

Abstract
Objective
To investigate a lifespan health behavior mechanism relating childhood personality to adult clinical health.
Methods
Childhood Big Five personality traits at mean age 10, adult Big Five personality traits, adult clinically assessed dysregulation at mean age 51 (a summary of dysregulated blood glucose, blood pressure, and lipids), and a retrospective, cumulative measure of lifespan health-damaging behavior (lifetime smoking, physical inactivity, and Body Mass Index from age 20) were assessed in the Hawaii Personality and Health Cohort (N = 759). Structural equation modelling was used to test the conceptual model with direct and indirect paths from childhood Conscientiousness to adult Conscientiousness, lifespan health-damaging behaviors, educational attainment, adult cognitive ability, and adult clinic health.
Results
For both men and women, childhood Conscientiousness influenced health-damaging behaviors through educational attainment, and lifespan health-damaging behaviors predicted dysregulation. Childhood Conscientiousness predicted adult Conscientiousness, which did not predict any other variables in the model. For men, childhood Conscientiousness predicted dysregulation through educational attainment and health-damaging behaviors. For women, childhood Conscientiousness predicted dysregulation through educational attainment and adult cognitive ability.
Conclusions
Assessing cumulative lifespan health behaviors is a novel approach to the study of health behavior mechanisms. Childhood Conscientiousness appears to influence health assessed more than forty years later through complex processes involving educational attainment, cognitive ability, and the accumulated effects of health behaviors but not adult Conscientiousness.
Keywords: Childhood personality, clinical health, health behaviors, educational attainment, cognitive ability
Substantial evidence has accumulated to demonstrate that the Big Five personality traits measured in adulthood (Extraversion, Agreeableness, Conscientiousness, Emotional stability, and Intellect/Openness), are associated prospectively with health status and mortality (Bogg & Roberts, 2013; Jokela et al., 2013; Kern & Friedman, 2008). Furthermore, the Big Five personality traits assessed in childhood, in particular childhood Conscientiousness and related traits of self-regulation, predict mortality (Friedman et al., 1993) and objectively assessed health outcomes later in life (Hampson, Edmonds, Goldberg, Dubanoski, & Hillier, 2013; Moffitt et al., 2011). Lifespan personality-health research is now focused on identifying mechanisms to account for these long-term associations between childhood personality and adult health outcomes (Friedman & Kern, 2014). Ideally, this research uses longitudinal samples that have been assessed from childhood to adulthood on appropriate measures of personality, health, and potential mediating mechanisms. However, such studies are exceedingly rare. The current study contributes to this sparse literature by examining whether a retrospective report of cumulative health behaviors performed over substantial periods of the lifespan explain some portion of the association between childhood personality and clinically assessed health status more than 40 years later.
Of the several mechanisms proposed to account for the effects of personality on later health outcomes (Friedman, 2000; Hampson & Friedman, 2008; Smith, 2006), health behavior models have so far proved to be the most compelling, and suggest potential opportunities for intervention. Health behavior models propose that personality traits influence the performance of health-damaging and health-enhancing behaviors that are risk and protective factors for the leading causes of morbidity and mortality in the United States (Mokdad, Marks, Stroup, & Gerberding, 2004; U.S. Department of Health and Human Services, 2004). There is ample evidence that personality traits measured in adulthood, particularly Conscientiousness, are associated with health-related behaviors, including smoking, physical activity, and eating habits (Bogg & Roberts, 2004). Studies have also examined health behaviors as mediators of the influence of adult personality on mortality (e.g., Hagger-Johnson et al., 2012; Hill, Turiano, Hurd, Mroczek, & Roberts, 2011; Lodi-Smith et al., 2010; Turiano, Chapman, Gruenewald, & Mroczek, 2013; Turiano, Hill, Roberts, Spiro, & Mroczek, 2012). As comprehensively reviewed by Turiano et al. (2013), these and other studies of adult personality traits and health outcomes show varying degrees of support for health-behavior mechanisms.
Studies of health-behavior mechanisms to account for the association between childhood personality and adult health outcomes are rare (Friedman et al., 1995; Martin, Friedman, & Schwartz, 2007). The leading causes of mortality such as heart disease and diabetes develop over decades and are associated with health-damaging behavior patterns including smoking, physical inactivity and poor diet. We theorized that childhood Conscientiousness influences adult health outcomes by directing an individual onto enduring pathways of more or less healthful behaviors that have cumulative effects on health over time. That is, health outcomes should be worse for individuals who have had greater lifetime exposure to smoking, inactivity, and excessive calorie consumption. A limitation of much of the previous work investigating health-behavior mechanisms is the lack of measures that capture accumulation of multiple behaviors over time. In the present study, we partially rectified this by using a cumulative index composed of retrospective reports of these behaviors over previous periods of the lifespan. Because we expect health behaviors to have cumulative effects over time, and childhood Conscientiousness is likely to influence these, we further theorized that child Conscientiousness will be a stronger predictor of adult health status in comparison to adult Conscientiousness. That is, we predicted lasting effects of child Conscientiousness on adult health that would only be partially, if at all, superseded by later influences from adult Conscientiousness.
The present study examined a chain-of influence model (Shanahan, Hill, Roberts, Eccles, & Friedman, 2014) in which health behaviors reportedly performed over decades were hypothesized to explain the association between childhood personality and later health status. In addition to using a retrospective, cumulative measure of lifespan health-damaging behavior, this study is novel in several other important respects that addressed limitations of previous work. It is one of very few studies with both child and adult personality and objectively assessed adult health outcomes. This study also included two other major influences on health outcomes, namely educational attainment and adult cognitive ability. Both are associated with childhood personality (Duckworth, Quinn, & Tsukayama, 2012; Lönnqvist, Vainikainen, & Verkasalo, 2012), as well as health and longevity (Calvin et al., 2011; Deary, Weiss, & Batty, 2010; Hagger-Johnson, Shickle, Deary, & Roberts, 2010), and are therefore likely to affect the development of health-enhancing or health-damaging behaviors over the lifespan.
