

Abstract
Background:
Hypodontia is often used as a collective term for congenital absence of primary or secondary teeth, although specifically it describes the absence of one to six teeth excluding third molars. The prevalence of hypodontia varies from 0.03 to 10.1% in various populations.
Materials and Methods:
In this retrospective study, we reviewed the records of Turkish orthodontic patients treated between 1994 and 2003. A total of 1236 orthodontic patients (507 girls, 729 boys) were included in this study. The age of the patients ranged from 11 to 20 years. Data were collected and entered into the SPSS 20 program for statistical analysis. The Chi-square test was used to analyze differences in the distribution of hypodontia, sex, and malocclusion type.
Results:
In the total sample of 1236 patients who were orthodontically treated, hypodontia was found in 82 children, including 45 girls and 37 boys. The prevalence of hypodontia was 7%. Patients with more severe hypodontia showed a tendency to exhibit a class II relationship. The mandibular second premolar were the most commonly missing teeth in 48 girls and 26 boys.
Conclusion:
Hypodontia may lead to some clinical problems including malocclusions, esthetic and functional complaints, and also psychological problems. All cases should be evaluated by an interdisciplinary approach for appropriate treatment choice. Our data emphasize the importance of detailed and careful radiographic examination. This helps in long-term and effective treatment planning according to a child's individual requirements.
Keywords: Absence of third molar, non-syndromic hypodontia, orthodontic patient
INTRODUCTION
Hypodontia is often used as a collective term for congenital absence of primary or secondary teeth, although specifically it describes the absence of one to six teeth excluding third molars. Oligodontia refers to the absence of more than six teeth, excluding third molars. Dental agenesis affects more frequently the permanent dentition rather than the primary dentition.[1,2,3,4]
The etiology of hypodontia can be a combination of genetic and environmental factors, and it can occur as an isolated condition (non-syndromic hypodontia) or can be associated with a systemic condition or syndrome (syndromic hypodontia).[5,6,7] Hypodontia may detrimentally affect the aesthetics and function.[4,8,9,10]
Congenitally missing teeth may cause serious aesthetic, functional, emotional, and physical problems, especially during adolescence. Hypodontia usually requires complex treatments, ranging from single restorations to surgery and multiple restorations, associated with lifelong maintenance.[9,11]
The prevalence of hypodontia varies from 0.03 to 10.1% in various populations.[12] Some studies have reported the prevalence of hypodontia in the orthodontic patients.[2,13,14,15] and ranging from 2.7%[15] to 11.3%.[16] On the other hand, clinicians often claim that the prevalence of hypodontia has increased during recent decades.[12,17] The reason may be that the period of four decades is too short to investigate an evolutionary trend in the human dentition.
Despite numerous studies on hypodontia, there are limited comprehensive studies in the literature regarding hypodontia among Turkish children. Therefore, the aim of this study was to determine the frequency of hypodontia in orthodontically treated children and to determine the association between tooth size, gender, number of missing teeth, affected region, the upper or lower arch, the left or right side, and Angle's classification.
MATERIALS AND METHODS
In this retrospective study, we reviewed the records of Turkish orthodontic patients treated between 1994 and 2003.
All subjects had visited the orthodontic departments of the Schools of Dentistry of Marmara University Istanbul, Turkey. A total of 1236 orthodontic patients (507 girls, 729 boys) were included in this study. The age of the patients ranged from 11 to 20 years.
Hypodontia was recorded when a tooth was absent on the panoramic radiograph. Hypodontia was diagnosed if one to six teeth were absent. Children whose radiographs were not of diagnostic clarity were excluded. Children were excluded if they had any associated developmental anomalies (eg, ectodermal dysplasia, cleft lip or palate, and Down syndrome) and had no previous loss of teeth due to trauma, caries, periodontal disease, or orthodontic extraction or a history of orthodontic treatment.
The type of permanent missing teeth, the affected side, the jaw and the type of malocclusion were recorded. Based on the type of permanent missing teeth, the patient's gender and the affected side and jaw were also recorded. Panoramic views were used to confirm a diagnosis of hypodontia[18,19]
A total of 1236 subjects remained and were evaluated using dental casts and panoramic radiographs.
