

Abstract
Background:
The aim of the study was to evaluate, in vitro, the surface roughness of two composite resins submitted to simulated toothbrushing with three different dentifrices.
Materials and Methods:
Totally, 36 samples of Z350XT and 36 samples of Empress Direct were built and randomly divided into three groups (n = 12) according to the dentifrice used (Oral-B Pro-Health Whitening [OBW], Colgate Sensitive Pro-Relief [CS], Colgate Total Clean Mint 12 [CT12]). The samples were submitted to 5,000, 10,000 or 20,000 cycles of simulated toothbrushing. After each simulated period, the surface roughness of the samples was measured using a roughness tester.
Results:
According to three-way analysis of variance, dentifrice (P = 0.044) and brushing time (P = 0.000) were significant. The composite resin was not significant (P = 0.381) and the interaction among the factors was not significant (P > 0.05). The mean values of the surface roughness (µm) followed by the same letter represent no statistical difference by Tukey's post-hoc test (P <0.05): Dentifrice: CT12 = 0.269a; CS Pro- Relief = 0.300ab; OBW = 0.390b. Brushing time: Baseline = 0,046ª; 5,000 cycles = 0.297b; 10,000 cycles = 0.354b; 20,000 cycles = 0.584c.
Conclusion:
Z350 XT and Empress Direct presented similar surface roughness after all cycles of simulated toothbrushing. The higher the brushing time, the higher the surface roughness of composite resins. The dentifrice OBW caused a higher surface roughness in both composite resins.
Keywords: Composite resins, dentifrices, tooth abrasion, toothbrushing
Introduction
Dentifrices have been a source of concern and subject of study for many professionals, since it is one of the main resources used in daily oral care by the population. Dentifrices have different components, such as detergents, fluoride, therapeutic ingredients, flavors, and abrasives. Among the abrasives, the most common are calcium carbonate and silica.1 These abrasives have an important role in cleaning teeth, removing bacteria and stains from the tooth surface. However, the dentifrice should promote optimal tooth surface cleaning with minimal abrasion,2 since dentifrices with high amounts of abrasives can damage hard tissue, soft tissue and restorations, causing gingival recession, cervical abrasion, and dentin hypersensitivity.3,4
Currently, patients increasingly value esthetic and seek simplified and safe results for their oral problems.5 Thus, the composite resins have been widely used in restorative treatments. However, it should be considered that the success and longevity of these restorations are related to the material, the dentist, and the patient.6 The patients are responsible to care for their dietary habits, preventive measures, availability of fluoride, and oral hygiene since carious lesions have been the most common cause of direct composite resin restorations replacements.7
Studies have been conducted to evaluate the surface roughness of composite resins caused by the abrasivity of some dentifrices. Amaral et al.8 evaluated the action of abrasive dentifrices on esthetic restorative materials after simulated toothbrushing cycles. The researchers found a significant difference between the abrasivity of dentifrices, but not among the composite resins. The dentifrices that used silica and carbonate were less abrasive compared to the ones containing bicarbonate. Liljeborg et al.9 assessed the acrylic surface roughness caused by different values of relative dentin abrasivity (RDA), which is the abrasivity characteristic of dentifrices provided by the manufacturer. In this study, an association was analyzed between the value of RDA, provided by the manufacturer, with the surface roughness (Ra) found for each dentifrice after simulated toothbrushing. Surprisingly, the correlation between RDA and Ra value was too low. Dentifrice with low RDA (40) showed higher Ra (5.73 µm), while the other with high RDA (130) obtained Ra of 1.84 µm; a third dentifrice with the lowest value of RDA (30) showed a Ra value of 1.13 µm.
