether the order of questionnaires affected the variables by conducting independent t tests on each of the variables of interest (centrality, salience, anticipated stigma, and distress). There were no significant effects of order (all ps > .10).
Categories and Descriptives
As can be seen in the first column of Table 1, the most frequent concealed identity within the sample was mental illness, followed by appearance concerns.
Table 1. Concealed Stigmatized Identities by Type and Number of Participants.
| Identity type | Study 1 | Study 2 |
|---|---|---|
| Mental illness | 81 | 61 |
| Weight/appearance issues | 36 | 62 |
| Family members with medical or psychological issues | 29 | 9 |
| Sexually related activity | 26 | 13 |
| Medical condition | 25 | 6 |
| Abusive family | 24 | 13 |
| Family members with addictions | 20 | 12 |
| Rape | 15 | 16 |
| Sexual orientation | 14 | 18 |
| Childhood sexual abuse | 12 | 5 |
| Previous drug use | 9 | 13 |
| Criminal actions | 5 | 3 |
| Abortion | 4 | 4 |
| Total | 300 | 235 |
The first column of Table 2 shows the mean levels and standard deviations for each of the variables. There is no theoretical reason why men and women should differ on these variables, and indeed they do not. There were no gender differences in mean levels of depression, anxiety, anticipated stigma, centrality, or salience (all ps > .33). There was a small gender difference on the cultural stigma ratings (men = 5.18, women = 4.99), t(298) = 2.00, p = .05, but this difference was not replicated in Study 2.
Table 2. Means (SDs) of Variables in Studies 1 and 2.
| Variable | Study 1 | Study 2 |
|---|---|---|
| Anticipated stigma | 2.80 (1.38) | 2.71 (1.42) |
| Centrality | 4.17 (1.50) | 4.60 (1.37) |
| Salience | 1.26 (1.88) | 2.26 (2.23) |
| Cultural stigma | 5.04 (0.67) | 5.04 (0.67) |
| Distress | 0.02 (0.60) | — |
| CES-D | 20.63 (11.77) | 22.02 (12.50) |
| STAI-T | 2.37 (0.54) | — |
| Illness symptoms | — | 17.13 (11.10) |
Note. All measures were scaled such that greater values indicate higher levels of each construct. Anticipated stigma, centrality, and cultural stigma were rated on 7-point scales ranging from 1 to 7. Salience was measured as thoughts per day. Distress is a composite measure of standardized scores of depression (CES-D) and anxiety (STAI-T). Depression (CES-D) and illness symptoms (PILL) are reported as sums. Trait Anxiety (STAI-T) was rated on a 4-point scale ranging from 1 to 4. Dashes indicate that data were not obtained. CES-D = Center for Epidemiological Studies-Depression scale; STAI-T = State-Trait Anxiety Inventory-Trait scale; PILL = Pennebaker Inventory of Limbic Languidness.
Overall, participants showed a great deal of variability in the extent to which they deemed the identity central to the self. The mean fell in the middle of the scale with a 1.5-point standard deviation. Thus, the sample includes participants for whom the concealed identity ranged from not at all definitional of the self to extremely central to the self. Likewise, the frequency with which the identity was on the minds of the participants varied greatly. Some participants rarely thought of the identity: 32% of the sample reported they thought of the identity once a month or less, whereas 34% of the sample reported they thought of their identity once a day or more. Participants reported relatively low levels of anticipated stigma, reflecting their beliefs that they were unlikely to suffer from overt discrimination.
Finally, distress was quite high in the sample. The mean on the depression scale was 20.63. A frequency analysis showed that 59% of the sample fell at or over a score of 16, which is used as the clinical cutoff point for depression diagnosis (Radloff, 1977). Surveys of the general population have found mean CES-D scores around 9 (Weissman, Sholomskas, Pottenger, Prusoff, & Locke, 1977), although surveys of young adults have sometimes shown a mean closer to 15 (Radloff, 1991).
Predicting Distress
Table 3 (above the diagonal) shows the bivariate correlations between the variables. As predicted, anticipated stigma, identity centrality, salience of identity thoughts, and cultural stigma were all positively related to psychological distress.
Table 3. Bivariate Correlations Among Variables in Studies 1 and 2.
| Variable | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. Anticipated stigma | — | .26** | .36** | .28** | .43** |
| 2. Centrality | .17** | — | .32** | .09 | .40** |
| 3. Salience | .12 | .32** | — | .14* | .40* |
| 4. Cultural stigma | .02 | –.04 | .12 | — | .24** |
| 5. Distressa | .33** | .32** | .22** | –.03 | — |
| 6. Illness symptoms | .27** | .16* | .16* | .16* | .38** |
Note. Correlations above the diagonal are from Study 1. Correlations below the diagonal are from Study 2.
Distress in Study 1 is based on a composite of the Center for Epidemiological Studies–Depression scale (CES-D) and the State–Trait Anxiety Inventory–Trait scale; distress in Study 2 is based on the CES-D only.
p < .05.
p < .01.
Examining the direct effects of stigma-related factors
Although previous research and theory has discussed each variable individually as a predictor of distress, no previous research has examined all four variables simultaneously. Given that many of the variables were correlated with each other, a linear regression predicting distress in which all predictors were entered simultaneously was conducted.4 In this way, the unique effect of each stigma variable could be examined. All of the intraindividual variables (anticipated stigma, centrality, salience) were entered on the first step, followed by cultural stigma on the second step. As seen in Table 4, anticipated stigma, centrality, and salience were each significant predictors of distress. Supporting our hypotheses, more anticipated stigma, increased centrality, and increased salience were each uniquely related to increased distress. In the second step of the regression, cultural stigma significantly added to the variance accounted for in distress. Thus, cultural stigma—a variable completely external to the participants—impacted distress. There was practically no change in the betas of the intraindividual variables, indicating that cultural stigma was a relatively separate source of distress. The full model was significant, F(4, 295) = 35.38, p < .001, accounting for a third of the variance in distress (R2 = .32). Thus, results supported our hypothesis that these four variables are unique predictors of distress for people with concealable stigmatized identities.
Table 4. Linear Regression Predicting Distress.
| Predictor | Step 1 β | Step 2 β |
|---|---|---|
| Anticipated stigma | .29*** | .26*** |
| Centrality | .26* | .26*** |
| Salience | .21*** | .21*** |
| Cultural stigma | .11* |
p < .05.
p < .001.
Examining the mediated model
A second goal with the current data was to consider both the direct and indirect effects of these factors on psychological distress. We theorized that, as shown in Figure 1, anticipated stigma would have a direct effect on distress but would also work indirectly through its relationships with centrality and salience. Cultural stigma was predicted to have only a direct effect on distress. Using Amos 6.0 software (Arbuckle, 2005), we utilized structural equation modeling to test the model. Direct maximum likelihood estimation of missing data was used to allow information from the full sample (N = 300) to be used in the structural analyses. Each of our variables was represented as a measured variable in the model. The exogenous variables (anticipated stigma and cultural stigma) were correlated in order to represent the causal influences of variables not measured in the model (Kline, 2005). Finally, we assessed model fit with four indexes: chi-square, root-mean-square error of approximation (RMSEA; Steiger, 1998), comparative fit index (CFI; Bentler, 1990), and the Akaike information criterion (AIC; Akaike, 1987). A nonsignificant chi-square value, an RMSEA value of .06 or lower, and a CFI value greater than .95 indicate good fit (Hu & Bentler, 1999). Because we also wanted to be able to compare alternative, nonhierarchical models to our hypothesized model, we also reported the AIC, which is a goodness-of-fit measure that is adjusted to penalize for model complexity. Thus, when comparing alternative, nonhierarchical models, the one with the lower AIC is preferred (Hu & Bentler, 1995).
