

Abstract
Hispanic women have higher rates of neural tube defects and report lower total folic acid intakes than non‐Hispanic white (NHW) women. Total folic acid intake, which is associated with neural tube defect risk reduction, has been found to vary by acculturation factors (i.e. language preference, country of origin, or time spent in the United States) among Hispanic women. It is unknown whether this same association is present for blood folate status. The objective of this research was to assess the differences in serum and red blood cell (RBC) folate concentrations between NHW women and Mexican American (MA) women and among MA women by acculturation factors. Cross‐sectional data from the 2001–2010 National Health and Nutrition Examination Survey (NHANES) were used to investigate how blood folate concentrations differ among NHW or MA women of childbearing age. The impact of folic acid supplement use on blood folate concentrations was also examined. MA women with lower acculturation factors had lower serum and RBC folate concentrations compared with NHW women and to their more acculturated MA counterparts. Consuming a folic acid supplement can minimize these disparities, but MA women, especially lower acculturated MA women, were less likely to report using supplements. Public health efforts to increase blood folate concentrations among MA women should consider acculturation factors when identifying appropriate interventions.
Keywords: acculturation, folate biomarkers, Mexican Americans, NHANES, red blood cell folate, serum folate
Introduction
Consuming adequate amounts of folic acid, the synthetic form of folate, can reduce the risk of having a serious birth defect of the brain or spine (called a neural tube defect) (MRC Vitamin Study Research Group 1991; Berry et al. 1999). Research has found that compared with non‐Hispanic white (NHW) women, Hispanic women have a higher reported prevalence of neural tube defects (Williams et al. 2005). Additionally, some studies indicate that lower acculturated Hispanics are at an even higher risk for neural tube defects compared with their more acculturated counterparts (Velie et al. 2006; Canfield et al. 2009).
Acculturation is a term that has been used to describe an individual's integration into a dominant culture (Thomson & Hoffman‐Goetz 2009). This process has been studied for multiple behaviours and health outcomes in the Hispanic population, including dietary intakes, birth outcomes, obesity, diabetes and alcohol use (Flores et al. 2007; Carmichael et al. 2008; Canfield et al. 2009; Sofianou et al. 2011; Buttenheim et al. 2013). Several studies have reported differences by acculturation factors in folate intake or in consumption of foods that are high in folate among Hispanic women (Guendelman & Abrams 1995; Dixon et al. 2000; Neuhouser et al. 2004; Harley et al. 2005; Hamner et al. 2011). Although these studies' findings have not always been consistent, it is important to understand whether acculturation factors could impact overall folate intake. Further, it is critical to understand the factors that can impact total folate intake from synthetic sources (folic acid) and natural sources (natural food folate). However, assessing total folate intake has several limitations. Dietary assessment tools have been found to have measurement error (Henriquez‐Sanchez et al. 2009; Subar A.F. et al. 2003), and it can be difficult to compare findings when two different tools have been used (Kowalkowska et al. 2013). Many tools are also unable to differentiate between natural food folate and synthetic folic acid intake. This can be problematic when trying to assess whether a woman is meeting the US Public Health Service recommendation of 400 μg of folic acid [Centers for Disease Control and Prevention (CDC) 1992]. As a result of these imprecisions, the use of biomarkers such as serum folate or red blood cell (RBC) folate concentrations could provide a more accurate picture of a woman's folate status. However, no study has assessed how acculturation factors impact blood folate status among women of childbearing age.
Given the higher prevalence of neural tube defects among Hispanic women (Williams et al. 2005), the link between folic acid and neural tube defects, (MRC Vitamin Study Research Group 1991; Berry et al. 1999) and the suggestion of differences in folate intake by acculturation, we wanted to investigate whether there was also an association between biomarkers of folate status and acculturation. The objective of this research was to investigate differences in serum and RBC folate concentrations between NHW women and Mexican American (MA) women and among MA women by acculturation status. This information could help inform prevention efforts and potentially provide another factor that should be considered when assessing blood folate status.
Key messages
This study's findings suggest that Mexican American women with lower acculturation factors have significantly lower serum and red blood cell folate concentrations than both their non‐Hispanic white and more acculturated Mexican American counterparts.
Consumption of a folic acid‐containing supplement has the potential to mitigate differences in blood folate concentrations by acculturation status among Mexican American women.
Consideration of acculturation status is important when developing targeted messages, materials, and interventions to increase blood folate status among Mexican American women.
Participants and methods
National Health and Nutrition Examination Survey (NHANES), 2001–2010
Data from the continuous NHANES survey for 2001–2010 were used for this analysis. NHANES 2001–2010 was conducted in 2‐year phases (2001–2002, 2003–2004, 2005–2006, 2007–2008 and 2009–2010) using a stratified multistage probability design. Each 2‐year cycle captured a nationally representative sample of the non‐institutionalized civilian population. Respondents participated in both a household questionnaire and a physical examination at the Mobile Examination Center (MEC), with an overall, unweighted response rate for the examined sample ranging between 75% and 80% during the data collection period. Data from 2001 to 2010 were combined and analysed and weighted using MEC sample weights (10‐year sample weights for serum folate and 4‐year sample weights for RBC folate). The analysis sample was restricted to non‐pregnant female respondents aged 15–44 years who attended the MEC and reported being of NHW or MA race/ethnicity. NHANES has oversampled MA from 2001 to 2010, which allows us to present reliable estimates for this subpopulation. All participants in NHANES provide written informed consent.