A large supply of new dentifrices has been available on the market nowadays, which makes the choice more difficult for patients. Furthermore, the speed of production has surpassed independent studies without ties to manufacturers.10
Concerned about the integrity of composite resin restorations from the abrasivity of dentifrices available, this study aims to answer the following questions: (a) does toothbrushing with dentifrice change the surface roughness of composite resins? (b) is the surface roughness the same, regardless of the type of dentifrice or composite resin evaluated? Therefore, the aim of the study was to evaluate, in vitro, the surface roughness of two composite resins submitted to simulated toothbrushing with three different dentifrices in periods of 6 months, 1 year, and 2 years. The null hypothesis is that toothbrushing with dentifrices does not influence the surface roughness of composite resins.
Materials and Methods
Selection of composite resin specimens
The composite resins Empress Direct (Ivoclar Vivadent, Schaan, Liechtenstein) and Z350 XT (3M/ESPE, St. Paul, MN, USA), enamel shade A1, were selected. The specifications of each composite resin brand are described in Table 1.
Table 1.
Specifications and manufacturer of composite resins.

The composite resin specimens were made using a silicone matrix with orifices of 5 mm in diameter and height. The matrix was positioned on a glass plate and filled with composite resin. A polyester strip was then placed on the composite resin followed by a glass plate in order to obtain a flat surface. The composite resin was then light-cured with the light-emitting diode light unit Radii-cal (SDI, Australia) for 20 s at a distance of 1 mm from the surface of the specimen. The composite resin surface in contact with the polyester strip received the toothbrushing with dentifrices. For each composite resin, 36 specimens where fabricated and stored in distilled water at 37°C for 24 h to complete the polymerization and simulate conditions of the oral cavity environment.
Experimental groups
The 36 specimens of each composite resin were randomly divided into three groups (n = 12). Each group was subject to simulated toothbrushing with three different dentifrices: Oral-B Pro-Health Whitening (OBW), Colgate Sensitive (CS) Pro-Relief, Colgate Total Clean Mint 12 (CT12). The dentifrice CT12 was considered the control group. The composition of each dentifrice is shown in Table 2.
Table 2.
Composition and manufacturer of dentifrices tested.
Analysis of surface roughness
The initial surface roughness of each specimen was measured with a roughness tester SL-201 (Mitutoyo Surftest Analyzer, Tokyo, Japan). Three consecutive measurements of the specimen were taken in different regions (one central, one right, and one left), with cut-off of 0.25, obtaining the mean average from the three measurements.
Simulated toothbrushing
The simulated toothbrushing machine developed by Idea Institute of PUCRS was used for this study. Each specimen was fixed in the center (orifice) of an acrylic plate (55 mm × 25 mm × 4 mm), respectively for the diameter and height, enabling the test surface to remain 1 mm beyond the edge of the orifice, which housed the specimen. Utility wax was applied to fix the specimens. Each plate was placed in an acrylic tank, which was attached to the brushing machine by metal pins. The acrylic tank was filled with a mixture composed of 1 g of dentifrice paste per 1 ml of distilled water. Soft bristle Classic Colgate (Colgate-Palmolive, São Bernardo do Campo, SP, Brazil) toothbrushes were used, with a load of 200 g. The speed of brushing was 250 cycles per minute, carried out in 5,000 cycles, 10,000 cycles, and 20,000 cycles of simulated toothbrushing, cumulatively, that corresponds to approximately 6 months, 12 months, and 24 months of brushing,11 respectively. The dentifrice pastes and toothbrushes were changed every cycle.
After every brushing cycle, the specimens were washed in running water and ultrasonically cleaned in distilled water for 10 min, followed by drying with compressed air. The roughness of the surface was measured again.
The surface roughness reading was perpendicular to the brushing direction of the toothbrush bristles. For the correct positioning of the specimen in the brushing machine and to always ensure readability in the same direction (perpendicular to the brushing), a mark with a diamond bur and high-speed handpiece was made on the border of each specimen.