We first tested the saturated model. Consistent with our hypotheses, the paths from cultural stigma to centrality and salience were nonsignificant (all ps > .49) and were deleted from the model. The trimmed model (see Figure 3) fit the data well, χ2(2) = 0.59, ns, CFI = 1.0, RMSEA = .00, AIC = 36.6, and all remaining paths were significant (all ps < .05). There was a significant direct effect of cultural stigma on psychological distress. Anticipated stigma had a direct effect on distress, but it also had indirect effects on psychological distress through centrality and salience. Taken together, the model that provided the best fit for our data indicates that anticipated stigma associated with one's concealed identity impacts psychological distress directly and indirectly on the basis of the extent to which the identity is central and salient to the self. Cultural stigma, or degree of actual social devaluation associated with one's concealed identity, directly affects one's experience of psychological distress.
Figure 3.

Structural equation model of anticipated stigma, centrality, salience, and cultural stigma effects on psychological distress reflecting results of Study 1.
Alternative explanations
With correlational data it is impossible to definitively determine direction of causality or to rule out all possible alternative third-variable explanations. We can, however, offer additional analyses to identify plausible alterative models and compare such models to our hypothesized model in order to help draw useful conclusions from our data (Tomarken & Waller, 2003).
First, it is possible that the directions of the causal relationships between the variables in the proposed model were different from how we theorized them to occur. In order to examine this alternative hypothesis, we tested the fit of a model in which centrality, salience, and cultural stigma were exogenous variables, and we examined the direct and indirect effects of these two variables on anticipated stigma and distress. Path coefficients largely replicated the original model, but this alternative model showed slightly worse fit for the data, χ2(1) = 2.61, ns, CFI = .99, RMSEA = .07, AIC = 40.6. In addition, the AIC for the alternative model was higher (40.6 vs. 36.6), indicating that our hypothesized model is preferred.
Second, it is possible that our model may fit well for only particular subgroups of participants. One such alternative is that the model fitted for only the mental illness group. To test for the possibility that those in the mental illness group (who were also likely high in depression and anxiety) were driving our results, we tested an alternative model without them. This model fit equally well, χ2(2) = 0.21, ns, CFI = 1.00, RMSEA = 0.0, AIC = 36.2. All of the path coefficients were of similar weight, and all remained significant. Thus, our original hypothesized model fit equally well for people whose concealable stigmatized identity was not mental illness.
Likewise, given that our sample was predominantly female, it may also be plausible that this model fit the data better for women than for men. Thus, we ran the model separately for men and women. Our hypothesized model fit well for both women, χ2(2) = 1.32, ns, CFI = 1.00, RMSEA = 0.0, AIC = 37.3, and men, χ2(2) = 0.40, ns, CFI = 1.00, RMSEA = .00, AIC = 36.4, when examined separately.
Finally, a third alternative explanation is that there was some general personality factor or style—such as a proneness to be more negative, anxious, or neurotic—that was predicting both distress and the stigma variables. While we cannot rule out all possibilities, we did collect a measure of rumination. Rumination is a style of thinking in which people chronically brood on negative thoughts. Consistent with previous research (e.g., Nolen-Hoeksema, Stice, Wade, & Bohon, 2007), the relationship between rumination and distress was quite strong in our sample (r = .61). To help rule out the possibility that such a personality variable might account for the relationships found between our identity-related stigma variables and distress, we conducted an additional linear regression. In the first step, we entered rumination. As expected, rumination was a strong predictor of distress (β = .61, p < .001). In the second step, we entered our identity-related variables: anticipated stigma, centrality, salience, and cultural stigma. If a negative coping style such as rumination explained the relationship between the identity variables and distress, the relationship between the identity variables and distress should drop to nonsignificant. They did not. Each of the variables remained significant predictors of distress at p < .05, with the exception of cultural stigma, which slipped to p = .06. Thus, even controlling for a major psychological vulnerability factor toward depression and negative thought, anticipated stigma, centrality, salience, and cultural stigma remained predictive of psychological distress.
Examining Associative Stigma
Our final set of hypotheses for these data examined whether there were differences in the reported distress level for people with associative versus personal stigma and whether these differences were mediated by the lower levels of anticipated stigma, centrality, and salience that people with an associative stigma (compared with personal stigma) are likely to possess. As predicted, compared with those with a personal stigma, participants with an associative stigma reported significantly less distress, less anticipated stigma, lower identity centrality, and less salience (see Table 5 for means and standard deviations). Next, we examined whether the identity variables (centrality, salience, and anticipated stigma) were associated with distress for those with an associative stigma. Examining correlations for those with an associative stigma only, we found that centrality (r = .35), salience (r = .32), and anticipated stigma (r = .37) were all significantly related to distress (p < .01). Thus, despite the lower levels of distress, the relationships between the identity variables and distress were similar for people with an associative stigma and people with a personal stigma. Cultural stigma was not significantly predictive of distress (r = .11, ns), but this was not surprising given there were only three different types of associative stigma (family members with mental illness, family members with addiction, and family members with abusive relationships), and all had fairly similar cultural stigma ratings (4.11 to 4.88).
Table 5. Comparing Means (SDs) for Personal Stigma and Associative Stigma.
| Variable | Personal stigma | Associative stigma |
|---|---|---|
| Anticipated stigma | 2.98 (1.37) | 2.07 (1.16) |
| Centrality | 4.32 (1.48) | 3.59 (1.43) |
| Salience | 1.46 (2.00) | 0.44 (0.92) |
| Cultural stigma | 5.18 (0.66) | 4.48 (0.37) |
| Distress | 0.07 (0.62) | −0.17 (0.49) |
Note. Differences between means are significant at p < .05.
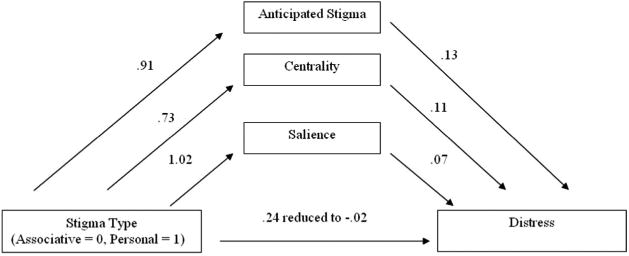
Finally, we examined whether the association between stigma type (associative vs. personal) and distress was mediated by the identity variables. As shown above, we know that possessing an associative stigma (vs. possessing a personal stigma) is associated with (a) less distress and (b) lowered mean levels of each of the identity variables. In addition, (c) each of the identity variables is significantly correlated with distress. In order to examine mediation with multiple mediators (Kenny, Kashy, & Bolger, 1998), in the final step we examined whether the relationship between stigma type (associative vs. personal) and distress would be eliminated when the mediating variables are included. We conducted a linear regression predicting distress in which the categorical variable of stigma type (coded 0 = associative stigma, 1 = personal stigma) was entered in the first step, and the three identity variables (centrality, salience, and anticipated stigma) were entered in the second step. As predicted, stigma type was significant in the first step (β = .16, p < .01), but this relationship dropped to zero (β = –.01, ns) when the identity variables were entered, each of which were significant predictors of distress.
Because we were examining multiple correlated mediators, we used a method developed by Preacher and Hayes (2008) to produce the path coefficients presented in Figure 4. Bootstrapping and use of multivariate coefficient products resulted in practically identical results. We first examined whether the total effect of stigma type on distress (B = 0.24, p < .01) was accounted for by the mediators when they were considered as a group. When the three mediators were included, the direct effect of stigma type on distress was reduced to zero (B = −0.02, ns), mirroring the effect shown when using simultaneous regression above. Figure 4 shows that each path coefficient was significant at p < .01. In addition to accounting for a significant amount of the distress as a group, each of the indirect paths could be examined. The indirect effects for each path were computed while controlling for the effects of the other mediators. Each indirect effect was significant (p < .01), with a point estimate of .12 for anticipated stigma, .08 for centrality, and .07 for salience. In summary, people with an associative stigma reported less distress than did those with a personal stigma, and this difference was completely mediated by the higher levels of anticipated stigma, identity centrality, and identity salience of people with personal concealed stigmatized identities.
Figure 4.
Mediation model of personal stigma versus associative stigma on psychological distress reflecting results of Study 1.