Serum and RBC folate
Serum and RBC folate concentrations were collected for survey years 2001–2010. From 2001 to 2006, blood folate concentrations were assessed using the BioRad (Laboratories Headquarters, 1000 Alfred Nobel Drive, Hercules, CA 94547) (Quantaphase II) radioassay. Beginning in 2007, blood folate concentrations were assessed using the microbiologic assay. Equations have been developed to convert results using BioRad to the equivalent values using the microbiologic assay (Fazili et al. 2007). However, Fazili et al. have indicated that blood folate concentrations measured with the BioRad radioassay vary depending on an individual's methylenetetrahydrofolate reductase (MTHFR) genotype (Fazili et al. 2008). These differences are particularly noticeable for RBC folate concentrations (Molloy et al. 1998; Fazili et al. 2008). Because MTHFR genotype data are not publicly available for participants with RBC folate concentrations from 2001 to 2006, and we could not account for the effect of the BioRad radioassay measurement error by MTHFR genotype, we limited our analyses to RBC folate concentrations from 2007 to 2010 because they were measured with the microbiologic assay, which is more accurate and is not as affected by MTHFR genotype. Serum folate concentrations do differ by analytic method; however, the ability to convert between the two methods is not as dependent on genotype (Fazili et al. 2007; Yetley et al. 2011). Therefore, we utilized data from 2001 to 2010 for serum folate with adjustments to the 2001–2006 data to account for the differences in methodology as recommended by the National Center on Health Statistics (NCHS) [National Center for Health Statistics Centers for Disease Control and Prevention (NCHS CDC) 2006].
Acculturation factors
NHANES collects information on acculturation factors for individuals who are aged ≥12 years and who report being of Hispanic origin. These measures include primary language spoken in the home, country of origin and years living in the United States. As done previously, individuals were classified into three categories for language spoken: (1) report primarily speaking English all or most of the time; (2) report speaking equal English and Spanish; or (3) report primarily speaking Spanish all or most of the time (Hamner et al. 2011). For country of origin and time in the United States, variables were dichotomized, United States vs. Mexico and <15 years vs. ≥15 years, respectively (Hamner et al. 2011). For purposes of these analyses, lower acculturation groups were considered those women who reported speaking Spanish all or most of the time at home, being born in Mexico, or residing in the United States for <15 years. Each acculturation factor was treated as an exclusive category because of the high correlation between the individual factors (e.g. 86% of women who reported speaking Spanish all or most of the time were born in Mexico).
Covariates
Data on race/ethnicity, age, education level, poverty income ratio, supplement use, language preference, country of origin and time in the United States were collected during a household interview survey. Participants reported their race/ethnicity as either NHW, non‐Hispanic black, MA, other Hispanic or other race/ethnicity; however, we only included respondents who reported NHW and MA race/ethnicity in our analyses. Education level was categorized into three levels: (1) less than high school; (2) high school or general educational development; or (3) college or above. A ratio of family income to the poverty threshold was explored and ratios less than 1.0 were considered below the poverty threshold. Supplement use was based on whether the participant reported consuming a folic acid‐containing supplement in the past 30 days.
Statistical analysis
Frequencies of socio‐demographic characteristics and geometric mean blood folate concentrations for each race and ethnic group of interest were estimated. Geometric means were estimated for blood folate concentrations because the data were not normally distributed and were logged to improve normality. Chi‐square tests and t‐tests were used to determine statistical differences in demographic characteristics and in blood folate concentrations, respectively. P‐values < 0.05 were considered significant. Additionally, we investigated the proportion of women in our sample whose RBC folate concentrations fell below a widely cited blood folate concentration estimate associated with a birth prevalence rate of neural tube defects of 8 per 10 000 live births (Daly et al. 1995). The analyses were conducted using SAS 9.2 and SUDAAN 10.0 to account for the complex sampling design of NHANES. The estimates were weighted according to NCHS guidelines (NCHS CDC 2006).
Analytic sample
There were a total of 4985 NHW and MA nonpregnant women aged 15–44 years who went to the MEC during the years 2001–2010. Of these women, 4670 had serum blood folate data available for analysis from 2001 to 2010 and 1831 had RBC folate data available for analysis from 2007 to 2010. There were no differences in demographic characteristics between women who did or did not provide blood samples from 2001 to 2010 with the exception that MA women who provided blood samples tended to be slightly older than MA women who didn't provide blood (data not shown). Therefore, all demographic analyses are presented for the entire sample (n = 4985).
Results
Demographic characteristics
Among the 4985 NHW and MA women 15–44 years old in 2001–2010, 86.7% were NHW and 13.3% were MA (weighted percentages; Table 1). Among MA women, 50.9% reported primarily speaking Spanish, 53.2% reported being born in Mexico, and 35.1% reported living in the United States for <15 years (Table 1). Compared with NHW women, MA women were more likely to be younger, less educated, live below the poverty threshold, and not report consuming a folic acid‐containing supplement. Regardless of acculturation factors, MA and NHW women were significantly different by demographic characteristics (P < 0.05). Among MA women, age, education level, poverty income ratio and folic acid‐containing supplement use differed by language spoken, country of origin and time in the United States (P < 0.05 for all comparisons by acculturation; Table 1). However, almost all reported supplement users consumed a similar amount of folic acid from supplements (about 300–400 μg d−1), regardless of race or acculturation (Table 1).
Table 1.
