

Abstract
Background:
Oral hygiene has been given due importance since ages. Different cultures have been using different methods for the maintenance of good oral hygiene. The study was done to find out the oral hygiene levels in children of tribal population and to correlate the brushing methods used and the oral hygiene levels.
Methodology:
A total of 5129 children of 5-12 years age (boys 2778, girls 2351) were checked for the simplified oral hygiene index in the study.
Results:
The overall oral hygiene status of 1267 girls and 1348 boys was fair, whereas 821 girls and 937 boys was good and 263 girls and 493 boys was poor. It has been shown that fair oral hygiene practices were being followed by the children.
Conclusion:
Children using twigs and other materials for oral hygiene had nearly equally good oral hygiene when compared to the tooth brush and tooth paste, though children using toothbrush and tooth paste had slightly better oral hygiene.
Keywords: Brushing methods, oral hygiene, Tribal children
Introduction
Oral hygiene has been given due importance since ages. Different cultures have been using different methods for the maintenance of good oral hygiene. Traditionally, twigs of neem and meswak have been used for cleaning teeth. The Eastern Ghats region of the South Indian subcontinent contains tribal population. The tribal population of the Eastern Ghats had no access to the new oral hygiene aids such as brush and paste and were using the locally available twigs and other materials for oral hygiene. From the past few decades, the tribal population have got access to the new oral hygiene aids such as tooth brush and tooth paste. Though most of the tribal population used twigs and other materials for cleaning their teeth many of them have switched over to the tooth brush and tooth paste. Along with the new oral hygiene aids, the tribal population also got access to the refined foods, candies, sweets, and chocolates, which are cariogenic.
Oral health is a vital component of the general health of an individual. With increased awareness of oral hygiene among the population, oral hygiene methods have improved. Although most of the people use stems of some trees to clean their teeth, studies among the population show that caries prevalence is low or comparable to that of their counterparts in rural area.1
Objectives
To find out the oral hygiene levels in children of tribal population
To correlate the brushing methods used and the oral hygiene levels.
Methodology
A total of 5129 children of 5-12 years age (boys 2778, girls 2351) were included in the study. The oral hygiene status of the children was examined using simplified oral hygiene index (OHI-S).2 OHI-S was developed in 1964 by Green and Vermillion and has two components Debris index-simplified and calculus index-simplified.
For OHI-S the score is as follows:
Good: 0.0-1.2; Fair: 1.3-3.0; Poor: 3.1-6.0.
Results
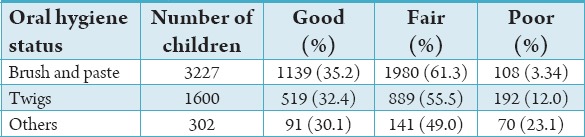
A total of 5129 school going children were examined, among these children, 3227 (62.9%) brushing their teeth with tooth brush and paste, 1600 children (31.1%) using twigs and 301 (5.8%) using other aids for brushing (Table 1). The overall oral hygiene status of 1267 girls and 1348 boys was fair, whereas 821 girls and 937 boys was good and 263 girls and 493 boys was poor. It has been shown that fair oral hygiene practices were being followed by the children (Table 2). 1980 (61.3%) children have shown fair hygiene levels with tooth brush and paste whereas 889 (55.5%) children have shown fair oral hygiene using twigs and 141 (49.0%) children showed fair oral hygiene with other aids. Maximum levels of poor oral hygiene levels (23.1%) were seen in children using other oral hygiene aids (Table 3).
Table 1.
Various brushing methods used.

Table 2.
Oral hygiene status.
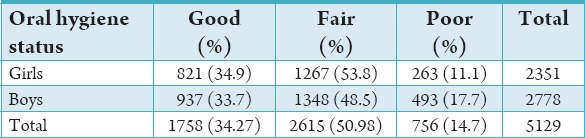
Table 3.
Comparison of brushing habits with different aids.
Discussion
A total of 2615 showed fair oral hygiene and 1758 children showed good oral hygiene and 756 children showed poor oral hygiene. The results show that most of the children show fair to good oral hygiene levels in the tribal population. It supports the study done by Rao and Bharambe also concludes that the tribal population had good oral hygiene compared to their rural counterparts in their study.1 Though most of the children used tooth brush and tooth paste which shows better oral hygiene levels when compared to twigs and other material. Those children using twigs also showed fair oral hygiene levels. Twigs such as neem and meswak have been traditionally used for oral hygiene and are known for their medicinal value. Meswak twigs had shown significant reduction in the levels of Aggregatibacter actinomycetemcomitans in the subgingival plaque according to Al-Otaibi et al.3 In a study by Sarita and Tuominen twigs were most commonly used cleaning method in the tribal population of Tanzania. The sociodemographic factors and the methods of oral cleanliness were not significantly associated with the occurrence of plaque, calculus, and gingival bleeding.4 Some studies on the contrary by Singh revealed poor oral hygiene status among both the fringe end groups. Vast differences were noted between the groups with respect to oral health practices, dietary habits, and dental use pattern. Education for tribal children, male gender, low frequency of cleaning teeth, and higher in between-meal sugar consumption were significantly related to dental caries.5