Discussion
In the current study we sought to test a model for predicting psychological distress for people with concealable stigmatized identities. To our knowledge, this is the first test of a framework combining both intraindividual variables and an external variable for predicting distress. In support of our hypotheses, the extent to which people anticipate social devaluation if the identity is revealed, the more central the identity is to the self, the more salient the identity is, and the extent to which the identity is considered culturally stigmatized each uniquely predicted variance in psychological distress in a sample of participants with a wide variety of concealable stigmatized identities.
In order to gain insight into the processes of how stigma can ultimately impact distress levels, we used structural equation modeling to simultaneously examine the direct and indirect effects of anticipated and cultural stigma on distress through centrality and salience. As predicted, we found that cultural stigma—a measure of devaluation completely external to the study participants— had a direct effect on distress but no indirect effects through centrality or salience. Anticipated stigma, however, had a more complicated relationship to distress. The direct effect from anticipated stigma to distress remained strong, but anticipated stigma also worked indirectly through its relationships with centrality and salience. Thus, people who anticipate social devaluation and rejection if they reveal their identity also report greater centrality and salience of the identity, which in turn relate to increased reports of distress. To our knowledge, these results are the first to provide a general framework for understanding the mechanisms through which stigma impacts the lives of those who live with a concealable stigmatized identity.
Our sample also afforded us the chance to examine associative stigma. Three of the identities in our sample stemmed from associations with stigmatized family members, including family members with mental illness, addictions, and abusive relationships. Although the magnitude of the correlations between each of the stigma variables (anticipated stigma, centrality, and salience) and distress were the same for people with personal stigma versus associative stigma, people with an associative stigma reported less anticipated stigma, centrality, salience, and distress. Further, we found that the difference in level of distress was completely mediated by anticipated stigma, centrality, and salience. Thus, our theoretical framework holds across a broad spectrum of concealable stigmatized identities, including those characterized as either personal or associative stigmas.
Study 1 provided initial support for our framework examining how anticipated stigma, centrality, salience, and cultural stigma relate to psychological distress in a sample of people with concealable stigmatized identities. These findings are important because they extend previous theorizing to the context of concealable stigmatized identities and allow researchers to further understand the phenomenological experience of living with such an identity. However, given the novelty of our approach, we wanted to replicate our general pattern of findings in a second sample of people with concealable stigmatized identities. Further, we chose to extend the model by examining the effects of stigma on health.
Study 2
Stigma has been frequently linked to poorer health outcomes (for reviews, see Major & O'Brien, 2005; Williams et al., 2003). Stigma's role in negative health consequences is multiply determined, including indirect effects on health through psychological distress (i.e., the two are often strongly comorbid) and direct effects on health through increased stress of both experiences of discrimination and institutionalized discrimination built into the health care system.
In Study 2, we tested a model in which anticipated stigma, centrality, salience, and cultural stigma predicted psychological distress and illness symptoms (see Figure 2). Consistent with the results from Study 1, we expected to replicate the pattern of direct and indirect effects between the stigma-related variables and psychological distress. We also predicted, on the basis of a large body of work showing that psychological distress and negative health outcomes are highly comorbid (e.g., Gallo, Armenian, Ford, Eaton, & Khachaturian, 2000; Knox et al., 2006; Penninx et al., 1998), a strong direct relationship between the experience of psychological distress and illness symptoms.
Our hypotheses for the relationships between anticipated stigma, centrality, salience, and cultural stigma and illness symptoms were more tentative because they had not been previously examined. Because previous research has shown effects of perceived prejudice and experienced discrimination on health (e.g., Katz & Nevid, 2005; Kessler et al., 1999), we hypothesized that both anticipated stigma and cultural stigma would have direct effects on the experience of health problems. We had no a priori reason to predict that centrality and salience would have direct effects and thus predicted that they would only indirectly affect health outcomes through the experience of psychological distress.
In sum, by testing the pattern of relationships shown in Figure 2, we aimed to replicate the pattern of findings in Study 1 and to examine how these stigma variables impact health outcomes for people living with a concealable stigmatized identity.
Method
Participants
We used the same recruitment strategy as noted in Study 1. However, we used a new method to determine eligibility: Students were presented with a checklist and were asked to indicate whether they were currently concealing any of the 13 identities we examined in Study 1. A total of 3,956 students were prescreened with the checklist over the course of 3 semesters. Of these, 1,063 (27%) reported possessing a concealable stigmatized identity and were eligible to sign up for the study. Because the study was completely anonymous, we did not link participants' answers in prescreening to their data collected in the study. Once participants came to the study, they were asked to describe their concealed identity in their own words, just as was done in Study 1. A total of 272 participants completed the survey. Of these, 235 participants indicated a codable stigmatized identity and were included in analyses. Participants completed the survey as partial fulfillment of a course requirement. Participants were predominantly female (63.0%) and Caucasian (82.6%), and the mean age was 18.87 years (SD = 1.38).
Procedure
Procedures of Study 2 replicated those of Study 1. Participants were first given the same explanation of a concealed identity. The participants were then asked to describe their hidden experience or identity in their own words and were told that it would be referred to as their “concealed identity” in the survey.
Measures
Nature of the concealed identity
Although participants were eligible to complete this study only if they indicated during the prescreening session that they had one of the 13 different types of stigmas we examined in Study 1, participants were again asked to write about their concealed identity in an open-ended essay. Two raters coded these open-ended responses into one of the 13 types of identities we examined in Study 1 (see the second column of Table 1 for the full list and frequency counts). Responses that were considered uncodable (e.g., the question was left blank or the response did not include enough information for the coders to categorize it) or that did not fall into these 13 categories because they were not clearly stigmatized (e.g., death of a family member, past failures on important exams, hidden temper) were excluded. Interrater reliability was again high (κ = .89), and discrepancies were resolved through discussion. As with Study 1, participants indicated living with their concealed identities for a mean length of time of approximately 5 years.
Anticipated stigma
In order to assess the extent to which people thought they would be socially stigmatized if they revealed their identity, we had participants complete the same 15-item scale used in Study 1 (α = .96).
Identity centrality
We used the same modified version of the Importance to Identity subscale of the Collective Self-Esteem scale (Luhtanen & Crocker, 1992) used in Study 1 to examine the centrality of the concealable stigma to self (α = .74).
Identity salience
Participants completed the same one-item measure used in Study 1 to assess the frequency with which they reported thinking about their concealed identity. Again, responses were converted to a response rate of times per day for analyses.
Psychological distress
Only the 20 items from the CES-D were used as a measure of psychological distress for this study (α = .93).
Illness symptoms
The Pennebaker Inventory of Limbic Languidness (PILL; Pennebaker, 1982) was used to assess current illness symptoms. The PILL is a 54-item assessment of common physical symptoms and sensations (e.g., chest pain, nausea, coughing), and validation studies show that scores on the PILL are related to the actual number of physician visits within the past year, the number of days that activities of daily living have been limited due to health problems, and the number of work absences due to health problems (Pennebaker, 1982). Participants were asked to rate the frequency with which they had experienced each symptom on the following 5-point Likert scale: 1 (have never/almost never experienced symptom), 2 (less than 3– 4 times per year), 3 (every month), 4 (every week), 5 (more than once each week). The PILL is scored by summing the total number of symptoms that participants indicated experiencing once every month or more (i.e., scores of 3, 4, or 5). Consistent with findings from prior research that has utilized the PILL (e.g., Pennebaker, 1982; Richards, Beal, Seagal, & Pennebaker, 2000; Sloan, Marx, & Epstein, 2005), the internal reliability of this scale was high (α = .95).
Cultural stigma
Because our sample in Study 2 consisted of the same types of concealable stigmatized identities that we assessed in Study 1, we used the same ratings of cultural stigma that were reported in Study 1.
Results
Descriptive information about the sample is given in Tables 1–3. Generally, means and standard deviations for all variables were similar to those found in Study 1. Again, for the sake of completeness we examined whether there were differences between men and women in the mean levels of each of the variables. Men and women did not significantly differ in level of depression, health outcomes, anticipated stigma, centrality, or cultural stigma (all ps > .47). There was a marginal difference in salience levels reported (men = 1.86, women = 2.44), t(228) = −1.9, p = .06.