Demographic and behavioural characteristics of NHW and MA women aged 15–44 years by race/ethnicity and acculturation factors, National Health and Nutrition Examination Survey 2001–2010*, †
| Women 15–44 years | MA | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Language spoken | Country of origin | Time in the United States | |||||||
| NHW | MA | Primarily Spanish | Equal English/Spanish | Primarily English | Mexico | United States | <15 years | ≥15 years | |
| Total | |||||||||
| n | 3080 | 1905 | 875 | 362 | 667 | 907 | 991 | 603 | 1269 |
| Total | 86.7 (84.3, 88.8) | 13.3 (11.2, 15.7) | 50.9 (47.0, 54.8) | 15.9 (13.7, 18.3) | 33.2 (29.9, 36.7) | 53.2 (48.6, 57.7) | 46.8 (42.4, 51.4) | 35.1 (30.9, 39.6) | 64.9 (60.4, 69.1) |
| Age (years) | |||||||||
| n | 3080 | 1905 | 875 | 362 | 667 | 907 | 991 | 603 | 1269 |
| 15–24 | 31.8 (29.9, 33.8) | 36.0 (33.8, 38.2) ‡ | 28.3 (25.5, 31.3) ‡ , § | 48.9 (42.1, 55.8) ‡ | 41.5 (37.9, 45.2) ‡ | 25.7 (23.0, 28.7) ‡ , § | 47.6 (44.0, 51.2) ‡ | 32.8 (29.0, 26.8) ‡ , § | 37.8 (34.9, 40.9) ‡ |
| 25–34 | 30.2 (28.3, 32.2) | 33.0 (30.3, 35.9) | 35.1 (31.1, 39.5) | 31.2 (24.3, 39.0) | 30.7 (25.7, 36.2) | 36.0 (32.1, 40.1) | 29.8 (25.7, 34.4) | 40.0 (34.8, 45.4) | 29.0 (25.8, 32.7) |
| 35–44 | 38.0 (35.9, 40.1) | 31.0 (28.1, 34.0) | 36.6 (32.7, 40.6) | 20.0 (15.1, 25.9) | 27.8 (23.5, 32.5) | 38.3 (34.3, 42.4) | 22.6 (19.3, 26.3) | 27.2 (22.7, 32.3) | 33.0 (29.4, 36.9) |
| Education level | |||||||||
| n | 3078 | 1903 | 874 | 361 | 667 | 906 | 990 | 603 | 1267 |
| <High school | 20.7 (19.1, 22.3) | 51.7 (48.1, 55.2) ‡ | 66.8 (62.7, 70.7) ‡ , § | 43.5 (37.2, 50.1) ‡ , § | 32.4 (28.1, 37.1) ‡ | 65.0 (61.0, 68.9) ‡ , § | 36.6 (32.9, 40.4) ‡ | 67.7 (62.7, 72.3) ‡ , § | 42.5 (38.7, 46.4) ‡ |
| High school graduate/GED | 21.1 (19.4, 22.9) | 19.8 (17.7, 22.0) | 16.0 (13.3, 19.1) | 24.2 (18.8, 30.7) | 23.4 (20.1, 27.0) | 17.5 (14.6, 20.9) | 22.5 (19.6, 25.7) | 16.9 (13.6, 20.8) | 21.4 (18.9, 24.1) |
| ≥College | 58.3 (55.8, 60.7) | 28.6 (25.4, 31.9) | 17.2 (14.1, 20.8) | 32.2 (25.6, 39.7) | 44.2 (39.6, 49.0) | 17.5 (14.6, 20.9) | 40.9 (36.9, 45.1) | 15.4 (12.0, 19.7) | 36.1 (32.5, 39.9) |
| Poverty income ratio | |||||||||
| n | 2950 | 1743 | 780 | 324 | 638 | 811 | 925 | 548 | 1178 |
| <Poverty threshold | 14.6 (12.7, 16.7) | 35.0 (31.7, 38.4) ‡ | 45.0 (40.2, 49.8) ‡ , § | 31.3 (25.3, 38.0) ‡ , § | 22.5 (18.3, 27.4) ‡ | 43.4 (38.8, 48.2) ‡ , § | 25.5 (21.4, 30.1) ‡ | 48.9 (43.1, 54.7) ‡ , § | 27.4 (23.8, 31.3) ‡ |
| ≥Poverty threshold | 85.4 (83.3, 87.3) | 65.0 (61.6, 68.3) | 55.1 (50.2, 59.8) | 68.7 (62.0, 74.8) | 77.5 (72.6, 81.7) | 56.6 (51.8, 61.2) | 74.5 (69.9, 78.6) | 51.1 (45.3, 56.9) | 72.4 (68.7, 76.2) |
| Folic acid‐containing supplement use (%) | |||||||||
| n | 3079 | 1904 | 874 | 362 | 667 | 906 | 991 | 602 | 1269 |
| User | 36.5 (34.1, 38.9) | 17.6 (15.8, 19.5) ‡ | 14.4 (11.9, 17.4) ‡ , § | 14.2 (10.1, 19.7) ‡ , § | 24.0 (20.6, 27.8) ‡ | 15.0 (12.7, 17.7) ‡ , § | 20.6 (18.1, 23.4) ‡ | 14.4 (11.8, 17.4) ‡ , § | 19.4 (16.9, 22.1) ‡ |
| Mean FA intake (μg d−1) | 381.2 (360.2, 402.3) | 368.2 (321.7, 414.8) | 389.6 (315.4, 463.8) | 289.0 (191.0, 386.9) ‡ | 369.9 (310.9, 428.9) | 381.8 (317.7, 445.8) | 356.6 (304.6, 408.7) | 379.8 (296.0, 463.6) | 357.2 (310.6, 403.9) |
FA, folic acid; GED, General Educational Development; MA, Mexican American; NHW, non‐Hispanic white. *Values are % (95% confidence intervals). † N values might not add up because of missing data (education, n = 4; poverty income ratio, n = 292; supplement use, n = 2; language, n = 1; country of origin, n = 7; time in the United States, n = 33). ‡Different from NHW, P < 0.05 (Rao‐Scott modified chi‐square test for age, education, poverty, and supplement use). §Different from most acculturated within acculturation factor, P < 0.05 (Rao‐Scott modified chi‐square test for age, education, poverty, and supplement use).