The model was tested using data from the Hawaii Longitudinal Study of Personality and Health. Previously, it was reported for this sample that childhood Conscientiousness was the only Big Five trait to be associated with objectively assessed cardiovascular and metabolic health over 40 years later, even after controlling for adult Conscientiousness (Hampson et al., 2013). The present study builds on this finding to investigate a possible lifespan health-damaging behavior mechanism underlying the association between childhood Conscientiousness and objectively assessed physiological dysregulation in adulthood (a combination of cardiovascular and metabolic biomarkers that included systolic and diastolic blood pressure, lipids, fasting blood glucose, and urine protein). We hypothesized that lower childhood Conscientiousness predicts higher levels of health-damaging behavior across the lifespan, and that a greater accumulation of lifespan health-damaging behavior predicts greater adult dysregulation when also allowing for pathways through educational attainment and cognitive ability (see Figure 1). The influence of childhood Conscientiousness on dysregulation was expected to be greater than that of adult Conscientiousness. On the basis of the established gender differences in mortality and morbidity, and the gender differences observed here and in previous findings (Hampson et al., 2013; Hampson, Goldberg, Vogt, & Dubanoski, 2006), we tested this model separately for men and women on an exploratory basis.
Figure 1.
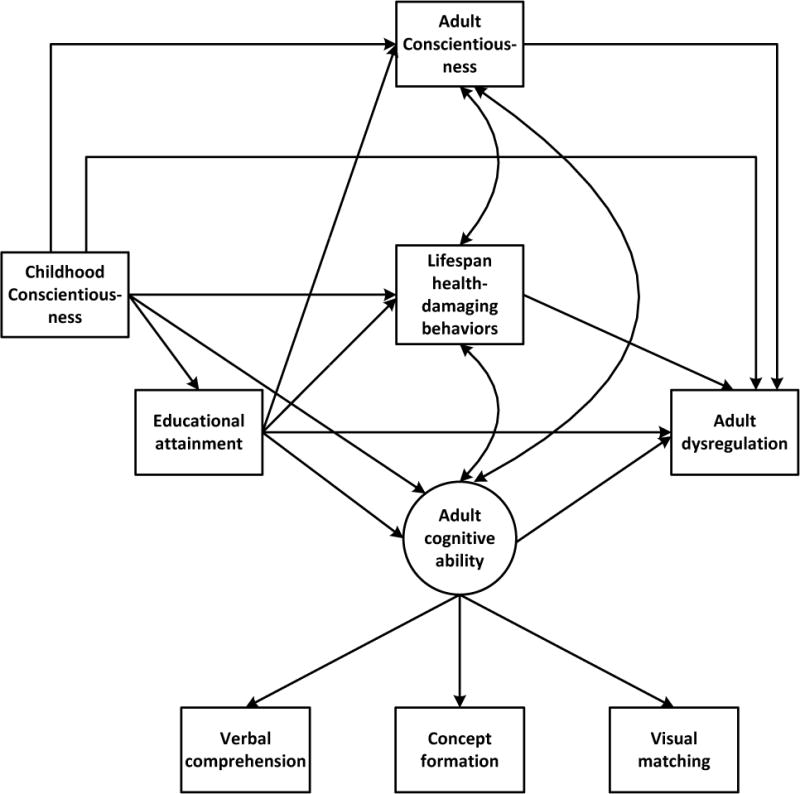
Hypothesized initial model from childhood Conscientiousness to dysregulation including indirect paths through lifespan health-damaging behaviors, educational attainment and adult cognitive ability, with lifespan health-damaging behaviors and adult cognitive ability allowed to correlate.
Method
Participants and Procedures
Timeline
Between 1959 and 1967, children in entire elementary school classrooms on two Hawaiian islands were assessed on their personality traits by their teachers towards the end of one school year. In 1998, efforts to find these children, now middle-aged adults, were begun. When each member of the original cohort was located (i.e., rolling recruitment), they were invited to join the study. Since joining, participants have completed one or more of six questionnaires (Q1 – Q6) and, from 2003 onwards, have been invited to attend a half-day medical and psychological examination. In addition to the childhood personality assessment, measures used here were drawn from items in Q1 (adult personality, smoking, educational attainment), Q3 (smoking, physical activity and inactivity), and Q4 (BMI), and the clinic visit (cognitive ability, physiological dysregulation). On average, Q3 was completed 5.4 years after Q1 (SD = .40, range <1 – 7.5 years), and Q4 was administered 2 years after Q3. The clinic visit occurred 1.2 years after Q3 (SD = 2.2, range −2.7 – 7.3 years).
Sample
Of the 2,418 in the original child cohort, 79 were already deceased and 19 only had first names recorded, leaving 2,320 to locate. Of these, 1,938 (84%) have been found. Among those found, 36 immediately refused further contact and one was illiterate, reducing the potential sample to 1,901. Of these, 1,387 (73%) have been recruited and completed at least one questionnaire. To be included in the subsample for this report, participants had to have participated in the medical and psychological examination at 51 years, and to have completed the first questionnaire. Five participants were excluded because of substantial differences in the traits used in their childhood personality assessment at their school. These requirements limited the eligible subsample to 372 men and 387 women (N = 759).
Compared to participants who provided demographic information on the first questionnaire or by phone but did not attend the medical and psychological examination (n = 622), this subsample included more Japanese Americans (35% vs 28%), fewer Caucasians (16% vs. 24%) and Native Hawaiians or other Pacific Islanders (19% vs. 25%), and more “Other” ethnicities (30% vs. 23%). They also had higher educational attainment (M = 6.88 vs. 6.57), but did not differ on any of the childhood Big Five traits.
Measures
Childhood personality
For the children in the present sample, teachers assessed their entire elementary school classrooms (Grades 1, 2, 5, or 6; M age = 10 years) by rank-ordering children on each of a comprehensive set of 43–49 personality attributes, which included 39 items common to all children, using a 9-step quasi-normal distribution. Definitions for each attribute, developed by teachers, were provided. Orthogonal factor scores (standard scores) for the Big Five were derived for subgroups of children who were rated on the same set of attributes (Goldberg, 2001). Mean alpha reliabilities across subgroups for these factor scores (Ten Berge & Hofstee, 1999) were as follows: .75 (Extraversion), .62 (Agreeableness), .77 (Conscientiousness), .68 (Emotional Stability), and .60 (Intellect/Imagination) (Edmonds, Goldberg, Hampson, & Barckley, 2013). The validity of these childhood measures as predictors of adult outcomes has been demonstrated in previous studies (e.g., Goldberg, 2001; Hampson et al., 2006; Hampson, Goldberg, Vogt, & Dubanoski, 2007; Woods & Hampson, 2010).