Again, there was a great deal of variability in centrality, with mean level of centrality just above the midpoint of the scale. The salience of concealed identity also ranged across the whole scale, although overall salience was higher in this study compared with that in Study 1. Approximately 16% of the sample reported thinking about the identity once a month or less, whereas 58% reported thinking about the identity once a day or more. Mean levels of anticipated stigma were again relatively low. Scores on the depression inventory revealed relatively high levels of depression, with 66% of the sample falling above the cutoff point of 16 used to diagnose depression (Radloff, 1977). Participants reported a mean sum of 17.28 (SD = 11.10) on the PILL, which is similar to the mean sums reported in the original validation study for the PILL (M = 17.9, SD = 4.5; Pennebaker, 1982) and subsequent research utilizing this measure (M = 21.6, SD = 11.2; Sloan et al., 2005) among college samples.
Predicting distress and health
Again we used structural equation modeling to test a model of the direct and indirect effects of anticipated stigma, centrality, and salience on distress and illness symptoms. Direct maximum likelihood estimation of missing data was used to allow information from the full sample (N = 235) to be used in the analyses. Each of our variables was represented as a measured variable in the model. Anticipated stigma and cultural stigma again acted as the only exogenous variables in the model, and they were again correlated in order to represent the causal influences of variables not measured in the model (Kline, 2005). We first tested the full, saturated model. Unlike in our Study 1 model, the paths from anticipated stigma to salience, and from cultural stigma to distress, were nonsignificant (all ps > .40), so they were deleted from the model. Additionally, as predicted, the paths from cultural stigma to centrality, centrality to illness symptoms, and salience to illness symptoms were also nonsignificant (all ps >.40), so they were also deleted from the model. The trimmed model (see Figure 5) fit the data well, χ2(5) = 3.07, ns, CFI = 1.0, RMSEA = .00, AIC = 47.07, and all remaining paths were significant (all ps < .05) except for the path from salience to depression, which was marginally significant (p = .08). The model accounted for 19% of the variance in depression and 19% of the variance in reported illness symptoms.
Figure 5.

Structural equation model of anticipated stigma, centrality, salience, cultural stigma, and distress effects on health reflecting results of Study 2. PILL = Pennebaker Inventory of Limbic Languidness. †p = .08.
We then replicated the series of alternative models we tested in Study 1. We tested the fit of a model in which centrality, salience, and cultural stigma each acted as exogenous variables, and we examined the direct and indirect effects of these three variables on anticipated stigma and distress. Path coefficients largely replicated the original model, and this alternative model provided adequate fit for the data, χ2(5) = 4.13, ns, CFI = 1.0, RMSEA = .00, AIC = 48.13. The chi-square, CFI, and RMSEA fit indexes of this alternative model were similar to those obtained in our hypothesized model, although the AIC for the alternative model was slightly higher (48.13 vs. 47.07), indicating that our hypothesized model was preferred.
We also tested an alternative model without participants who reported a mental illness. This model fit similarly well, χ2(5) = 6.78, ns, CFI = .98, RMSEA = .05, AIC = 50.79. All of the path coefficients were of similar weight, and all remained significant. Thus, our original hypothesized model fitted equally well for people whose concealable stigmatized identity was not mental illness.
Likewise, given that our sample was predominantly female, it may also be plausible that this model fit the data better for women than for men. Thus, we ran the model separately for men and women. Our hypothesized model fit well for both women, χ2(5) = 4.06, ns, CFI = 1.00, RMSEA = .00, AIC = 48.08, and men, χ2(5) = 6.52, ns, CFI = .94, RMSEA = .06, AIC = 50.52, when examined separately. Although the fit statistics were lower for the men-only model than for the women-only model, these statistics indicate that their data did fit the model on the basis of conventional values.
Discussion
We sought to replicate the basic pattern of results of Study 1 and use our conceptual framework to examine self-reported illness symptoms. Study 2 again demonstrated that anticipated stigma, centrality, and salience directly predicted distress. Anticipated stigma also affected distress indirectly through centrality but not through salience. Interestingly, cultural stigma did not directly predict psychological distress but it did predict illness symptoms.5
As expected, distress (as measured by depression) was the strongest predictor of illness symptoms. Anticipated stigma also had a direct effect on illness symptoms, signifying that the more people believed others would devalue them if their identity were known, the more illness symptoms they experienced. Moreover, cultural stigma directly predicted illness symptoms—people who possessed identities that were more culturally devalued reported greater illness symptoms. However, contrary to our expectations, anticipated stigma was not significantly related to salience, and cultural stigma had a small but significant effect on one intraindividual variable, salience, which was marginally related to distress. Taken together, the results present a framework for understanding how intraindividual factors and external stigma can impact both psychological distress and health for people living with concealable stigmatized identities.
General Discussion
Despite the fact that both researchers and practitioners have acknowledged that stigma is a powerful predictor of life outcomes (Link & Phelan, 2006; Major & O'Brien, 2005; DHHS, 1999), current research lacks a thorough understanding of how stigma affects psychological and health well-being. Furthermore, social psychological research examining the effects of stigma has been largely one-sided, focusing predominantly on visible stigmas such as race and gender (for reviews, see Crocker et al., 1998; Major & O'Brien, 2005). In the current research, we proposed, and found support for, a conceptual framework that can be used to examine how both intraindividual factors (i.e., anticipated stigma, centrality, and salience) and an external factor (i.e., level of cultural stigma) are related to psychological distress and illness symptoms for people who live with a concealable stigmatized identity.
Study 1 demonstrated that anticipated stigma, centrality, salience, and cultural stigma each independently relate to greater psychological distress among people who live with concealable stigmatized identities. Study 1 also showed that the effect of anticipated stigma on distress occurred through its impact on centrality and salience. Thus, the intraindividual experience of stigma had both direct and indirect effects on psychological well-being.
Study 2 largely replicated these results. Again, we demonstrated that anticipated stigma, centrality, and salience had a direct effect on psychological distress, although the effect of salience on distress was weaker than that of the other variables. Further, Study 2 results demonstrated that the effect of anticipated stigma on distress also occurs indirectly, although its effects occurred via only centrality and not salience. Importantly, in order to get a more holistic sense of how stigma impacts people's psychological and health well-being, we examined how these processes impact both psychological distress and illness symptoms. These results demonstrated that anticipated stigma does have a direct and negative effect on both psychological and health well-being and that cultural stigma has a direct effect on health well-being. However, the effect of the other intraindividual processes— centrality and salience—may impact health only indirectly, by predisposing people to experience more psychological distress.
Results from the current research give greater theoretical insight into the role of stigma in the lives of people living with a concealable stigmatized identity. We took a multidimensional approach to examining the effect of stigma on psychological distress by assessing both anticipated and cultural stigma. Examining anticipated stigma is particularly important for people with concealable stigmatized identities. If their identity is truly concealed from most people they come into contact with, then they may have experienced little direct discrimination. Instead, knowing that their identities are devalued and potentially being exposed to hostile talk and attitudes about their identity by unknowing others (e.g., Wahl, 1999) will lead them to anticipate that others will devalue them if their identities become known. Although participants' reported levels of anticipated stigma were relatively low (they did not think it was highly likely that others would discriminate against them if they revealed the identity), they were a strong predictor of psychological distress and directly predicted poorer health functioning. Similar to identity threat (Steele, Spencer, & Aronson, 2002), stigma has an insidious, undermining effect even in the absence of direct discrimination. The worry and concern about possible devaluation alone can lead to negative outcomes.
In addition, our measure of anticipated stigma addressed some of the conceptual murkiness of previous measures. In our measure we ask directly, “If others knew your concealed identity, how likely would the following be to occur …,” followed by a host of potential types of discrimination and social rejection. Previous research has tended to ask to what extent people know the stereotypes about their group or agree with the stereotypes rather than ask whether they think discrimination is likely to happen to them personally. We believe this is a real strength of the measure and more directly taps the way that a concealed stigmatized identity impacts the self. People often do not know what will happen when they reveal the identity, but their concerns about it will likely affect their behavior.
