

Description
A 4-month-old Dominican girl was born prematurely with numerous malformations (figures 1–4) including facial asymmetry, low-implanted left ear, short neck, short trunk, barrel chest, a left preaxillary thoracic depression, thoracolumbar scoliosis and an enormous lumbosacral meningocele. Family history was non-contributory and prenatal maternal folate supplementation was adequate. On examination, the alert and playful normocephalic infant had an opisthotonos-positioned head and diminished leg movements, without bladder or bowel dysfunction. A CT of the head was clear (figure 3B), and normal developmental milestones were met. Roentgenography (figure 2A) revealed costovertebral abnormalities unique to Jarcho-Levin syndrome (JLS), confirmed on three-dimensional CT reconstruction (figure 2B). Subsequently, close respiratory surveillance and chest physiotherapy was initiated, and the meningocele was repaired surgically in the usual fashion (figure 4). Intraoperatively, a myelomeningocele was definitively ruled out as no nerve roots were contained within the herniation. However, nerve roots were found to be adhered to the neck of the sac internally. We theorise that this finding, in addition to arachnoid septations, were responsible for the lower extremity weakness. The infant had an uneventful postoperative course, with an improved neurological examination and stable condition at 6-month follow-up. Specifically, our patient exhibited a greater degree of spontaneous active movement of her lower extremities. In addition, she demonstrated increased strength against resistance of the muscles innervated by L5-S1 by means of plantar and dorsiflexion as well as hallux extension, especially during stimulation of Babinski reflex.
Figure 1.

Patient's phenotype and marked thoracic depression (arrowheads).
Figure 2.
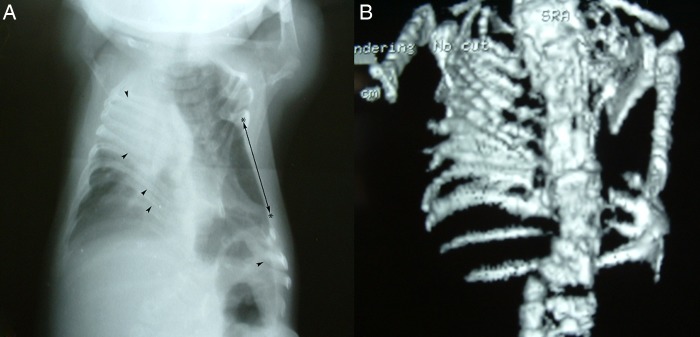
(A) Chest X-ray depicting ribs fanning out from their costovertebral joints (‘fan-like’ or ‘crab-like’ appearance) and a shortened spine with left lumbosacral scoliosis, altogether resulting in posterior rib fusions (arrowheads). A prominent intercostal hollow (*←→*) is seen, along with abnormal vertebral segmentation defects (‘pebble beach sign’) at the corresponding spinal segments. These findings characterise the spondylothoracic dysplasia subtype of JLS; notice the absence of intrinsic rib abnormalities (ie, aberrant rib count, bifurcations, thickenings, or more anteriorly located costal fusions). (B) Three-dimensional CT reconstruction of the same patient. JLS, Jarcho-Levin syndrome.
Figure 3.
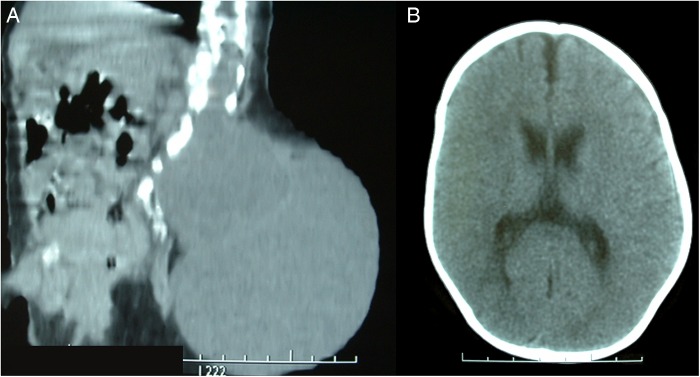
(A) Sagittal CT reconstruction defining contiguous left laminae defects and a large lumbosacral meningocele. Arachnoidal septations are seen within the meningocele's sac. (B) Head CT is normal in most cases of JLS, but should be performed to rule out other congenital syndromes. JLS, Jarcho-Levin syndrome.
Figure 4.

