

Abstract
Breast cancer prescreening is carried out prior to the gold standard screening using X-ray mammography and/or ultrasound. Prescreening is typically carried out using clinical breast examination (CBE) or self-breast examinations (SBEs). Since CBE and SBE have high false-positive rates, there is a need for a low-cost, noninvasive, non-radiative, and portable imaging modality that can be used as a prescreening tool to complement CBE/SBE. This review focuses on the various hand-held optical imaging devices that have been developed and applied toward early-stage breast cancer detection or as a prescreening tool via phantom, in vivo, and breast cancer imaging studies. Apart from the various optical devices developed by different research groups, a wide-field fiber-free near-infrared optical scanner has been developed for transillumination-based breast imaging in our Optical Imaging Laboratory. Preliminary in vivo studies on normal breast tissues, with absorption-contrasted targets placed in the intramammary fold, detected targets as deep as 8.8 cm. Future work involves in vivo imaging studies on breast cancer subjects and comparison with the gold standard X-ray mammography approach.
Keywords: diffuse optical imaging, near-infrared, hand-held devices, breast cancer, prescreening, early detection
Introduction: breast cancer statistics
One in eight women in the USA is at the risk of developing breast cancer.1 In 2013, approximately 232,340 new cases of invasive breast cancer developed.1 Annually, 1.3 million new cases of breast cancer are diagnosed worldwide,2 and 1.38 million new cases developed in 2011 worldwide.3 Half of the breast cancer cases occur in economically developing countries.3 Since 1990, death rates related to breast cancer have dropped by 34%.1 About 60% of breast cancer deaths occur in economically developing countries.3 Mortality has seen a decrease in developed countries due to earlier diagnosis and greater treatment options.2
American Cancer Society has set guidelines for detecting breast cancer in women aged 40 and older, which include an annual mammogram, an annual clinical breast examination (CBE), and an optional self-breast examination (SBE).1 Details of these various examinations are described in the “Different modalities used to image breast cancer” section. Prior to the description of the different examination or imaging tools used in breast cancer, the physiology and stages of breast cancer are described in the following section.
Breast cancer stages and imaging
The disease of breast cancer occurs when there are malignant cancer cells in the breast tissue.4 The causes of breast cancer are either external or internal. External causes include tobacco, chemicals, radiation, and infectious organisms. Internal factors are mutations that are inherited as well as those that occur from metabolism, hormones, and immune conditions. Combinations of external and internal factors may lead to the initiation or promotion of breast cancer. It may take as long as 10 years of experiencing external factors before the cancer is detected.5
Stages of breast cancer
The different stages of detecting breast cancer are screening, diagnosis, and prognosis. Screening is performing exams on individuals who do not show symptoms of breast cancer in order to determine whether there is cancer. Screening helps to detect the cancer early before symptoms manifest and prior to spreading to other tissues. Common modalities used in breast cancer screening are SBEs, CBE, and mammograms.
Having screened for breast cancer, further diagnostic tests are performed to confirm the disease and also to determine if the tumor(s) observed is benign or malignant. Being diagnosed with breast cancer, the patient then requires other tests to determine the prognosis and decide on treatment options. Some of these tests include estrogen and progesterone receptor test, human epidermal growth factor type 2 receptor test, and multigene tests. Some of the imaging techniques used in the diagnostic stage are ultrasonography and magnetic resonance imaging (MRI).6 These tests give specific information to help identify the stage of the tumor and whether it is growing rapidly or slowly. Staging is then performed in order to classify the cancer into a stage ranging from zero to four, with four being the most advanced. Some imaging modalities used throughout this stage are chest X-rays, computerized tomography (CT) scans, and bone scans.4
After being diagnosed, the patient may undergo neoadjuvant therapy or primary therapy. Neoadjuvant therapy is a means to decrease tumor size if the tumor is too large to successfully remove. Primary therapy follows neoadjuvant therapy or may be the first step taken after diagnosis. It typically consists of surgery, more specifically mastectomies or lumpectomies, to remove the tumor. Following primary therapy, there is an adjuvant therapy which aims to prevent the recurrence of the cancer and promote longevity of the patient.7 Post-adjuvant therapy patients require periodic monitoring to ascertain that they are tumor free. The prognostic stage is monitoring using imaging modalities that include mammograms, breast MRI, ultrasound (US), positron emission tomography (PET), and/or CT scans.8
Different modalities used to image breast cancer
The conventional prescreening/screening imaging modalities, along with the emerging imaging modalities for breast cancer, are given in Table 1.9–48,50
Table 1.
Conventional breast cancer prescreening/screening and emerging imaging modalities
| Modality | Physics | Application | Advantages | Disadvantages | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|---|
| Examinations | SBE | Self-physical examination for detecting breast lesions | Prescreening | Increases public awareness Can be used on high-risk populations Easy technique that can be performed at home |
No effect on mortality of breast cancer30 High rates of false positives and overdiagnosis31 |
12%–14%32 | – |
| CBE | Clinical breast examination for detecting breast lesions | Prescreening | Reduced breast cancer mortality | No randomized controlled trails have been conducted of CBE in women not receiving other forms of screening30 | 57.14%34 | 97.11%34 | |
| Can detect breast cancer missed by mammography (sometimes) May be effective in reducing mortality in women |
Increased false-positive results32 Does not permit one to determine malignancy with assurance33 High rates of false positives and overdiagnosis31 |
40%–69%32 | 86%–99%32 | ||||
| Conventional imaging Emerging modalities | X-ray mammography (structural imaging) | High energy X-rays travel in a straight path and are attenuated by interaction with tissue | Screening (gold standard), diagnostic, prognostic | High specificity and sensitivity to detecting cancers Portable device |
10% of false-positive cases Poor contrast compared to CT or MRI |
68.6% (in 40–44 year olds) 83.3% (in 80–89 year olds)35 |
91.4%–94.4% (w/hormone replacement therapy)35 |
| Fast imaging time (approximately <1 minute) Good resolution (∼mm) More accuracy in dense breasts when using digital mammography |
Uses ionizing radiation Less sensitive in radiographically dense breasts35 |
||||||
| Ultrasound (structural imaging) | Acoustic waves (mechanical) are introduced into the body and are reflected back toward a receiver | Screening, diagnostic, prognostic | High diagnostic utility among women with dense breasts30 Portable device Fast imaging time (approximately <1 minute) Nonionizing (safe) |
High false-positive rates30 Poor contrast Poor resolution (∼cm) |
Increases from 36% to 95% with Doppler36 | Decreases from 86% to 79% with Doppler36 | |
| CT (structural) | 3D arrays of X-rays travel in a straight path and are attenuated by interaction with tissue | Screening, diagnostic, prognostic | Good resolution (∼mm) Poor contrast Fast imaging time (approximately <1 minute) |
Non-portable device Expensive device |
– | – | |
| MRI (structural) | RF signal is used to align water molecules to a changing magnetic field where the resultant RF signal is collected | Screening, diagnostic, prognostic | Sensitivity is nearly 100%12,37 Can better detect intraductal spread of cancer12 |
Specificity values vary12 and are poor37 MRI-guided biopsies are difficult and require compatible equipment12 |
88.1%38 | 67.7%38 | |
| Good technique for post- chemotherapy imaging12 Excellent resolution (<mm) Nonionizing radiation |
Only the lateral side of the breast is visible12 Not portable Slow imaging time (approximately over 20 minutes) Expensive device Good contrast |
||||||
| PET (nuclear) – functional imaging | High-energy radioactive isotopes create two gamma rays that travel in opposite directions toward detectors | Screening, diagnostic, prognostic | Good contrast Functional information |
Ionizing radiation Poor resolution (∼cm) Not portable Expensive device Slow imaging time (approximately over 20 minutes) |
96%39 | 77%39 | |
| Scintimammography – (functional imaging) | Uses nonspecific radionuclides to identify malignant lesions | Diagnostic | Good contrast Functional information |
Ionizing radiation Not portable Slow imaging time High false positives40,41 Low sensitivity for small cancers (<1–1.5 cm) and ductal carcinoma in situ42 |
93%43 | 87%43 | |
| Thermography (functional imaging) | Identifies vascular and temperature changes | Screening, diagnostic | Noninvasive Non-radiative Less imaging time Promise for dense breasts44 |
Easily affected by temperature Large breasts are poorly imaged High false positives and false negatives26 |
97%45 | 14%45 | |
| Electrical impedance tomography (functional and structural) | Measures local dielectric properties of cancer cells, including electrical conductance and capacitance | Diagnostic, but works better for screening46 | Noninvasive, non-radiative, and risk free Works well with dense breasts Relatively inexpensive46–48 Scans in approximately 15 minutes |
High false-positive rates49 Poor spatial resolution than CT or MRI |
72.2%50 38%46 |
67%50 95%46 |
|
| Microwave imaging (functional) | Employs microwave or millimeter waves to image dielectric bodies | Diagnostic | Noninvasive Non-radiative |
Poor resolution at higher depth48 Low contrast in fibroglandular tissues |
– | – | |
| Optical imaging (functional) | Employs near-infrared light (650–900 nm) to measure differences in absorption and scattering coefficients across different tissues | Screening, diagnostic, prognostic | Noninvasive Non-radiative Relatively inexpensive and portable Low imaging time (<1 minute) Good contrast (since functional information) |
Highly scattered signal limits its depth imaging Limited spatial resolution when optical fibers are used |
– | – |
Abbreviations: SBE, self-breast examination; CBE, clinical breast examination; CT, computerized tomography; MRI, magnetic resonance imaging; PET, positron emission tomography; RF, radio frequency.
