

Abstract
Background:
Complete removal of irritants is not possible with mechanical therapy alone. Adjunctive use of systemic administration of antibiotics results in the distribution of drug throughout the body, which can give rise to toxicity. Curcumin (diferuloylmethane), a constituent of Curcuma longa plant, which possess antioxidant, anti-inflammatory, anti-carcinogenic, anti-microbial, anti-hyper algesic and hypocholesterolemic properties. The aim of the present study is to compare the effects of the curcumin gel as an adjunct to subgingival scaling and root planning with the effect achieved using subgingival scaling and root planning alone.
Materials and Methods:
Thirty patients either male or female with chronic localized or generalized periodontitis aged between 25 and 60 years with pocket depth of 5-7 mm affecting at least two nonadjacent sites were included. In the experimental site scaling and root planning was performed, followed by placement of the curcumin gel and periodontal pack application. In the control site, subgingival scaling alone was performed followed by periodontal pack application. Parameters included were: Plaque index (PI), gingival index (GI), probing depth (PD) and clinical attachment loss. These parameters were recorded on day 0, 30 and 45 days.
Results:
Significant reduction in mean was observed in PI, GI, PD and gain in clinical attachment level were demonstrated in both the groups from baseline to 45 days. However, statistical significant reduction was observed in PI at baseline and 30th day and GI at 30th day.
Conclusion:
Curcumin can be effectively used along with scaling and root planning. Future research is required to determine the long-term effects of curcumin on a large sample of subjects.
Keywords: Antioxidant, curcumin, sub gingival scaling and root planning
Introduction
The ultimate goal of periodontal therapy is to cure inflamed tissue, eliminate the diseased pockets and reduce the number of pathogenic bacteria. Various treatment modalities include mechanical therapy, chemotherapy and systemic administration of antibiotics. Conventional therapy includes scaling, root planning, and curettage. Complete removal of irritants is not possible with mechanical therapy alone. Adjunctive use of systemic administration of antibiotics results in the distribution of drug throughout the body, which can give rise to toxicity problems.1
It is not always possible to predictably deliver an agent to the deeper parts of the pocket with the supragingival irrigation. Mechanical therapy when combined with local delivery systems such as the curcumin gel reduces microbes and improves clinical parameters when compared to scaling root planing alone.2
Various local delivery devices have been used for the targeted delivery of antimicrobial agents, which includes fibers, strips and compacts, gels, micro particles, films, and nano-particles. Natural ways to treat periodontal disease includes number of herbs that can help to eliminate inflammation and infection associated with periodontal diseases. Polyphenols are a group of phytochemicals that are rich sources for anti-oxidants. Among polyphenols, the most widely used substance is Turmeric, a rhizome of Curcuma longa, found to be distributed in tropical and subtropical regions of the world mainly as a spice. It is popularly called Haldi in India and named as a curry spice by British.
Turmeric belongs to zingiberaceae family and cultivated in several parts of the Indian subcontinent, South East Asia and South America. It has widely used in cookery, cosmetics, fabric dying and medicine. The dimensions of this rhizome range between 2.7 and 7 cm in length and about 2.5 cm in diameter.3
Turmeric contains various phyto constituents with (6.3%) of proteins, (5.1%) of fat, (3.5%) minerals, (5%) of diaryl heptanoid coloring material known curcuminoids. Rhizomes with orange pulp contain free arabinose (1%), fructose (12%), glucose (2%), zingeberous starch grains (it was 30-60 µm long). The rhizomes contain curcuminoids, curcumin, demethoxy curcumin, bis demethoxy curcumin, 5’-methoxycurcumin and dihydrocurcumin, which are found to be natural antioxidants.4
Chemically, it is a diferuloylmethane molecule [1,7-bis (4-hydroxy-3- methoxyphenyl)-1,6-heptadiene-3,5-dione)] containing two ferulic acid residues joined by a methylene bridge. By donating an electron or hydrogen atom to reactive oxygen species, curcumin exhibits anti-oxidant property. The o-methoxyphenol group and methylenic hydrogen are responsible for the antioxidant activity of curcumin.5
Curcumin possess antioxidant, anti-inflammatory, anti-carcinogenic, anti-microbial, anti-hyper algesic and hypo cholesterolemic properties. Curcumin has also been shown to counter inflammatory responses similarly to the action of steroids, but without side effects. Following oral administration (up to 8 g/day) it is poorly absorbed, and only the traces of the compound appear in the blood. Curcumin is associated with limited systemic bioavailability as it is poorly absorbed. Serum levels peaked between 1 and 2 h post-dose and declined rapidly.4
Curcumin is available in various forms. The uses of gel as a delivery system enhance bioavailability of the drug by increasing the residence time of drugs on the skin. Ease of administration, non-greasy, patient compliance, high residence time on the skin and better drug release are the advantages seen with gel delivery systems.