Serum folate (2001–2010)
Compared with NHW women, MA women had significantly lower serum folate concentrations (16.8 ng mL−1 vs. 14.9 ng mL−1, P < 0.05; Table 2). This difference was seen regardless of level of acculturation (P < 0.05 for all comparisons between NHW and MA by acculturation). Additionally, compared with their more acculturated MA counterparts, MA women with the lowest acculturation factors (i.e. those who reported primarily speaking Spanish, being born in Mexico, or living in the United States <15 years) had significantly lower serum folate concentrations (P < 0.05; Table 2).
Table 2.
Geometric mean serum folate and RBC folate concentrations of NHW and MA women aged 15–44 years by race/ethnicity and acculturation factors, National Health and Nutrition Examination Survey 2001–2010*
| Women 15–44 years | MA | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Language spoken | Country of origin | Time in the United States | |||||||
| NHW | MA | Primarily Spanish | Equal English/Spanish | Primarily English | Mexico | United States | <15 years | ≥15 years | |
| Serum folate (ng mL−1) (2001–2010) † | |||||||||
| n | 2874 | 1796 | 828 | 341 | 626 | 863 | 926 | 571 | 1195 |
| Total | 16.8 (16.4, 17.3) | 14.9 (14.4, 15.2) § | 14.4 (13.9, 14.9) § , ¶ | 14.4 (13.5, 15.6) § | 15.6 (14.9, 16.4) § | 14.6 (14.0, 15.0) § , ¶ | 15.2 (14.6, 15.8) § | 14.3 (13.7, 14.9) § , ¶ | 15.2 (14.6, 15.6) § |
| Stratified by folic acid supplement use | |||||||||
| n | 978 | 293 | 116 | 41 | 136 | 126 | 167 | 82 | 207 |
| Users | 20.9 (20.3, 21.8) | 19.5 (18.4, 20.5) § | 19.1 (17.8, 20.7) § | 20.9 (18.7, 23.1) | 19.3 (18.0, 20.9) | 19.1 (17.6, 20.5) § | 19.9 (18.5, 21.1) | 19.1 (17.5, 20.9) | 19.5 (18.4, 20.9) |
| n | 1895 | 1502 | 711 | 300 | 490 | 736 | 759 | 488 | 988 |
| Non‐users | 14.7 (14.3, 15.2) | 13.9 (13.5, 14.3) § | 13.7 (13.2, 14.3) § | 13.6 (12.4, 14.7) | 14.6 (13.7, 15.5) | 13.9 (13.5, 14.4) § | 14.2 (13.5, 14.7) § | 13.6 (13.1, 14.2) § | 14.3 (13.7, 14.9) |
| RBC folate (ng mL−1) (2007–2010) ‡ | |||||||||
| n | 1205 | 626 | 311 | 105 | 210 | 318 | 302 | 180 | 422 |
| Total | 464 (450, 483) | 424 (399, 446) § | 403 (384, 424) § , ¶ | 441 (392, 498) | 441 (407, 473) | 403 (384, 424) § , ¶ | 446 (416, 478) | 395 (380, 416) § , ¶ | 437 (407, 464) |
| Stratified by folic acid supplement use | |||||||||
| n | 357 | 104 | 50 | 16 | 38 | 55 | 49 | 33 | 67 |
| Users | 556 (534, 578) | 508 (464, 550) | 498 (455, 545) § | 556 (437, 706) | 498 (433, 572) | 508 (464, 556) | 503 (437, 578) | 508 (446, 572) | 508 (455, 567) |
| n | 848 | 522 | 261 | 89 | 172 | 263 | 253 | 147 | 355 |
| Non‐users | 424 (412, 441) | 407 (384, 433) | 388 (365, 412) § , ¶ | 420 (376, 469) | 428 (392, 464) | 384 (365, 403) § , ¶ | 433 (399, 469) | 376 (358, 395) § , ¶ | 424 (392, 455) |
MA, Mexican American; NHW, non‐Hispanic white. *Values are age‐adjusted geometric means (95% confidence interval). † N values might not add up because of missing data (supplement use, n = 2; language, n = 1; country of origin, n = 7; time in the United States, n = 30). ‡ N values might not add up because of missing data (supplement use, n = 0; language, n = 0, country of origin, n = 6; time in the United States, n = 24). §Different from NHW, P < 0.05. ¶Different from most acculturated within acculturation factor, P < 0.05.
Compared with NHW women who were supplement users, MA women who were supplement users and reported primarily speaking Spanish or being born in Mexico had significantly lower serum folate concentrations (P < 0.05; Table 2). Among MA women who were supplement users, differences by acculturation factors were attenuated and not statistically significant.