Adult personality traits
The first questionnaire included the 44-item Big Five Inventory (John & Srivastava, 1999). Participants rated the self-descriptiveness of each item (1 = very inaccurate, 5 = very accurate). Alpha reliabilities for this measure for the Hawaii cohort are as follows: .84 (Extraversion), .78 (Agreeableness), .80 (Conscientiousness), .82 (Emotional Stability), and .79 (Intellect/Openness) (Edmonds et al., 2013).
Lifespan health-damaging behaviors: smoking, physical inactivity, and obesity
Smoking history was assessed by items from Q1 and Q3. Where participants reported never smoking on Q1 but provided a smoking history on Q3 (n = 60), their latter responses were used. Ever smokers (at least 100 cigarettes in their entire life) were asked the age when they started smoking regularly, whether they smoked now and, if so, how much they smoked per day. Ex-smokers were asked their age when they first started smoking, their age when they quit, and on average how much they smoked per day over all the years they smoked. Life-time smoking history was coded as 0 = ≤ 100 cigarettes, 1 = previously smoked < 8 pack-years, 2 = previously smoked ≥ 8 pack-years, 3 = currently smoke (in last year) ≤ ½ pack a day, 4 = currently smoke (in last year) ≥ 1 pack a day. A pack year, derived from participants’ smoking histories, was defined as the equivalent of smoking one pack a day for one year. The median number of pack years for ex-smokers was 8. This measure assessed the extent of previous smoking among ex-smokers, as well as extent of smoking among current smokers to better capture lifetime cigarette exposure.
Cumulative physical inactivity over the lifespan was assessed by separate questions on Q3 asking participants to check the time periods when they “engaged in no exercise and were quite inactive,” and to check the time periods when they “engaged in sports or were otherwise quite physically active.” For each question, they checked as many of the following 10 periods as applied: before entering school, during elementary school, during junior high, during high school, from age 18–25, from age 26–30, from age 31–35, from age 36–40, from age 41–45, and from age 46 onward. The sum of periods of physical inactivity minus the sum of periods of activity was calculated to create a cumulative physical inactivity score (maximum score = 10).
Body Mass Index (BMI; kg/m2) across adult life was assessed on Q4 by self-reported height and weight at age 20, 30, and 40. Height reported for one age was assumed to be the same if missing for others. Where height or weight was missing, BMI was imputed from other items assessing obesity, which were less often missing.1 The sum of BMI across ages 20, 30 and 40 was used as a cumulative measure of obesity. Using a sum versus a mean would make no difference to correlations or betas in the analytic model. The sum of the three time periods was used to reflect the concept of cumulative exposure to the health-damaging effects of obesity. Missing data on components of the summative variables of physical inactivity or BMI would potentially underestimate lifetime exposure to these variables, thus operating against our hypotheses. While not a direct measure of quantity or quality of food intake, obesity has been used as an indicator of behaviors conducive to weight gain in previous comparable longitudinal studies (Friedman et al., 1993; Turiano et al., 2013). Retrospective dietary recall over the lifespan was deemed impractical and error prone.
Smoking behavior, physical inactivity, and BMI across the lifespan were not highly inter-correlated (smoking and BMI: r = .11; smoking and physical inactivity: r = −.04; BMI and physical inactivity r = −.05). We reasoned that greater accumulated exposure to one or more of these behaviors would have negative consequences for health. Each measure was z-scored for men and women combined and the three measures were summed to form an index of accumulated exposure to health-damaging behaviors across the lifespan (higher scores equal more unhealthy behavior).
Clinical indicators of health status
A composite measure of dysregulation was formed from the following cardiovascular and metabolic biomarkers: systolic and diastolic blood pressure (means of two assessments), total cholesterol/HDL ratio, HDL (reversed), fasting triglycerides, fasting blood glucose, and urine protein (log transformed). Previously, we included obesity and medication taking in this measure (Hampson et al., 2013; Hampson, Goldberg, Vogt, Hillier, & Dubanoski, 2009). These two components were removed from the present measure because they can both be construed as health behaviors, one of the hypothesized mediators in this study: obesity is a proxy for diet, and medication taking is a proxy for treatment seeking and adherence.2 Moreover, obesity to age 40 (as a proxy for diet) was included in the measure of lifetime health behaviors. A participant’s dysregulation score was derived by standardizing each measure across men and women and summing the standard deviations from the mean. There were 9 participants who were missing either one or two measures. In an earlier investigation of dysregulation, we allowed for the possibility of curvilinear models for some components of dysregulation where both extreme high and low scores were associated with poor health. Across the indicators of dysregulation, few (1–2%) participants fell in the very low, unhealthy range (Hampson et al., 2009). This justified treating dysregulation as a linear gradient where higher scores indicate poorer health, and low scores indicate better overall health.
Educational attainment
Participants checked their highest level of educational attainment ranging from 1 = eighth grade or less to 9 = postgraduate or professional degree.
Adult cognitive ability
Three domains of cognitive ability were assessed using tests from the Woodcock Johnson III battery (Woodcock, Mather, & McGrew, 2001): verbal comprehension (picture vocabulary, synonyms, antonyms, analogies), concept formation (identifying the dimensions on which two sets of drawn objects differ), and timed visual matching (finding pairs of identical numbers in strings of numbers). These three domains were used as indicators for a latent construct of cognitive ability.
Results
Means and standard deviations for men and women on all study variables, and significant gender differences, are presented in Table 1. In childhood, women were viewed by their teachers as less extraverted, more conscientious, and less emotionally stable as children than were men. As adults, women had higher cognitive ability and less dysregulation than men. For both genders, the only childhood personality trait to correlate with dysregulation was Conscientiousness. The only adult trait to correlate with dysregulation was adult Conscientiousness for women (r = −.11). The correlations among all the study variables are shown in Table 2. Residualized change scores for Conscientiousness (regressing adult scores on child scores) were not significantly correlated with dysregulation for men (r = .05) or women (r = −.08) indicating that change in Conscientiousness from child to adult did not account for additional variance beyond the child trait, which is consistent with the modest stability of Conscientiousness from childhood to adulthood for this cohort (r = .25; Edmonds et al., 2013).
