

Abstract
Hemiarthroplasty of the hip is a commonly performed procedure for subcapital neck of femur fractures. Dislocation of the hemiarthroplasty is a recognised but uncommon complication. Dislocations can be complicated by the uncoupling or dissociation of the femoral head component from the femoral stem. Dissociations are rare and require open reduction. We present a case of a patient with a hip hemiarthroplasty dislocation and dissociation subsequent to a fall.
Background
Hemiarthroplasty of the hip for subcapital neck of femur fractures is a commonly performed procedure. Dislocation of the hemiarthroplasty is an uncommon complication with a reported incidence of between 1.2% and 3.4%.1 2 Dissociation of a hemiarthroplasty where the femoral stem and femoral head components separate is a rare complication.
Case presentation
A 71-year-old woman with an unsteady gait presented to the emergency department with right hip pain subsequent to a simple fall from standing height. Radiographs demonstrated a subcapital neck of femur fracture, for which she underwent a hip hemiarthroplasty (figure 1) (Charnley round back femoral component and Hastings femoral head component). The patient had multiple medical comorbidities, including mild vascular dementia, necessitating a prolonged postoperative admission. She had a subsequent fall 4 weeks following her hemiarthroplasty causing significant pain and an inability to weight bear on the right side. On examination of the patient, it was noted that the right lower limb was shortened and externally rotated, raising concern for a dislocation. A radiograph of the pelvis showed a dislocation of the hemiarthroplasty with proximal migration. It was also noted that the femoral head component and femoral stem component were not concentric, raising suspicion of dissociation (figure 2).
Figure 1.
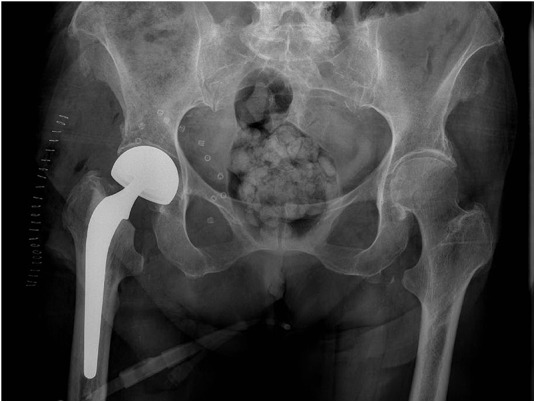
Anteroposterior radiograph of the right hip demonstrating a satisfactory hip hemiarthroplasty subsequent to a subcapital neck of femur fracture.
Figure 2.
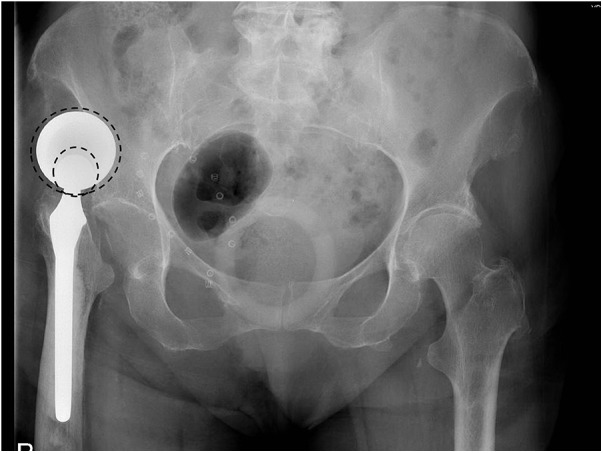
Anteroposterior radiograph of the right hip demonstrating a dislocation of right hip hemiarthroplasty. The femoral head component and the stem do not appear concentric (dotted circles) raising suspicion for a dissociation of the implants.
Treatment
The patient was taken to the operating room where the dissociation of the hemiarthroplasty was confirmed by screening with an image intensifier (figure 3). The patient underwent a revision hemiarthroplasty under spinal anaesthesia.