Compared with NHW women who did not report consuming a supplement, MA women who did not report consuming a supplement and reported primarily speaking Spanish, living in the United States <15 years, or either being born in the United States or in Mexico had significantly lower serum folate concentrations (P < 0.05). Among MA women who did not report consuming a supplement, there were no significant differences in serum folate concentrations by acculturation factors.
RBC folate (2007–2010)
Geometric mean RBC folate concentrations were 464 ng mL−1 and 424 ng mL−1 for NHW women and MA women, respectively (P < 0.05; Table 2). Compared with NHW women, MA women with lower acculturation factors (i.e. those who reported primarily speaking Spanish, being born in Mexico, or living in the United States <15 years) had significantly lower RBC folate concentrations. Among all MA women, those who reported primarily speaking Spanish, being born in Mexico, or living in the United States for <15 years had significantly lower RBC folate concentrations compared with their more acculturated MA counterparts (P < 0.05; Table 2).
Among NHW women and MA women who reported consuming a supplement, there were no significant differences in RBC folate concentrations, with one exception: MA women who reported primarily speaking Spanish had lower RBC folate concentrations than NHW women.
RBC folate concentrations for NHW and MA women who did not report consuming a supplement did not differ (424 ng mL−1 vs. 407 ng mL−1, respectively). MA women who did not report consuming a supplement and who had the lowest acculturation factors (i.e. those who reported primarily speaking Spanish, being born in Mexico, or living in the United States <15 years) had significantly lower RBC folate concentrations than NHW women who did not report consuming a supplement and their more acculturated MA counterparts (P < 0.05; Table 2).
Discussion
Monitoring of blood folate concentrations on a national scale has occurred for many years in the United States (Pfeiffer et al. 2007, 2012; Yetley & Johnson 2011). An apparent racial/ethnic disparity in blood folate concentrations between NHW women and MA women has been observed both before and after folic acid fortification (Pfeiffer et al. 2012). Looking at post‐fortification data in the present study, our results show that this disparity is even more pronounced when blood folate concentrations for MA women are stratified by acculturation factors. In fact, MA women with lower acculturation factors (those who reported primarily speaking Spanish, being born in Mexico, or living in the United States < 15 years) had significantly lower serum and RBC folate concentrations than both NHW women and their more acculturated MA counterparts.
Consumption of a supplement containing folic acid can have an impact on blood folate status. To account for this effect, we stratified our analyses by supplement use and found that regardless of use, MA women with lower acculturation factors tended to have lower serum folate concentrations than NHW women. The impact of supplement use on RBC folate concentrations was slightly different; among supplement users, differences by race/ethnicity and acculturation were attenuated or no longer present. However, among women who did not report consuming a supplement, MA women with lower acculturation factors had significantly lower RBC folate concentrations than both their more acculturated MA counterparts and NHW women. RBC folate concentrations are a better indicator of long‐term folate status (Chanarin 1986; Gibson 2005). Therefore, these results suggest that among women who did not report consuming a supplement, race/ethnicity and acculturation factors might greatly contribute to the presence of disparities.
To the authors' knowledge, this is the first report to assess the relationship between acculturation and blood folate concentrations among MA women of childbearing age. Other acculturation literature on women of childbearing age has focused on changes in dietary or other health outcomes. Changes in dietary and supplemental folate intake as a result of acculturation could influence blood folate concentrations. A systematic review of acculturation and diet among Latinos reported that lower acculturated individuals had higher overall intakes of folate and greater intakes of foods rich in natural folate (Ayala et al. 2008). Contrary to these findings, Hamner et al. reported that folate intake from natural food folate did not differ by acculturation factors among MA women, but total folic acid intake (folic acid coming from enriched cereal grain products, ready‐to‐eat cereals, and dietary supplements) was lower among MA women who reported lower acculturation factors, 283 μg folic acid per day [95% confidence interval (CI): 211, 353] among MA women who reported primarily speaking English compared with 206 μg folic acid per day (95% CI: 164, 248) and 224 μg folic acid per day (95% CI: 175, 272) among MA women who reported speaking equal English/Spanish and primarily Spanish, respectively (Hamner et al. 2011). Although the findings in these previous studies do not necessarily agree, they do suggest the existence of differences in dietary folate intake by acculturation. Our study supports these earlier conclusions in that we found evidence of differences in serum and RBC folate concentrations by both race/ethnicity and acculturation, but the impact is different depending on which biomarker is assessed and whether supplements are consumed or not.
Public health relevance is an important issue to consider when looking at the differences in our reported serum and RBC folate concentrations. Although statistical differences between groups were observed, the overall clinical relevance between RBC folate concentrations of geometric means of 464 ng mL−1 and 424 ng mL−1 might not be readily apparent. However, a paper by Daly et al. reported that the lowest risk of having a neural tube defect‐affected pregnancy was associated with women who had RBC folate concentrations ≥906 nmol L−1 (≥400 ng mL−1; Daly et al. 1995). Analytic differences in measuring RBC blood folate concentrations should be taken into account as the method for assessing RBC folate concentrations differed slightly between Daly et al. (1995) and the method used for analysing NHANES samples (NCHS CDC 2006). Therefore, we have converted this value (Daly et al. 1995) into the equivalent value if the same analytic method as used in NHANES had been used (Equation: Y = (X0.7876 + 34.2802)/2.266, where Y is the Daly converted RBC folate concentration and X is the RBC folate concentration from the NHANES data; Daly converted: 330 ng mL−1; unpublished formula from the data presented in Pfeiffer et al., 2011). Using this cut‐point, we can put our reported NHANES values into a larger public health context. Overall, the geometric mean RBC folate concentration of our sample is above the Daly et al. value. However, a greater proportion of MA women who did not report consuming a supplement and who had lower acculturation factors did not meet the Daly et al. value (330 ng mL−1; Fig. 1). Nearly a quarter of MA women overall (24.5%), and approximately 30% of MA women with lower acculturation factors (i.e. those who reported primarily speaking Spanish, being born in Mexico, or living in the United States <15 years) who did not report consuming a supplement, are at risk of having a RBC folate concentration below a value associated with the lowest risk for having a neural tube defect‐affected pregnancy. Even among supplement users, about twice as many MA women with lower acculturation factors (11.4–12.5%), compared with NHW women (6.0%), did not meet the Daly et al. value (Fig. 1), indicating the potential for this population to be at increased risk for a neural tube defect‐affected pregnancy.