Analysis by scanning electron microscopy (SEM)
From each of the composite resins, 12 additional specimens were obtained, as previously described. The 12 specimens were randomly divided into three groups (n = 4), each group being subjected to the simulated toothbrushing with dentifrice as described above. Of the four samples, one was analyzed by SEM before simulated toothbrushing, the second after 5,000 cycles, the third after 10,000 cycles, and the fourth after 20,000 cycles of simulated toothbrushing. The specimens were dried in dehumidifier with silica gel for 72 h, metallized with gold (Balzers, Liechtenstein) and observed under a scanning electron microscope (JSM 6060, Eindhoven, Netherlands) at ×4,000 magnification for qualitative analysis of the surface.
Statistical analysis
The values of surface roughness were submitted to the Kolmogorov-Smirnov normality test. Three-way analysis of variance (ANOVA) was used to test the effect of composite resin, dentifrice, and brushing time on the surface roughness, followed by Tukey's test at a significance level of 5%.
Results
Three-way ANOVA analysis showed that the dentifrice (P = 0.044) and the brushing time (P = 0.000) had a significant effect on the surface roughness. The composite resin was not significant (P = 0.381) and the interaction among the factors was not significant (P > 0.05).
CT12 had the lowest surface roughness mean (0.269 µm), which was not significantly different from CS (0.300 µm). The highest surface roughness mean was obtained with OBW (0.390 µm), which was not significantly different from the CS (Table 3).
Table 3.
Surface roughness mean value (µm) of different dentifrices.
The highest surface roughness mean was obtained after 20,000 brushing cycles (0.584 µm), differing statistically from the other cycles. The 5,000 cycles (0.297 µm) and 10,000 cycles (0.354 µm) had no statistical difference. The lowest surface roughness mean was obtained for the measurement performed at baseline (0.046 µm), differing statistically from the other cycles (Table 4).
Table 4.
Surface roughness mean (µm) according to the brushing time.
Analysis by SEM
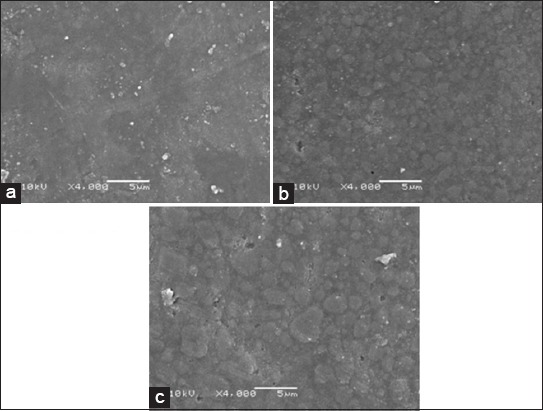
The SEM images of Figure 1a-d correspond to the Z350 XT composite resin. There was substantial surface smoothness of the composite resin (Figure 1a) before toothbrushing. After 5,000 cycles of brushing, dentifrice OBW (Figure 1d) caused significant surface roughness of the composite resin compared to dentifrice CT12 (Figure 1b) and CS (Figure 1c).
Figure 1.
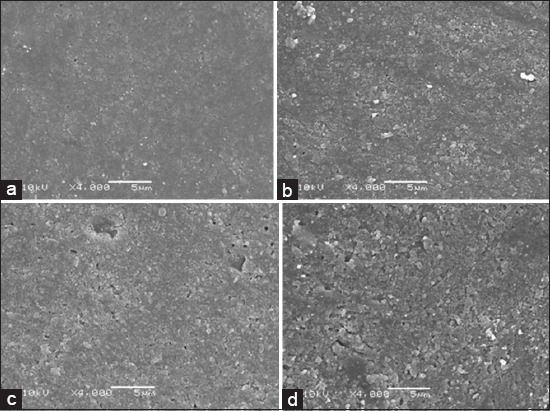
(a-d) Surface morphology of composite resin Z350 XT after 5,000 cycles of simulated toothbrushing (×4,000) (a) 0 cycles; (b) abrasion with Colgate Total 12 Clean Mint; (c) abrasion with Colgate Sensitive Pro-Relief; (d) abrasion with Oral B Pro-Health Whitening.
Figure 2 corresponds to Empress Direct composite resin. The increasing number of brushing cycles caused a higher removal of the resin matrix and thus greater exposure of the filler particles.