Statistical analysis
Data were collected and entered into the SPSS 20 program for statistical analysis (Statistical Package for Social Sciences, SPSS Inc., Chicago, IL, USA). The Chi-square test was used to analyze differences in the distribution of hypodontia, sex and malocclusion type. The level of significance was set at 5%.
RESULTS
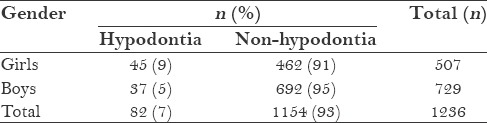
Of the total sample of 1236 patients (507 (41%)) were girls and 729 ((59%) were boys) who were orthodontically treated. Hypodontia was found in 82 children, including 45 girls (9%) and 37 boys (5%). The prevalence of hypodontia was 7%. The mean age of children was 17.05 years (SD = 2,5). There was significant difference between the prevalence of hypodontia in boys and girls (Chi-square = 6.972, P = 0.008). The distribution of patients by gender is shown in Table 1.
Table 1.
Distribution of hypodontia (%) by gender
As shown in Table 2, the distribution of malocclusion type (according to the Angle's classification) no difference between gender (Chi-square = 1.904 P = 0.592).
Table 2.
Distribution of malocclusion type (%) by gender
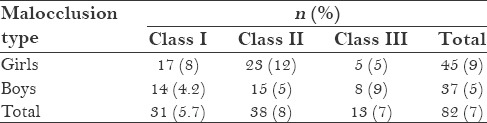
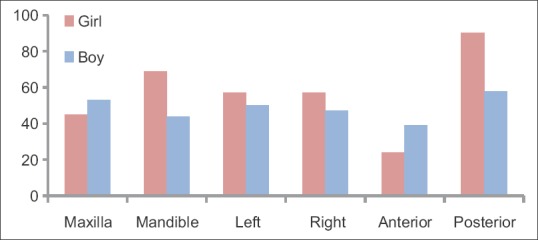
Patients with more severe hypodontia showed a tendency to class II relationship. The distribution of skeletal morphology in hypodontia and non-hypodontia patients is shown in Table 3. The prevalence of hypodontia was higher (8%) in patients with class II malocclusion. The lowest prevalence was seen among patients with class III malocclusion (5,7%). however, the distribution of malocclusion type (according to the Angle's classification) no differed in hypodontia patients (Chi-square = 1.576 P = 0.455). The frequency of hypodontia patients in those class I, class II, and class III malocclusion was 31 (17 girls and14 boys, 5.7%); 38 (23 girls and 15 boys, 8%), and 13 (5 girls and 8 boys, 7%) respectively [Figure 1].
Table 3.
Distribution of malocclusion type (%) in patients with and without hypodontia

Figure 1.
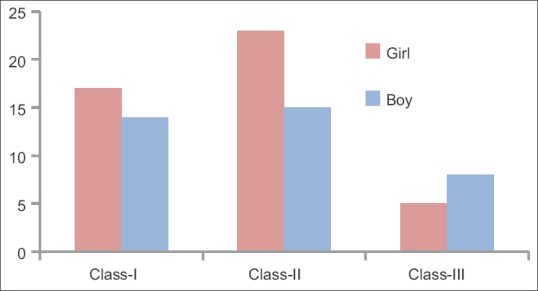
Distribution of malocclusion types in boys and girls
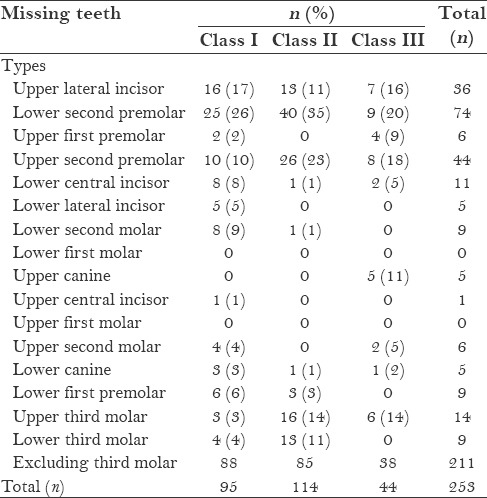
The relationship between the type of malocclusion and the number of missing teeth was determined [Table 4]. Table 5 shows the distribution of the patients by gender and the number of missing teeth.