SBE and CBE
Breast cancer prescreening is carried out prior to the gold standard screening using X-ray mammography and/or US. Prescreening is typically carried out using CBE or SBEs. CBE is carried out by the physician for early detection of skin irregularities9 or abnormalities in the breast tissue. Breast self-examination is carried out by women to increase public awareness and to become familiar with appearance and feel of their breasts.9,10 Approximately two thirds of women older than 40 years undergo periodic CBE. However, there exists minimal evidence to measure the effectiveness of CBE in detecting breast cancer. The advantage of SBE is that the patients can become familiar with their anatomy and perform the screening modality in a private setting at home. While CBE demonstrated a maximum sensitivity of 40%–69%, SBE had a low sensitivity of 12%–14%.32 Furthermore, it has been shown in randomized control trial that SBE has no positive effect compared to not performing it and that it actually leads to false positives. In general, both CBE and SBE have high false-positive rates and overdiagnose, that there is a need for an objective imaging modality at the prescreening stage.
X-ray mammography
Breast cancer screening involves screen-film and digital mammography, computer-aided detection, US, and MRI. Screen-film mammography involves using X-rays to obtain images that are captured on a film, while digital mammography captures the X-rays through digital means which can then be read on a printed film or electronically on a computer. Digital mammograms are convenient to the radiologist interpreting the X-ray by allowing him/her to change the values of brightness, contrast, and magnification; however, they are at a greater price to the patients. Studies have demonstrated screen-film mammography to have a higher sensitivity than that of digital film mammography. Although computer-aided detection is supported by a small amount of data, it can locate lesions, such as calcifications, on mammograms, thereby increasing the amount of cancer detected as well as increasing the accuracy of radiologists.11 In general, mammography reduces the risk of dying from breast cancer by 15%–20%, which can lead to a greater number of treatment options.9 The advanced applications of digital mammography include tomosynthesis and contrast-enhanced digital mammography. In tomosynthesis, multiple digital X-ray images are obtained at multiple angles of the X-ray tube in order to yield 3D images or individual slices in dynamic cine.12–14 In contrast-enhanced digital mammography, a contrast agent (generally iodine based) is injected intravenously, and multiple X-ray images are obtained with a high contrast-to-noise ratio, which in turn reduce the visibility of microcalcifications.15,16
Magnetic resonance imaging
Not commonly used for screening but more so for diagnosing, MRI uses a combination of a magnetic field, radio waves, and computer processing in order to create images. Occasionally, it is used for screening young women with known increased risk of breast cancer due to gene mutations when mammograms are not ideal. A study has also shown that using MRI in the screening stage leads to unnecessary biopsies and further examinations when compared to mammography screening.11 The disadvantages of using MRI is its high cost of about ten times the cost of a mammogram, its low specificity relative to mammograms, the need for contrast agents (in some cases), and the long amount of time required to image a patient, especially exacerbated by a patient with low tolerance to enclosed spaces.11 The advanced applications of MRI for breast cancer imaging include diffusion and perfusion imaging, proton magnetic resonance spectroscopy (MRS), and MR elastography. While the diffusion perfusion imaging offers information related to tissue microstructure from focusing on water protons, perfusion imaging follows the flow of blood to show the microvasculature.17 Proton MRS measures the resonance of protons to provide a spectrum in order to identify choline, a biomarker for cancer. In MR elastography, electromechanical drivers vibrate the breast to generate acoustic shear waves that are further imaged by MRI.12
Ultrasounds
USs have recently been approved by the Food and Drug Administration to aid in screening of breast cancer in patients with dense breast tissue, apart from its application as a diagnostic imaging tool. US employs sound waves to create images of the tissue features.18 The advantages of US are that it can differentiate benign and malignant masses as well as cysts and solid masses. The main drawback is that its effectiveness varies depending on the skill of the US technician. US also has a greater amount of false positives compared to mammography, up to 12.9% compared to 6%, respectively.11 In the clinic, the most common mode of US imaging is to obtain 2D images from B-mode scanning. In certain cases, compound imaging is carried out by combining multiple US images into one. Although compound imaging is better in quality than B-mode imaging, it suppresses the shadows that can be used to determine malignancy.12 On the other hand, Doppler US uses the Doppler effect to track blood flow in order to find malignant tumors through their neoan-giogenesis.19,20 The advanced applications of US imaging at preclinical stage include sonoelastography (SE), tissue harmonic imaging, and US spiral computed tomography. While in SE, US images of the breast are obtained during its displacement, frequencies are filtered appropriately in tissue harmonic imaging in order to improve the contrast. US spiral CT is a combination of US and CT imaging used to obtain volumetric 3D images of the breast, although it can miss tumors located proximal to the chest wall.21
Nuclear imaging
Nuclear imaging yields functional images based on molecular properties, unlike the anatomical images as in X-ray, US, and MRI. Also, this technique involves radiation and is expensive, requires little or no breast compression, and shows promise in detecting cancer, especially in high-risk patients.12 In radio-immunoscintigraphy, tumor-associated antigens are targeted by an injected radiopharmaceutical agent, with antigen expression differing between normal and cancer cells. Scintimammography (SMM) is an imaging technique used in the diagnostic phase. It uses nonspecific radionuclides to identify malignant lesions. Usually, it follows a mammogram and identifies the lesions found in the mammogram. It is also a useful postprimary and post-adjuvant therapy because it identifies tumor changes and recurrence as well as necrosis in the specific area.22 SMM has higher specificity than MRI, which makes it clinically applicable to detect lesions larger than 1 cm in diameter. PET, generally using 18F-fluorodeoxyglucose, uses glucose metabolism to detect cancer, especially in detection of malignancies and metastatic disease in solid organ tumors.12 The advanced applications of nuclear breast imaging include positron emission mammography (PEM) and PET/CT. PEM focuses on imaging only the breast tissues unlike the entire body as in PET imaging, and serves as the best screening tool in high-risk patients.23 PET/CT is a multimodal imaging approach that combines PET (for functional information) and CT (for anatomical information).24
Emerging modalities (experimental stage)
Some of the emerging technologies for breast cancer imaging include thermography, microwave imaging, electrical impedance imaging spectroscopy (EIS), Raman spectroscopy, and diffuse optical imaging (DOI).
Thermography is another imaging technique used in the diagnostic phase. It identifies vascular and temperature changes noninvasively and without radiation.25 A study performed by Sterns et al has proven this modality to result in a large amount of false positives and false negatives. The study also reported inconsistent interpretation of the thermograph.26 Another study states thermograph findings to be more evident of the metabolic rate and expansion state as opposed to its actual size and depth. The advantage of demonstrating metabolic and growth rate is that a prediction can be made that determines risk of the patient. For instance, one study reports that 38% of false-positive patients develop breast cancer within 4 years.10
EIS is also used in the diagnostic phase of breast cancer. This modality measures local dielectric properties of cancer cells, including electrical conductance and capacitance. This is performed by applying current to the patient with varying frequency, current, flow, and voltage. The values gained from cancer cells are different than those of normal cells. A study performed by Malich et al shows a sensitivity of 80.5% and a specificity of 64.7%. The features in the patient’s anatomy, such as scars, hairs, and bone, can result in false positives. A high amount of false positives along with an effectiveness that varies with the conductor of the EIS results in limited clinical use.27 In a review article by Vreugdenburg et al, it was found that only one study used EIS for screening, whereas the other studies focused on women with already diagnosed breast cancer. The study focusing on screening did not use a valid reference test to ascertain if the patients were healthy or had cancer. The study did not recommend the use of EIS for screening due to lack of data regarding the ability of EIS to detect cancer in asymptomatic women.28
Microwave imaging employs microwave or millimeter waves to image dielectric bodies.29 This modality offers low contrast between healthy fibroglandular tissues, where the majority of breast tumors occur, and malignant tumors pose as a challenge for microwave imaging of the breast tissue. The challenges of high tissue attenuation resulting in limited depth of wave penetration, and loss of resolution with higher penetration depth limit its immediate clinical translation for breast cancer.
The various other emerging modalities (not described here) include DOI, Raman spectroscopy, diffraction techniques (eg, diffraction-enhanced imaging and small angle X-ray scattering), compression and palpation method (via piezoelectric sensing), X-ray diffraction of hair, breath detection using gas chromatography and mass spectroscopy, and canine scent detection.12
DOI: physics and breast cancer application
In the past three decades, DOI is emerging as a breast cancer imaging device with applicability at both diagnostic and prognostic stages of breast cancer imaging. DOI uses near-infrared (NIR) light between 650 nm and 900 nm to image the differences in the blood oxygenations between the tumor and normal breast tissues. Based on the nature of the optical imaging instrument, its applicability for early-stage breast cancer detection is also attempted by various research groups, as described in the following sections.
Wavelengths of light from 650 nm to 900 nm are minimally absorbed and preferentially scattered upon interaction with tissue allowing for deeper light penetration than possible at other optical wavelengths (Figure 1).51 The technology that uses light in this NIR wavelength region to noninvasively image deep tissues is called as NIR optical imaging (or DOI). The low absorption occurs due to the main absorbers in physiological tissue, that is, water and oxy- and deoxy-hemoglobin, which absorb less light than at other optical wavelengths.52 The difference in optical properties (ie, absorption and scattering of the light) between normal and diseased tissues is used to characterize tissues and detect abnormalities.