Figure 2.
Surface morphology of composite resin Empress Direct after simulated toothbrushing abrasion with Colgate Total 12 Clean Mint (×4,000) (a) 0 cycle; (b) 5,000 cycles; (c) 10,000 cycles.
Discussion
The clinical wear of a restoration may result from numerous factors, such as functional and centric contacts, attrition of the food bolus, and areas of interproximal contact. The toothbrush abrasion, however, has been an important phenomenon in regards to wear of composite resins, which is most commonly seen on the buccal surface.12 Hence, the marketing of various dentifrices, the abrasivity of three different dentifrices was evaluated in this study: CT12, containing silica; CS Pro-Relief, composed of calcium carbonate and bicarbonate; OBW, based on silica and titanium dioxide.
The dentifrice factor was significant and directly influenced the surface roughness results, rejecting the null hypothesis. This finding concurs with other studies that found that the action of toothbrushing associated with the use of abrasive dentifrices has been responsible for an increase on surface roughness of composite resins.8,13-18
The lowest surface roughness mean was obtained with the dentifrice CT12 (0.269 µm), confirming Barbieri et al.18 study that the same dentifrice was responsible for a low abrasion of composite resins analyzed. The CT12 contains silica as an abrasive agent that exhibits low abrasivity.1 Amaral et al.8 study concluded that dentifrices based on silica or calcium carbonate are less abrasive than those containing sodium bicarbonate. This possibly justifies the fact that the dentifrice CS, which has bicarbonate in the composition, caused a higher surface roughness compared to CT12, although no statistical difference was found.
The dentifrice OBW showed the highest Ra (0.390 µm) mean, different from CT12. This result corroborates the findings of Amaral et al.8 and Barbieri et al.18, in which the whitening dentifrices also results in higher surface roughness both containing silica abrasives in combination with other agents. The study of Menezes et al.4 found a significant difference in Ra caused by whitening dentifrices on bovine root dentin, stating that the change of Ra depends on the dentifrice used.
According to Cury et al.1 there are dentifrices with low, medium, and high abrasivity. Among the lower abrasivity are the dentifrices in the form of gel, containing silica as the abrasive agent. However, when this mineral is combined with other abrasives such as calcium carbonate, sodium pyrophosphate, titanium oxide, and sodium phosphate, it is considered a high abrasive dentifrice. This finding is consistent with the results of this study, in which the dentifrice OBW, responsible for a statistically significant abrasivity, has silica as an abrasive agent in combination with titanium dioxide, classifying it as a highly abrasive dentifrice.1
According to Gusmão et al.,19 the main cause factor of abrasivity is not limited to the type nor quantity of abrasive present in the dentifrice, but the physical characteristics of the mineral as the size and the shape of the particles. Silica, for example, when used in fine particles with regular shapes, preserves its mild abrasivity mineral characteristic, but when coarse and irregular particles are incorporated, it is highly abrasive. Thus, only the gel or cream formula, or the type of the abrasive agent present in the dentifrice has not been sufficient to characterize its abrasivity to the tooth structures and composite resins.
The simulated toothbrushing abrasion is considered an established model in the literature, because it is an important in-vitro wear factor, able to simulate a clinical condition. According Sexson and Phillips,20 for each session of brushing a patient performs approximately 15 cycles. Thus, maintaining an oral hygiene based on two daily sessions of brushing, 10,000 cycles are performed by the end of 1 year.