Table 4.
Relationship between the number of missing teeth and Angle's classification
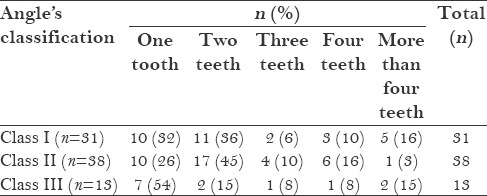
Table 5.
Distribution of the patients by gender and number of missing teeth

Overall, in both maxillary and mandibular arches, the mandibular second premolars were the most commonly missing teeth in 48 girls (42%) and 26 boys (27%). This was followed by maxillary second premolar in girls [27 (24%)] and maxillary lateral incisor in boys [24 (25%)].
The maxillary first and second molars, mandibular first molars, and maxillary central incisor in both arches showed no congenital absence in the sample of Turkish girls. The types of teeth without congenital absence were fewer in Turkish boys (just mandibular canines, maxillary and mandibular first molars). Hypodontia was more prevalent in the maxillary arch in boys (55%) than (39%) in girls. On the other hand, hypodontia was more prevalent in the mandibular arch in girls (61%) than in boys (45%). The distribution of missing teeth by location (maxillary or mandibular arch) is shown in Table 6.
Table 6.
Distribution of missing teeth according to location

A total of 211 teeth (excluding third molars) were missing (45 in girls and 37 in boys). There were 24 missing anterior teeth in girls, 39 missing anterior teeth in boys, and 90 and 58 missing posterior teeth in girls and boys, respectively. The majority of missing teeth [114 (54%)] were in girls.
In total, 57 (50%) teeth in girls and 47 (49%) in boys were absent on the right side and boys; 57(%50) and 50(%51) teeth were absent on the left side in girls and in boys, respectively. The majority of patients had one or two teeth missing, but rarely three or more were found missing [Table 6].
The prevalence of missing teeth was higher in the anterior segment (incisors and canines) than in the posterior segment (premolars and molars) in boys. But it was higher in the posterior segment in girls than in boys [Table 6, Figure 2].
Figure 2.
Location of the missing teeth
Mandibular second premolar was the most common missing tooth in class II (4%) than in class I (28%) and class III (24%) malocclusions. This was followed by upper second premolar in class II (31%) than in class III (21%) and class I (11%) malocclusions [Table 7].
Table 7.
Prevalence of missing teeth in different malocclusions
Bilateral hypodontia was observed in 72 teeth in class I (44%) and 30 teeth (18%) in class III malocclusions. Twenty-three unilaterally missing teeth (49%) were observed in class II, which was followed by 16 in class I (34%) and 8 in class III (17%) malocclusions [Table 8]. The percentage of patients with oligodontia was 0.32% (4 males), which yields a prevalence rate of 0.32%.
Table 8.
Prevalence of missing teeth in different types of malocclusions with respect to the affected jaw and side

In this study, congenital absence of the third molar was observed more frequently in the hypodontia group (17%) than in the non-hypodontia group (6%) [Table 9]. Congenital absence of third molar was higher in class 3 classification (24%) than in class 2 classification (23%) and class 1 classification (6%). On the other hand, the highest prevalence of congenital absence of third molar was class 3 classification in girls (60%) [Table 10].
Table 9.
Distribution of missing third molar and Angle's classification
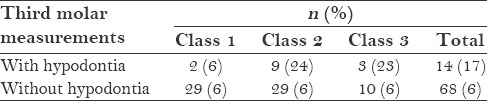
Table 10.
Relationship of Angle's classification and absence of third molar in boys and girls

DISCUSSION
The present study revealed the prevalence of hypodontia to be 7% in this sample of orthodontically treated children, excluding third molars. This frequency is higher than the 1.6–9.6% reported for a normal population, and while not being statistically significant, it is considerably lower than the 9.1 and 11.3% reported for orthodontically treated children in Iran[20] and Slovenia,[16] respectively. On the other hand, the prevalence in Mexican orthodontic patients was 2.7%,[14] which was lower than the prevalence observed in the present study.