Figure 1.
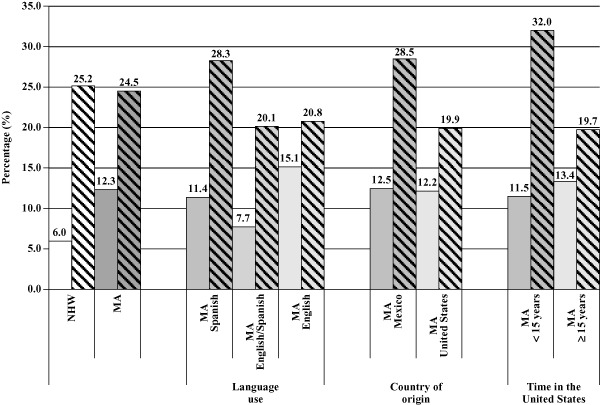
Proportion of women who have red blood cell folate concentrations less than 400 ng mL−1 (906 nmol L−1) by race/ethnicity and acculturation and supplement use, National Health and Nutrition Examination Survey (NHANES) 2007–2010; The value of 400 ng mL−1 (906 nmol L−1) was converted to the NHANES equivalency to be consistent with results reported previously (conversion formula: {[(906 × 0.7876) + 34.2802]/2.266} = 330 ng ml−1; unpublished formula from the data presented in Pfeiffer et al., 2011). The banded fill pattern in the figure represent supplement non‐users. The Daly et al. value of 400 ng mL−1 (906 nmol L−1) is associated with a birth prevalence rate of neural tube defects of 8 per 10 000 live births; MA, Mexican American; NHW, non‐Hispanic white.
This study was subject to several limitations. First, we were unable to use a validated scale to measure acculturation because the variables needed were not available in NHANES. However, we did use several variables that are often utilized in developing acculturation scales, and language use has been found to be a strong indicator for explaining a large proportion of the variation in acculturation (Cuellar et al. 1980; Marin et al. 1987). Second, our findings cannot be generalized to the entire Hispanic population, but only to MA women living in the United States. Third, NHANES is a cross‐sectional survey, and we were unable to assess temporal or causal relationships. Fourth, the intention of this paper was to describe the current blood folate status among women by race/ethnicity and acculturation status and determine to what degree folic acid supplement use may affect this relationship; therefore, we conducted bivariate analyses only. Multivariate analyses would be important for determining the main predictors of blood folate concentrations in this population and could be explored in future research. Lastly, statistically significant differences might not equate to a biological or clinically significant difference. We do attempt to put our findings into a public health context by comparing our findings to reported RBC folate concentrations associated with the lowest risk of having a neural tube defect‐affected pregnancy. This study also had several strengths. NHANES is a nationally representative data source, and we are able to provide reliable estimates for different subsets of the population including MA women. This study also uses biomarkers to assess blood folate status, which are not subject to as many limitations as dietary intake data.
We found that serum and RBC folate concentrations were significantly lower among lower acculturated MA women than NHW women. While folic acid supplement use has the potential to minimize this disparity, more than 80% of MA women do not report using supplements. These analyses suggest the need for interventions to target the most vulnerable populations, especially MA women with lower acculturation factors. While there is great potential to increase supplement use among MA women, previous public health campaigns to increase consumption of a folic acid‐containing supplement have had limited impact. Public health campaigns specifically targeting Hispanic women have been attempted previously, but tend to be costly and result in small increases in supplement use among these women and might not be sustainable (Flores et al. 2007). One intervention that may be more effective for this population is folic acid fortification of corn masa flour, which could potentially increase the folic acid intake of MA women with lower acculturation factors (Hamner et al. 2013). For example, nearly 80% of MA women with lower acculturation factors (i.e. those who reported primarily speaking Spanish, being born in Mexico, or living in the US <5 years) reported consumption of corn masa flour compared with 50–60% of MA women with higher acculturation factors (i.e. those who reported primarily speaking English, being born in the United States or living in the United States ≥15) and 27% of NHW women (Hamner et al. 2013). While no federal regulation currently exists to fortify corn masa flour with folic acid, the first step would be submitting a petition to the FDA to either develop a new standard of identity for ‘enriched’ corn masa flour products or to amend the current FDA food additive regulation for folic acid (Fleischman & Oinuma 2011). The latter has been submitted as of June 2012 (Gruma Corporation et al. 2012). A final ruling on the food additive petition for corn masa flour could take several years.
Our findings suggest that acculturation factors could be an important way to identify women who might be at risk of having a blood folate concentration that is below a value associated with the lowest risk of a neural tube defect‐affected pregnancy. This information is important for state‐ and local‐level birth defects prevention activities that include the development of targeted messages, materials and interventions.