Table 1.
Descriptive Statistics for Men and Women
| Men (n = 372) Mean (SD) |
Women (n = 387) Mean (SD) |
Cohen’s d | |
|---|---|---|---|
| Age (in years) at clinic examination | 51.57 (2.78) | 51.49 (2.82) | .03 |
| Educational attainment (1 = ≤ 8th grade, 9 = postgraduate) |
6.83 (1.82) | 6.93 (0.77) | .06 |
| Childhood personality | |||
| Extraversion | .14 (.96) | −.05 (1.01) | .20* |
| Agreeableness | −.05 (.98) | .09 (.99) | .14 |
| Conscientiousness | −.24 (1.00) | .43 (.88) | .71* |
| Emotional Stability | .09 (.97) | −.10 (1.00) | .19* |
| Intellect/openness | .10 (1.08) | .03 (.92) | .08 |
| Cognitive ability | −.14 (.86) | .11 (.76) | .30* |
| Lifespan health-damaging behavior | −.05 (1.76) | −.04 (1.73) | .01 |
| Dysregulation | .18 (.55) | −.18 (.53) | .68* |
Note. Childhood personality, lifespan health-damaging behaviors, cognitive ability, and dsysregulation are in standard scores. Significant differences between men and women are shown.
p < .05
Table 2.
Correlations among all constructs in the model, women above the diagonal and men below the diagonal
| 1 | 2 | 3 | 4 | 5 | 6 | ||
|---|---|---|---|---|---|---|---|
| 1 | Child Conscientiousness | .15** | .16** | .23** | −.11 | −.13* | |
| 2 | Adult Conscientiousness | .24** | .09 | .09 | −.16* | −.11* | |
| 3 | Educational attainment | .16** | .11* | .55** | −.28** | −.18** | |
| 4 | Cognitive ability | .11* | .05 | .60** | −.22** | −.15** | |
| 5 | Lifespan health-damaging behavior | −.20** | −.14* | −.27* | −.27** | .20** | |
| 6 | Dysregulation | −.10* | .03 | −.23** | −.15** | .33** |
p < .05,
p < .01
Figure 1 shows the hypothesized directional and correlational paths tested in the initial model. Adult cognitive ability and lifespan health-damaging behavior were allowed to correlate because adult cognitive ability could not have influenced health behaviors reportedly performed decades earlier. Adult Conscientiousness was allowed to correlate with lifespan health-damaging behaviors and adult cognitive ability. Model testing was conducted using Mplus Version 7.0 (Muthén & Muthén, 1998–2012) with maximum likelihood estimation for missing data3. Model fit was evaluated by the chi-square statistic and, because it is sensitive to sample size, it was supplemented by the two-index approach recommended by Hu and Bentler (1999): the root mean square error of approximation (RMSEA), and the comparative fit index (CFI). They suggested cutoffs of .06 for RMSEA and .95 for CFI for excellent fit, and statistics close to these cutoffs are considered acceptable. While retaining the direct path from childhood Conscientiousness to adult dysregulation, other hypothesized but non-significant paths were removed sequentially, starting with the least significant path first. Using this trimmed model, we tested the significance of all indirect paths use using a bootstrapping method within MPlus (Bollen & Stine, 1990; Shrout & Bolger, 2002).
The final models provided support for a cumulative health behavior mechanism (see Figures 2a for men and 2b for women. The models accounted for 7.4% of the variance in dysregulation for women and 16.5% of the variance in dysregulation for men. For both genders, childhood Conscientiousness predicted adult Conscientiousness, but adult Conscientiousness did not predict any other variables in the model. In addition, childhood Conscientiousness predicted lifespan health-damaging behaviors through educational attainment, and lifespan health-damaging behaviors predicted dysregulation. Thereafter, the indirect effects differed across the models for men and women (see Table 3). In the model for men, higher childhood Conscientiousness was associated with less dysregulation through less health-damaging behavior. Educational attainment was also involved in predicting health behavior and dysregulation: consistent with a chain of influence, the indirect path from childhood Conscientiousness to dysregulation through educational attainment and health-damaging behaviors was significant. Men’s cognitive ability did not predict dysregulation, but a significant direct path from educational attainment to dysregulation was retained in the model.
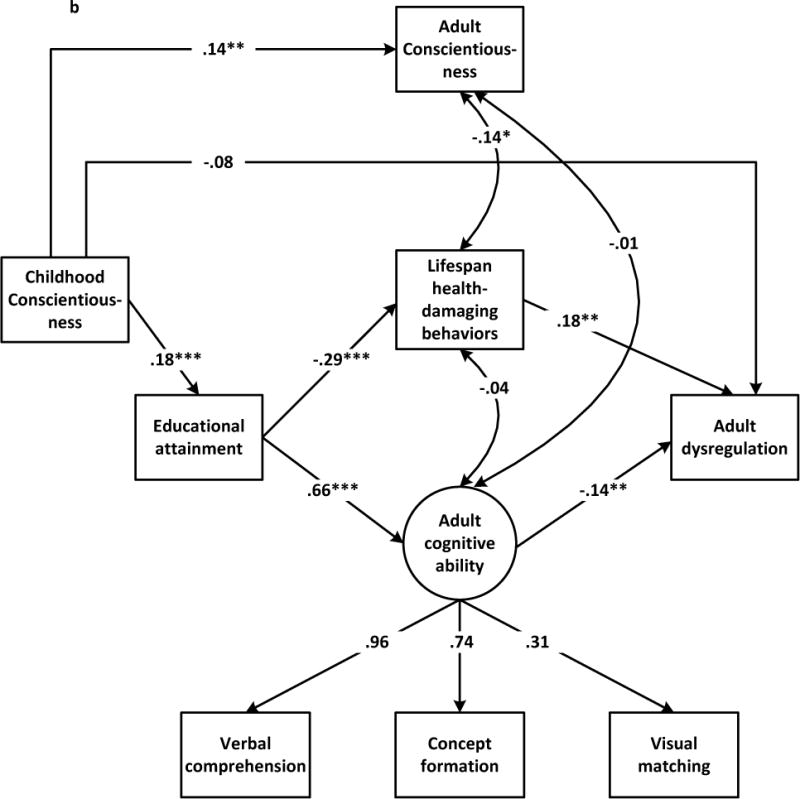
Figure 2.