Stigma does not take place solely within the individual; instead it originates from the social devaluation attached to a particular identity within the society. Although social scientists recognize the social construction of stigma, we rarely attempt to measure it. In the current work, we developed a novel measure of cultural stigma in which we obtained ratings of relative devaluation of each of the identities represented in our samples, and then we used the external stigma ratings to predict distress and health. We found that this external measure of stigma was related to distress (in Study 1) and health (in Study 2), even controlling for the effects of the intra-individual variables. By demonstrating the power of cultural stigma, we hope to highlight that stigma does not occur solely within the individual.
In addition to developing new measures of anticipated and cultural stigma, we sought to address a theoretical quandary about centrality. We found that centrality is positively related to distress, signifying that the more central the identity is to the self, the more distress is reported. Although people with visible stigmas may reap psychological benefits from identity centrality because they can utilize mechanisms that provide group-based social support and attributional processes (e.g., Crocker & Major, 1989), according to our data identity centrality seems to render people who live with a concealed identity more vulnerable to distress. That is, because they may anticipate and experience prejudice due to their identity but cannot necessarily use their group-based identity to buffer themselves from these negative outcomes, people whose concealed identities are central to their self-definition may be increasingly susceptible to psychological distress. This finding points to the necessity for more nuanced work on different types of stigmatized identities. While we believe many of the concerns and experiences of people living with concealed versus visible identities overlap, the dimension of visibility may shape identity and coping in some fundamentally different ways (Quinn, 2006).
Results also showed that people whose concealed stigmatized identity is highly salient in their daily lives report increased psychological distress. Previous experimental works shows that actively hiding a salient stigmatized identity results in more cognitive work due to increased concern with controlling and suppressing thoughts about the stigmatized identity (Smart & Wegner, 1999). Likewise, dealing with increasingly negative and intrusive thoughts about an identity (Major & Gramzow, 1999) is related to more distress. Thus, the current work maps onto previous work showing that the more frequently a person is thinking about a stigmatized identity, the more distressing the identity is likely to be. More research is needed to answer whether the distress results from the increased cognitive work of hiding information (Smart & Wegner, 1999), from the potential feelings of shame or inauthenticity that come from hiding an important part of the self (Kelly, 2002), or from a close relationship between identity frequency and intrusive thoughts about being stigmatized (Major & Gramzow, 1999). Moreover, while we treated salience as a trait-level variable, it is likely that particular situations make the identity more or less salient. Thus, identity salience may fluctuate more than do centrality or anticipated stigma on a day-to-day basis. It is also possible, however, that people learn to avoid contexts that are related to the identity, thereby working to keep the level of salience relatively stable.
Beyond adding to the literature on anticipated stigma, cultural stigma, centrality, and salience, we also examined associative stigma in Study 1. Although the concept of associative, or courtesy, stigma has been around in the psychological literature since at least the 1960s, and the larger concept of family stigma (e.g., that disgraced family members taint the honor of the whole family) is strong in many cultures around the world, there has been little research on the psychological ramifications. In our sample, three of the concealed identities stemmed from associations with stigmatized family members, including family members with mental illness, addictions, and abusive relationships. As with people reporting personal stigmas, those reporting associative stigmas were also affected by the anticipated stigma, centrality, and salience of the identity. The differences in mean levels of centrality, salience, and anticipated stigma also lend concurrent validity to these measures. That is, if they are important variables related to stigmatized identities, they should be lower for people with less stigmatized identities and higher for people with more stigmatized identities. That is exactly what we found.
Limitations
There are several limitations to the current research. First, because we focused on explicating general processes, and because we have only small numbers of many of the identities, it is not possible to test our model on each specific identity. Thus, we must be cautious about whether these variables will be equally predictive for different concealable stigmatized identities. Future research could examine identities separately as well as add identity-specific variables to increase prediction (e.g., level of sexual assault activism for people who have experienced rape). The fact that the centrality, salience, and anticipated stigma variables predicted distress for both personal and associative stigmas supports the generalizability of the work across a range of identities. However, because the research was done with a college population, future work needs to examine whether the models generalize to both a broader adult population and to more specific and marginalized populations who may already be bearing the brunt of other stigmatized conditions such as homelessness and poverty.
Our primary goal in the current work was to establish a conceptual framework for understanding which factors may undermine psychological and health well-being for people with concealable stigmatized identities and to provide data to substantiate the basic structure of this model. In this work, we examined the utility of our basic conceptual model by imposing a set of causal relationships on our data and examining whether these relationships adequately fit the data across two separate samples. Results indicate that this basic structure adequately represented the relationships among these variables across both studies. However, it is important to keep in mind the limitations of structural equation modeling. The nature of these relationships represents the specific covariance structure of our data, a structure that may have some degree of variability depending on the makeup of the sample in question. This variability is likely one reason why the impact of cultural stigma on psychological distress did not replicate in Study 2. The relationships between cultural stigma and other variables are especially tied to the composition of the identities that our participants possessed and the degree to which these identities were socially stigmatized. Thus, given that the proportion of each type of identity (and its concomitant social stigmatization) varied from Study 1 to Study 2, this variability will inevitably influence the results of our analyses. Therefore, although we expect that future work will replicate the basic pattern of results that we have obtained across two separate samples, the specific path weights and relative fit of this model in other samples will ultimately depend on the unique covariance structure of those data.
Another limitation to the current research is its cross-sectional nature. With correlational data collected at only one point in time, it is not possible to establish causal direction. It is possible that people who are already distressed report more identity centrality, more salience, and anticipate more stigma from others. Although we tried to rule out several alternative models with additional analyses, a longitudinal design in which we collect distress and health data over multiple time periods is needed to further address questions of directionality. We expect that the relationship is likely bidirectional over time.
We examined several theoretically derived predictors of distress, but there are at least two important variables not included in our current model. The amount of discrimination actually experienced over the lifetime is likely to predict distress. Previous research has shown that people with mental illness report greater depression when they have had experiences of discrimination (Markowitz, 1998) and rejection (Link et al., 1997). Experiencing discrimination due to sexual orientation is positively related to loneliness and depression and negatively related to self-esteem (Diaz, Ayala, & Bein, 2004; Ramirez-Valles, Fergus, Reisen, Poppen, & Zea, 2005). Thus, to the extent that people have revealed their identities to others, experiences of discrimination will be important to include in future work.
The current model also does not address issues around disclosure experiences. Previous research on disclosure of stigmatized identities (e.g., HIV, sexual orientation, child abuse, sexual assault, and mental illness) has shown that revealing the stigmatized identity can have a number of both positive (e.g., greater cognitive resolution, increased relationship closeness, and decreased feelings of isolation) and negative (e.g., increased trauma-related symptoms, loss of relationships, physical harm) consequences (e.g., Cain, 1991; Derlega, Winstead, Greene, Serovich, & Elwood, 2004; Gidron, Peri, Connolly, & Shalev, 1996; Herek, Gillis, Cogan, & Glunt, 1997; Lepore, Fernandez-Berrocal, Ragan, & Ramos, 2004). Thus, explaining disclosure and connecting it to other stigma-related feelings and cognitions is a particularly ripe area for future research.
Conclusion
At the broadest level, living with stigma— both visible and concealable— encompasses issues of identity and self-definition (centrality, salience, collective esteem), treatment and relationships (anticipated stigma, experienced stigma), outcomes (psychological distress, health, achievement, employment), and the social context in which people live (cultural stigma). Our work underscores the notion that the influence of these factors on well-being is neither simple nor direct. Some people exhibit distress; others do not. Some situations result in negative outcomes; some do not. The good news of stigma research is that many people, despite living in a culture that often devalues them, can be happy, resilient, and well adjusted. Ultimately, the goal for researchers is to be able to predict which people within stigmatized groups will be vulnerable or resilient and why. In this article, we have examined how this complex constellation of processes unfolds among those who possess a concealable stigmatized identity. In doing so, we have provided a conceptual framework that we hope will stimulate research efforts designed to understand the impact of stigmatized identities on all facets of well-being.