Hypodontia was found more frequently in females than in males [Table 1]. Statistically significant differences have been found in some studies.[16] Most authors report a small but insignificant predominance of hypodontia in females.[21]
In our study, the prevalence of hypodontia was higher (8%) in patients with class II malocclusion than in those with class III malocclusion (5.7%). Another study[16] found higher prevalence of hypodontia in their class I study sample.
On the other hand, we found that the higher prevalence of hypodontia in patients with class III malocclusion can be partially explained by the fact that hypodontia was more prevalent in the maxilla (26%) than in the mandible (10%). Results of the other study were similar to our study.[20]
In this study, the mandibular second premolars were the most commonly missing teeth in 48 girls (42%) and 26 (27%) boys. Similarly, some studies[12,13,15] found that the most commonly missing tooth was the mandibular second premolar, followed by the maxillary lateral incisor and the maxillary second premolar. On the other hand, some studies[14,16,21] found a significantly higher incidence of missing maxillary lateral incisors.
Hypodontia was more prevalent in the maxillary arch in boys (55%) than in girls (39%), and was frequently found on the right side than on the left (50–(50%) in girls, 49-(51%) in boys). Some studies[16,21] was more prevalent in the maxilla than mandible.
In this study, the majority of patients had one or two teeth missing, similar to that reported in some studies.[16,21]
Bilateral hypodontia was more common than unilateral hypodontia in this study. Some other studies[4,14,15,22] also reported that missing teeth were mostly found bilaterally.
We found that congenital absence of the third molar more frequent in the hypodontia group than in the non-hypodontia group. Other studies[7,23] reported similar our results, wherein congenital absence of the third molar was strongly associated with hypodontia.
CONCLUSION
Hypodontia may lead to some clinical problems including malocclusions, esthetic and functional complaints, and also psychological problems. All cases should be evaluated by an interdisciplinary approach for appropriate treatment choice. Our data emphasize the importance of detailed and careful radiographic examination. This helps in long-term and effective treatment planning according to a child's individual requirements.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Shimizu T, Maeda T. Prevalence and genetic basis of tooth agenesis. Jpn Dent Sci Rev. 2009;45:52–8. [Google Scholar]
- 2.Altug-Atac AT, Erdem D. Prevalence and distribution of dental anomalies in orthodontic patients. Am J Orthod Dentofacial Orthop. 2007;131:510–4. doi: 10.1016/j.ajodo.2005.06.027. [DOI] [PubMed] [Google Scholar]
- 3.De Coster PJ, Marks LA, Martens LC, Huysseune A. Dental agenesis: Genetic and clinical perspectives. J Oral Pathol Med. 2009;38:1–17. doi: 10.1111/j.1600-0714.2008.00699.x. [DOI] [PubMed] [Google Scholar]
- 4.Goya HA, Tanaka S, Maeda T, Akimoto Y. An orthopantomographic study of hypodontia in permanent teeth of Japanese pediatric patients. J Oral Sci. 2008;50:143–50. doi: 10.2334/josnusd.50.143. [DOI] [PubMed] [Google Scholar]
- 5.Bergendal B. Oligodontia ectodermal dysplasia--on signs, symptoms, genetics, and outcomes of dental treatment. (13-78).Swed Dent J Suppl. 2010;205:7–8. [PubMed] [Google Scholar]