Figure 1.

Spectrum of absorption from 400 nm to 1,000 nm.
Notes: The biological optical imaging window allows deeper penetration of light from the wavelengths of around 650–900 nm due to minimal absorption by the tissue components, HbO, Hb, and H2O in this wavelength range. Adapted by permission from Macmillan Publisher Ltd: Weissleder R. A clearer vision for in vivo imaging. Nat Biotechnol. 2001;19(4):316–317, Copyright ©2001.53
Abbreviation: Hb, hemoglobin.
Deeper tissue penetration allows optical imaging to be implemented as an imaging technology for breast cancer detection, diagnosis, and/or prognosis. Optical imaging provides a functional imaging approach with decent spatial resolution and contrast. Optical imaging also requires less imaging time compared to MRI, and is also less expensive. The combination of benefits offered by optical imaging in terms of less imaging time (<1 minute), good spatial and excellent temporal resolution, good contrast (from functional imaging), and relatively inexpensive instrumentation suggests that optical imaging is potentially an emerging technology for future clinical applications in the areas of breast cancer imaging, brain mapping, and any noninvasive body tissue imaging. Additionally, the source powers employed during optical imaging are within the safe limits (typically <50 mW), and NIR light is non-radiative in nature.
Optical imaging and breast cancer
Optical imaging has been utilized toward various aspects of clinical breast imaging: i) measurement of optical and physiological properties of healthy breast tissue; ii) detecting the presence of abnormal tissue (ie, tumors); iii) distinguishing between benign and malignant tumors; iv) monitoring response to neoadjuvant chemotherapy; v) sentinel lymph node mapping; and vi) tomographic imaging of the entire breast.54 These breast imaging applications in some cases involved the use of external fluorescent contrast agents to improve the optical contrast of the diseased regions from the normal breast tissue.55,56
Optical imaging uses NIR light as a continuous-wave (CW), frequency (frequency domain, FD), or pulse (time domain) signals. In CW imaging, the source light intensity remains constant in time and attenuates as it propagates through the tissue due to absorption and (indirectly) to scattering. FD imaging uses time-dependent intensity-modulated light that becomes attenuated and phase shifted as it propagates through the tissue. Time-domain imaging uses time-dependent (pico-or nanosecond) pulses of light that broaden and attenuate as it propagates through the tissue. Different types of optical devices developed for breast cancer detection employing one or more of these measurement techniques have been developed toward DOI of breast tissue. The most commonly employed sources in these devices include laser diodes and light-emitting diodes (LEDs), and the detectors being silicon photodiodes, photon multiplier tubes, avalanche photo diodes, or CCD cameras. The optical devices using one of these sources/detectors can be grouped into three major kinds of devices: bed-based imagers, parallel plate imagers, and hand-held imagers. The hand-held imagers54,57–94 are capable of only reflectance imaging, while parallel and bed-based imagers are capable of transillumination and reflectance imaging. Hand-held imagers are generally smaller, less expensive, and portable devices which have the benefit of being placed easily by a technician. The small device ensures that all breast shapes and sizes can be imaged with minimal patient discomfort and lack of tissue compression. Bed-based imagers95–105 are a category of imagers which require a subject to lie down and suspend the breast tissue to be imaged in special imaging bins or enclosures, which facilitate data collection and 3D tomographic imaging. Parallel plate imagers106–112 are similar to bed-based imagers, but instead of relying on circular bins, they implement compressive plates similar to X-ray mammography systems. This reduces the exclusion of subjects by reducing their tissue thickness via compression. While the focus of the bed-based and parallel plate imagers has been predominantly for 3D tomographic imaging of breast cancer, the hand-held optical devices have focused on spectroscopic information of the breast at both the diagnostic and prognostic stages.
In general, optical breast imaging in the clinic has not been systematic, and various research groups have focused on technological developments of their devices.56 When focusing only on clinically oriented optical mammography studies with approximately 2,000 women, it was observed that ∼85% of breast lesions are detectable.56 Additional dimensionality to the optical mammography is provided by integrating and co-registering the functional information of diffuse optical spectroscopy and imaging with X-ray mammography and MRI, which provide structural information or vascular flow information, respectively. One of the goals of the optical breast imaging research community is to develop DOI platforms that can be used as stand-alone devices or in conjunction with MRI, mammography, or US. These platforms would potentially assist in detecting the breast cancer disease in mammographically dense tissues, distinguishing between malignant and benign lesions, and understanding the impact of neoadjuvant chemotherapies. More recently, hand-held optical devices are developed with a focus on early-stage detection of breast cancer as a first-response device.
Optical imaging for breast prescreening
Role of optical imaging in breast prescreening
Prescreening of the breast typically involves: i) breast self-examination – a recommendation for all women to become familiar with both appearance and feel of their breasts and report any changes to their physician; and ii) CBE – an examination performed by a clinician in which he/she utilizes the pads of the fingers to feel the breasts, assessing the shape, texture, and the presence of any bumps. Conventionally and clinically used screening approaches include mammography, US, and MRI,11 as described in the Introduction section. Optical imaging is an emerging prescreening or screening tool in the area of breast cancer.113
Various research groups have developed hand-held optical devices (or scanners) for breast cancer imaging,54,57 for detection, diagnosis, and/or prognosis. The optical devices that focus on early detection (for potential prescreening) of breast cancer are tabulated in Table 2 and shown in Figure 2. The concept of developing portable, low-cost, hand-held optical devices for early-stage detection of breast cancer began in the late 1990s64 by Tromberg’s research group. Tromberg’s device (Device #1) employed laser diodes (of multiple wavelengths) and avalanche photodiodes (as detectors) to obtain FD-based optical spectroscopic information from breast tissues and compare the optical properties of a normal breast with that of the benign lesions. Device #1 (Table 1) was also used in several studies (for a total of ∼100 subjects) to compare healthy and tumor-containing breast tissue.71,72,75 The results showed differences in the optical properties of the tissue based on subject age, tumor size, and tumor pathology. The second device (Device #2) developed by researchers at University of California Irvine was also based on FD diffuse optical spectroscopic imaging using laser diodes (at multiple wavelengths) and avalanche photodiodes. Based on the measured differences in the absorption coefficients between the diseased (ie, tumor) and normal breast tissue, the device detected the presence of a lesion in in vivo human breast tissue.77–79 The only other FD-based optical device (Device #6) was that developed by Zhu and her group at University of Connecticut.61,87,114 Unlike other hand-held optical devices, Zhu’s device performed multimodal optical and US imaging to obtain 3D diffuse optical tomographic imaging of the breast. This device imaged the benign and malignant breast lesions in human subjects.
Table 2.
Optical imaging devices developed for prescreening or early-stage breast cancer imaging
| Number | Reference | Modality | Measurement technique | Source type | Detector type | Size | Clinical application(s) |
|---|---|---|---|---|---|---|---|
| 1 | Tromberg et al64 | DOS | FD (300 kHz–1 GHz) | Laser diodes (10–30 mW) (674 nm, 811 nm, 849 nm, 956 nm) | APD | – | Compare optical properties of normal and benign lesion-containing breast tissue |
| 2 | No et al79 | DOS | FD (10 MHz–1 GHz) | Eight laser diodes (50 mW) (783 nm) | APD | – | Noninvasive breast cancer detection based on frequency-domain photon migration |
| 3 | Nioka and Chance80 | DOS | CW | Light-emitting diodes (10–15 mA) (760 nm, 805 nm, 850 nm) | Eight silicon diode detectors | ∼9 cm diameter | Determine sensitivity and specificity of detecting breast cancer in 116 human subjects. Obtained 93% specificity and 96% sensitivity |
| 4 | Chance et al59 | DOS | CW | Two light-emitting diodes (20 mA) (800 nm) – out of phase sources | One silicon diode detector | 9.3×6.5×3 cm3 (similar in size to glucose meter) | Detection and 2D localization of breast cancer lesion in a human subject |
| 5 | Cheng et al83 | DOS | CW | Laser diodes (0.15 W/cm2) (690 nm, 830 nm) | PMT | 5.5×5.5×10.2 cm3 | Determine sensitivity and specificity of detecting ductal carcinoma in 50 human subjects. Obtained 92% diagnosed sensitivity and 67% diagnosed specificity |
| 6 | Zhu et al114 | DOT and US | FD (200 MHz) | Eight dual-wavelength laser diodes (690 nm, 780 nm, 830 nm) | APD | – | Image benign and malignant lesions at early stage in breast tissue |
| 7 | Flexman et al115 | DOS (wireless) | CW | Laser diodes (10 mW) (780 nm, 808 nm, 850 nm, 904 nm) | Two silicon photodiodes | 11.5×16×2.5 cm3 | Liquid phantom studies to demonstrate measurement of HbO, HbR, and scattering in tissues. In vivo data not available |
| 8 | Xu et al60 | DOI (P-Scan Imager, Vioptix Inc.) | CW | Eight dual-wavelength laser diodes (690 nm, 830 nm) | Eight silicon photodiodes | 5.5×5.5×10.2 cm3 | In vivo human tissue studies for dynamic characterization by reconstructing absorption coefficients. In vivo breast imaging studies are not available |
| 9 | Labib et al116 | Breast illumination | CW | 617 nm visible red light | Naked eye | – | Imaged 310 women (43.6±12.4 years) for breast screening. Obtained 73.7% specificity, 93% sensitivity, 91.4% PPV, 77.8% NPV, and 88.2% accuracy. Detects lesions 15 mm and above |
| 10 | Rodriguez et al117 | DOI (NIROS) | CW | Light-emitting diode (710 nm) | CMOS camera | 5×7×15 cm3 | In vivo breast imaging studies using tumor- like targets. No data from breast cancer subjects |
Abbreviations: APD, avalanche photodiode; CMOS, complementary metal oxide semiconductor; CW, continuous wave; DOI, diffuse optical imaging; DOS, diffuse optical spectroscopy; DOT, diffuse optical tomography; FD, frequency domain; NIROS, near-infrared optical scanner; PMT, photon multiplier tube; PPV, Positive predictive value; NPV, Negative predictive value; US, ultrasound.