In the present study, the brushing time was statistically significant. The highest surface roughness mean was obtained after 20,000 cycles, the equivalent of 24 months of brushing (0.584 µm), differing statistically from 5,000 cycles, equivalent to 6 months of brushing (0.297 µm) and 10,000 cycles, equivalent to 12 months of brushing (0.354 µm). This finding concurs with other studies.13,15,16,18
In the present study, a nanohybrid composite resin (Empress Direct) and a nanocomposite resin (Z350 XT) were used, and there was no statistical difference in surface roughness among the composite resins. Senawongse and Pongprueksa,14 after evaluating the surface roughness of micro-hybrid, nanohybrid, and nanocomposite resins, also found no significant difference among the materials, although the nanocomposite resin demonstrated fewer irregularities. On the other hand, Suzuki et al.,15 after evaluating the surface roughness of nanohybrid and nanocomposite resins in 50,000 cycles of simulated toothbrushing, concluded that there was significant difference in rates of roughness of composite resins. The nanohybrid composite resins had higher Ra, and nanocomposite resins showed better results, especially Filtek Supreme XT, which was considered a clinically successful composite resin. This finding is not equivalent with the present study, in which both composites (Empress Direct and Z350 XT) performed similarly to a performance evaluation of 24 months (20,000 cycles). This difference in results among studies is probably related to the amount of toothbrushing cycles performed on each study.
According to the manufacturer, the composite resin Z350 XT consists of a combination of zirconia and silica nanoparticles in nanoclusters reducing the interstitial space between the particles and increasing the amount of load. The resin matrix with nanoparticles results in better physical properties and greater wear resistance, which means that during the abrasion these nanoclusters wear at a speed similar to the surrounding resin matrix. The result is a smooth, glossy, and durable polished surface.
Through the analysis of the SEM images, it was found that both composite resins had higher surface irregularities, higher resin matrix wear, and exposure of the filler particles when brushed with the dentifrice OBW. This wear was higher with the increase in the number of brushing cycles. These wear patterns are commonly found in evaluations by SEM after abrasive test.13-16,18
Regarding the clinical significance of this study, it is evident that the surface roughness of composite resins changes according to the type of dentifrice used and the time of brushing, and the whitening dentifrice OBW had greater capacity to change the surface of composite resins.
Conclusions
Within the limitations of the methodology used, it was possible to conclude that:
The composite resins Z350 XT and Empress Direct showed similar surface roughness after all cycles of simulated toothbrushing
The higher the brushing time, the higher the surface roughness of composite resins
The dentifrice OBW caused a higher surface roughness in both composite resins.
Footnotes
Conflicts of Interest: None
Source of Support: Nil
References
- 1.Cury JA, Rosing CK, Tenuta LM. Are dentifrices all the same? Int J Braz Dent. 2010;6:254–6. [Google Scholar]
- 2.Wiegand A, Schlueter N. The role of oral hygiene: does toothbrushing harm? Monogr Oral Sci. 2014;25:215–9. doi: 10.1159/000360379. [DOI] [PubMed] [Google Scholar]
- 3.Kodaka T, Kuroiwa M, Kuroiwa M, Okumura J, Mori R, Hirasawa S, et al. Effects of brushing with a dentifrice for sensitive teeth on tubule occlusion and abrasion of dentin. J Electron Microsc (Tokyo) 2001;50(1):57–64. doi: 10.1093/jmicro/50.1.57. [DOI] [PubMed] [Google Scholar]
