

Abstract
Background:
Work-related musculoskeletal pain is one of the occupational hazards in dentists. Aims: To find the prevalence and severity of musculoskeletal pain in dentists, to compare musculoskeletal pain among dentists practicing yoga, those practicing physical activities, and those without any physical activity, and also to know the effects of sex, age, and workload on musculoskeletal pain.
Materials and Methods:
A self-reporting work-related questionnaire and the Nordic questionnaire for analysis of musculoskeletal disorders were given to graduated dentists attending Indian dental conference in Mumbai, to know the musculoskeletal pain experienced in the last 12 months and feedback was obtained from 220 dentists.
Results:
The prevalence of musculoskeletal pain in dentists was 34.5%. Prevalence of musculoskeletal pain was 10.5%, 21.7%, and 45.6% in dentists with regular yoga practice, other physical activity, and no physical activity, respectively. There was statistically significant difference in the prevalence of musculoskeletal pain among dentists who were practicing yoga when compared with those in no regular activity group.
Conclusion:
Within the limitations of the study, there was significant role of physical activity on the quality and quantity of work-related musculoskeletal disorders experienced by dentists. Yoga was found to be more effective than other modes of physical activities. More research is needed on musculoskeletal problems in dentists, with an emphasis on larger sample sizes and correlating other factors like age and sex of the dentists, duration of practice, years of practicing yoga, and working hours per week.
Keywords: Dentists, musculoskeletal pain, yoga
INTRODUCTION
Work-related musculoskeletal disorders (MSDs) are one of the most important occupational health issues in healthcare workers. Musculoskeletal pain can be an occupational health problem for medical professionals, particularly dentists, who sit in static postures using precision hand and wrist movements.[1]
Majority of dentists (87.2%) suffer from at least one symptom of musculoskeletal diseases at some point in their life.[2] Patients with occupational diseases have not only physical, psychological, and social consequences, but also economic and security impact when they reach a level of severity that directly affects the work capacity, causing absences and early retirement.[3]
A number of studies have found that the mechanisms leading to work-related musculoskeletal pain are multifactorial. This pain can be attributed to numerous risk factors including prolonged static postures, repetitive movements, suboptimal lighting, poor positioning, genetic predisposition, mental stress, physical conditioning, and age.[4,5]
Basic operating posture is considered an important occupational health issue for oral health care clinicians. It is generally agreed that the physical posture of the operator, while providing care, should be such that all muscles are in a relaxed, well-balanced, and neutral position. Postures outside of this neutral position are likely to cause musculoskeletal discomfort.[5]
There is some evidence for the effectiveness of strengthening exercises in reducing work-related MSDs. There is also a growing interest in the use of stretching exercises to reduce the risk of work-related MSDs.[6,7]
Yoga is an ancient system of relaxation, exercise, and healing that has origins in Indian philosophy. As a system of healing, it takes a primary approach of prevention or keeping oneself well by the daily practice. Yoga is often practiced by healthy individuals with the aim to achieve relaxation, fitness, and a healthy lifestyle. Yoga has also been recommended and used for a variety of medical conditions.[8]
The practice of yoga in the Indian subcontinent has been documented as early as 3000 BC. Yoga is a science of the mind and soul. Many researchers have found that yoga is effective for relieving stress and anxiety conditions that impact many physical and mental health conditions.[8]
Dentists are among the group of professionals who have been increasingly referred for physical therapy and seeking ergonomic advice in the recent past. There is a scope for further decreasing the prevalence and severity of these disorders by performing regular specific exercises. In most of the studies, the dentists are reported to be relatively inactive and very few perform some form of physical activity and acknowledge the benefits of the same. Musculoskeletal complaints have a significant negative impact on the self-reported general health of dentists. The best ergonomic working principles should be taught to the students, and dental schools should provide a comfortable working environment to those practicing dentistry.[9]
The aims and objectives of this study were to find out the prevalence and severity of musculoskeletal pain in dentists, to compare musculoskeletal pain among dentists practicing yoga, those practicing other physical exercises, and those without any physical exercise, and also to know the effects of sex, age, and workload on musculoskeletal pain.