Upper: Preoperative photograph of the left-sided meningocele with fragile superficial vessels. Lower: Postoperative photograph of the final skin closure.
In 1938, Jarcho and Levin1 described this rare autosomal recessive syndrome of short-trunk dwarfism and respiratory insufficiency resulting from segmental costovertebral malformations. Mutations in the genes DLL3 and MESP2 on chromosomes 19 and 15, respectively, are the most commonly implicated.2 More recently, two clinical subtypes have been recognised: spondylocostal dysplasias (SCD, characterised by intrinsic rib abnormalities) and spondylothoracic dysplasias (STD, or Lavy-Moseley syndrome).3 4 Simple karyotype could be normal in these individuals. Genetic testing can be performed for mutations in DLL3, MESP2, LFNG and HES7. However, the initial diagnosis is radiological. Although rare, 17 cases of associated neural tube defects have been reported in JLS. Most frequently, these are split cord malformations5–8 and myelomeningoceles,5 9 10 usually located at rostral thoracolumbar segments. These segments correspond to levels where the more severe vertebral segmentation defects occur, suggesting either causation or a shared embryological origin. Thus, cases of caudal meningocele, which must separate from severely deformed vertebrae, are extremely uncommon. Unfortunately, the flawed thoracic anatomy inherent to JLS, particularly the STD-subtype, causes serious respiratory insufficiency, anaesthetic complications, pneumonia and early death. This often precludes or pre-empts the neurosurgical repair of associated defects. We demonstrate the successful management of an unusual case of STD with an associated large lumbosacral meningocele.
Learning points.
Patients with neural tube defects should be comprehensively evaluated for other associated congenital malformations.
The coexistence of congenital costovertebral malformations, such as in Jarcho-Levin syndrome (JLS), alters management decision-making. In these patients, an early initiation of aggressive respiratory support and chest physiotherapy (the mainstay managements of JLS) can be lifesaving and allows the safe surgical correction of associated malformations. An expansion thoracoplasty, however, is often required in severely compromised patients.
The presence of intrinsic rib abnormalities, which include an aberrant rib count, bifurcations, thickening, or more anteriorly located costal fusions, help distinguish the spondylocostal dysplasia-subtype from the severest form: the spondylothoracic dysplasia-subtype.
Footnotes
Contributors: JLMS and SF contributed to the conception and design of this study. JLMS drafted the manuscript, and JLMS and AAD revised it critically and made corrections. JLMS, AAD and SF approved the final version.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Jarcho S, Levin PM. Hereditary malformation of the vertebral bodies. Bull John Hopkins Hosp 1938;62:216–26. [Google Scholar]
- 2.Turnpenny PD, Young E. Icvas. Spondylocostal Dysostosis, Autosomal Recessive. In: Pagon RA, Adam MP, Ardinger HH et al., eds. GeneReviews(R). Seattle, WA: University of Washington, Seattle; All rights reserved, 1993. [Google Scholar]
- 3.Lavy NW, Palmer CG, Merritt AD. A syndrome of bizarre vertebral anomalies. J Pediatr 1966;69:1121–5. 10.1016/S0022-3476(66)80304-9 [DOI] [PubMed] [Google Scholar]
- 4.Moseley JE, Bonforte RJ. Spondylothoracic dysplasia—a syndrome of congenital anomalies. AJR 1969;106:166–9. 10.2214/ajr.106.1.166 [DOI] [PubMed] [Google Scholar]
- 5.Giacoia GP, Say B. Spondylocostal dysplasia and neural tube defects. J Med Genet 1991;28:51–3. 10.1136/jmg.28.1.51 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Reyes MG, Morales A, Harris V et al. Neural defects in Jarcho-Levin syndrome. J Child Neurol 1989;4:51–4. 10.1177/088307388900400109 [DOI] [PubMed] [Google Scholar]
- 7.Kansal R, Mahore A, Kukreja S. Jarcho-Levin syndrome with diastematomyelia: a case report and review of literature. J Pediatr Neurosci 2011;6:141–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kutuk MS, Ozgun MT, Tas M et al. Prenatal diagnosis of split cord malformation by ultrasound and fetal magnetic resonance imaging: case report and review of the literature. Childs Nerv Syst 2012;28:2169–72. 10.1007/s00381-012-1900-z [DOI] [PubMed] [Google Scholar]
- 9.Duru S, Ceylan S, Guvenc BH. Segmental costovertebral malformations: association with neural tube defects. Report of 3 cases and review of the literature. Pediatr Neurosurg 1999;30:272–7. 10.1159/000028810 [DOI] [PubMed] [Google Scholar]
- 10.Yi S, Yoon DH, Shin HC et al. A thoracic myelomeningocele in a patient with spondylocostal dysostosis. Case report. J Neurosurg 2006;104(1 Suppl):37–40. [DOI] [PubMed] [Google Scholar]