Materials and Methods
This randomized controlled clinical study (split-mouth design) with ethical committee approval, was carried out in the Department of Periodontics, MNR Dental College and Hospital, Sangareddy, Hyderabad. This study was conducted as per guidelines of Helsinki declaration 2000 and informed consent was obtained from all subjects who were willing to participate in this study. The study design was approved by the ethical committee of the institution.
In this study, 30 patients either male or female with chronic localized or generalized periodontitis aged between 25 and 60 years with pocket depth of 5-7 mm involving various quadrants of the mouth with two non-adjacent sites were included. The diagnosis of periodontitis was based on the historical data, clinical and radiographic features. A separate proforma sheet was used to record the relevant data. The material used is the curcumin gel (Cure next, About Health Care). Each gram contains 10 mg C. longa extract.
Selected sites were randomized into control and experimental sites by a coin toss. In the experimental site scaling and root planning was performed, followed by placement of the curcumin gel and periodontal pack application. In the control site, subgingival scaling and root planning alone was performed, followed by periodontal pack application. Parameters included were: Plaque index (PI) (Turesky-Gilmore-Glickman modification of the Quigley-Hein, 1970),6 gingival index (GI) (Loe and Silness, 1963),7 probing depth (PD) and clinical attachment loss (CAL) with no gingival recession.
PD was measured with UNC 15 mm probe, acrylic stent as a guide for reproducibility from the gingival margin to base of the pocket. CAL was measured from cemento-enamel junction to the base of the pocket. These parameters were recorded on day 0, 30 and 45 days.
Periodontal therapy
After thorough scaling and root planning, control sites were covered with Coe-Pak. To prevent contamination from saliva, cotton roll isolation was done in the experimental site. Curcumin gel was carried with a 2 ml disposable syringe equipped with a blunted 25-gauge needle, which was bent along its shank. Gel formation occurred as the temperature increases in the oral cavity. Coe-Pak was used to cover the pocket so as to prevent the ingress of oral fluids as well as to allow the retention of the material within the pocket. Oral hygiene instructions were given. Subjects were recalled after 7 days, and periodontal dressing was removed. Patient recalled after 30 and 45 days of the placement of the curcumin gel in order to assess the various clinical parameters.
Statistical analysis
Statistical analysis was performed using t-test. Comparison of clinical parameters within the group at baseline, 30 and 45 days was recorded by paired t-test. Unpaired t-test was used to analyze the post-treatment changes in the control and experimental group.
Results
Thirty patients with 60 sites were treated in this study. In the test site, experimental material was placed after subgingival scaling and root planning. Control sites received only subgingival scaling and root planning. All the sites healed uneventfully at the end of 45 days. Curcumin gel was found to be biologically acceptable without any complications or allergic reactions.
Significant reduction in mean was observed from baseline to 45th day in all the clinical parameters in both experimental and control groups (Table 1).
Table 1.
Comparison of PI, GI, PD, CAL of test and control groups.

However, statistically significant reduction was not observed in PI on 45th day. Statistically significant reduction was not observed in GI at baseline and 30th day in both experimental and control groups. Negative correlation was observed in GI on 45th day.
