

Abstract
Introduction
Fractures of the orbital-maxillo-zygomatic complex are among the most common fractures affecting the facial skeleton. Goal of surgical treatment is the realignment of fracture lines for a complete functional and aesthetic rehabilitation.
Materials and Methods
From January 2008 to January 2011 in the Department of Maxillofacial Surgery of Complesso Integrato Columbus of the Università Cattolica del Sacro Cuore in Rome, 25 patients, affected by comminute fractures of the anterior wall of the maxillary sinus associated with fractures of the orbital-maxillary complex were selected. The synthesis of the larger fracture fragments was performed by plates and screws (1.5 mm) while a biocompatible glue (N-Butyl-2-Cyanoacrylate–Glubran2®) was applied to treat the comminute fractures of the anterior wall of the maxillary sinus.
Results and Conclusion
The aim of our article is to report our experience and a review of the literature on application of–Butyl-2-Cyanoacrylate for treatment of comminute fractures of the anterior wall of the maxillary sinus. According to the results achieved in our study the N-Butyl-2-Cyanoacrylate can be indicated to treat comminuted fractures of the anterior wall of the maxillary sinus which could not easily be treated with internal rigid fixation.
Keywords: Orbital frsctures, Zygomatic fractures, Maxillary sinus fractures, N-Butyl-2-Cyanoacrylate, Maxillary sinus anterior wall fractures
Introduction
Fractures of the orbital-maxillo-zygomatic complex are among the most common fractures affecting the facial skeleton. Goal of surgical treatment is the realignment of fracture lines for a complete functional and aesthetic rehabilitation.
Currently titanium plates and screws ranging from 1 to 2 mm of width are considered the gold standard for osteo-synthesis of facial fractures. Thanks to the evolution of the techniques and surgical instruments, the surgeon is usually able to restore the anatomy of the skull, especially for the larger bone fragments [1].
However, frequently maxillofacial surgeons face the challenging condition of treating complex bone fractures of the facial skeleton, characterized by comminuted fragments of the anterior maxillary wall or the floor of the orbit; among the scientific-medical achievements, glues represent an important aid to treat such kind of fractures [2–4].
Biocompatible glues are already successfully used in cranio-facial surgery as hemostatic agents, embolic substances, to treat retinal tears, lacerations and corneal ulcers [5].
Among the synthetic glues, the N-Butyl-2-Cyanoacrylate (Glubran2®), might find interesting application in the treatment of comminute bone fractures due to its high adhesive, hemostatic properties, high biocompatibility and slow resorption without foreign body reaction [5, 6].
The aim of our article is to report our experience and a review of the literature on application of N-Butyl-2-Cyanoacrylate for treatment of fractures involving the maxillo-facial complex with a focus on the comminute fractures of the anterior wall of the maxillary sinus.
Materials and Methods
From January 2008 to January 2011, 100 patients were referred at our Department for orbital-maxillo-zygomatic complex, 25 of those were treated using Glubran2.
Of these 25 patients, 10 were women and 15 were men. The inclusion criteria of our study were:
Non-allergic patients,
Aged 18 to 35 years,
No immune system diseases,
Tripod and comminute fracture of the anterior wall of the maxillary sinus and displacement of fragments into the maxillary sinus.
All cases were treated by an open reduction of the fracture lines involving the malar bone to restore the anatomical entirety of the orbital contour (Fig. 1).
Fig. 1.

Pre-operative view of the patient and CT scan
A subciliary incision to approach the orbital floor and the lower orbital rim was performed in 9 cases. An incision under the eyelid was made in 13 cases. In 1 case, the access to the lower margin of the orbit and to the anterior wall of the maxillary sinus was performed under the eyelid through the traumatic wound. In all cases, a third lateral eyebrow incision to access the lateral side of the orbital cavity was carried out. The intraoral access (24 cases) and the trans-lesional incision localized under the eyelid (1 case) were made to access the anterior wall of the maxillary sinus.
The synthesis of the larger fracture fragments was performed by plates and screws (1.5 mm). We applied the glue, N-Butyl-2-Cyanoacrylate (Glubran2®), to treat the comminute fractures of the anterior wall of the maxillary sinus. This glue, applied in a humid environment, rapidly polymerizes and creates a thin film characterized by high strength; it ensures a solid adhesion of the tissues and an effective antiseptic barrier (Fig. 2).
Fig. 2.