Figure 2.

Different hand-held probes developed for early detection of breast cancer, showing their source–detector layouts and the actual device.
Note: The source-detector configuration and the actual device are shown for each of the devices (A-I) in Table 2. (A) Adapted from Tromberg BJ. Optical scanning and breast cancer. Acad Radiol. 2005;12(8):923–924, with permission from Elsevier.62 (B) ©2005 IEEE. Reprinted, with permission, from No KS, Chou PH. Mini-FDPM and heterodyne mini-FDPM: handheld non-invasive breast cancer detectors based on frequency-domain photon migration. IEEE Trans Circ Syst I Reg Papers. 2005;52(12):2672–2685.77 (C) Adapted from Chance B, Nioka S, Zhang J, et al. Breast cancer detection based on incremental biochemical and physiological properties of breast cancers: a six-year, two-site study. Acad Radiol. 2005;12(8):925–933, with permission from Elsevier.138 (D) Adapted with permission from Chance B, Zhao Z, Wen S, Chen Y. Simple ac circuit for breast cancer detection and object detection. Rev Sci Instrum. 2006;77:064301. Copyright ©2006, AIP Publishing LLC.59 (E) Adapted with permission from Xu RX, Qiang B, Mao JJ, Povoski SP. Development of a handheld near-infrared imager for dynamic characterization of in vivo biological tissue systems. Appl Opt. 2007;46(30):7442–7451.59 (F) Adapted from Zhu Q, Huang M, Chen N, et al. Ultrasound-guided optical tomographic imaging of malignant and benign breast lesions: initial clinical results of 19 cases. Neoplasia. 2003;5(5):379–388, with permission from Elsevier.114 (G) Adapted from Flexman ML, Kim HK, Stoll R, Khalil MA, Fong CJ, Heilscher AH. A wireless handheld probe with spectrally constrained evolution strategies for diffuse optical imaging of tissue. Rev Sci Instrum. 2012;83:033108. Copyright ©2012, AIP Publishing LLC.115
Abbreviation: CMOS, complementary metal oxide semiconductor.
Many hand-held optical devices (Devices #3–5, #7–10) were based on CW imaging mode. Chance and his group developed two portable devices (Devices #3 and #4) of different source–detector configurations and each using LEDs as sources and silicon photodiodes as detectors.59,80 Device #3 was used in an extensive study to show the differences in the biochemical and physiological properties of breast tissue containing growing cancers, compared to corresponding normal tissue in the contralateral breast.80 In a 6-year study on 116 patients with 44 confirmed malignancies, they reported the ability to distinguish cancerous from noncancerous breast tissue with a sensitivity of 96% and specificity of 93%. The second device from Chance’s group (Device #4) employed two LEDs that were out of phase in order to generate destructive interference signals.59 The detected signal at the detector placed mid-way between the two sources provided a null signal, which shifts in the presence of any abnormality. This principle was used in detection and 2D localization of any breast lesions/abnormalities.59 Another spectroscopic-based hand-held device (Device #5 in Table 2), which used laser diodes as sources, was used to detect breast cancer in 50 females who have been indicated of suspected breast cancer from X-ray mammography.83 The device used in these studies (Device #5, P-Scan Imager) was developed by Vioptix Inc. as a CW-based NIR spectroscopic device that provides real-time 2D mapping of blood oxygen saturation and total hemoglobin. From their preliminary studies, the device provided 92% diagnostic sensitivity and 67% diagnostic specificity in detecting ductal carcinoma.83 Another research group from Ohio State University, Xu et al, also used the same P-Scan imager (Device #8 in Table 2) for phantom and in vivo human subject studies to dynamically characterize the tissue in response to dynamic compression stimuli.60 The device demonstrated that it can detect tissue optical, mechanical, and physiological changes under the dynamic loading condition, although requiring further evaluation for breast cancer studies. One of the latest devices employing laser diodes as sources was made wireless.115 However, to date, only liquid phantom studies using Device #7 were performed to demonstrate the measurements of HbO, HbR, and scattering properties of the tissue.
On the contrary to the NIR-based hand-held devices, a breast illuminator employed visible red light (617 nm wavelength) to transmit the breast tissues and visualize the optical contrast using the naked eye.116 In a study at the National Cancer Institute at Cairo University, BreastLight (Device #9) was employed on 310 women, and the results were compared to X-ray mammography and histopathology (when suspicious cases were found in mammography). Breast illumination using BreastLight device and X-ray mammography were concordant in 277/310 cases (89.4%). The breast illumination device provided a sensitivity of 93%, specificity of 73.7%, a positive predictive value of 91.4%, and a negative predictive value of 77.8%, demonstrating the device as a potential breast cancer prescreening tool.
At our Optical Imaging Laboratory at Florida International University, a portable hand-held wide-field NIR optical scanner (NIROS) (Device #10) was developed for DOI of breast tissues via transillumination mode of imaging.117 The details of this device and the preliminary in vivo studies are described in the following section.
Our ongoing efforts in breast prescreening using optical imaging
Most of the hand-held optical imagers available to date, whether for prescreening/screening or diagnostic/prognostic applications, employ optical fibers to illuminate/detect NIR signals. The use of optical fibers allows precise launching and collection of NIR optical signals at point locations on the tissue surface. The intensity and location of these source and detector points using optical fibers when measured allow 3D tomographic imaging. However, the use of optical fibers can also be disadvantageous. Many optical fibers or fiber bundles are required to enhance the spatial resolution of the imaging system, but at the cost of increased bulkiness, reduced flexibility (especially in hand-held devices), and instrumentation expense. In recent years, a few research groups have developed fiber-free NIR imaging systems using wide-field detectors (eg, CCD or complementary metal oxide semiconductor [CMOS] camera) for noncontact imaging.118–137 These imagers employ either reflectance or transmittance mode to image tissue phantoms, blood vessels, and/or veins of the skin surface. Unlike the fiber-based devices (with contact) that can image deep tissues as in breast imaging, the fiber-free noncontact optical devices developed to date have been used for sub-surface imaging (≤1 cm deep).
In our Optical Imaging Laboratory, a fiber-free handheld NIROS has been developed toward deep tissue imaging (>1 cm target depth) in both reflectance and transmittance mode. Preliminary in vivo breast imaging studies using the scanner as a noncontact device were performed to determine its deep target detectability and its potential applicability as a breast cancer prescreening tool.
Instrumentation
The fiber-free noncontact hand-held NIROS comprises a hand-held probe (Figure 2, Device #10), a controller box, and a computer with custom-developed image acquisition/processing toolbox. The hand-held probe (weighing <1 lb) consists of a 710 nm LED source light for area illumination and an NIR-sensitive CMOS camera for area detection. The LED source encased in a heat sink is driven by an LED driver (placed in the controller box) that controls the radiating power of the source. The LED driver and the CMOS camera are synchronized in the data acquisition timing via a microcontroller unit, and both the source and detector are powered by the computer’s USB port. The diffuse reflected/transilluminated NIR signals from the tissue surface are detected by the camera after the signals have been filtered using a 645-nm long-pass optical filter and focused using an 8.5 mm focusing lens. A MATLAB-based imaging software was developed in order to automate the data acquisition, data storage, and data processing. For the breast imaging studies, two transparent parallel acrylic plates were used to hold the breast tissue during transillumination-based imaging using NIROS (Figure 3).
Figure 3.
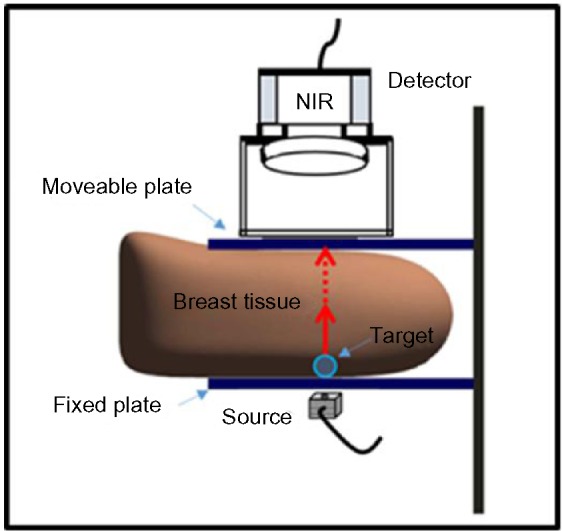
Setup for breast imaging studies consisting of the breast tissue placed in between two transparent plates.
Notes: A detector is placed above the top plate, the source is placed beneath the bottom plate, and a target is placed beneath the breast tissue and above the bottom plate.
Abbreviation: NIR, near-infrared.