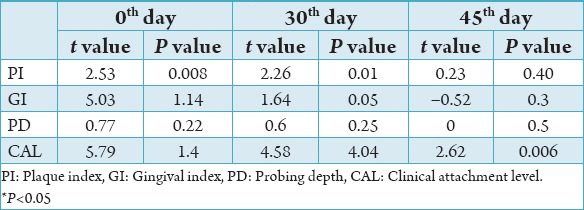
Reduction in mean was found from baseline to 45th day in PD and CAL of both experimental and control groups. However statistically significant reduction was not observed in PD and CAL in both experimental and control groups with CAL showing significant reduction on 45th day (Table 2).
Table 2.
Comparison of P and t value.
Discussion
Turmeric in mouthwash form was used by Bhandari and Shankwalkar8 whereas turmeric in gel form was used in this study. Antimicrobial activity of turmeric was observed by Mun et al.9 and Hamed et al.10
Curcumin possess wound healing and anti-inflammatory property by virtue of which it reduces the inflammatory mediators generated via arachiodonic acid pathway and thereby reduced inflammatory edema and vascular engorgement of connective tissue.11
Curcumin exhibits its anti-inflammatory effect by increasing cortisone production by adrenal glands and by decreasing histamine levels and also by inhibiting the synthesis of prostaglandulins and neutrophil function. Curcumin is half as effective in chronic inflammation as it is effective as cortisone or phenylbutazone in acute inflammation.11
Curcumin also plays a significant role in wound healing by promoting migration of fibroblasts in the wound bed and by bringing about fibrosis of connective tissue. Curcumin promotes migration of epithelial cells to wounded sites by promoting localization of transforming growth factor-beta 1 thus helping re epithelization.4
A short term clinical trial has shown that curcumin irrigation was superior in restoring gingival health by reducing gingivitis using BOP and visual assessment of redness as indicators of gingival health.2
Clinical and microbiological efficacy of curcumin as an irrigant was evaluated by few studies and found no long-term benefits over duration of 6 months. Efficacy of curcumin as an adjunct to scaling and root planning was compared with the gold standard chlorhexidine solution over a period of 6 months. Results of this study shown a significant improvement in clinical and microbiological parameters in both the test and control groups. No significant difference observed in redness and bleeding on probing between chlorhexidine and control groups at 1-month interval. By the end of the study, number of sites which bleeds on probing found to be increased in curcumin group. Thus, the results concluded that curcumin does not possess long term effects as the concentration of curcumin used is not sustained.12
Behal et al.13 conducted a clinical trail in order to compare the effect of 2% whole turmeric gel along with scaling and root planning with the effect achieved using scaling and root planning alone. The effects on PI, GI, bleeding on probing, pocket depth, relative attachment levels, trypsin-like enzyme activity of red complex microorganisms namely Treponema denticola, Bacteroids forsythus was assessed in a split-mouth study involving 30 subjects with chronic localized and generalized periodontitis. The results of the study concluded that 2% gel is more effective when used along with scaling and root planning than scaling and root planning alone in the treatment of periodontal pockets.14
Suhag et al.15 conducted a randomized clinical trail in which scaling and root planning was performed, followed by triple irrigation regimen with either saline (0.9%), chlorhexidine (0.2%), curcumin (1%), or served as non-irrigated control sites on day 0 (baseline) immediately following instrumentation in experimental site. When the regimen was repeated for the next 5 consecutive days and on days 15 and 21, there was a significant reduction in redness and bleeding on probing in the curcumin group on day 5. However, no significant difference was observed in the subsequent visits. The results of this study concluded that 1% curcumin solution can effectively decrease inflammatory signs than chlorhexidine and saline irrigation.11
Hence in the present study, curcumin was found to be effective in removing local factors when performed along with scaling and root planning. The experimental material was well accepted by the patient. Neither complications nor allergic reactions was found.
The curcumin gel used in the present study is easy to use, which can be inserted into the pocket with the help of a syringe. Curcumin shows better retention within the pocket because of its bioadhesive property. Furthermore, curcumin gel was biologically acceptable to all patients without any complications or allergic reactions.
