

Abstract
Left ventricular aneurysms are a frequent complication of acute extensive myocardial infarction and are most commonly located at the ventricular apex. A timely diagnosis is vital due to the serious complications that can occur, including heart failure, thromboembolism, or tachyarrhythmias. We report the case of a 78-year-old male with history of previous anterior myocardial infarction and currently under evaluation by chronic heart failure. Transthoracic echocardiogram revealed a huge thrombosed and calcified anteroapical left ventricular aneurysm. Coronary angiography demonstrated that the left anterior descending artery was chronically occluded, and revealed a big and spherical mass with calcified borders in the left hemithorax. Left ventriculogram confirmed that this spherical mass was a giant calcified left ventricular aneurysm, causing very severe left ventricular systolic dysfunction. The patient underwent cardioverter-defibrillator implantation for primary prevention.
Keywords: Myocardial infarction, Echocardiography, Coronary artery disease, Left ventricular aneurysm, Coronary angiography
Core tip: Early diagnosis of ventricular aneurysms following acute transmural myocardial infarction is vital due to the serious complications that can occur. We report the case of a 78-year-old male with history of previous anterior myocardial infarction and currently under evaluation by chronic decompensated heart failure. Subsequent investigation revealed a huge thrombosed and calcified anteroapical left ventricular aneurysm. The peculiar findings of echocardiography, fluoroscopy and left ventriculography are shown with demonstrative images.
INTRODUCTION
True left ventricular aneurysms are a frequent complication following acute extensive myocardial infarction. Early diagnosis is crucial due to the serious complications that can potentially occur, including heart failure, thromboembolism, or tachyarrhythmias.
CASE REPORT
A 78-year-old male with history of previous anterior myocardial infarction and currently under evaluation by chronic decompensated heart failure (NYHA functional class III), underwent transthoracic echocardiogram revealing the presence of a huge and peripherally calcified anteroapical left ventricular aneurysm with a giant mural thrombus (Figures 1, 2, 3). Elective coronary angiography was performed which demonstrated that the left anterior descending artery was chronically occluded (Figure 4) and nonsignificant lesions in the other coronary arteries. Fluoroscopic imaging revealed a complete oval calcified image enclosed within an abnormal cardiac silhouette (Figure 5). Left ventriculogram confirmed that this image corresponded of a giant calcified and thrombosed left ventricular aneurysm, causing severe left ventricular systolic dysfunction (Figure 6). The calculated left ventricular ejection fraction was only 7%. The patient underwent cardioverter-defibrillator implantation for primary prevention.
Figure 1.
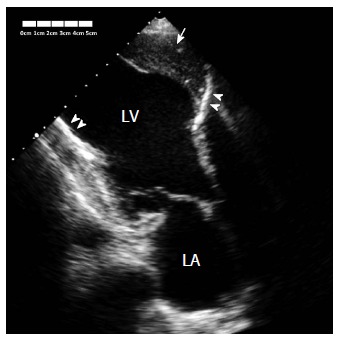
Transthoracic echocardiogram using apical three chamber view showing the big anterior left ventricular aneurysm (arrow). The wall of the aneurysm was calcified (arrowheads), and the aneurysm was covered with thrombus (arrow). LA: Left atrium; LV: Left ventricle.
Figure 2.
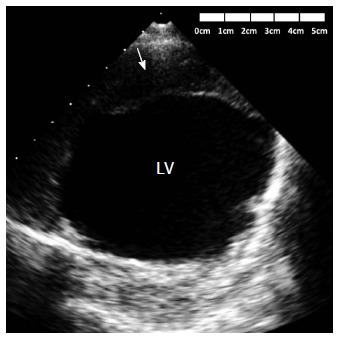
Transthoracic echocardiogram using parasternal short axis view at the midventricular level showing the thrombus (arrow) covering the anterior wall aneurysm. LV: Left ventricle.
Figure 3.
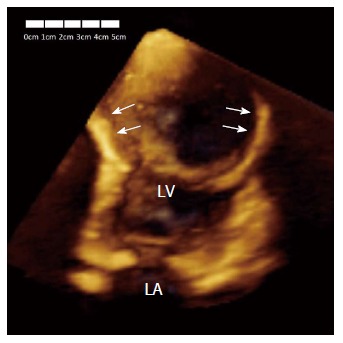
Three-dimensional echocardiography in apical four chamber view showing the big size of the aneurysm (arrows). LA: Left atrium; LV: Left ventricle.
Figure 4.
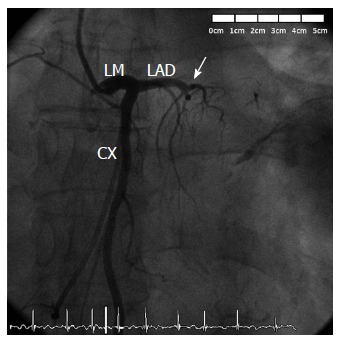
Left coronary angiography demonstrating a proximal occlusion of the left anterior descending artery (arrow). CX: Circumflex coronary artery; LAD: Left anterior descending coronary; LM: Left main coronary artery.