In vivo breast imaging studies using NIROS
The Florida International University IRB-approved studies imaged ten healthy female subjects over the age of 21 years with no known history of breast cancer. The breast imaging studies were performed with the breast tissue placed in between the two transparent plates to provide for transmission imaging mode. As seen in Figure 3, the top plate is adjustable in order to perform studies with or without applied pressure and to accommodate different breast tissue sizes. The detector is placed above the top plate, and the LED source is placed beneath the bottom fixed plate. A 0.46 cm3 target was filled with a solution of 0.8% India ink in Liposyn in order to create a tumor-like agent with high-absorption properties. The target was positioned beneath the breast tissue and above the bottom plate and moved to different locations (noted by clock positions) throughout the study.
The goal of the studies was to qualitatively determine the ability of NIROS to detect the targets when both the applied pressure and target locations were varied. Images were acquired with and without pressure by adjusting the top moveable plate and also by moving the target to various clock locations in order to assess NIROS’s capacity to determine where the targets were placed. The studies were performed in transmission mode with the source below the tissue and the detector above the breast tissue. The images were acquired without external light; only the laptop was on with the screen brightness at the minimum setting, in order to minimize noise. The power of the LED was measured several times throughout the study, and the CMOS exposure time was adjusted for each subject as well as the focus.
Image processing was carried out using a custom-developed MATLAB-based software. The first step was to co-register the raw NIR images, so that the two images are aligned on the same coordinate system. This was followed by subtraction of the NIR image of the breast tissue obtained without the target from the NIR image obtained with the target present. The regions outside the breast tissue were masked (or cropped) in order to improve the image contrast by removing the noise. Finally, minimum and maximum pixel values were set by the user in order to distinguish areas of increased or decreased absorption in the image, allowing for the recognition of the target with improved contrast. The targets were seen as areas with increased absorption.
Experimental results from two different subjects are shown below in Figures 4 and 5. Figure 4 shows a set of images from subject #1’s left breast at a constant pressure. Figure 4B has the target, and Figure 4A does not have a target. Figure 4C is the final image after data processing including co-registration, subtraction, and masking. The region of increased absorption in the final image reveals where the target was placed.
Figure 4.
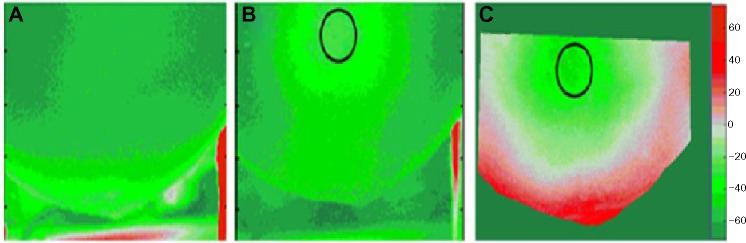
Transmitted NIR optical images of the left breast from subject #1 that were captured at a constant pressure applied on the breast (in all images).
Notes: (A) NIR image was captured without pressure and without target. (B) NIR image was captured without pressure and with the target placed at the location indicated by the black hollow circle at 12 o’clock. (C) Post-processed NIR image after co-registering, subtracting, and masking. The black hollow circle in (B and C) depicts the 2D location of the target at 12 o’clock position in the intramammary fold of the left breast.
Abbreviation: NIR, near-infrared.
Figure 5.
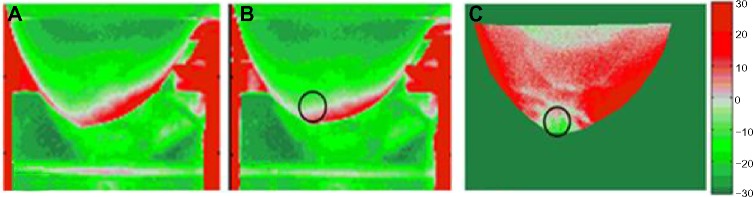
Transmitted NIR optical images of the left breast from subject #2 that were captured at a constant pressure applied on the breast (in all images).
Notes: (A) NIR image was captured with applied pressure and without target. (B) NIR image was captured with applied pressure and with the target placed at the location indicated by the hollow black circle at 6 o’clock. (C) Post-processed NIR image after co-registering, subtracting, and masking. The black hollow circle in (B) and (C) depicts the 2D location of the target at 6 o’clock position in the intramammary fold of the left breast.
Abbreviation: NIR, near-infrared.
Figure 5 also shows a set of images from subject #2 with applied pressure and with the target in the 6 o’clock location. The target can be distinguished in the last picture (Figure 5C) as the region in green in the bottom portion of the breast. It was also noticed that when the target was placed furthest away from the source, as in Figure 5, the target was still detectable due to its higher absorption. The greatest distance between the target and the top plate at which a target was able to be detected was at 8.8 cm. Hence, while the raw images do not reveal information about the location of the target, the target’s location can indeed be seen in the final image once image processing has been performed.
The preliminary in vivo studies on the normal breast tissues with a superficially placed target in the intramammary fold have shown that an increased absorption was clearly observed from the target site (up to 8.8 cm deep) when (maximum comfortable) pressure was applied. To date, an area illumination and area detection-based NIR device have demonstrated only sub-surface imaging (1 cm or less). NIROS has demonstrated detection of deep targets using area illumination/detection approach, along with post-processing techniques to improve the target detection greater than 8 cm deep. Although the images cannot precisely locate the target in 2D, their detected location was close to the true clock location as seen in Figures 4 and 5.
In an actual breast cancer case, NIROS may translate to imaging the contralateral breast and comparing the differences in the absorption across the two tissues, via symmetric clockwise imaging of the breast (as in an US approach). Currently, work is carried out to image both the left and right breast tissues and compare the two, as there are structural differences between the two. These structural differences can lead to differences in NIR images (from physiological differences). Hence, understanding the hemodynamic differences between normal left and right breasts can help differentiate between the breast abnormalities with respect to the contralateral breast (acting as a reference) in the future. There are ongoing efforts to perform extensive in vivo studies under various experimental conditions to determine the capabilities of the noncontact hand-held NIROS in detecting smaller and deeper targets.
Studies in the past have revealed that only half of the insured women over the age of 40 are claiming annual mammogram screenings, despite medical recommendations endorsed across the USA and the world. Reasons for noncompliance suggested from various studies include discomfort during the exam, concern over radiation exposure, access to facilities, inconvenience/lack of time, embarrassment/cultural barriers, and denial. Thus, to improve breast cancer screening compliance, a need exists for a safe, comfortable, accessible, and convenient breast cancer prescreening tool to better triage the subjects for early detections/treatment options. There is a potential for a functional imaging tool to provide additional information to the CBE or SBEs at the prescreening stage that may provide more information to the clinicians. Although the hand-held noncontact NIROS cannot determine the accurate location of a target, as other 3D tomography-based optical imagers, it may have the potential to detect the presence of any abnormalities (or target(s)) as an initial assessment to breast prescreening. The ability to perform deep tissue imaging using a portable hand-held NIROS allows for in vivo breast studies. Following the extensive in vivo studies on normal subjects, studies will be performed on breast cancer subjects to validate the above-stated hypothesis and determine the capabilities of the device for breast cancer prescreening. In this effort, NIROS is currently modified to allow hemodynamic imaging (using a dual-wavelength source system) such that the changes in oxy- and deoxy-hemoglobin from breast tissues can be determined apart from changes in absorption alone.
Conclusion
In this review, the existing and clinically applied breast cancer prescreening tools and screening imaging modalities are described. With a need for a systematic prescreening or early detection of breast cancer, the application of optical imaging modality is described. Although various research groups have developed many optical imaging devices for detection, diagnosis, and prognosis of breast cancer, a few of these devices have focused on early detection or prescreening. While a few of these hand-held optical devices have performed in vivo clinical studies on breast cancer subjects, there still remains extensive work to be performed to assess optical devices as potential future breast prescreening devices.