Acknowledgments
This research was supported by a University of Connecticut Research Foundation grant to Diane M. Quinn, and preparation of the article was supported in part by predoctoral Ruth L. Kirschstein National Research Service Award 1F31MH080651 to Stephenie R. Chaudoir. We thank Jennifer Crocker, Valerie Earnshaw, Rachel Kallen, and Jeffrey Sanchez-Burks for their comments on drafts of the article and Shondell Diaz, Karen Grudzinski, Zahra Nims, and Sarah Pennington for help with data collection and coding.
Footnotes
Throughout the article we use the term concealable stigmatized identities. We feel this term is most appropriate for two reasons. First it denotes that the person has an identity that is stigmatized by the broader culture. That is, the person does not have a “natural” or “innate” stigma but instead some sort of experience or attribute that has been culturally construed as stigmatized—a stigmatized identity. In this way we hope to both call attention to the cultural construction of stigma and avoid further dehumanizing people with stigmatized identities. Second, we use the word identity instead of mark, attribute, or label because we believe that part of the power of stigma is how it affects the self. Indeed, the presumption behind almost all psychological work on stigma is that the power of stigma is the power to change the self and identity. However, as we make clear in the sections on centrality and salience, simply possessing a stigmatized identity does not mean that it is central to the person's self-definition. Instead, people can and do vary in whether they feel the stigmatized identity is an important part of the self.
The prediction is based on the assumption that the person regularly keeps the stigmatized identity concealed or closeted. To the extent that a person is “out” and the identity is no longer concealed, processes more akin to those of visible stigmatized identities may be applicable.
Because of the nature of concealed stigmatized identities, we designed this study to be as noncoercive as possible. We wanted participants to be able to easily not answer the questions or discuss their concealed stigmatized identity if they did not feel comfortable. We also did not want them to feel further stigmatized by participating. Thus, we built several safeguards into the design. The first was the description of a “concealed identity,” which was deliberately written with neutral language and accompanied by both positive and negative concealed identities so that participants would not feel “marked” by being in the study—and so that if they wanted to write down some other, more neutral identity, they could. Second, in both studies, the data were submitted truly anonymously. We did not collect any identifying information with the data and we did not link the survey answers back to prescreening responses. Third, participants completed the survey in individual cubicles such that they would not feel that others knew they were in the study or wondered what they might have written about. Finally, we did carefully gauge their reactions at the end of the study for any indications of emotional upset, and we gave them a chance to write privately about what they thought of the study. There were no indications of negative reactions.
We also conducted the linear regression with gender and time since stigma onset in the first step. These variables were not significant predictors of distress and did not change the beta weights or significance of the rest of the variables.
Given that the cultural stigma–psychological distress relationship did not replicate in Study 2, we tested whether this null relationship was due to the fact that we assessed only depression in Study 2 rather than the depression–anxiety composite measure of distress used in Study 1. We reanalyzed our model from Study 1, using only depression as our primary outcome (rather than a composite of both depression and anxiety). This model yielded similar fit, and the relationship between cultural stigma and depression remained significant (β = .12, p < .05). Using anxiety only (rather than the composite) as our primary outcome also yielded similar fit and a marginally significant relationship between cultural stigma and anxiety (β = .09, p = .08). Thus, the nonreplication of the cultural stigma to psychological distress relationship in Study 2 does not appear to have been driven by the fact that we did not include anxiety in this outcome.
References
- Akaike H. Factor analysis and AIC. Psychometrika. 1987;52:317–332. [Google Scholar]
- Allport GW. The nature of prejudice. Cambridge, MA: Addison-Wesley; 1954. [Google Scholar]
- Arbuckle JL. Amos 6.0. Chicago: SPSS; 2005. [Google Scholar]
- Bentler PM. Comparative fit indexes in structural models. Psychological Bulletin. 1990;107:238–246. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- Birenbaum A. On managing a courtesy stigma. Journal of Health and Social Behavior. 1970;11:196–206. [Google Scholar]
- Bourguignon D, Seron E, Yzerbyt V, Herman G. Perceived group and personal discrimination: Differential effects on personal self-esteem. European Journal of Social Psychology. 2006;36:773–789. [Google Scholar]
- Branscombe NR, Schmitt MT, Harvey RD. Perceiving pervasive discrimination among African Americans: Implications for group identification and well-being. Journal of Personality and Social Psychology. 1999;77:135–149. [Google Scholar]
- Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. Journal of Consulting and Clinical Psychology. 2000;68:748–766. doi: 10.1037//0022-006x.68.5.748. [DOI] [PubMed] [Google Scholar]
- Cain R. Stigma management and gay identity development. Social Work. 1991;36:67–73. [PubMed] [Google Scholar]
- Corrigan PW, Miller FE. Shame, blame, and contamination: A review of the impact of mental illness stigma on family members. Journal of Mental Health. 2004;13:537–548. doi: 10.1037/0893-3200.20.2.239. [DOI] [PubMed] [Google Scholar]
- Corrigan PW, Watson AC. The paradox of self-stigma and mental illness. Clinical Psychology: Science and Practice. 2002;9:35–53. [Google Scholar]
- Crocker J, Major B. Social stigma and self-esteem: The self-protective properties of stigma. Psychological Review. 1989;96:608–630. [Google Scholar]
- Crocker J, Major B, Steele C. Social stigma. In: Gilbert DT, Fiske ST, Lindzey G, editors. The handbook of social psychology. 4th. Vol. 2. New York: McGraw–Hill; 1998. pp. 504–553. [Google Scholar]
- Cross WE., Jr . Shades of black: Diversity in African American identity. Philadelphia: Temple University Press; 1991. [Google Scholar]
- Cutrona CE, Russell DW, Brown PA, Clark LA, Hessling RM, Gardner KA. Neighborhood context, personality, and stressful life events as predictors of depression among African American women. Journal of Abnormal Psychology. 2005;114:3–15. doi: 10.1037/0021-843X.114.1.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cutrona CE, Wallace G, Wesner KA. Neighborhood characteristics and depression: An examination of stress processes. Current Directions in Psychological Science. 2006;15:188–192. doi: 10.1111/j.1467-8721.2006.00433.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Derlega VJ, Winstead BA, Greene K, Serovich J, Elwood WN. Reasons for HIV disclosure/nondisclosure in close relationships: Testing a model of HIV-disclosure decision making. Journal of Social & Clinical Psychology. 2004;23:747–767. [Google Scholar]
- Diaz RM, Ayala G, Bein E. Sexual risk as an outcome of social oppression: Data from a probability sample of Latino gay men in three U.S. cities. Cultural Diversity & Ethnic Minority Psychology. 2004;10:255–267. doi: 10.1037/1099-9809.10.3.255. [DOI] [PubMed] [Google Scholar]