Source of funding
None.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Contributions
The authors' responsibilities were as follows: CMM and HCH designed the research, wrote the paper and were responsible for the final content; CMM analysed data and performed statistical analyses. Both authors read and approved the final manuscript.
Acknowledgements
We thank Sasha Guo, Yan Ping Qi and Sarah Tinker for statistical support and guidance in conducting the analyses and Christine Pfeiffer for her technical assistance. This project was supported by an appointment to the Research Participation Program for the Centers for Disease Control and Prevention administered by the Oak Ridge Institute for Science and Education through an agreement between the Department of Energy and CDC.
Marchetta, C. M. , and Hamner, H. C. (2016) Blood folate concentrations among women of childbearing age by race/ethnicity and acculturation, NHANES 2001–2010. Matern Child Nutr, 12: 39–50. doi: 10.1111/mcn.12134.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
References
- Ayala G.X., Baquero B. & Klinger S. (2008) A systematic review of the relationship between acculturation and diet among Latinos in the United States: implications for future research. Journal of the American Dietetic Association 108, 1330–1344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berry R.J., Li Z., Erickson J.D., Li S., Moore C.A., Wang H. et al (1999) Prevention of neural‐tube defects with folic acid in China. China–U.S. Collaborative Project for Neural Tube Defect Prevention. The New England Journal of Medicine 341, 1485–1490. [DOI] [PubMed] [Google Scholar]
- Buttenheim A.M., Pebley A.R., Hsih K., Chung C.Y. & Goldman N. (2013) The shape of things to come? Obesity prevalence among foreign‐born vs. US‐born Mexican youth in California. Social Science and Medicine 78, 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Canfield M.A., Ramadhani T.A., Shaw G.M., Carmichael S.L., Waller D.K., Mosley B.S. et al (2009) Anencephaly and spina bifida among Hispanics: maternal, sociodemographic, and acculturation factors in the National Birth Defects Prevention Study. Birth Defects Research. Part A, Clinical and Molecular Teratology 85, 637–646. [DOI] [PubMed] [Google Scholar]
- Carmichael S.L., Shaw G.M., Song J. & Abrams B. (2008) Markers of acculturation and risk of NTDs among Hispanic women in California. Birth Defects Research. Part A, Clinical and Molecular Teratology 82, 755–762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC) (1992) Recommendations for the use of folic acid to reduce the number of cases of spina bifida and other neural tube defects. MMWR. Morbidity and Mortality Weekly Report 41(RR‐14);001. [PubMed] [Google Scholar]
- Chanarin I. (1986) Folate deficiency In: Folates and pterins (eds Blakley R. & Whitehead V.), pp. 75–146. John Wiley & Sons: New York. [Google Scholar]
- Cuellar I., Harris L.C. & Jasso R. (1980) An acculturation scale for Mexican American normal and clinical populations. Hispanic Journal of Behavioral Sciences 2, 199–217. [Google Scholar]
- Daly L.E., Kirke P.N., Molloy A., Weir D.G. & Scott J.M. (1995) Folate levels and neural tube defects. Implications for prevention. JAMA: The Journal of the American Medical Association 274, 1698–1702. [DOI] [PubMed] [Google Scholar]
- Dixon L.B., Sundquist J. & Winkleby M. (2000) Differences in energy, nutrient, and food intakes in a US sample of Mexican‐American women and men: findings from the Third National Health and Nutrition Examination Survey, 1988–1994. American Journal of Epidemiology 152, 548–557. [DOI] [PubMed] [Google Scholar]
- Fazili Z., Pfeiffer C.M. & Zhang M. (2007) Comparison of serum folate species analyzed by LC‐MS/MS with total folate measured by microbiologic assay and Bio‐Rad radioassay. Clinical Chemistry 53, 781–784. [DOI] [PubMed] [Google Scholar]
- Fazili Z., Pfeiffer C.M., Zhang M., Jain R.B. & Koontz D. (2008) Influence of 5,10‐methylenetetrahydrofolate reductase polymorphism on whole‐blood folate concentrations measured by LC‐MS/MS, microbiologic assay, and Bio‐Rad radioassay. Clinical Chemistry 54, 197–201. [DOI] [PubMed] [Google Scholar]
- Fleischman A.R. & Oinuma M. (2011) Fortification of corn masa flour with folic acid in the United States. American Journal of Public Health 101, 1360–1364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flores A.L., Prue C.E. & Daniel K.L. (2007) Broadcasting behavior change: a comparison of the effectiveness of paid and unpaid media to increase folic acid awareness, knowledge, and consumption among Hispanic women of childbearing age. Health Promotion Practice 8, 145–153. [DOI] [PubMed] [Google Scholar]
- Gibson R.S. (2005) Principles of Nutritional Assessment, 2nd edn, Oxford University Press: New York. [Google Scholar]
- Gruma Corporation, Spina Bifida Association, March of Dimes Foundation, American Academy of Pediatrics, Royal DSM N.V. & National Council of La Raza (2012) Filing of Food Additive Petition FAP 2A4796. (ed U.S. Food and Drug Administration).