Figure 3.
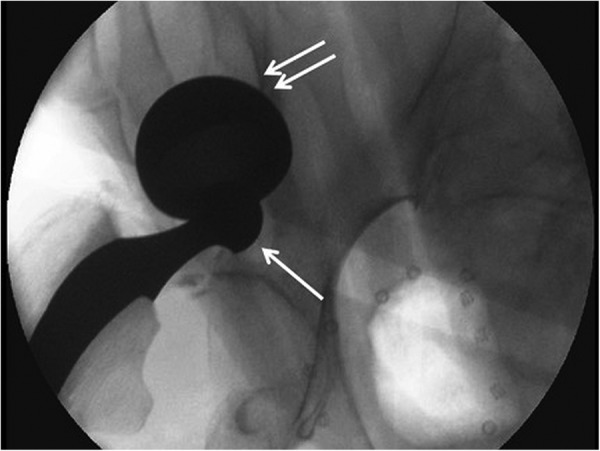
A fluoroscopic pre operative image demonstrating uncoupling or dissociation of the hemiarthroplasty implants.
Intraoperative assessment discovered significant disruption to the previous capsule and abductor repair. There was no fracture of the acetabulum seen and the femoral component was found to be well fixed. The femoral head component was replaced with another Hastings implant of the same size. The hip was reduced and confirmed to be stable through its full range of motion. The abductors were carefully repaired in layers and reinforced proximally with suture anchors. Postoperative radiographs (figure 4) were satisfactory and recovery was uneventful. The patient was mobilised within 48 h of surgery.
Figure 4.
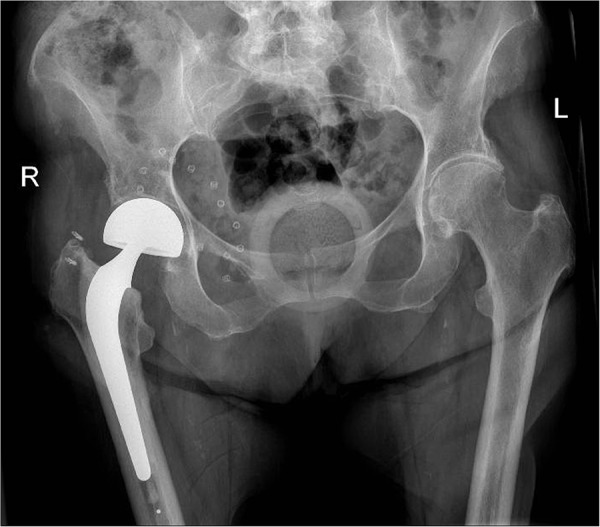
Postoperative radiograph demonstrating the revision hip hemiarthroplasty.
Outcome and follow-up
Three years postoperatively, the patient remains pain free and has had no further episodes of dislocation despite multiple falls due to her unsteady gait. She remains able to ambulate short distances with a frame.
Discussion
Dislocation of a hemiarthroplasty is uncommon and has a reported overall rate of approximately 3.4%.1 2 There is no significant difference in the complication rates between unipolar and bipolar hip hemiarthroplasty.3 4 Dissociation of the hemiarthroplasty is a rare complication with the largest case-series to date having only five cases.5 When dissociated, the femoral head component most commonly remains within the acetabulum or in close proximity. In our case, the femoral head component was completely out of the acetabulum and had migrated proximally.
It is believed that the most common mechanism of dissociation involves the femoral head component locking against the acetabular rim during dislocation.5 Improper implant size or position, excessive wear of polyethylene liner and failure of the locking ring mechanism, can all contribute to dissociation above.5–7 Dissociation as a complication of an attempted closed reduction of a dislocated hemiarthroplasty has also been reported where the femoral head component impinges on the posterior wall resulting in a ‘bottle-opener’ effect during traction.8–10 Closed reduction should only be attempted in theatre with an image intensifier, which allows for conversion to an open reduction if necessary.