- Eccleston CP, Major BN. Attributions to discrimination and self-esteem: The role of group identification and appraisals. Group Processes & Intergroup Relations. 2006;9:147–162. [Google Scholar]
- Erickson E. The problem of ego-identity. Journal of the American Psychoanalytic Association. 1956;4:56–121. doi: 10.1177/000306515600400104. [DOI] [PubMed] [Google Scholar]
- Frable DE, Platt L, Hoey S. Concealable stigmas and positive self-perceptions: Feeling better around similar others. Journal of Personality and Social Psychology. 1998;74:909–922. doi: 10.1037//0022-3514.74.4.909. [DOI] [PubMed] [Google Scholar]
- Friedman MA, Brownell KD. Psychological correlates of obesity: Moving to the next research generation. Psychological Bulletin. 1995;117:3–20. doi: 10.1037/0033-2909.117.1.3. [DOI] [PubMed] [Google Scholar]
- Gallo JJ, Armenian HK, Ford DE, Eaton WW, Khachaturian AS. Major depression and cancer: The 13-year follow-up of the Baltimore epidemiologic catchment area sample (United States) Cancer Causes, and Control. 2000;11:752–758. doi: 10.1023/a:1008987409499. [DOI] [PubMed] [Google Scholar]
- Gidron Y, Peri T, Connolly JF, Shalev AY. Written emotional expression in posttraumatic stress disorder: Is it beneficial for the patient? Journal of Nervous and Mental Disease. 1996;184:505–507. doi: 10.1097/00005053-199608000-00009. [DOI] [PubMed] [Google Scholar]
- Goffman E. Stigma: Notes on the management of spoiled identity. Englewood Cliffs, NJ: Prentice–Hall; 1963. [Google Scholar]
- Gray-Little B, Hafdahl AR. Factors influencing racial comparisons of self-esteem: A quantitative review. Psychological Bulletin. 2000;126:26–54. doi: 10.1037/0033-2909.126.1.26. [DOI] [PubMed] [Google Scholar]
- Griffith KH, Hebl MR. The disclosure dilemma for gay men and lesbians: “Coming out” at work. Journal of Applied Psychology. 2002;87:1191–1199. doi: 10.1037/0021-9010.87.6.1191. [DOI] [PubMed] [Google Scholar]
- Hebl MR, Dovidio JF. Promoting the “social” in the examination of social stigmas. Personality and Social Psychology Review. 2005;9:156–182. doi: 10.1207/s15327957pspr0902_4. [DOI] [PubMed] [Google Scholar]
- Herek GM, Gillis JR, Cogan JC, Glunt EK. Hate crime victimization among lesbian, gay, and bisexual adults. Journal of Interpersonal Violence. 1997;12:195–215. [Google Scholar]
- Hu LT, Bentler PM. Evaluating model fit. In: Hoyle RH, editor. Structural equation modeling: Concepts, issues, and applications. Thousand Oaks, CA: Sage; 1995. pp. 76–99. [Google Scholar]
- Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. [Google Scholar]
- Katon W, Ciechanowski P. Impact of major depression on chronic medical illness. Journal of Psychosomatic Research. 2002;53:859–863. doi: 10.1016/s0022-3999(02)00313-6. [DOI] [PubMed] [Google Scholar]
- Katz S, Nevid JS. Risk factors associated with posttraumatic stress disorder symptomatology in HIV-infected women. AIDS Patient Care and STDs. 2005;19:110–120. doi: 10.1089/apc.2005.19.110. [DOI] [PubMed] [Google Scholar]
- Kelly AE. The psychology of secrets. New York: Kluwer Academic/Plenum; 2002. [Google Scholar]
- Kenny DA, Kashy DA, Bolger N. Data analysis in social psychology. In: Gilbert DT, Fiske ST, Lindzey G, editors. The handbook of social psychology. 4th. Vol. 1. New York: McGraw–Hill; 1998. pp. 233–265. [Google Scholar]
- Kessler RC, Mickelson KD, Williams DR. The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. Journal of Health and Social Behavior. 1999;40:208–230. [PubMed] [Google Scholar]
- Kline RB. Principles and practice of structural equation modeling. 2nd. New York: Guilford Press; 2005. [Google Scholar]
- Knox S, Barnes A, Kiefe C, Lewis CF, Iribarren C, Matthews KA, et al. History of depression, race, and cardiovascular risk in CARDIA. International Journal of Behavioral Medicine. 2006;13:44–50. doi: 10.1207/s15327558ijbm1301_6. [DOI] [PubMed] [Google Scholar]
- Lepore SJ, Fernandez-Berrocal P, Ragan J, Ramos N. It's not that bad: Social challenges to emotional disclosure enhance adjustment to stress. Anxiety, Stress & Coping: An International Journal. 2004;17:341–361. [Google Scholar]
- Link BG. Understanding labeling effects in the area of mental disorders: An assessment of the effects of expectations of rejection. American Sociological Review. 1987;52:96–112. [Google Scholar]
- Link BG, Cullen FT, Struening EL, Shrout PE. A modified labeling theory approach to mental disorders: An empirical assessment. American Sociological Review. 1989;54:400–423. [Google Scholar]
- Link BG, Phelan JC. Conceptualizing stigma. Annual Review of Sociology. 2001;27:363–385. [Google Scholar]
- Link BG, Phelan JC. Stigma and its public health implications. Lancet. 2006 Feb 11;367:528–529. doi: 10.1016/S0140-6736(06)68184-1. [DOI] [PubMed] [Google Scholar]
- Link BG, Struening EL, Neese-Todd S, Asmussen S, Phelan JC. Stigma as a barrier to recovery: The consequences of stigma for the self-esteem of people with mental illnesses. Psychiatric Services. 2001;52:1621–1626. doi: 10.1176/appi.ps.52.12.1621. [DOI] [PubMed] [Google Scholar]
- Link BG, Struening EL, Rahav M, Phelan JC, Nuttbrock L. On stigma and its consequences: Evidence from a longitudinal study of men with dual diagnoses of mental illness and substance abuse. Journal of Health and Social Behavior. 1997;38:177–190. [PubMed] [Google Scholar]
- Luhtanen R, Crocker J. A collective self-esteem scale: Self-evaluation of one's social identity. Personality and Social Psychology Bulletin. 1992;18:302–318. [Google Scholar]
- Major B. New perspectives on stigma and psychological well-being. In: Levin S, van Laar C, editors. Stigma and group inequality: Social psychological perspectives. Mahwah, NJ: Erlbaum; 2006. pp. 193–210. [Google Scholar]
- Major B, Gramzow RH. Abortion as stigma: Cognitive and emotional implications of concealment. Journal of Personality and Social Psychology. 1999;77:735–745. doi: 10.1037//0022-3514.77.4.735. [DOI] [PubMed] [Google Scholar]
- Major B, O'Brien LT. The social psychology of stigma. Annual Review of Psychology. 2005;56:393–421. doi: 10.1146/annurev.psych.56.091103.070137. [DOI] [PubMed] [Google Scholar]
- Major B, Quinton WJ, Schmader T. Attributions to discrimination and self-esteem: Impact of group identification and situational ambiguity. Journal of Experimental Social Psychology. 2003;39:220–231. [Google Scholar]
- Mak WWS, Poon CYM, Pun LYK, Cheung SF. Meta-analysis of stigma and mental health. Social Science & Medicine. 2007;65:245–261. doi: 10.1016/j.socscimed.2007.03.015. [DOI] [PubMed] [Google Scholar]
- Markowitz FE. The effects of stigma on the psychological well-being and life satisfaction of persons with mental illness. Journal of Health and Social Behavior. 1998;39:335–347. [PubMed] [Google Scholar]
- McCoy SK, Major B. Group identification moderates emotional responses to perceived prejudice. Personality and Social Psychology Bulletin. 2003;29:1005–1017. doi: 10.1177/0146167203253466. [DOI] [PubMed] [Google Scholar]
- Mendoza-Denton R, Downey G, Purdie VJ, Davis A, Pietrzak J. Sensitivity to status-based rejection: Implications for African American students' college experience. Journal of Personality and Social Psychology. 2002;83:896–918. doi: 10.1037//0022-3514.83.4.896. [DOI] [PubMed] [Google Scholar]
- Mickelson KD. Perceived stigma, social support, and depression. Personality and Social Psychology Bulletin. 2001;27:1046–1056. [Google Scholar]