MATERIALS AND METHODS
Participants
The study was conducted on 150 male and 150 female dentists of age from 30 to 70 years, who attended the 65th Indian Dental Association conference in Mumbai on February 9–12, 2012.
Study design
The design of the study is presented in Figure 1. Dentists with minimum of 8 years of clinical practice and 30 practicing hours per week were considered for this study. Dentists practicing either yoga (under the supervision of a qualified yoga master) or some other physical activity like brisk walking, jogging, or aerobics, for a period of more than 1 year and a minimum of four times in a week for at least 1 h per day were considered as the group with some physical activity. Other dentists were considered as the group with no physical activity. Dentists with any systemic disease that can influence the musculoskeletal system, such as arthritis, osteoporosis, uncontrolled diabetes, and any neurological disorders, were not considered for evaluation.
Figure 1.
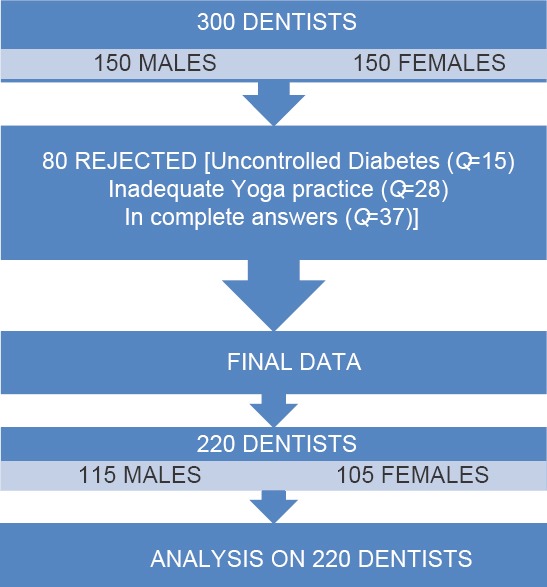
Design for the study
Data extraction
Informed consent was obtained from the participants after explaining the purpose of the study to them. A self-reporting work-related questionnaire, which was pre-tested for its relevance among 10 dentists.[10] The Nordic questionnaire for analysis of MSDs and an information sheet were given to the 300 dentists. Information on MSDs was collected, including information on the location of MSDs’ symptoms in the past 12 months, whether it interfered with daily activities, and whether medical treatment had been sought in the previous 12 months. The dentists were also asked whether they had taken sick leave for their pain in the previous 12 months and, if so, how many days of leave they had taken. Multiple choice and “fill in the blank” style questions were used throughout. Further clarification was given to those dentists who did not fully understand the questionnaire. Additional information was requested on age, gender, number of years since graduation, field of dental practice, and number of hours worked per week.
Assessment
Intensity of pain was assessed by a 0–10 numeric Pain Rating Scale (0: No pain; 1–3: Mild pain; 4–6: Moderate pain; 7–10: Severe pain), irrespective of the location of pain. In cases of mild pain, dentists did not take any medication. In cases of moderate pain, they used analgesics for a day, whereas in cases of severe pain, they used medication for more than a day and sometimes even hospitalization and bed rest was needed.
Data analysis
The data were entered into Statistical Package for Social Sciences (SPSS) version 16 software (Chicago IL, USA) and statistically analyzed with Kruskal–Wallis (H) test, Z test for two proportions, and Chi-Square test. As and when it was necessary, pooling technique was adapted because of smaller units.
RESULTS
A total of 80 feedback forms were rejected because 15 had poorly controlled diabetes, 28 were practicing yoga or any other physical activity for a period of less than 1 year, and the remaining 37 had incomplete answers. Final data collected from 220 dentists were considered for evaluation, of which 105 were from females and 115 from males.