- 6.Mostowska A, Biedziak B, Jagodzinski PP. Novel MSX1 mutation in a family with autosomal-dominant hypodontia of second premolars and third molars. Arch Oral Biol. 2012;57:790–5. doi: 10.1016/j.archoralbio.2012.01.003. [DOI] [PubMed] [Google Scholar]
- 7.Zhu J, Yang X, Zhang C, Ge L, Zheng S. A novel nonsense mutation in PAX9 is associated with sporadic hypodontia. Mutagenesis. 2012;27:313–7. doi: 10.1093/mutage/ger080. [DOI] [PubMed] [Google Scholar]
- 8.Pemberton TJ, Das P, Patel PI. Hypodontia: Genetics and future perspectives. Braz J Oral Sci. 2005;4:695–709. [Google Scholar]
- 9.Nunn JH, Carter NE, Gillgrass TJ, Hobson RS, Jepson NJ, Meechan JG, et al. The interdisciplinary management of hypodontia: Background and role of paediatric dentistry. Br Dent J. 2003;194:245–51. doi: 10.1038/sj.bdj.4809925. [DOI] [PubMed] [Google Scholar]
- 10.Nik-Hussein NN. Hypodontia in the permanent dentition: A study of its prevalence in Malaysian children. Aust Orthod J. 1989;11:93–5. [PubMed] [Google Scholar]
- 11.Kokich VG, Kokich VO. Congenitally missing mandibular second premolars: Clinical options. Am J Orthod Dentofacial Orthop. 2006;130:437–44. doi: 10.1016/j.ajodo.2006.05.025. [DOI] [PubMed] [Google Scholar]
- 12.Mattheeuws N, Dermaut L, Martens G. Has hypodontia increased in Caucasians during the 20th century? A meta-analysis. Eur J Orthod. 2004;26:99–103. doi: 10.1093/ejo/26.1.99. [DOI] [PubMed] [Google Scholar]
- 13.Thongudomporn U, Freer TJ. Prevalence of dental anomalies in orthodontic patients. Aust Dent J. 1998;43:395–8. [PubMed] [Google Scholar]
- 14.Silva Meza R. Radiographic assessment of congenitally missing teeth in orthodontic patients. Int J Paediatr Dent. 2003;13:112–6. doi: 10.1046/j.1365-263x.2003.00436.x. [DOI] [PubMed] [Google Scholar]
- 15.Endo T, Ozoe R, Kubota M, Akiyama M, Shimooka S. A survey of hypodontia in Japanese orthodontic patients. Am J Orthod Dentofacial Orthop. 2006;129:29–35. doi: 10.1016/j.ajodo.2004.09.024. [DOI] [PubMed] [Google Scholar]
- 16.Fekonja A. Hypodontia in orthodontically treated children. Eur J Orthod. 2005;27:457–60. doi: 10.1093/ejo/cji027. [DOI] [PubMed] [Google Scholar]
- 17.Polder BJ, Van’t Hof MA, Van der Linden FP, Kuijpers-Jagtman AM. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol. 2004;32:217–26. doi: 10.1111/j.1600-0528.2004.00158.x. [DOI] [PubMed] [Google Scholar]
- 18.Peker I, Kaya E, Darendeliler-Yaman S. Clinical and radiographical evaluation of non-syndromic hypodontia and hyperdontia in permanent dentition. Med Oral Patol Oral Cir Bucal. 2009;14:e393–7. [PubMed] [Google Scholar]
- 19.Kazancı F, Celikoglu M, Yıldırım H, Ceylan I. Tooth agenesis code (TAC) values in a sample of orthodontic patient population. J Dent Fac Atatürk Uni. 2010;20:12–8. [Google Scholar]
- 20.Vahid-Dastjerdi E, Borzabadi-Farahani A, Mahdian M, Amini N. Non-syndromic hypodontia in an Iranian orthodontic population. J Oral Sci. 2010;52:455–61. doi: 10.2334/josnusd.52.455. [DOI] [PubMed] [Google Scholar]
- 21.Gomes RR, da Fonseca JA, Paula LM, Faber J, Acevedo AC. Prevalence of hypodontia in orthodontic patients in Brasilia, Brazil. Eur J Orthod. 2010;32:302–6. doi: 10.1093/ejo/cjp107. [DOI] [PubMed] [Google Scholar]
- 22.Sisman Y, Uysal T, Gelgor IE. Hypodontia. Does the prevalence and distribution pattern differ in orthodontic patients? Eur J Dent. 2007;1:167–73. [PMC free article] [PubMed] [Google Scholar]
- 23.Garn SM, Lewis AB, Vicinus JH. Third molar polymorphism and its significance to dental genetics. J Dent Res. 1963;42(Suppl):1344–63. doi: 10.1177/00220345630420061001. [DOI] [PubMed] [Google Scholar]