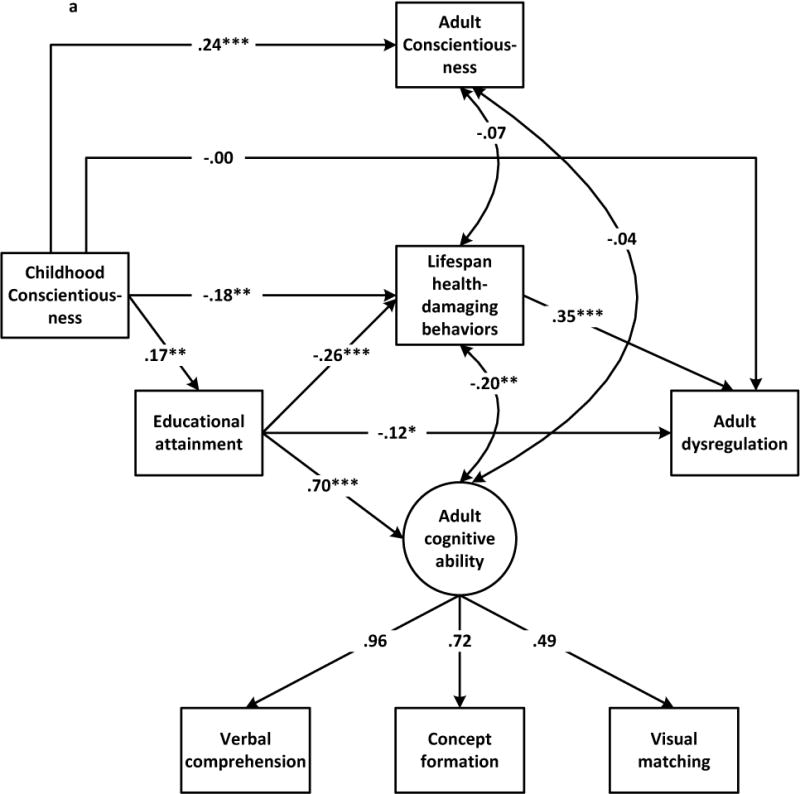
a. Path diagram showing standardized factor loading and regression weights for the trimmed model from men’s childhood Conscientiousness to adult dysregulation (N = 372). Fit statistics for the trimmed model: χ2 = 22.83, df = 11, p =.02, RMSEA = .05, 90% CI = .02, .08, CFI =.98; for the initial model: χ2 = 19.07, df = 9, p =.02, RMSEA = .06, 90% CI = .02, .09, CFI =.98.
b. Path diagram showing standardized factor loading and regression weights for the trimmed model from women’s childhood Conscientiousness to adult dysregulation (N = 387). Fit statistics for the trimmed model: χ2 = 26.78, df = 13, p =.01, RMSEA = .05, 90% CI = .02, .08, CFI =.98; for the initial model: χ2 = 21.48, df = 9, p =.01, RMSEA = .06, 90% CI = .03, .09, CFI =.98.
Table 3.
Standardized Direct and Indirect Effects
| Indirect path | Effect | p value | 95% CI |
|---|---|---|---|
| Men | |||
| C→Adult C | .238 | .000 | .140, .336 |
| C→EA | .170 | .001 | .070, .270 |
| C→LHDB | −.181 | .003 | −.299, −.181 |
| EA→LHDB | −.256 | .000 | −.383, −.128 |
| EA→Cog Ability | .697 | .000 | .632, .763 |
| EA→Dysreg | −.123 | .027 | −.232, −.014 |
| LHDB→Dysreg | .352 | .000 | .216, .488 |
| C→EA→LHDB | −.043 | .016 | −.080, −.007 |
| C→LHDB→Dysreg | −.064 | .029 | −.120, −.007 |
| C→EA→LHDB→Dysreg | −.015 | .046 | −.030, −.000 |
| C→EA→Dysreg | −.021 | .086 | −.043, .001 |
| Women | |||
| C→Adult C | .145 | .004 | .046, .244 |
| C→EA | .178 | .000 | .079, .276 |
| EA→LHDB | −.292 | .000 | −.408, −.292 |
| EA→Cog Ability | .662 | .000 | .592, .732 |
| LHDB→Dysreg | .179 | .004 | .057, .301 |
| Cog Ability→Dysreg | −.137 | .011 | −.243, −.032 |
| C→EA→LHDB | −.052 | .006 | −.089, −.015 |
| C→EA→Cog Ability→Dysreg | −.016 | .012 | −.029, −.004 |
| C→EA→LHDB→Dysreg | −.009 | .134 | −.021, .003 |
Note. C = childhood Conscientiousness; Adult C = adult Conscientiousness; EA = educational attainment; LHDB = lifespan health-damaging behavior; Dysreg = dysregulation
For women, the indirect path from childhood Conscientiousness to dysregulation through educational attainment and health-damaging behaviors was not significant. However, the indirect effect of Conscientiousness on dysregulation through cognitive ability was significant: higher Conscientiousness was related to higher educational attainment, which was associated with greater cognitive ability, which was associated with less dysregulation.
Discussion
This study examined a cumulative lifespan health behavior mechanism to account for associations between childhood Conscientiousness and adult health status. The primary finding was that the models for both men and women included paths between constructs suggestive of a chain of influence from childhood Conscientiousness through lifespan health-damaging behaviors to adult dysregulation. Our findings suggest that the association between childhood Conscientiousness and mortality found in previous studies could be explained in part by cumulative behavioral mechanisms leading to poorer health in adulthood that impacts longevity. A test of this complete pathway will eventually be possible with the Hawaii cohort.