Figure 5.
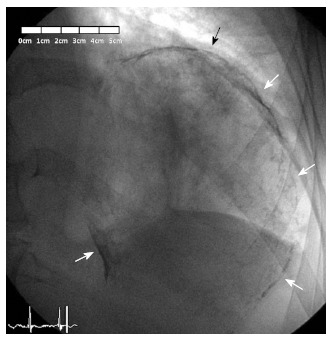
Fluoroscopic imaging in right anterior oblique projection showing a complete oval calcified mass (arrows), corresponding with the left ventricular aneurysm.
Figure 6.
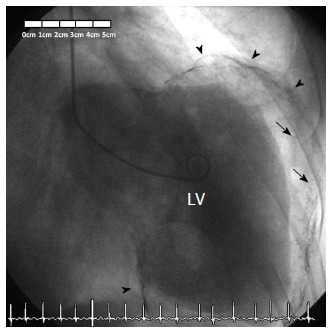
Left ventriculogram confirming diagnosis of a giant calcified and partially thrombosed left ventricular aneurysm, with severe left ventricular systolic dysfunction. The wall of the aneurysm is calcified (arrowheads), and the aneurysm is covered with thrombus (arrows). LV: Left ventricle.
DISCUSSION
Left ventricular aneurysms are a frequent complication of acute extensive myocardial infarction and are most commonly located at the ventricular apex[1,2]. A timely diagnosis is vital due to the serious complications that can occur, including heart failure, thromboembolism, or tachyarrhythmias. The benefits of surgical repair of left ventricular aneurysm have long been debated. Although a large amount of studies have showed that aneurysmectomy might improve the outcome[3], the results from the STICH trial have questioned the benefit of this treatment[4]. Therefore, indication for aneurysmectomy depends on the decision of individual surgeons, and should be based on the assessment of the left ventricular dimensions, mitral valve regurgitation severity, extent of myocardial scar tissue and viability of the other regions of the left ventricle, and surgery should be performed in centers with a high surgical experience.
COMMENTS
Case characteristics
A 78-year-old male with history of previous anterior myocardial infarction and currently under evaluation by chronic decompensated heart failure.
Clinical diagnosis
Giant thrombosed left ventricular aneurysm.
Differential diagnosis
Intrathoracic mass.
Imaging diagnosis
Echocardiography and coronary angiography were used for the diagnosis of left ventricular aneurysm.
Treatment
The patient received an implantable cardioverter-defibrillator for primary prevention and was referred for consideration of cardiac transplantation.
Related reports
True left ventricular aneurysms are widely recognized as a common and serious complication following acute transmural myocardial infarction. However, this case is particular because of the huge size of the aneurysm.
Experiences and lessons
The recognition of ventricular aneurysms is of great importance due to the numerous complications that can potentially occur. Echocardiography and catheterism are fundamental tests for diagnosis.
Peer-review
It is a interesting case and well described.
Footnotes
Institutional review board statement: The case report was reviewed and approved by the Hospital Clinico San Carlos Institutional Review Board.
Informed consent statement: The patient provided informed written consent to publish the case report.
Conflict-of-interest statement: There is no conflict of interest concerning this manuscript.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: March 7, 2015
First decision: March 20, 2015
Article in press: April 30, 2015
P- Reviewer: Bagur R, Cebi N, Lee TS S- Editor: Ji FF L- Editor: A E- Editor: Wang CH
References
- 1.Tikiz H, Atak R, Balbay Y, Genç Y, Kütük E. Left ventricular aneurysm formation after anterior myocardial infarction: clinical and angiographic determinants in 809 patients. Int J Cardiol. 2002;82:7–14; discussion 14-16. doi: 10.1016/s0167-5273(01)00598-8. [DOI] [PubMed] [Google Scholar]
- 2.Abrams DL, Edelist A, Luria MH, Miller AJ. Ventricular aneurysm. a reappraisal based on a study of sixty-five consecutive autopsied cases. Circulation. 1963;27:164–169. doi: 10.1161/01.cir.27.2.164. [DOI] [PubMed] [Google Scholar]
- 3.Castelvecchio S, Menicanti L, Donato MD. Surgical ventricular restoration to reverse left ventricular remodeling. Curr Cardiol Rev. 2010;6:15–23. doi: 10.2174/157340310790231626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jones RH, Velazquez EJ, Michler RE, Sopko G, Oh JK, O’Connor CM, Hill JA, Menicanti L, Sadowski Z, Desvigne-Nickens P, et al. Coronary bypass surgery with or without surgical ventricular reconstruction. N Engl J Med. 2009;360:1705–1717. doi: 10.1056/NEJMoa0900559. [DOI] [PMC free article] [PubMed] [Google Scholar]