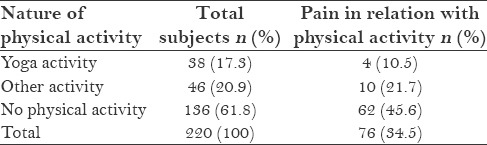
The data of prevalence of musculoskeletal pain in relation to physical activity among dentists is given in Table 1. Among 220 dentists, 76 had musculoskeletal pain with different intensities in the last 12 months, making the prevalence 34.5%. About 61.82% of the dentists (136) did not practice any physical activity on a regular basis, 17.27% (38) were practicing yoga, and 20.91% (46) were practicing some other type of physical activities. The prevalence of musculoskeletal pain in dentists practicing yoga was 10.5%, and it was 21.7% in those dentists practicing some sort of physical activity. The prevalence of musculoskeletal pain in dentists without any regular physical activity was 45.6%. Majority of the dentists experienced pain in the neck and lower back regions.
Table 1.
Data of prevalence of musculoskeletal pain among dentists in relation with their physical activity
There was a statistically significant difference (P < 0.05) between the type of pain experienced by dentists with yoga practice [Table 2], with other physical activity, and without any physical activity [Kruskal–Wallis (H) test value = 8.844, P = 0.031].
Table 2.
Comparison of type of musculoskeletal pain in relation with dentists’ physical activity

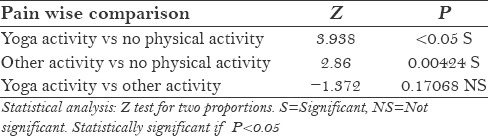
We also investigated the role of yoga activity in musculoskeletal pain [Table 3]. We found statistically significant difference between prevalence of pain among dentists who were practicing yoga (Z test value = 3.938, P < 0.05) when compared with those in no regular physical activity group. We found statistically significant differences (P < 0.05) between musculoskeletal pain experienced by dentists without any physical activity and those with any other physical activity (Z test value = 2.86, P = 0.00424). There was no statistically significant difference between the prevalence of pain in dentists who were practicing yoga and those who were practicing other physical activity (Z test = −1.372, P = 0.17068), which proved the null hypothesis.
Table 3.
Pain wise comparison between dentists in relation with their physical activity
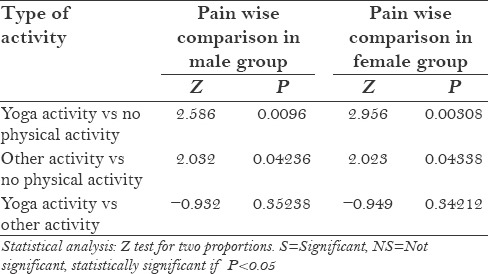
A similar trend was found in the musculoskeletal pain experienced by both male and female dentists [Table 4]. We found statistically significant difference in the prevalence of pain among dentists who were practicing yoga (Z test value = 2.586, P = 0.0096 in males; Z test value = 2.956, P = 0.00308 in females) when compared with those in no regular physical activity group.
Table 4.
Musculoskeletal pain wise comparison in male and female dentist groups in relation with their physical activity
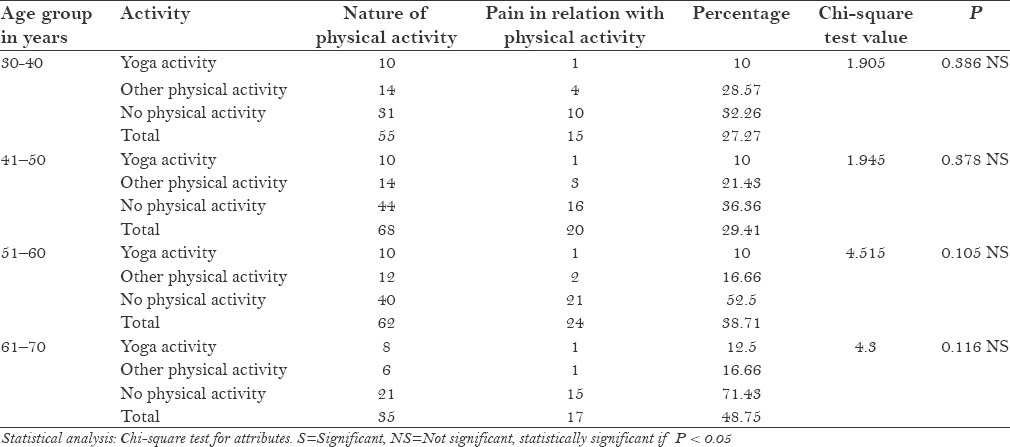
With increase in age [Table 5] (mean age 48.3 years), there was an increase in prevalence of musculoskeletal pain experienced by dentists (Chi-square test), with no statistically significant difference found in the prevalence of musculoskeletal pain among dentists of different age groups.