The indirect path from childhood Conscientiousness to health-damaging behavior through educational attainment was significant for both genders, as was the path from health-damaging behavior to dysregulation. The entire indirect path from childhood Conscientiousness through educational attainment and health damaging behaviors to dysregulation was significant for men but not women. Men in this sample had higher mean levels of dysregulation than women, indicating that they were in poorer cardiovascular and metabolic health. On average, women develop cardiovascular disease 10 or more years later than men (Rossouw, 2002), so it is possible that the entire indirect effect for women may become stronger after an additional ten years of cumulative lifespan health-damaging behaviors and when their cardiovascular and metabolic health has deteriorated further. The 10-year follow-up clinical health assessment at mean age 61 that has just begun for the Hawaii cohort will enable us to test this possibility.
The present findings suggest that educational attainment is an important element in lifespan behavioral pathways to health status. It is well-established that higher levels of education reduce the likelihood of health-damaging behaviors such as smoking (Pampel, Krueger, & Denney, 2010), and education may increase knowledge and understanding of health-enhancing behaviors and their importance for disease prevention and management. Better educated individuals may be more likely to recognize disease symptoms and to obtain medical care (Glied & Lleras-Muney, 2008; Gottfredson, 2004), and to enjoy other benefits of higher socio-economic status, which may also account for the direct effect of educational attainment on dysregulation for men.
The present study also suggests the importance of cognitive ability for pathways from personality to health. For women, but not men, childhood Conscientiousness predicted dysregulation through educational attainment and cognitive ability. This finding for women is consistent with a previous study of adults, in which cognitive ability partially mediated the effects of adult Conscientiousness on mortality (Hill et al., 2011). However, it is not clear why the model for men did not show a comparable effect.
The present study also has broader implications for lifespan research on personality and health. Socioeconomic disparities in mortality disappear by the time people reach their 80’s, presumably because by this age prevention and treatment cannot delay inevitable biological aging (Phelan, Link, Diez-Roux, Kawachi, & Levin, 2004). A comparable question may be asked regarding disparities relating to personality traits (Shanahan et al., 2014). At what age do health advantages accruing to those with higher Conscientiousness no longer hold? The present study suggests that childhood Conscientiousness continues to confer health advantages at least up to the fifties. Adult Conscientiousness did not predict dysregulation beyond childhood Conscientiousness. Change in Conscientiousness had no effects on health in the present study, but the association between personality change over shorter periods and health outcomes should be examined in future research. Traits in childhood may have long-lasting consequences by directing individuals onto paths to adult development that include educational attainment, maintenance of cognitive ability, and habitual behaviors. In this way, the downstream effects of childhood personality can be independent of adult personality traits, which are only modestly correlated at best with childhood traits over time spans as long at 40 years (Edmonds et al., 2013). In future research, it would be useful to determine the generality of the present findings, but few studies have assessments of childhood personality, adult personality, and health outcomes. It would be valuable to learn more about how the pathways from early personality to later health are established, for example by examining child or adolescent personality influences on the formation and maintenance of health habits.
Inevitably, this study has limitations. The measure of lifespan health-damaging behaviors was limited to smoking, physical inactivity, and BMI. Other important health behaviors to include would be alcohol and other substance use, and health care utilization, but these lifetime data were not available for this cohort. BMI is only an indirect measure of behaviors related to an imbalance between caloric intake versus expenditure, and gives no indication of quantity or quality of food intake. More direct measures of dietary habits would be preferable. BMI is also somewhat confounded with physical activity. Ideally, health behaviors would be measured at regular time points across the lifespan instead of retrospectively. The retrospective index only approximated a measure of accumulating risk over the lifespan. Cognitive ability was first assessed at mean age 51 in this cohort. Because educational attainment is typically achieved prior to this age, we placed educational attainment as causally prior to cognitive ability in our models. Although cognitive ability remains relatively stable across the lifespan, the direction of association between educational attainment and ability is likely to be reciprocal and dependent on many other contextual factors (Deary et al., 2010). Treating ability at age 51 as the consequence of educational attainment remained faithful to the temporal ordering of the assessment of these variables in this study, and the likelihood that educational attainment is completed well before age 51 for most people, but may have oversimplified the actual association between them. With only one assessment of health outcomes, it was not possible to determine when in the lifespan the effects of cumulative health-damaging behaviors can be first observed. This information would be valuable for identifying optimal time points for interventions, and for the further investigation of the likely complex and reciprocal relations among personality, health behaviors, and health in adulthood. While the childhood personality assessment preceded the adult assessments by at least four decades, the ordering of the adult assessments corresponded less well to the temporal hypotheses.
Only modest amounts of variance were accounted for by the models, and the indirect effects were small. It is important to keep in mind the size of the raw bivariate correlation between childhood Conscientiousness and dysregulation (r = −.13 and −.10 for women and men, respectively), which necessarily limits the size of indirect effects. Numerous factors other than those studied here influenced health outcomes across 40 years. Seen in this light, the identification of any significant indirect effects over such a long period is remarkable. Despite calls for research on lifespan mechanisms to explain associations between personality and health (Friedman, 2000; Hampson & Friedman, 2008; Smith, 2006) there have been few studies to attempt this. The present study identified modest indirect effects pointing to possible underlying lifespan mechanisms, which may be seen as a valuable initial contribution to this sparse literature.
Despite these and other limitations, the main novel contribution made by this study to the field of personality and health has been to investigate a lifespan behavioral mechanism that unfolds over time periods measured in decades, not months. Future longitudinal studies will shed more light on the complex processes linking personality to subsequent health outcomes. Investigating pathways linking childhood personality with later biomarkers of cardiovascular and metabolic health may identify opportunities to disrupt unhealthy trajectories leading to morbidity and mortality.
Supplementary Material
Acknowledgments
This research was supported by a grant R01AG20048 from the National Institute on Aging of the National Institutes of Health. The authors thank Benjamin P. Chapman, Karen A. Matthews, and Howard Friedman for their comments on an earlier draft.