- 4.De Menezes M, Turssi CP, Hara AT, Messias DC, Serra MC. Abrasion of eroded root dentine brushed with different toothpastes. Clin Oral Investig. 2004;8(3):151–5. doi: 10.1007/s00784-004-0262-7. [DOI] [PubMed] [Google Scholar]
- 5.Nash RW. Patient demand is increasing for posterior aesthetics. Dent Today. 2010;29(5):74. 76, 78-9. [PubMed] [Google Scholar]
- 6.da Rosa Rodolpho PA, Cenci MS, Donassollo TA, Loguércio AD, Demarco FF. A clinical evaluation of posterior composite restorations: 17-year findings. J Dent. 2006;34:427–35. doi: 10.1016/j.jdent.2005.09.006. [DOI] [PubMed] [Google Scholar]
- 7.Köhler B, Rasmusson CG, Odman P. A five-year clinical evaluation of Class II composite resin restorations. J Dent. 2000;28:111–6. doi: 10.1016/s0300-5712(99)00059-7. [DOI] [PubMed] [Google Scholar]
- 8.Amaral CM, Rodrigues JA, Erhardt MC, Araujo MW, Marchi GM, Heymann HO, et al. Effect of whitening dentifrices on the superficial roughness of esthetic restorative materials. J Esthet Restor Dent. 2006;18(2):102–8. doi: 10.2310/6130.2006.00017_1.x. [DOI] [PubMed] [Google Scholar]
- 9.Liljeborg A, Tellefsen G, Johannsen G. The use of a profilometer for both quantitative and qualitative measurements of toothpaste abrasivity. Int J Dent Hyg. 2010;8(3):237–43. doi: 10.1111/j.1601-5037.2009.00433.x. [DOI] [PubMed] [Google Scholar]
- 10.Hilgenberg SP, Pinto SC, Farago PV, Santos FA, Wambier DS. Physical-chemical characteristics of whitening toothpaste and evaluation of its effects on enamel roughness. Braz Oral Res. 2011;25(4):288–94. doi: 10.1590/s1806-83242011005000012. [DOI] [PubMed] [Google Scholar]
- 11.dos Santos PH, Consani S, Correr Sobrinho L, Coelho Sinhoreti MA. Effect of surface penetrating sealant on roughness of posterior composite resins. Am J Dent. 2003;16(3):197–201. [PubMed] [Google Scholar]
- 12.Chimello DT, Palma-Dibb RG, Corona SA, Lara EH. Assessing wear and surface roughness of different composite resins after toothbrushing. Mater Res. 2001;4:285–9. [Google Scholar]
- 13.Teixeira EC, Thompson JL, Piascik JR, Thompson JY. In vitro toothbrush-dentifrice abrasion of two restorative composites. J Esthet Restor Dent. 2005;17(3):172–80. doi: 10.1111/j.1708-8240.2005.tb00109.x. [DOI] [PubMed] [Google Scholar]
- 14.Senawongse P, Pongprueksa P. Surface roughness of nanofill and nanohybrid resin composites after polishing and brushing. J Esthet Restor Dent. 2007;19(5):265–73. doi: 10.1111/j.1708-8240.2007.00116.x. [DOI] [PubMed] [Google Scholar]
- 15.Suzuki T, Kyoizumi H, Finger WJ, Kanehira M, Endo T, Utterodt A, et al. Resistance of nanofill and nanohybrid resin composites to toothbrush abrasion with calcium carbonate slurry. Dent Mater J. 2009;28(6):708–16. doi: 10.4012/dmj.28.708. [DOI] [PubMed] [Google Scholar]
- 16.Heintze SD, Forjanic M, Ohmiti K, Rousson V. Surface deterioration of dental materials after simulated toothbrushing in relation to brushing time and load. Dent Mater. 2010;26(4):306–19. doi: 10.1016/j.dental.2009.11.152. [DOI] [PubMed] [Google Scholar]
- 17.da Costa J, Adams-Belusko A, Riley K, Ferracane JL. The effect of various dentifrices on surface roughness and gloss of resin composites. J Dent. 2010;38(Suppl 2):e123–8. doi: 10.1016/j.jdent.2010.02.005. [DOI] [PubMed] [Google Scholar]
- 18.Barbieri GM, Mota EG, Rodrigues-Junior SA, Burnett LH., Jr Effect of whitening dentifrices on the surface roughness of commercial composites. J Esthet Restor Dent. 2011;23(5):338–45. doi: 10.1111/j.1708-8240.2011.00426.x. [DOI] [PubMed] [Google Scholar]
- 19.Gusmão ES, Melo JA, Ramos CG, Santos RL, Araújo AC, Feitosa DS. Aplicabilidade clínica dos dentifrícios. Int J Dent. 2003;2:231–5. [Google Scholar]
- 20.Sexson JC, Phillips RW. Studies on the effects of abrasives on acrylic resins. J Prosthet Dent. 1951;1(4):454–71. doi: 10.1016/0022-3913(51)90031-5. [DOI] [PubMed] [Google Scholar]