- Guendelman S. & Abrams B. (1995) Dietary intake among Mexican‐American women: generational differences and a comparison with white non‐Hispanic women. American Journal of Public Health 85, 20–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamner H.C., Cogswell M.E. & Johnson M.A. (2011) Acculturation factors are associated with folate intakes among Mexican American women. The Journal of Nutrition 141, 1889–1897. [DOI] [PubMed] [Google Scholar]
- Hamner H.C., Tinker S.C., Flores A.L., Mulinare J., Weakland A.P. & Dowling N.F. (2013) Modelling fortification of corn masa flour with folic acid and the potential impact on Mexican‐American women with lower acculturation. Public Health Nutrition 16, 912–921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harley K., Eskenazi B. & Block G. (2005) The association of time in the US and diet during pregnancy in low‐income women of Mexican descent. Paediatric and Perinatal Epidemiology 19, 125–134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henriquez‐Sanchez P., Sanchez‐Villegas A., Doreste‐Alonso J., Ortiz‐Andrellucchi A., Pfrimer K. & Serra‐Majem L. (2009) Dietary assessment methods for micronutrient intake: a systematic review on vitamins. The British Journal of Nutrition 102 (Suppl. 1), S10–S37. [DOI] [PubMed] [Google Scholar]
- Kowalkowska J., Slowinska M.A., Slowinski D., Dlugosz A., Niedzwiedzka E. & Wadolowska L. (2013) Comparison of a full food‐frequency questionnaire with the three‐day unweighted food records in young polish adult women: implications for dietary assessment. Nutrients 5, 2747–2776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marin G., Sabogal F., Marin B.V., Oterosabogal R. & Perezstable E.J. (1987) Development of a short acculturation scale for hispanics. Hispanic Journal of Behavioral Sciences 9, 183–205. [Google Scholar]
- Molloy A.M., Mills J.L., Kirke P.N., Whitehead A.S., Weir D.G. & Scott J.M. (1998) Whole‐blood folate values in subjects with different methylenetetrahydrofolate reductase genotypes: differences between the radioassay and microbiological assays. Clinical Chemistry 44, 186–188. [PubMed] [Google Scholar]
- MRC Vitamin Study Research Group (1991) Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. MRC Vitamin Study Research Group. Lancet 338, 131–137. [PubMed] [Google Scholar]
- National Center for Health Statistics Centers for Disease Control and Prevention (NCHS CDC) (2006) ANALYTIC AND REPORTING GUIDELINES The National Health and Nutrition Examination Survey (NHANES). Hyattsville, Maryland.
- Neuhouser M.L., Thompson B. & Solomon C.C. (2004) Higher fat intake and lower fruit and vegetables intakes are associated with greater acculturation among Mexicans living in Washington state. Journal of the American Dietetic Association 104, 51–57. [DOI] [PubMed] [Google Scholar]
- Pfeiffer C.M., Johnson C.L., Jain R.B., Yetley E.A., Picciano M.F., Rader J.I. et al (2007) Trends in blood folate and vitamin B‐12 concentrations in the United States, 1988–2004. The American Journal of Clinical Nutrition 86, 718–727. [DOI] [PubMed] [Google Scholar]
- Pfeiffer C.M., Zhang M., Lacher D.A., Molloy A.M., Tamura T., Yetley E.A. et al (2011) Comparison of serum and red blood cell folate microbiologic assays for national population surveys. The Journal of Nutrition 141, 1402–1409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pfeiffer C.M., Hughes J.P., Lacher D.A., Bailey R.L., Berry R.J., Zhang M. et al (2012) Estimation of trends in serum and RBC folate in the U.S. population from pre‐ to postfortification using assay‐adjusted data from the NHANES 1988–2010. The Journal of Nutrition 142, 886–893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sofianou A., Fung T.T. & Tucker K.L. (2011) Differences in diet pattern adherence by nativity and duration of US residence in the Mexican‐American population. Journal of the American Dietetic Association 111, 1563–1569 e1562. [DOI] [PubMed] [Google Scholar]
- Subar A.F., Kipnis V., Troiano R.P., Midthune D., Schoeller D.A., Bingham S. et al (2003) Using intake biomarkers to evaluate the extent of dietary misreporting in a large sample of adults: The OPEN Study. American Journal of Epidemiology 158, 1–13. [DOI] [PubMed] [Google Scholar]
- Thomson M.D. & Hoffman‐Goetz L. (2009) Defining and measuring acculturation: a systematic review of public health studies with Hispanic populations in the United States. Social Science and Medicine 69, 983–991. [DOI] [PubMed] [Google Scholar]
- Velie E.M., Shaw G.M., Malcoe L.H., Schaffer D.M., Samuels S.J., Todoroff K. et al (2006) Understanding the increased risk of neural tube defect‐affected pregnancies among Mexico‐born women in California: immigration and anthropometric factors. Paediatric and Perinatal Epidemiology 20, 219–230. [DOI] [PubMed] [Google Scholar]
- Williams L.J., Rasmussen S.A., Flores A., Kirby R.S. & Edmonds L.D. (2005) Decline in the prevalence of spina bifida and anencephaly by race/ethnicity: 1995–2002. Pediatrics 116, 580–586. [DOI] [PubMed] [Google Scholar]
- Yetley E.A. & Johnson C.L. (2011) Folate and vitamin B‐12 biomarkers in NHANES: history of their measurement and use. The American Journal of Clinical Nutrition 94, 322S–331S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yetley E.A., Pfeiffer C.M., Phinney K.W., Fazili Z., Lacher D.A., Bailey R.L. et al (2011) Biomarkers of folate status in NHANES: a roundtable summary. The American Journal of Clinical Nutrition 94, 303S–312S. [DOI] [PMC free article] [PubMed] [Google Scholar]