Footnotes
Other weight items were: comparison of weight to peers (1 = much lighter, 5 = much heavier); self-reported waist size; and body type (Bhuiyan, Gustat, Srinivasan, & Berenson, 2003) at ages 20, 30, and 40. Separately by gender, BMI was predicted for cases with valid measures of BMI, and those regression weights were applied to the valid predictors to compute the missing BMI. Fewer than 8% of cases were imputed, and the means with the imputed values included were within .05 of the means before imputing.
Including medication use as a predictor of dysregulation made no appreciable difference to the pattern of results reported here.
Educational attainment was missing for 60 participants, and 6 were missing cognitive ability. Scores on all three components of lifespan health-damaging behavior were required resulting in 301 missing cases. When the trimmed models were rerun excluding these160 men and 141 women, the path coefficient were comparable in size and sign (see online supplementary materials).
Contributor Information
Sarah E. Hampson, Oregon Research Institute, Eugene, Oregon
Grant W. Edmonds, Oregon Research Institute, Eugene, Oregon
Lewis R. Goldberg, Oregon Research Institute, Eugene, Oregon
Joan P. Dubanoski, Kaiser Permanente Center for Health Research Hawaii, Honolulu, Hawaii
Teresa A. Hillier, Kaiser Permanente Center for Health Research Hawaii, Honolulu, Hawaii
References
- Bhuiyan AR, Gustat J, Srinivasan SR, Berenson GS. Differences in body shape representations among young adults from a biracial (black-white), semirural community: The Bogalusa Heart Study. American Journal of Epidemiology. 2003;158:792–797. doi: 10.1093/aje/kwg218. [DOI] [PubMed] [Google Scholar]
- Bogg T, Roberts BW. Conscientiousness and health-related behaviors: A meta-analysis of the leading behavioral contributors to mortality. Psychological Bulletin. 2004;130:887–919. doi: 10.1037/0033-2909.130.6.887. [DOI] [PubMed] [Google Scholar]
- Bogg T, Roberts BW. The case for conscientiousness: Evidence and implications for a personality trait marker of health and longevity. Annals of Behavioral Medicine. 2013;45:278–288. doi: 10.1007/s12160-012-9454-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bollen KA, Stine R. Direct and indirect effects: Classical and bootstrap estimates of variability. Sociological Methodology. 1990;20:115–140. doi: 10.2307/271084. [DOI] [Google Scholar]
- Calvin C, Deary I, Fenton C, Roberts B, Der G, Leckenby N, Batty G. Intelligence in youth and all-cause-mortality: Systematic review with meta-analysis. International Journal of Epidemiology. 2011;40:626–644. doi: 10.2307/271084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deary IJ, Weiss A, Batty G. Intelligence and personality as predictors of illness and death: How researchers in differential psychology and chronic disease epidemiology are collaborating to understand and address health inequalities. Psychological Science in the Public Interest. 2010;11:53–79. doi: 10.1177/1529100610387081. [DOI] [PubMed] [Google Scholar]
- Duckworth AL, Quinn PD, Tsukayama E. What No Child Left Behind leaves behind: The roles of IQ and self-control in predicting standardized achievement test scores and report card grades. Journal of Educational Psychology. 2012;104:439–451. doi: 10.1037/a0026280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Edmonds GW, Goldberg LR, Hampson SE, Barckley M. Personality stability from childhood to midlife: Relating teachers’ assessments in elementary school to observer- and self-ratings 40 years later. Journal of Research in Personality. 2013;47:505–513. doi: 10.1016/j.jrp.2013.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman H. Long-term relations of personality and health: Dynamisms, mechanisms, tropisms. Journal of Personality. 2000;68:1089–1108. doi: 10.1111/1467-6494.00127. [DOI] [PubMed] [Google Scholar]
- Friedman HS, Kern ML. Personality, well-being, and health. Annual Review of Psychology. 2014;65:719–742. doi: 10.1146/annurev-psych-010213-115123. [DOI] [PubMed] [Google Scholar]
- Friedman HS, Tucker JS, Schwartz JE, Martin LR, Tomlinson-Keasey C, Wingard DL, Criqui MH. Childhood conscientiousness and longevity: Health behaviors and cause of death. Journal of Personality and Social Psychology. 1995;68:696–703. doi: 10.1037//0022-3514.68.4.696. [DOI] [PubMed] [Google Scholar]
- Friedman H, Tucker J, Tomlinson-Keasey C, Schwartz J, Wingard D, Criqui M. Does childhood personality predict longevity? Journal of Personality and Social Psychology. 1993;65:176–185. doi: 10.1037//0022-3514.65.1.176. [DOI] [PubMed] [Google Scholar]
- Glied S, Lleras-Muney A. Technological innovation and inequality in health. Demography. 2008;45:741–761. doi: 10.1353/dem.0.0017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldberg LR. Analyses of Digman’s child personality data: Derivation of Big Five factor scores from each of six samples. Journal of Personality. 2001;69:709–743. doi: 10.1111/1467-6494.695161. [DOI] [PubMed] [Google Scholar]
- Gottfredson LS. Intelligence: Is it the epidemiologists’ elusive “fundamental cause” of social class inequalities in health? Journal of Personality and Social Psychology. 2004;86:174–199. doi: 10.1037/0022-3514.86.1.174. [DOI] [PubMed] [Google Scholar]
- Hagger-Johnson G, Sabia S, Nabi H, Brunner E, Kivimaki M, Shipley M, Singh–Manoux A. Low conscientiousness and risk of all-cause, cardiovascular and cancer mortality over 17 years: Whitehall II cohort study. Journal of Psychosomatic Research. 2012;73:98–103. doi: 10.1016/j.jpsychores.2012.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hagger-Johnson GE, Shickle DA, Deary IJ, Roberts BA. Direct and indirect pathways connecting cognitive ability with cardiovascular disease risk: Socioeconomic status and multiple health behaviors. Psychosomatic Medicine. 2010;72:777–785. doi: 10.1097/PSY.0b013e3181ebf064. doi:01.10.2010. [DOI] [PubMed] [Google Scholar]