Acknowledgments
A part of the work has been supported by NIH (R15 CA 119253) funds and FIU Division of Research Seed Funds.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.DeSantis C, Ma J, Bryan L, Jemal A. Breast cancer statistics, 2013. CA Cancer J Clin. 2014;64:52–62. doi: 10.3322/caac.21203. [DOI] [PubMed] [Google Scholar]
- 2.Panieri E. Breast cancer screening in developing countries. Best Pract Res Clin Obstet Gynaecol. 2012;26:283–290. doi: 10.1016/j.bpobgyn.2011.11.007. [DOI] [PubMed] [Google Scholar]
- 3.Jemal A, Bray F, Center M, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2001;61(2):69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 4.Cancer.gov . PDQ® Breast Cancer Treatment. Bethesda, MD: National Cancer Institute; 2014. [Accessed Nov 2014]. Available from: http://cancer.gov/cancertopics/pdq/treatment/breast/Patient. [Google Scholar]
- 5.Cancer.org . Cancer Facts and Figures 2014. Georgia: American Cancer Society, Inc; 2014. [Accessed Nov 2014]. Available from: http://www.cancer.org/acs/groups/content/@research/documents/webcontent/acspc-042151.pdf. [Google Scholar]
- 6.Andreea GI, Pegza R, Lascu L, Bondari S, Stoica Z, Bondari A. The role of imaging techniques in diagnosis of breast cancer. Curr Health Sci J. 2011;37(2):55–61. [Google Scholar]
- 7.Cancer.gov . Adjuvant and Neoadjuvant Therapy for Breast Cancer. National Institutes of Health; [Accessed November 3, 2014]. [reviewed June 16, 2009]. Available from: http://www.cancer.gov/cancertopics/factsheet/Therapy/adjuvant-breast. [Google Scholar]
- 8.Graham LJ. Current approaches and challenges in monitoring treatment responses in breast cancer. J Cancer. 2014;5(1):58–68. doi: 10.7150/jca.7047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cancer.org . Breast Cancer Facts and Figures 2013–2014. Georgia: American Cancer Society, Inc; 2013. [Accessed Nov 2014]. Available from: http://www.cancer.org/acs/groups/content/@research/documents/document/acspc-042725.pdf. [Google Scholar]
- 10.Nationalbreastcancer.org . Clinical Breast Exam: The National Breast Cancer Foundation. National Cancer Institute; [Accessed November 3, 2014]. Available from: http://www.nationalbreastcancer.org/breast-self-exam. [Google Scholar]
- 11.Elmore J, Armstrong K, Lehman C, Fletcher S. Screening for breast cancer. J Am Med Assoc. 2005;293(10):1245–1256. doi: 10.1001/jama.293.10.1245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Nover AB, Jagtap S, Anjum W, et al. Modern breast cancer detection: a technological review. Int J Biomed Imaging. 2009;2009:1–14. doi: 10.1155/2009/902326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Niklason LT, Christian BT, Niklason LE, et al. Digital tomosynthesis in breast imaging. Radiology. 1997;205(2):399–406. doi: 10.1148/radiology.205.2.9356620. [DOI] [PubMed] [Google Scholar]
- 14.Smith A. Full-field breast tomosynthesis. Radiol Manage. 2005;27(5):25–31. [PubMed] [Google Scholar]
- 15.Pisano ED, Yaffe M. Digital mammography. Breast Dis. 1998;10(3–4):127–135. doi: 10.3233/bd-1998-103-413. [DOI] [PubMed] [Google Scholar]
- 16.Diekmann F, Bick U. Tomosynthesis and contrast-enhanced digital mammography: recent advances in digital mammography. Eur Radiol. 2007;17(12):3086–3092. doi: 10.1007/s00330-007-0715-x. [DOI] [PubMed] [Google Scholar]
- 17.Sinha S, Sinha U. Functional magnetic resonance of human breast tumors: diffusion and perfusion imaging. Ann N Y Acad Sci. 2002;980:95–115. doi: 10.1111/j.1749-6632.2002.tb04891.x. [DOI] [PubMed] [Google Scholar]
- 18.Cancer.org. American Cancer Society 2014. [Accessed November 2, 2014]. updated September 25, 2014. Available from: http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-diagnosis.
- 19.Planche K, Vinnicombe S. Breast imaging in the new era. Cancer Imaging. 2004;4(2):39–50. doi: 10.1102/1470-7330.2003.0033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Del Cura JL, Elizagaray E, Zabala R, Legórburu A, Grande D. The use of unenhanced Doppler sonography in the evaluation of solid breast lesions. AJR Am J Roentgenol. 2005;184(6):1788–1794. doi: 10.2214/ajr.184.6.01841788. [DOI] [PubMed] [Google Scholar]
- 21.Azhari H, Sazbon D. Volumetric imaging with ultrasonic spiral CT. Radiology. 1999;212(1):270–275. doi: 10.1148/radiology.212.1.r99jl18270. [DOI] [PubMed] [Google Scholar]
- 22.Newman J. Scintimammography in breast cancer diagnosis. Radiol Technol. 1998;70(2):153. [PubMed] [Google Scholar]
- 23.Tafra L. Positron emission mammography: a new breast imaging device. J Surg Oncol. 2008;97(5):372–373. doi: 10.1002/jso.20941. [DOI] [PubMed] [Google Scholar]
- 24.Von Schulthess GK. Cost considerations regarding an integrated CT-PET system. Eur Radiol. 2000;10(Suppl 3):S377–S380. doi: 10.1007/pl00014098. [DOI] [PubMed] [Google Scholar]
- 25.Kane RL. Breast thermography: helping make breast cancer prevention possible. Orig Internist. 2010:135–138. [Google Scholar]
- 26.Sterns EE, Curtis AC, Miller S, Hancock JR. Thermography in breast diagnosis. Cancer. 1982;50(2):323–325. doi: 10.1002/1097-0142(19820715)50:2<323::aid-cncr2820500226>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- 27.Malich A, Böhm T, Facius M, et al. Electrical impedance scanning as a new imaging modality in breast cancer detection – a short review of clinical value on breast application, limitations and perspectives. Nucl Instrum Methods Phys Res A. 2003;497(1):75–81. [Google Scholar]
- 28.Vreugdenburg TD, Willis CD, Mundy L, Hiller JE. A systematic review of elastography, electrical impedance scanning, and digital infrared thermography for breast cancer screening and diagnosis. Breast Cancer Res Treat. 2013;137(3):665–676. doi: 10.1007/s10549-012-2393-x. [DOI] [PubMed] [Google Scholar]
- 29.Nikolova NK. Microwave imaging for breast cancer. Microwave Mag IEEE. 2011;12(7):78–94. [Google Scholar]
- 30.Al-Forheidi M, Al-Mansour MM, Ibrahim EM. Breast cancer screening: a review of benefits and harms and recommendations for developing and low-income countries. Med Oncol. 2013;30(2):471. doi: 10.1007/s12032-013-0471-5. [DOI] [PubMed] [Google Scholar]
- 31.Miller AB, Baines CJ. The role of clinical breast examination and breast self-examination. Preventative Med. 2011;53(3):118–120. doi: 10.1016/j.ypmed.2011.05.001. [DOI] [PubMed] [Google Scholar]
- 32.Ma I, Dueck A, Gray R, et al. Clinical and self breast examination remain important in the ear of modern screening. Ann Surg Oncol. 2012;19(5):1484–1490. doi: 10.1245/s10434-011-2162-9. [DOI] [PubMed] [Google Scholar]
- 33.Khalili AF, Shahnazi M. Breast cancer screening (breast self-examination, clinical breast exam, and mammography) in women referred to health centers in Tabriz, Iran. Indian J Med Sci. 2010;64(4):149–162. [PubMed] [Google Scholar]
- 34.Ratanachaikanont T. Clinical breast examination and its relevance to diagnosis of palpable breast lesion. J Med Assoc Thai. 2005;88(4):505–507. [PubMed] [Google Scholar]
- 35.Carney PA, Miglioretti DL, Yankaskas BC, et al. Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography. Ann Intern Med. 2003;138(3):168–175. doi: 10.7326/0003-4819-138-3-200302040-00008. [DOI] [PubMed] [Google Scholar]
- 36.Moon WK, Im GJ, Noh DY, Han MC. Nonpalpable breast lesions: evaluation with power Doppler US and a microbubble contrast agent-initial experience. Radiology. 2000;217(1):240–246. doi: 10.1148/radiology.217.1.r00oc03240. [DOI] [PubMed] [Google Scholar]
- 37.Saslow D, Boetes C, Burke W, for the American Cancer Society Breast Cancer Advisory Group et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75–89. doi: 10.3322/canjclin.57.2.75. [DOI] [PubMed] [Google Scholar]
- 38.Bluemke DA, Gatsonis CA, Chen MH, et al. Magnetic resonance imaging of the breast prior to biopsy. J Am Med Assoc. 2004;292(22):2735–2742. doi: 10.1001/jama.292.22.2735. [DOI] [PubMed] [Google Scholar]
- 39.Lind P, Igerc I, Beyer T, Reinprecht P, Hausegger K. Advantages and limitations of FDG PET in the follow-up of breast cancer. Eur J Nucl Med Mol Imaging. 2004;31(Suppl 1):S125–S134. doi: 10.1007/s00259-004-1535-8. [DOI] [PubMed] [Google Scholar]
- 40.Liberman M, Sampalis F, Mulder DS, Sampalis JS. Breast cancer diagnosis by scintimammography: a meta-analysis and review of the literature. Breast Cancer Res Treat. 2003;80(1):115–126. doi: 10.1023/A:1024417331304. [DOI] [PubMed] [Google Scholar]
- 41.Klaus AJ, Klingensmith WC, 3rd, Parker SH, Stavros AT, Sutherland JD, Aldrete KD. Comparative value of 99mTc-sestamibi scintimammography and sonography in the diagnostic workup of breast masses. AJR Am J Roentgenol. 2000;174(6):1779–1783. doi: 10.2214/ajr.174.6.1741779. [DOI] [PubMed] [Google Scholar]