Table 5.
Comparison of MSD pain between dentists of different age groups in relation with their physical activity
DISCUSSION
Dentistry is one of the professions that demands prolonged static position with limited mobility. The static forces resulting from these postures have been shown to be much more tasking than dynamic forces. Repeated prolonged static postures resisting gravity during their work are thought to initiate a series of events that could account for pain and injuries. Sometimes career-ending problems are seen in dentists because of these MSDs.[11] Though there are case reports on the dentists suffering from work-related musculoskeletal pain, only limited studies have been published regarding the prevalence of work-related musculoskeletal pain among Indian dentists.
In our study, the prevalence of pain was 34.5% (n = 76) among dentists, with a majority of them having mild (n = 41, 18.6%) or moderate (n = 32, 14.5%) pain and very few (n = 3, 1.4%) suffering from severe pain. This is lesser than the prevalence of musculoskeletal pain reported among Italian (54%)[12] and Greek (62%)[13] dentists. This difference might be due to the differences in perception of musculoskeletal pain, type of clinical practice, nature of physical activities, and other non-standardized variables.
There was not much difference in the prevalence of pain experienced by male (35.65%) and female dentists (33.33%) as a whole. A similar trend was observed in pain prevalence between both genders irrespective of their physical activity, with the highest prevalence found among dentists without any physical activity (males 45.8%, females 45.3%) and the lowest prevalence found in dentists with regular yoga practice (males 11.8%, females 9.5%). Though gender wise there was no difference, these observations emphasize the role of yoga in minimizing musculoskeletal pain.
Increased prevalence of pain was found with increase in age.[14] In our study, there was a little difference in prevalence of pain with an increase in age up to 50 years in those practicing yoga. Above 50 years of age, there was an increase in prevalence of pain with the highest prevalence of 48.6% reported by dentists aged above 60 years. Higher difference in pain prevalence between yoga practicing dentists and dentists without any physical activity was observed in age groups above 50 years than in the age groups below 50 years. These observations stress the significance of regular yoga practice to keep physical fitness, especially in higher age group. In a previous study, with increase in age, there was decrease in pain because of adaptability to the chair position.[15] It was hypothesized that more experienced dentists learn to adjust their work posture to avoid such problems, or that those dentists with musculoskeletal problems have left the profession.[16,17,18]
There was no significant difference found between dentists working up to 50 h/week in both the groups practicing yoga and not practicing yoga. In the group practicing more than 50 h/week, there was less prevalence of pain among yoga practitioners than non-yoga practitioners. It was also observed that lesser pain was experienced by dentists who were resting for more than 5 min between each patient, irrespective of their age, sex, experience, practicing hours per week, and yoga practice. Dentists working most of the time in a sitting position and regularly practicing sports seem to experience less pain, limitation of movements, and MSDs.
Length of appointment time appeared to influence pain in a study,[12] with those dentists providing longer appointments experiencing more pain. There was lesser pain experienced by dentists taking off for more than one session per week, irrespective of their age, sex, experience, practicing hours per weekm and yoga practice.
Using analgesics was a common practice found among dentists all age groups when they suffered from pain of varying severity.[13,14] But there was lesser intake of pain killers, both in quantity and frequency, among dentists practicing yoga (25%), other physical activity (30%), and dentists who were not practicing any activity (40.32%). These results are supported by other studies showing that 37.5%[13] and 37%[14] dentists seek medical attention for MSDs.
No dentist below 60 years of age, practicing yoga or other activity was absent from job due to musculoskeletal pain. In the 61–70 years age group, two dentists were absent from work for 2 days, of which one was practicing yoga and the other was practicing other activity. In both age groups, the period of rest taken was 2 days, not more than two times in the last 1 year period.