- Muehrer P. Research on co-morbidity, contextual barriers and stigma: An introduction to the special issue. Journal of Psychosomatic Research. 2002;53:843–845. doi: 10.1016/s0022-3999(02)00519-6. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S. Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology. 1991;100:569–582. doi: 10.1037//0021-843x.100.4.569. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Morrow J. A prospective study of depression and posttraumatic stress symptoms after a natural disaster: The 1989 Loma Prieta earthquake. Journal of Personality and Social Psychology. 1991;61:115–121. doi: 10.1037//0022-3514.61.1.115. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Stice E, Wade E, Bohon C. Reciprocal relations between rumination and bulimic, substance abuse, and depressive symptoms in female adolescents. Journal of Abnormal Psychology. 2007;116:198–207. doi: 10.1037/0021-843X.116.1.198. [DOI] [PubMed] [Google Scholar]
- Pachankis JE. The psychological implications of concealing a stigma: A cognitive-affective-behavioral model. Psychological Bulletin. 2007;133:328–345. doi: 10.1037/0033-2909.133.2.328. [DOI] [PubMed] [Google Scholar]
- Pennebaker JW. The psychology of physical symptoms. New York: Springer–Verlag; 1982. [Google Scholar]
- Penninx BW, Guralnik JM, Pahor M, Ferrucci L, Cerhan JR, Wallace RB, et al. Chronically depressed mood and cancer risk in older persons. Journal of the National Cancer Institute Monographs. 1998;90:1888–1893. doi: 10.1093/jnci/90.24.1888. [DOI] [PubMed] [Google Scholar]
- Pinel EC. Stigma consciousness: The psychological legacy of social stereotypes. Journal of Personality and Social Psychology. 1999;76:114–128. doi: 10.1037//0022-3514.76.1.114. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Hayes AR. Asymptotic and resampling strategies for assessing and comparing indirect effects in simple and multiple mediator models. Behavior Research Methods. 2008;40:879–891. doi: 10.3758/brm.40.3.879. [DOI] [PubMed] [Google Scholar]
- Quinn DM. Concealable versus conspicuous stigmatized identities. In: Levin S, van Laar C, editors. Stigma and group inequality: Social psychological perspectives. Mahwah, NJ: Erlbaum; 2006. pp. 83–103. [Google Scholar]
- Quinn DM, Kahng SK, Crocker J. Discreditable: Stigma effects of revealing a mental illness history on test performance. Personality and Social Psychology Bulletin. 2004;30:803–815. doi: 10.1177/0146167204264088. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Radloff LS. The use of the Center for Epidemiologic Studies Depression Scale in adolescents and young adults. Journal of Youth and Adolescence. 1991;20:149–166. doi: 10.1007/BF01537606. [DOI] [PubMed] [Google Scholar]
- Ragins BR. Disclosure disconnects: Antecedents and consequences of disclosing invisible stigmas across life domains. Academy of Management Review. 2008;33(1):194–215. [Google Scholar]
- Ramirez-Valles J, Fergus S, Reisen CA, Poppen PJ, Zea MC. Confronting stigma: Community involvement and psychological well-being among HIV-positive Latino gay men. Hispanic Journal of Behavioral Sciences. 2005;27:101–119. [Google Scholar]
- Richards JM, Beal WE, Seagal JD, Pennebaker JW. Effects of disclosure of traumatic events on illness behavior among psychiatric prison inmates. Journal of Abnormal Psychology. 2000;109:156–160. doi: 10.1037//0021-843x.109.1.156. [DOI] [PubMed] [Google Scholar]
- Rind B, Tromovitch P, Bauserman R. A meta-analytic examination of assumed properties of child sexual abuse using college samples. Psychological Bulletin. 1998;124:22–53. doi: 10.1037/0033-2909.124.1.22. [DOI] [PubMed] [Google Scholar]
- Rosenfield S. Labeling mental illness: The effects of received services and perceived stigma on life satisfaction. American Sociological Review. 1997;62:660–672. [Google Scholar]
- Sellers RM, Caldwell CH, Schmeelk-Cone KH, Zimmerman MA. Racial identity, racial discrimination, perceived stress, and psychological distress among African American young adults. Journal of Health and Social Behavior. 2003;44:302–317. [PubMed] [Google Scholar]
- Sellers RM, Smith MA, Shelton JN, Rowley SAJ, Chavous TM. Multidimensional model of racial identity: A reconceptualization of African American racial identity. Personality and Social Psychology Review. 1998;2:18–39. doi: 10.1207/s15327957pspr0201_2. [DOI] [PubMed] [Google Scholar]
- Shafer AB. Meta-analysis of the factor structures of four depression questionnaires: Beck, CES-D, Hamilton, and Zung. Journal of Clinical Psychology. 2006;62:123–146. doi: 10.1002/jclp.20213. [DOI] [PubMed] [Google Scholar]
- Shrout PE, Fleiss JL. Intraclass correlations: Uses in assessing rater reliability. Psychological Bulletin. 1979;86:420–428. doi: 10.1037//0033-2909.86.2.420. [DOI] [PubMed] [Google Scholar]
- Sloan DM, Marx BP, Epstein EM. Further examination of the exposure model underlying the efficacy of written emotional disclosure. Journal of Consulting and Clinical Psychology. 2005;73:549–554. doi: 10.1037/0022-006X.73.3.549. [DOI] [PubMed] [Google Scholar]
- Smart L, Wegner DM. Covering up what can't be seen: Concealable stigma and mental control. Journal of Personality and Social Psychology. 1999;77:474–486. doi: 10.1037//0022-3514.77.3.474. [DOI] [PubMed] [Google Scholar]
- Spielberger CD, Vagg PR, Barker LR, Donham GW, Westberry LG. The factor structure of the State-Trait Anxiety Inventory. In: Spielberger CD, Sarason IG, editors. Stress and anxiety. Vol. 7. Washington, DC: Hemisphere; 1980. pp. 95–109. [Google Scholar]
- Steele CM, Spencer SJ, Aronson J. Contending with group image: The psychology of stereotype and social identity threat. In: Zanna MP, editor. Advances in experimental social psychology. Vol. 34. San Diego, CA: Academic Press; 2002. pp. 379–440. [Google Scholar]
- Steiger JH. A note on multiple sample extensions of the RMSEA fit index. Structural Equation Modeling. 1998;5:411–419. [Google Scholar]
- Tomarken AJ, Waller NG. Potential problems with “well fitting” models. Journal of Abnormal Psychology. 2003;112:578–598. doi: 10.1037/0021-843X.112.4.578. [DOI] [PubMed] [Google Scholar]
- Treynor W, Gonzalez R, Nolen-Hoeksema S. Rumination reconsidered: A psychometric analysis. Cognitive Therapy and Research. 2003;27:247–259. [Google Scholar]
- Twenge JM, Crocker J. Race and self-esteem: Meta-analyses comparing Whites, Blacks, Hispanics, Asians, and American Indians and comment on Gray-Little and Hafdahl (2000) Psychological Bulletin. 2002;128:371–408. doi: 10.1037/0033-2909.128.3.371. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services. Rockville, MD: Author; 1999. Mental health: A report of the surgeon general. Retrieved April 1, 2009, from http://www.surgeongeneral.gov/library/mentalhealth/home.html. [Google Scholar]
- Wahl OF. Mental health consumers' experience of stigma. Schizophrenia Bulletin. 1999;25:467–478. doi: 10.1093/oxfordjournals.schbul.a033394. [DOI] [PubMed] [Google Scholar]
- Weissman MM, Sholomskas D, Pottenger M, Prusoff BA, Locke BZ. Assessing depressive symptoms in five psychiatric populations: A validation study. American Journal of Epidemiology. 1977;106:203–214. doi: 10.1093/oxfordjournals.aje.a112455. [DOI] [PubMed] [Google Scholar]
- Westbrook LE, Bauman LJ, Shinnar S. Applying stigma theory to epilepsy: A test of a conceptual model. Journal of Pediatric Psychology. 1992;17:633–649. doi: 10.1093/jpepsy/17.5.633. [DOI] [PubMed] [Google Scholar]
- Wight RG, Aneshensel CS, Murphy DA, Miller-Martinez D, Beals KP. Perceived HIV stigma in AIDS caregiving dyads. Social Science & Medicine. 2006;62:444–456. doi: 10.1016/j.socscimed.2005.06.004. [DOI] [PubMed] [Google Scholar]
- Williams DR, Neighbors HW, Jackson JS. Racial/ethnic discrimination and health: Findings from community studies. American Journal of Public Health. 2003;93:200–208. doi: 10.2105/ajph.93.2.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yip T, Seaton EK, Sellers RM. African American racial identity across the lifespan: Identity status, identity content, and depressive symptoms. Child Development. 2006;77:1504–1517. doi: 10.1111/j.1467-8624.2006.00950.x. [DOI] [PubMed] [Google Scholar]