- 42.Khalkhali I, Itti E. Functional breast imaging using the single photon technique. Nucl Med Commun. 2002;23(7):609–611. doi: 10.1097/00006231-200207000-00003. [DOI] [PubMed] [Google Scholar]
- 43.Sampalis FS, Denis R, Picard D, et al. International prospective evaluation of scintimammography with t99mechnetium sestamibi. Am J Surg. 2001;182(4):399–403. doi: 10.1016/s0002-9610(01)00735-8. [DOI] [PubMed] [Google Scholar]
- 44.Arora N, Martins D, Ruggerio D, et al. Effectiveness of a noninvasive digital infrared thermal imaging system in the detection of breast cancer. Am J Surg. 2008;196(4):523–526. doi: 10.1016/j.amjsurg.2008.06.015. [DOI] [PubMed] [Google Scholar]
- 45.Parisky YR, Sardi A, Hamm R, et al. Efficacy of computerized infrared imaging analysis to evaluate mammographically suspicious lesions. AJR Am J Roentgenol. 2003;180(1):263–269. doi: 10.2214/ajr.180.1.1800263. [DOI] [PubMed] [Google Scholar]
- 46.Ng EYK, Fok SC, Peh YC, Ng FC, Sim LSJ. Computerized detection of breast cancer with artificial intelligence and thermograms. J Med Eng Technol. 2002;26(4):152–157. doi: 10.1080/03091900210146941. [DOI] [PubMed] [Google Scholar]
- 47.Stojadinovic A, Nissan A, Gallimidi Z, et al. Electrical impedance scanning for the early detection of breast cancer in young women: preliminary results of a multicenter prospective clinical trial. J Clin Oncol. 2005;23(12):2703–2715. doi: 10.1200/JCO.2005.06.155. [DOI] [PubMed] [Google Scholar]
- 48.Brown BH. Electrical impedance tomography (EIT): a review. J Med Eng Technol. 2003;27(3):97–108. doi: 10.1080/0309190021000059687. [DOI] [PubMed] [Google Scholar]
- 49.Martín G, Martín R, Brieva MJ, Santamaría L. Electrical impedance scanning in breast cancer imaging: correlation with mammographic and histologic diagnostic. Eur Radiol. 2002;12(6):1471–1478. doi: 10.1007/s00330-001-1275-0. [DOI] [PubMed] [Google Scholar]
- 50.Melloul M, Paz A, Ohana G, et al. Double-phase 99mTc-sestamibi scintimammography and trans-scan in diagnosing breast cancer. J Nucl Med. 1999;40(3):376–380. [PubMed] [Google Scholar]
- 51.Boas DA, Brooks DH, Miller EL, et al. Imaging the body with diffuse optical tomography. IEEE Signal Process Mag. 2001;18(6):57–75. [Google Scholar]
- 52.Wang LV, Wu H. Biomedical Optics: Principles and Imaging. Hoboken: Wiley; 2007. [Google Scholar]
- 53.Weissleder R. A clearer vision for in vivo imaging. Nat Biotechnol. 2001;19(4):316–317. doi: 10.1038/86684. [DOI] [PubMed] [Google Scholar]
- 54.Hsiang D, Shah N, Yu H, et al. Hand-held optical devices for breast cancer: spectroscopy and 3D tomographic imaging. IEEE J Sel Top Quantum Electron. 2011;18(4):1298–1312. [Google Scholar]
- 55.Tromberg B, Pogue BW, Paulsen KD, Yodh AG, Boas DA, Cerussi AE. Assessing the future of diffuse optical imaging technologies for breast cancer management. Med Phys. 2008;108(1):9–22. doi: 10.1118/1.2919078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Leff DR, Warren OJ, Enfield LC, et al. Diffuse optical imaging of the healthy and diseased breast: a systematic review. Breast Cancer Res Treat. 2008;108(1):9–22. doi: 10.1007/s10549-007-9582-z. [DOI] [PubMed] [Google Scholar]
- 57.Erickson SJ, Godavarty A. Hand-held based near-infrared optical imaging devices: a review. Med Eng Phys. 2009;31(5):495–509. doi: 10.1016/j.medengphy.2008.10.004. [DOI] [PubMed] [Google Scholar]
- 58.Hsiang D, Shah N, Yu H, et al. Coregistration of dynamic contrast enhanced MRI and broadband diffuse optical spectroscopy for characterizing breast cancer. Technol Cancer Res Treat. 2005;4(5):549–558. doi: 10.1177/153303460500400508. [DOI] [PubMed] [Google Scholar]
- 59.Chance B, Zhao Z, Wen S, Chen Y. Simple ac circuit for breast cancer detection and object detection. Rev Sci Instrum. 2006;77:064301. [Google Scholar]
- 60.Xu RX, Qiang B, Mao JJ, Povoski SP. Development of a handheld near-infrared imager for dynamic characterization of in vivo biological tissue systems. Appl Opt. 2007;46(30):7442–7451. doi: 10.1364/ao.46.007442. [DOI] [PubMed] [Google Scholar]
- 61.Zhu Q, Chen NG, Piao DQ, Guo PY, Ding XH. Design of near infrared imaging probe with the assistance of ultrasound localization. App Opt. 2001;40(19):3288–3303. doi: 10.1364/ao.40.003288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Tromberg BJ. Optical scanning and breast cancer. Acad Radiol. 2005;12(8):923–924. doi: 10.1016/j.acra.2005.07.003. [DOI] [PubMed] [Google Scholar]
- 63.Pham TH, Coquoz O, Fishkin JB, Anderson E, Tromberg BJ. Broad bandwidth frequency domain instrument for quantitative tissue optical spectroscopy. Rev Sci Instrum. 2000;71(6):2500–2513. [Google Scholar]
- 64.Tromberg BJ, Coquoz O, Fishkin JB, et al. Non-invasive measurements of breast tissue optical properties using frequency-domain photon migration. Philos Trans R Soc Lond B Biol Sci. 1997;352:661–668. doi: 10.1098/rstb.1997.0047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Lanning R, Tromberg B. Non-invasive characterization of breast cancer using near infrared optical spectroscopy. UCI Undergraduate Res J. 1999;II:43–49. [Google Scholar]
- 66.Tromberg BJ, Shah N, Lanning R, et al. Noninvasive in vivo characterization of breast tumors using photon migration spectroscopy. Neoplasia. 2000;2(1–2):26–40. doi: 10.1038/sj.neo.7900082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Holboke MJ, Tromberg BJ, Li X, et al. Three-dimensional diffuse optical mammography with ultrasound localization in a human subject. J Biomed Opt. 2000;5(2):237–247. doi: 10.1117/1.429992. [DOI] [PubMed] [Google Scholar]
- 68.Cerussi AE, Berger AJ, Bevilacqua F, et al. Sources of absorption and scattering contrast for near-infrared optical mammography. Acad Radiol. 2001;8(3):211–218. doi: 10.1016/S1076-6332(03)80529-9. [DOI] [PubMed] [Google Scholar]
- 69.Shah N, Cerussi A, Eker C, et al. Noninvasive functional optical spectroscopy of human breast tissue. Proc Natl Acad Sci U S A. 2001;98(8):4420–4425. doi: 10.1073/pnas.071511098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Shah N, Cerussi AE, Jakubowski D, Hsiang D, Butler J, Tromberg BJ. Spatial variations in optical and physiological properties of healthy breast tissue. J Biomed Opt. 2004;9(3):534–540. doi: 10.1117/1.1695560. [DOI] [PubMed] [Google Scholar]
- 71.Bevilacqua F, Berger AJ, Cerussi AE, Jakubowski D, Tromberg BJ. Broadband absorption spectroscopy in turbid media by combined frequency-domain and steady-state methods. Appl Opt. 2000;39(34):6498–6507. doi: 10.1364/ao.39.006498. [DOI] [PubMed] [Google Scholar]
- 72.Cerussi AE, Jakubowski D, Shah N, et al. Spectroscopy enhances the information content of optical mammography. J Biomed Opt. 2002;7(1):60–71. doi: 10.1117/1.1427050. [DOI] [PubMed] [Google Scholar]
- 73.Jakubowski DB, Cerussi AE, Bevilacqua F, et al. Monitoring neoadjuvant chemotherapy in breast cancer using quantitative diffuse optical spectroscopy: a case study. J Biomed Opt. 2004;9(1):230–238. doi: 10.1117/1.1629681. [DOI] [PubMed] [Google Scholar]
- 74.Shah N, Gibbs J, Wolverton D, Cerussi A, Hylton N, Tromberg BJ. Combined diffuse optical spectroscopy and contrast-enhanced magnetic resonance imaging for monitoring breast cancer neoadjuvant chemotherapy: a case study. J Biomed Opt. 2005;10(5):051503. doi: 10.1117/1.2070147. [DOI] [PubMed] [Google Scholar]
- 75.Cerussi A, Shah N, Hsiang D, Durkin A, Butler J, Tromberg BJ. In vivo absorption, scattering, and physiologic properties of 58 malignant breast tumors determined by broadband diffuse optical spectroscopy. J Biomed Opt. 2006;11(4):044005. doi: 10.1117/1.2337546. [DOI] [PubMed] [Google Scholar]
- 76.Cerussi A, Hsiang D, Shah N, et al. Predicting response to breast cancer neoadjuvant chemotherapy using diffuse optical spectroscopy. Proc Natl Acad Sci U S A. 2007;104(10):4014–4019. doi: 10.1073/pnas.0611058104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.No KS, Chou PH. Mini-FDPM and heterodyne mini-FDPM: handheld non-invasive breast cancer detectors based on frequency-domain photon migration. IEEE Trans Circ Syst I Reg Papers. 2005;52(12):2672–2685. [Google Scholar]
- 78.No KS, Xie Q, Kwong R, Cerussi A, Tromberg BJ, Chou P. HBS: a handheld breast cancer detector based on frequency domain photon migration with full heterodyne; Proceedings of the IEEE BioCAS; November 29–December 1, 2006; London. pp. 114–117. [Google Scholar]