In practitioners not practicing either yoga or other physical activity, a similar trend was found with different rest periods,[13,15] frequencies, and magnitude. Eight (7%) were absent from job for 2 days, 3–5 times in the last 1 year, whereas five dentists above 60 years of age were absent from job (24%) for 3–5 days, 3–5 times in the last 1 year. These results are in accordance with the previous research results reporting that 9–10% of the dentists with MSDs were absent from work.[13,15]
No dentist practicing yoga was hospitalized for musculoskeletal problem, whereas only three dentists were hospitalized for 5–7 days. This lesser frequency may be because of the fact that as soon as the dentists developed moderate pain, they decreased their working sessions or working hours or both [45.7% (16/35)]. The decrease in number of working hours is difficult to compare, as there are sparse studies comparing yoga and other physical activities.
It was found that yoga was more effective than other modes of physical activities like aerobics, brisk walk, sports, etc., as 89.5% of yoga practitioners were free of musculoskeletal pain, in comparison with the dentists with other practices of whom only 78.3% were free of musculoskeletal pain.
The reasons are multifactorial. Yoga allows the practitioners to be more regular, irrespective of the factors such as weather, climate, place, accessibility, availability of gymnasiums, cost incurred, etc. Yoga is a more controlled activity, whereas other activities are controlled not only by the individual but also by others during the activity of sports. Suryanamaskara (Sun salutation), which improves flexibility, strength, and reduces stress and anxiety, was the most commonly practiced yogic activity in our study (n = 30).
Another important factor is that yoga not only strengthens the musculoskeletal system but also decreases stress by releasing endorphins and other hormones, which is another contributing factor for perception of musculoskeletal discomfort by an individual.
Physical exercise has been shown to be an effective preventive intervention for back, neck, and shoulder pain. Exercise is especially beneficial for dental care workers in that it prevents and treats MSDs and stress, and decreases the existing musculoskeletal pain. Dentists with better endurance of the back and shoulder girdle muscles tend to have less neck, back, and shoulder pain.[19,20]
The integration of 30 min of moderate physical activity into the daily activities of dental care practitioners may help to address the inactivity of the larger muscle groups of the legs and trunk and static muscle activity of the back, neck, and shoulders in a clinician's day.
One of the limitations of this study is its inability to correlate between age and sex of the dentists, duration of practice, years of practicing yoga, working hours per week, and site of musculoskeletal pain.
Some special breathing and meditation techniques may have a positive influence on the central nervous system to increase pain control and pain tolerance. The most common asanas in yoga like Salabasana, Dhanurasana, Shavasana, and Suryanamaskara are helpful in the management of neck pain and back pain.
More research is needed on the musculoskeletal problems in dentists, with an emphasis on larger sample size and correlating other factors like age and sex of the dentists, duration of practice, years of practicing yoga, and working hours per week to generalize the results and conclusions, and thereby formulate some guidelines to prevent or minimize work-related MSDs in dentists.
CONCLUSION
Within the limitations of the study, work-related MSDs are found to be a significant occupational health problem among the dentists. The role of some physical activity on the quality and quantity of work-related MSDs experienced by dentists is significant. Yoga is found to be more effective than other modes of physical activities because of its more controlled nature and its positive effect on the psychological stress and strain.