Intraoperatory application of the biological glue
The glue comes ready to use and was applied through an insulin syringe. The glue begins to solidify after about 1–2 s and finishes its reaction after 60–90 s. At the end of this reaction, the glue reaches its maximum strength.
The N-Butyl-2-Cyanoacrylate was applied only after the reduction and the contention by plates and screws of the larger bone fragments. When the fractures involved the infraorbital foramen (3 cases), the glue was applied close to the infraorbital nerve.
The wounds were always sutured once the glue polymerization was completed.
Each patient underwent a CT scan examination of the maxillo-facial complex before surgery, right after surgical procedure to evaluate the correct alignment of the fragments and after 3 months.
Clinical assessment was performed at 6, 12, 18 months of follow up (Fig. 3).
Fig. 3.
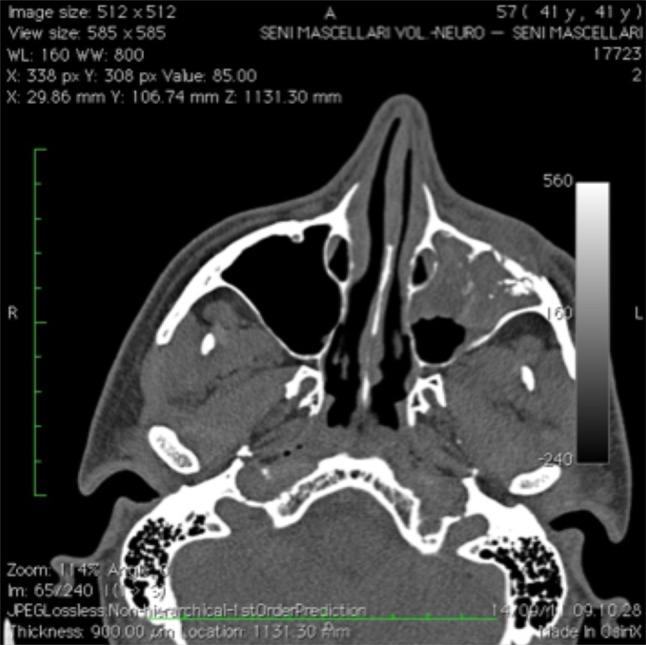
Post operative CT scan
Results
No case of infection or adverse reaction was reported.
Five patients reported hypoesthesia in the cutaneous regions innervated by the second branch of the trigeminal nerve.
However, over the next 6–12 months, the symptom completely disappeared in all patients.
The postoperative course showed no complications without delay on recovery time of the fracture. The N-Butyl-2-Cyanoacrylate proved a perfect contention, allowing the consolidation of small fragments of the anterior wall of the maxillary sinus. No cases of displacement of fragments neither cases of pseudoarthrosis were reported in our series.
Discussion
The maxillary sinus represents an important weak point of the maxillo-facial complex. Traumas, with an antero-posterior vector or with an angular direction from the bottom, can produce relevant bone fractures because of the maxillary sinus [6, 7]. Therefore, the traumatic energy radiates encountering very low resistance. This phenomenon explains the reason why the fractures of the anterior wall of the maxillary sinus are characterized by several comminuted fragments, often displaced into the maxillary sinus itself. The treatment of the fractures of the maxillary anterior wall is a challenge for the maxillo-facial surgeon. Periosteum of the fragments represents a pseudo-fixation that limits the displacement of the fragments into the cavity but prevents a good exposition and the correct repositioning of the fracture lines [1].
Currently, the contention is carried out through micro (1.0 mm width) and miniplates (1.5–2 mm width). However, for fractures characterized by small and comminute fragments, the rigid system is suboptimal, making the contention challenging. Isolated fractures of the anterior wall of the maxillary sinus do not usually require any treatment, because no significant muscular tensions or aesthetical sequelae would result. However exposure and reduction of comminute fracture of the anterior wall of maxilla may be taken into consideration when they are part of complex fractures, such as Le Fort fractures and zygomatic complex fractures.
The surgical glues must be biologically compatible, have quick action time and a suitable strength. Their action should last until the bone healing is completed.
Considering the lack of complication in this study and the simplicity of the technique, the use of glue can be advisable in those cases in which the fragments are too comminute for being fixed.
The application of surgical glues in orthopedics began in 1930, but it did not achieve satisfactory results. Allergic reactions, infections or pseudo-arthrosis were described [8, 9].