Conclusion
Curcumin is considered a safe, non-toxic and effective alternative for many traditional drugs because of its effects on various systems and therapeutic properties. Curcumin can be effectively used along with scaling and root planning. Curcumin is well accepted by the patient and is easy to use and requires less chair side time. Future research is required to determine the long-term effects of curcumin on a large sample of subjects.
Footnotes
Conflicts of Interest: None
Source of Support: Nil
References
- 1.Kumar P, Ansari SH, Ali J. Herbal remedies for the treatment of periodontal disease –A patent review. Recent Pat Drug Deliv Formul. 2009;3(3):221–8. doi: 10.2174/187221109789105603. [DOI] [PubMed] [Google Scholar]
- 2.Deevaraj SD, Neelakantan P. Curcumin- pharmacological actions and its role in dentistry. Asian J Pharm Res Health Care. 2014;6(1):19–22. [Google Scholar]
- 3.Sambhav J, Rohit R, Ankit Raj U, Garima M. Curcuma longa in the management of inflammatory diseases –A review. Int Ayur Med J. 2014;2(1):34–40. [Google Scholar]
- 4.Mathur V, Tijare M, Desai A, Gupta S, Kallianpur S. Curcumin –Oral cure from the Indian curry. Int J Pharmacother. 2014;4(3):137–40. [Google Scholar]
- 5.Suhag A, Dixit J, Dhan P. Role of curcumin as a sub gingival irrigant: A pilot study. PERIO. 2000;4(2):115–21. [Google Scholar]
- 6.Turesky S, Gilmore ND, Glickman I. Reduced plaque formation by the chloromethyl analogue of victamine C. J Periodontol. 1970;41(1):41–3. doi: 10.1902/jop.1970.41.41.41. [DOI] [PubMed] [Google Scholar]
- 7.Loe H, Silness J. Periodontal disease in pregnancy. I. prevalence and severity. Acta Odontol Scand. 1963;21:533–51. doi: 10.3109/00016356309011240. [DOI] [PubMed] [Google Scholar]
- 8.Bhandari H, Shankwalkar GB. Dissertation Submitted to the University of Bombay; 1980. Clinical assessment of action of combination of indigenous drugs on dental plaque, calculus and gingivitis. [Google Scholar]
- 9.Mun SH, Kim SB, Kong R, Choi JG, Kim YC, Shin DW. Curcumin reverse methicillin resistance in Staphylococcus aureus. Molecules. 2014;19(11):18283–95. doi: 10.3390/molecules191118283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hamed OA, Mehdawi N, Taha AA, Hamed EM, Al-Nuri MA, Hussein AS. Synthesis and antibacterial activity of novel curcumin derivatives containing heterocyclic moiety. Iran J Pharm Res. 2013;12(1):47–56. [PMC free article] [PubMed] [Google Scholar]
- 11.Nagpal M, Sood S. Role of curcumin in systemic and oral health: An overview. J Nat Sci Biol Med. 2013;4(1):3–7. doi: 10.4103/0976-9668.107253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gottumukkala SN, Konneru S, Mannem S, Mandalapu N. Effectiveness of subgingival irrigation of an indigenous 1% curcumin solution on clinical and microbiological parameters in chronic periodontitis patients: A pilot randomized clinical trail. Contemp Clinical Dent. 2013;4(2):186–91. doi: 10.4103/0976-237X.114874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Behal R, Mali AM, Gilda SS, Paradkar AR. Evaluation of local drug-delivery system containing 2% whole turmeric gel used as an adjunct to scaling and root planing in chronic periodontitis: A clinical and microbiological study. J Indian Soc Periodontol. 2011;15(1):35–8. doi: 10.4103/0972-124X.82264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lawande SA. Therapeutic applications of turmeric in dentistry. J Pharm Biomed Sci. 2013;27(27):586–91. [Google Scholar]
- 15.Suhag A, Dixit J, Dhan P. Role of curcumin as a subgingival irrigant - A pilot study. PERIO. 2007;2:115–21. [Google Scholar]