ACKNOWLEDGMENTS
The authors are thankful to all the dentists who participated in the study.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ratzon NZ, Yaros T, Mizlik A, Kanner T. Musculoskeletal symptoms among dentists in relation to work posture. Work. 2000;15:153–8. [PubMed] [Google Scholar]
- 2.Valachi B, Valachi K. Preventing musculoskeletal disorders in clinical dentistry: Strategies to address the mechanisms leading to musculoskeletal disorders. J Am Dent Assoc. 2003;134:1604–12. doi: 10.14219/jada.archive.2003.0106. [DOI] [PubMed] [Google Scholar]
- 3.Valachi B, Valachi K. Mechanisms leading to musculoskeletal disorders in dentistry. J Am Dent Assoc. 2003;134:1344–50. doi: 10.14219/jada.archive.2003.0048. [DOI] [PubMed] [Google Scholar]
- 4.Pollack R. Dental office ergonomics: How to reduce stress factors and increase efficiency. J Can Dent Assoc. 1996;62:508–10. [PubMed] [Google Scholar]
- 5.Lalumandier JA, McPhee SD. Prevalence and risk factors of hand problems and carpal tunnel syndrome among dental hygienists. J Dent Hyg. 2001;75:130–4. [PubMed] [Google Scholar]
- 6.Lehto TU, Helenius HY, Alaranta HT. Musculoskeletal symptoms of dentists assessed by a multidisciplinary approach. Community Dent Oral Epidemiol. 1991;19:38–44. doi: 10.1111/j.1600-0528.1991.tb00103.x. [DOI] [PubMed] [Google Scholar]
- 7.Rucker LM, Sunell S. Ergonomic risk factors associated with clinical dentistry. J Calif Dent Assoc. 2002;30:139–48. [PubMed] [Google Scholar]
- 8.Nayak NN, Shankar K. Yoga: A therapeutic approach. Phys Med Rehabil Clin N Am. 2004;15:783–98. doi: 10.1016/j.pmr.2004.04.004. vi. [DOI] [PubMed] [Google Scholar]
- 9.Andrews N, Vigoren G. Ergonomics: Muscle fatigue, posture, magnification, and illumination. Compend Contin Educ Dent. 2002;23:261–6. 268, 270 passim; quiz 274. [PubMed] [Google Scholar]
- 10.Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18:233–7. doi: 10.1016/0003-6870(87)90010-x. [DOI] [PubMed] [Google Scholar]
- 11.de Carvalho MV, Soriano EP, de França Caldas A, Jr, Campello RI, de Miranda HF, Cavalcanti FI. Work-related musculoskeletal disorders among Brazilian dental students. J Dent Educ. 2009;73:624–30. [PubMed] [Google Scholar]
- 12.Sartorio F, Vercelli S, Ferriero G, D’Angelo F, Migliario M, Franchignoni M. Work-related musculoskeletal diseases in dental professionals. 1. Prevalence and risk factors. G Ital Med Lav Ergon. 2005;27:165–9. [PubMed] [Google Scholar]
- 13.Leggat PA, Smith DR. Musculoskeletal disorders self-reported by dentists in Queensland, Australia. Aust Dent J. 2006;51:324–7. doi: 10.1111/j.1834-7819.2006.tb00451.x. [DOI] [PubMed] [Google Scholar]
- 14.Al Wazzan KA, Almas K, Al Shethri SE, Al-Qahtani MQ. Back and neck problems among dentists and dental auxiliaries. J Contemp Dent Pract. 2001;2:17–30. [PubMed] [Google Scholar]
- 15.Dajpratham P, Ploypetch T, Kiattavorncharoen S, Boonsiriseth K. Prevalence and associated factors of musculoskeletal pain among the dental personnel in a dental school. J Med Assoc Thai. 2010;93:714–21. [PubMed] [Google Scholar]
- 16.Alexopoulos EC, Stathi IC, Charizani F. Prevalence of musculoskeletal disorders in dentists. BMC Musculoskelet Disord. 2004;5:16. doi: 10.1186/1471-2474-5-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Marshall ED, Duncombe LM, Robinson RQ, Kilbreath SL. Musculoskeletal symptoms in New South Wales dentists. Aust Dent J. 1997;42:240–6. doi: 10.1111/j.1834-7819.1997.tb00128.x. [DOI] [PubMed] [Google Scholar]
- 18.Chowanadisai S, Kukiattrakoon B, Yapong B, Kedjarune U, Leggat PA. Occupational health problems of dentists in southern Thailand. Int Dent J. 2000;50:36–40. doi: 10.1111/j.1875-595x.2000.tb00544.x. [DOI] [PubMed] [Google Scholar]
- 19.Hayes M, Cockrell D, Smith DR. A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg. 2009;7:159–65. doi: 10.1111/j.1601-5037.2009.00395.x. [DOI] [PubMed] [Google Scholar]
- 20.Sharma P, Golchha V. Awareness among Indian dentist regarding the role of physical activity in prevention of work related musculoskeletal disorders. Indian J Dent Res. 2011;22:381–4. doi: 10.4103/0970-9290.87057. [DOI] [PubMed] [Google Scholar]