- Hampson SE, Edmonds GW, Goldberg LR, Dubanoski JP, Hillier TA. Childhood conscientiousness relates to objectively measured adult physical health four decades later. Health Psychology. 2013;32:925–928. doi: 10.1037/a0031655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hampson SE, Friedman HS. Personality and health: A lifespan perspective. In: John OP, Robins R, Pervin L, editors. The handbook of personality: Theory and research. 3. New York: Guilford; 2008. pp. 770–794. [Google Scholar]
- Hampson SE, Goldberg LR, Vogt TM, Dubanoski JP. Forty years on: Teachers’ assessments of children’s personality traits predict self-reported health behaviors and outcomes at midlife. Health Psychology. 2006;25:57–64. doi: 10.1037/0278-6133.25.1.57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hampson SE, Goldberg LR, Vogt TM, Dubanoski JP. Mechanisms by which childhood personality traits influence adult health status: Educational attainment and healthy behaviors. Health Psychology. 2007;26:121–125. doi: 10.1037/0278-6133.26.1.121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hampson SE, Goldberg LR, Vogt TM, Hillier TA, Dubanoski JP. Using physiological dysregulation to assess global health status: Associations with self-rated health and health behaviors. Journal of Health Psychology. 2009;14:232–241. doi: 10.1177/1359105308100207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hill PL, Turiano NA, Hurd MD, Mroczek DK, Roberts BW. Conscientiousness and longevity: An examination of possible mediators. Health Psychology. 2011;30:536–541. doi: 10.1037/a0023859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. doi: 10.1080/10705519909540118. [DOI] [Google Scholar]
- John OP, Srivastava S. The Big Five trait taxonomy: History, measurement, and theoretical perspectives. In: Pervin LA, John OP, editors. Handbook of personality: Theory and research. 2. New York: Guilford Press; 1999. pp. 102–138. [Google Scholar]
- Jokela M, Batty GD, Nyberg ST, Virtanen M, Nabi H, Sing-Manoux A, Kivimaki M. Personality and all-cause mortality: Individual-participant meta-analysis of 3,947 deaths in 76,150 adults. American Journal of Epidemiology. 2013;178:667–675. doi: 10.1093/aje/kwt170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kern ML, Friedman HS. Do conscientious individuals live longer? A quantitative review. Health Psychology. 2008;27:505–512. doi: 10.1037/0278-6133.27.5.505. [DOI] [PubMed] [Google Scholar]
- Lodi-Smith JL, Jackson JJ, Bogg T, Walton K, Wood D, Harms PD, Roberts BW. Mechanisms of health: Education and health-related behaviors partially mediate the relationship between conscientiousness and self-reported physical health. Psychology and Health. 2010;25:305–319. doi: 10.1080/08870440902736964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lönnqvist J, Vainikainen M, Verkasalo M. Teacher and parent ratings of seven‐year‐old children’s personality and psychometrically assessed cognitive ability. European Journal of Personality. 2012;26:504–514. doi: 10.1002/per.849. [DOI] [Google Scholar]
- Martin LR, Friedman HS, Schwartz JE. Personality and mortality risk across the life span: The importance of conscientiousness as a biopsychosocial attribute. Health Psychology. 2007;26:428–436. doi: 10.1037/0278-6133.26.4.428. [DOI] [PubMed] [Google Scholar]
- Moffitt TE, Arseneault L, Belsky D, Dickson N, Hancox RJ, Harrington H, Houts R, Poulton R, Roberts BW, Ross S, Sears MR, Thomson WM, Caspi A. A gradient of childhood self-control predicts health, wealth, and public safety. Proceedings of the National Academy of Sciences. 2011;108:2693–2698. doi: 10.1073/pnas.1010076108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States. Journal of the American Medical Association. 2004;291:1238–1245. doi: 10.1001/jama.291.10.1238. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide. 7. Los Angeles, CA: Muthén & Muthén; 1998–2012. [Google Scholar]
- Pampel F, Krueger P, Denney J. Socioeconomic disparities in health behaviors. Annual Review of Sociology. 2010;36:349–370. doi: 10.1146/annurev.soc.012809.102529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phelan JC, Link BG, Diez-Roux A, Kawachi I, Levin B. “Fundamental causes” of social inequalities in mortality: A test of the theory. Journal of Health and Social Behavior. 2004;45:265–285. doi: 10.1177/002214650404500303. [DOI] [PubMed] [Google Scholar]
- Rossouw J. Hormones, genetic factors, and gender differences in cardiovascular disease. Cardiovascular Research. 2002;53:550–557. doi: 10.1016/S0008-6363(01)00478-3. [DOI] [PubMed] [Google Scholar]
- Shanahan MJ, Hill PL, Roberts BW, Eccles J, Friedman HS. Conscientiousness, health, and aging: The life course of personality model. Developmental Psychology. 2014;50:1407–1425. doi: 10.1037/a0031130. [DOI] [PubMed] [Google Scholar]
- Shrout PE, Bolger N. Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychological Methods. 2002;7:422–445. doi: 10.1037//1082-989X.7.4.422. [DOI] [PubMed] [Google Scholar]
- Smith T. Personality as risk and resilience in physical health. Current Directions in Psychological Science. 2006;15:227–231. doi: 10.1111/j.1467-8721.2006.00441.x. [DOI] [Google Scholar]
- Ten Berge JMF, Hofstee WK. Coefficient alpha and reliabilities of unrotated and rotated components. Psychometrika. 1999;64:83–90. doi: 10.1007/BF02294321. [DOI] [Google Scholar]
- Turiano N, Chapman B, Gruenewald T, Mroczek D. Personality and the leading behavioral contributors of mortality. Health Psychology. 2013 doi: 10.1037/hea0000038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turiano NA, Hill PL, Roberts BW, Spiro A, Mroczek DK. Smoking mediates the effect of conscientiousness on mortality: The Veterans Affairs Normative Aging Study. Journal of Research in Personality. 2012;46:719–724. doi: 10.1016/j.jrp.2012.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services. The health consequences of smoking: A report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004. [Google Scholar]
- Woodcock RW, Mather N, McGrew KS. Woodcock–Johnson III tests of cognitive abilities examiner’s manual. Itasca, IL: Riverside; 2001. [Google Scholar]
- Woods SA, Hampson SE. Predicting adult occupational environments from gender and childhood personality traits. Journal of Applied Psychology. 2010;95:1045–1057. doi: 10.1037/a0020600. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.