Singh reveals more sugar consumption, dental fluorosis, poor dental hygiene, and untreated oral disease of tribal children. Under these situations, the implementation of community and prevention campaigns including restriction of candies in school compound for the tribal people is the key to good oral hygiene.6 The study by Kumar et al. shows that people were significantly characterized by a lack of preventive and previous dental care, high treatment needs, high prevalence of periodontal disease, and poor oral hygiene. Under these situations, the implementation of a basic oral health care preventive and treatment program for the Bhil population is a high priority.7 In a study by Baboo et al. the tribal distribution shows that the Tonga are the most susceptible tribe while the Lenje have the least caries. The relationship between caries and brushing habits, as well as consumption of confectionary, was established. The most common teeth affected and their relationship to age was also noted. It was concluded that urbanization had definitely contributed to the higher caries prevalence in the urban school children. Although the situation is not as bad as in the West, if it remains unchecked, 90% of the population may have caries in another 15 years.8
Broughton et al. showed that dental health care program service use was relatively less and symptom-related; most needed to see a dentist. The people believed that it was important to avoid sweets, visit dentists, and to clean their teeth, while about half thought that using fluoridated toothpaste and using dental floss were important. Some felt that drinking water with fluoride was important. Oral health related fatalism was eventual, with most thinking that most people usually get teeth problems, half of them believing that most people will need teeth removal at some stage and that most children eventually get dental decay. Mothers’ played an important role in nurturing the well-being of the young child includes the protection and maintenance of the growing child's oral health (or Ukaipo Niho). The findings provide important insights into Māori mothers’ oral health knowledge, beliefs and practices.9 This study by Kadanakuppe and Bhat revealed less prevalence of oral diseases among iruligas, highlighting the role of good oral hygiene practices prevalent among this remote population.10 Broughton et al. investigated the self-reported oral health and use of oral health services by rangatahi (teenagers) residing within the Waikato rohe (region) of the Waikato-Tainui tribal area. Most children brushed at least once daily. One-quarter reported hiding their smile, and just over one-fifth reported suffering from bad breath. Awareness of their current entitlement to free dental care was high, but it was lower among males. Just over one-third of participants had experienced one or more oral health impact profile (OHIP)-14 impacts; that was higher among females than males, with the largest difference being apparent with the physical disability subscale, where the prevalence of impacts among females was twice that among males. The prevalence of OHIP impacts was higher among those who reported experiencing bad breath often, and significant differences were observed in all seven OHIP domains (as well as in the mean overall OHIP-14 score and in the mean number of different impacts experienced often).11
Al-Otaibi et al. concluded that the meswak is more effective than tooth brushing for reducing plaque and gingivitis when preceded by professional instruction in its correct application. The meswak appeared to be more effective than tooth brushing for removing plaque from the embrasures thus enhancing interproximal health.12
Conclusion
Children using twigs and other materials for oral hygiene had nearly equally good oral hygiene when compared to the tooth brush and tooth paste though children using tooth brush and tooth paste had slightly better oral hygiene.
Footnotes
Conflicts of Interest: None
Source of Support: Nil
References
- 1.Rao SP, Bharambe MS. Dental caries and periodontal diseases among urban, rural and tribal school children. Indian Pediatr. 1993;30(6):759–64. [PubMed] [Google Scholar]
- 2.Greene JC, Vermillion JR. The simplified oral hygiene index. J Am Dent Assoc. 1964;68:7–13. doi: 10.14219/jada.archive.1964.0034. [DOI] [PubMed] [Google Scholar]
- 3.Al-Otaibi M, Al-Harthy M, Gustafsson A, Johansson A, Claesson R, Angmar-Månsson B. Subgingival plaque microbiota in Saudi Arabians after use of miswak chewing stick and toothbrush. J Clin Periodontol. 2004;31:1048–53. doi: 10.1111/j.1600-051X.2004.00618.x. [DOI] [PubMed] [Google Scholar]
- 4.Sarita PT, Tuominen R. Tooth cleaning methods and their effectiveness among adults in rural Tanzania. Proc Finn Dent Soc. 1992;88(3-4):139–45. [PubMed] [Google Scholar]
- 5.Singh A, Purohit B, Sequeira P, Acharya S. Oral health status of 5-year-old Aborigine children compared with similar aged marginalised group in south western India. Int Dent J. 2011;61(3):157–62. doi: 10.1111/j.1875-595X.2011.00033.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Singh A, Bharathi MP, Sequeira P, Acharya S, Bhat M. Oral health status and practices of 5 and 12 year old Indian tribal children. J Clin Pediatr Dent. 2011;35(3):325–30. doi: 10.17796/jcpd.35.3.c8063171438k4362. [DOI] [PubMed] [Google Scholar]
- 7.Kumar TS, Dagli RJ, Mathur A, Jain M, Balasubramanyam G, Prabu D, et al. Oral health status and practices of dentate Bhil adult tribes of southern Rajasthan, India. Int Dent J. 2009;59(3):133–40. [PubMed] [Google Scholar]
- 8.Baboo KS, Bhatia IK, Nkowane BS. A study of dental caries in rural and an urban primary school of Zambia. Med J Zambia. 1981;15(4):56–9. [PubMed] [Google Scholar]
- 9.Broughton JR, Person M, Maipi JT, Cooper-Te KR, Smith-Wilkinson A, Tiakiwai S, et al. Ukaipo niho: The place of nurturing for oral health. N Z Dent J. 2014;110(1):18–23. [PubMed] [Google Scholar]
- 10.Kadanakuppe S, Bhat PK. Oral health status and treatment needs of Iruligas at Ramanagara District, Karnataka, India. West Indian Med J. 2013;62(1):73–80. [PubMed] [Google Scholar]
- 11.Broughton JR, Teh Maipi J, Person M, Randall A, Thomson WM. Self-reported oral health and dental service-use of rangatahi within the rohe of Tainui. N Z Dent J. 2012;108(3):90–4. [PubMed] [Google Scholar]
- 12.Al-Otaibi M, Al-Harthy M, Söder B, Gustafsson A, Angmar-Månsson B. Comparative effect of chewing sticks and toothbrushing on plaque removal and gingival health. Oral Health Prev Dent. 2003;1:301–7. [PubMed] [Google Scholar]