In literature, improvements of the physico-chemical properties of surgical glues are described [2]. Among glues, cyanoacrylates are the only ones used in medical field [7].
The Butyl-2-cyanoacrylate is the most commonly used surgical glue for contention of bone fractures [3, 8–10]. It is simple to use and tends to polymerize in the presence of humid environment [10]. Thanks to its alkyl chain, it produces minimal inflammatory response and can be applied between surfaces of the bone stumps; these features make it a precious aid in alignment and synthesis of comminuted fragment of the anterior wall of maxillary sinus in the context of complex maxillofacial fractures and has shown in our experience no evidence of leading to non-union or malunion.
The use of surgical glues significantly improves the correct alignment of the small and thin bone fragments whilst reduces intra-operative time.
However, in literature few studies are described on the use of cyanoacrylate for the treatment of facial fractures.
Wiecko et al. in 1980 [6] was the first to use the cyanoacrylate for the treatment of 4 cases of fracture of the anterior wall of the frontal sinus with satisfactory results. In 1987 Mehta et al. [7] used the Butyl-2-cyanoacrylate for 10 cases of mandibular fracture, describing a reduction in the recovery time of the fractures. Kim in 1997 [8] showed, however, his experience on the use of Butyl-2-cyanoacrylate to repair small bone fragments after facial trauma, in particular, for the anterior wall of the maxillary sinus, the floor and the roof of the orbit and the frontal sinus, with excellent results. These data were confirmed during our study.
Conclusion
The N-Butyl-2-Cyanoacrylate cannot replace the current continuative methods to fix the maxillary buttress in case of maxillofacial fractures. However, it can provide a useful support in the treatment of comminuted fractures, affecting thin bones not subjected to compression and traction forces, such as the anterior wall of the maxillary sinus, the roof and the floor of the orbital cavity.
Based on our experience, we indicate the use of the N-Butyl-2-Cyanoacrylate for comminuted fractures of the anterior wall of the maxillary sinus, involved in more complex fractures that require surgical treatment.
Conflict of interests
The authors declare they have no conflict of interests.
Footnotes
The study was performed according to the guidelines of the Declaration of Helsinky.
References
- 1.Iannetti G (1977) Chirurgia delle malformazioni e delle fratture maxillo-facciali. LXIV Congresso Nazionale S, Margherita Ligure
- 2.Gosain AK. Plastic Surgery Educational Foundation DATA Committee. The current status of tissue glues: i. for bone fixation. Plast Reconstr Surg. 2002;109:2581–2583. doi: 10.1097/00006534-200206000-00066. [DOI] [PubMed] [Google Scholar]
- 3.Gosain AK, et al. Biomechanical evaluation of titanium, biodegradable plate and screw, and cyanoacrylate glue fixation systems in craniofacial surgery. Plast Reconstr Surg. 1998;101:582. doi: 10.1097/00006534-199803000-00004. [DOI] [PubMed] [Google Scholar]
- 4.Weber SC, Chapman MW. Adhesives in orthopaedic surgery. Clin Orthop. 1984;191:249. [PubMed] [Google Scholar]
- 5.Shermak MA, et al. Fixation of the craniofacial skeleton with butyl-2-cyanoacrylate and its effects on histotoxicity and healing. Plast Reconstr Surg. 1998;102:309–318. doi: 10.1097/00006534-199808000-00003. [DOI] [PubMed] [Google Scholar]
- 6.Wiecko J, et al. Use of tissue adhesives in the reconstruction of the frontal sinus. Polim Med. 1980;10:165. [PubMed] [Google Scholar]
- 7.Mehta MJ, et al. Osteosynthesis of mandibular fractures with N-butyl cyanoacrylate: a pilot study. J Oral Maxillofac Surg. 1987;45:393. doi: 10.1016/0278-2391(87)90006-1. [DOI] [PubMed] [Google Scholar]
- 8.Kim YO (1997) Use of cyanoacrylate in facial bone fractures. J Craniofac Surg 8:229 [DOI] [PubMed]
- 9.Lamborn PB, Jr, et al. Comparison of tensile strength of wounds closed by sutures and cyanoacrylates. Am J Vet Res. 1970;31:125–130. [PubMed] [Google Scholar]
- 10.Shermak MA, et al. Butyl-2-cyanoacrylate fixation of mandibular osteotomies. Plast Reconstr Surg. 1998;102:319–324. doi: 10.1097/00006534-199808000-00004. [DOI] [PubMed] [Google Scholar]