A dislocated hip hemiarthroplasty should be initially imaged to ensure there are no impediments to closed reduction, which includes dissociation. The management of a dissociated hemiarthroplasty is open reduction. Previous radiographs should be assessed to identify any implant malalignment that may predispose to dislocation. Intraoperatively, the acetabulum should be inspected for any fractures or defects and the femoral stem should be assessed for loosening and correct version. As our patient had a well-fixed stem in good alignment, only the Hastings femoral head component was replaced. In order to achieve stability, one should be prepared to revise all components of the hemiarthroplasty to prevent further dislocations.
Learning points.
Dislocation of hip hemiarthroplasties are uncommon and dissociations rare.
A dissociation may occur due to inadequate implant size or position, excessive wear of polyethylene liner, failure of the locking ring mechanism or as a complication of an attempted closed reduction of a dislocated hemiarthroplasty.
Hip hemiarthroplasty dislocations should be screened in theatre to rule out a dissociation and prevent a dissociation during closed reduction. Dissociations are managed with open reduction and may require revision of all components of the hemiarthroplasty.
Footnotes
Contributors: The patient's details and images were gathered by AM and ST. The literature review was completed by AM and PE. The patient was treated by J McKenna.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Sierra RJ, Schleck CD, Cabanela ME. Dislocation of bipolar hemiarthroplasty: rate, contributing factors, and outcome. Clin Orthop Relat Res 2006;442:230–8. 10.1097/01.blo.0000183741.96610.c3 [DOI] [PubMed] [Google Scholar]
- 2.Varley J, Parker MJ. Stability of hip hemiarthroplasties. Int Orthop 2004;28:274–7. 10.1007/s00264-004-0572-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Raia FJ, Chapman CB, Herrera MF et al. Unipolar or bipolar hemiarthroplasty for femoral neck fractures in the elderly? Clin Orthop Relat Res 2003;414:259–65. 10.1097/01.blo.0000081938.75404.09 [DOI] [PubMed] [Google Scholar]
- 4.Ong BC, Maurer SG, Aharonoff GB et al. Unipolar versus bipolar hemiarthroplasty: functional outcome after femoral neck fracture at a minimum of thirty-six months of follow-up. J Orthop Trauma 2002;16:317–22. 10.1097/00005131-200205000-00005 [DOI] [PubMed] [Google Scholar]
- 5.Georgiou G, Siapkara A, Dimitrakopoulou A et al. Dissociation of bipolar hemiarthroplasty of the hip after dislocation. A report of five different cases and review of literature. Injury 2006;37:162–8. 10.1016/j.injury.2005.09.014 [DOI] [PubMed] [Google Scholar]
- 6.Corteel J, Putz P. [Dislocation-dissociation of a bipolar hip prosthesis]. Acta Orthop Belg 1996;62:173–6. [PubMed] [Google Scholar]
- 7.Loubignac F, Boissier F. [Cup dissociation after reduction of a dislocated hip hemiarthroplasty]. Rev Chir Orthop Reparatrice Appar Mot 1997;84:469–72. [PubMed] [Google Scholar]
- 8.Grauke LJ, Richardson ML. Dissociation of a bipolar prosthesis after right hip hemiarthroplasty. Case Rep Radiol 2006;1:123–5. 10.2484/rcr.v1i4.55 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Star MJ, Colwell CW, Donaldson WF et al. Dissociation of modular hip arthroplasty components after dislocation. A report of three cases at different dissociation levels. Clin Orthop 1992;278:111–15. [PubMed] [Google Scholar]
- 10.Tabutin J, Damotte A. [Progressive intra-acetabular dislocation of bipolar hip prostheses: four cases]. Rev Chir Orthop Reparatrice Appar Mot 2004;90:79–82. 10.1016/S0035-1040(04)70011-2 [DOI] [PubMed] [Google Scholar]