- 79.No KS, Xie Q, Kwong R, et al. In vivo breast cancer measurement with a handheld laser breast scanner; Proceedings of the 50th IEEE International Midwest Symposium on Circuits and Systems; August 5–8 2007; Montreal, Quebec, Canada. pp. 1–4. [Google Scholar]
- 80.Nioka S, Chance B. NIR spectroscopic detection of breast cancer. Technol Cancer Res Treat. 2005;4(5):497–512. doi: 10.1177/153303460500400504. [DOI] [PubMed] [Google Scholar]
- 81.Sao V, Pourrezaei K, Akin A, Ayaz H. Breast tumor imaging using NIR LED based handheld continuous-wave imager; Proceedings of the IEEE 29th Annual North East Bioengineering Conference; March 22–23 2003; Newark, NJ. pp. 55–56. [Google Scholar]
- 82.Liu Q, Luo Q, Chance B. 2D phased array fluorescence wireless localizer in breast cancer detection; Proceedings of the IEEE/EMBS International Summer School Medical Devices Biosensors; June 26–July 2, 2004; Hong Kong, China. pp. 71–73. [Google Scholar]
- 83.Cheng X, Mao J, Bush R, Kopans DB, Moore RH, Chorlton M. Breast cancer detection by mapping hemoglobin concentration and oxygen saturation. Appl Opt. 2003;42:6412–6421. doi: 10.1364/ao.42.006412. [DOI] [PubMed] [Google Scholar]
- 84.Xu R, Qiang B, Mao J. Near infrared imaging of tissue heterogeneity: probe design and sensitivity analysis; Proceedings of the 27th Annual Conference on IEEE Engineering and Medicine Biology; September 1–4 2005; Shanghai, China. pp. 278–281. [DOI] [PubMed] [Google Scholar]
- 85.Xu RX, Olsen JO, Povoski SP, Yee LD, Mao J. Localization and functional parameter reconstruction of suspicious breast lesions by near infrared/ultrasound dual mode imaging; Proceedings of the 27th Annual Conference on IEEE Engineering and Medicine Biology; September 1–4 2005; Shanghai, China. pp. 4473–4476. [DOI] [PubMed] [Google Scholar]
- 86.Durduran T, Choe R, Yu G, et al. Diffuse optical measurement of blood flow in breast tumors. Opt Lett. 2005;30(21):2915–2917. doi: 10.1364/ol.30.002915. [DOI] [PubMed] [Google Scholar]
- 87.Xu C, Zhu Q. Optimal probe design for dual-modality breast imaging; Proceedings of the SPIE; Optical Tomography and Spectroscopy of Tissue VII; February 13, 2007; San Jose, CA. p. 64340B. [Google Scholar]
- 88.Ge J, Zhu B, Regalado S, Godavarty A. Three-dimensional fluorescence-enhanced optical tomography using a hand-held probe based imaging system. Med Phys. 2008;35(7):3354–3363. doi: 10.1118/1.2940603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Erickson SJ, Ge J, Sanchez A, Godavarty A. Two-dimensional fast surface imaging using a hand-held optical device: in-vitro and in-vivo fluorescence studies. Trans Oncol. 2010;3(1):16–22. doi: 10.1593/tlo.09157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Erickson SJ, Martinez S, DeCerce J, Romero A, Caldera L, Godavarty A. Fast coregistered breast imaging in vivo using a hand-held optical imager; Proceedings of the SPIE; Advanced Biomedical and Clinical Diagnostic Systems VIII; February 19, 2010; San Francisco, CA. pp. 75550P-1–75550P-6. [Google Scholar]
- 91.Solomon M, White BR, Bauer AQ, Perry G, Culver JP. Handheld video rate fluorescence diffuse optical tomography; OSA Biomedical Optics; April 11–14, 2010; Miami, FL. p. BTuD9. [Google Scholar]
- 92.Zhou C, Choe R, Shah N, et al. Diffuse optical monitoring of blood flow and oxygenation in human breast cancer during early stages of neoadjuvant chemotherapy. J Biomed Opt. 2007;12(5):051903. doi: 10.1117/1.2798595. [DOI] [PubMed] [Google Scholar]
- 93.Gonzalez J, Decerce J, Erickson SJ, et al. Hand-held optical imager (Gen-2): improved instrumentation and target detectability. J Biomed Opt. 2012;17(8):081402. doi: 10.1117/1.JBO.17.8.081402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Gonzalez J, Roman M, Hall M, Godavarty A. Gen-2 hand-held optical imager towards cancer imaging: reflectance and transillumination phantom studies. Sensors. 2012;12:1885–1897. doi: 10.3390/s120201885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Eppstein MJ, Hawrysz DJ, Godavarty A, Sevick-Muraca EM. Three-dimensional near-infrared fluorescence tomography with Bayesian methodologies for image reconstruction from sparse and noisy data sets. Proc Natl Acad Sci U S A. 2002;99:9619–9624. doi: 10.1073/pnas.112217899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Godavarty A, Eppstein MJ, Zhang C, et al. Fluorescence-enhanced optical imaging in large tissue volumes using a gain modulated ICCD camera. Phys Med Biol. 2003;48:1701–1720. doi: 10.1088/0031-9155/48/12/303. [DOI] [PubMed] [Google Scholar]
- 97.Godavarty A, Thompson AB, Roy R, et al. Diagnostic imaging of breast cancer using fluorescence-enhanced optical tomography: phantom studies. J Biomed Opt. 2004;9(3):488–496. doi: 10.1117/1.1691027. [DOI] [PubMed] [Google Scholar]
- 98.Floery D, Helbich TH, Riedl CC, et al. Characterization of benign and malignant breast lesions with computed tomography laser mammography (CTLM): initial experience. Invest Radiol. 2005;40(6):328–335. doi: 10.1097/01.rli.0000164487.60548.28. [DOI] [PubMed] [Google Scholar]
- 99.Schmitz CH, Klemer DP, Hardin R, et al. Design and implementation of dynamic near-infrared optical tomographic imaging instrumentation for simultaneous dual-breast measurements. Appl Opt. 2005;44(11):2140–2153. doi: 10.1364/ao.44.002140. [DOI] [PubMed] [Google Scholar]
- 100.Schmitz CH, Löcker M, Lasker JM, Hielscher AH, Barbour RL. Instrumentation for fast functional optical tomography. Rev Sci Instrum. 2002;73:429. [Google Scholar]
- 101.Al Abdi RM, Schmitz C, Ansari R, et al. A dual-mode simultaneous bilateral optical imaging system for breast cancer detection; OSA Biomedical Optics; April 11–14, 2010; Miami, FL. p. BSuB5. [Google Scholar]
- 102.AlAbdi R, Graber HL, Xu Y, Barbour RL. Optomechanical imaging system for breast cancer detection. J Opt Soc Am A Opt Image Sci Vis. 2011;28(12):2473–2493. doi: 10.1364/JOSAA.28.002473. [DOI] [PubMed] [Google Scholar]
- 103.Yates T, Hebden JC, Gibson A, Everdell N, Arridge SR, Douek M. Optical tomography of the breast using a multi-channel time-resolved imager. Phys Med Biol. 2005;50:2503. doi: 10.1088/0031-9155/50/11/005. [DOI] [PubMed] [Google Scholar]
- 104.Hebden JC, Yates TD, Gibson A, et al. Monitoring recovery after laser surgery of the breast with optical tomography: a case study. Appl Opt. 2005;44(10):1898–1904. doi: 10.1364/ao.44.001898. [DOI] [PubMed] [Google Scholar]
- 105.Enfield LC, Gibson AP, Everdell NL, et al. Three-dimensional time-resolved optical mammography of the uncompressed breast. Appl Opt. 2007;46(17):3628–3638. doi: 10.1364/ao.46.003628. [DOI] [PubMed] [Google Scholar]
- 106.Culver JP, Choe R, Holboke MJ, et al. Three-dimensional diffuse optical tomography in the parallel plane transmission geometry: evaluation of a hybrid frequency domain/continuous wave clinical system for breast imaging. Med Phys. 2003;30:235. doi: 10.1118/1.1534109. [DOI] [PubMed] [Google Scholar]
- 107.Choe R, Konecky SD, Corlu A, et al. Differentiation of benign and malignant breast tumors by in-vivo three-dimensional parallel-plate diffuse optical tomography. J Biomed Opt. 2009;14(2):024020. doi: 10.1117/1.3103325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Choe R, Corlu A, Lee K, et al. Diffuse optical tomography of breast cancer during neoadjuvant chemotherapy: a case study with comparison to MRI. Med Phys. 2005;32(4):1128–1139. doi: 10.1118/1.1869612. [DOI] [PubMed] [Google Scholar]
- 109.Ntziachristos V, Yodh AG, Schnall M, Chance B. Concurrent MRI and diffuse optical tomography of breast after indocyanine green enhancement. Proc Natl Acad Sci U S A. 2000;97(6):2767. doi: 10.1073/pnas.040570597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Fang Q, Carp SA, Moore RH, Kopans DB, Boas DA. Benign and malignant breast lesions with combined optical imaging and tomosynthesis; OSA Biomedical Optics; April 11–14 2010; Miami, FL. p. BSuB. [Google Scholar]
- 111.Fang Q, Selb J, Carp SA, et al. Combined optical and X-ray tomosynthesis breast imaging. Radiology. 2011;258(1):89–97. doi: 10.1148/radiol.10082176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Fang Q. Quantitative diffuse optical tomography using a mobile phone camera and automatic 3D photo stitching; OSA Biomedical Optics; April 28–May 2, 2012; Miami, FL. pp. BSu3A–96. [Google Scholar]
- 113.Hadjipanayis CG, Jiang H, Roberts DW, Yang L. Current and future clinical applications for optical imaging of cancer: from intraoperative surgical guidance to cancer screening. Semin Oncol. 2011;38(1):109–118. doi: 10.1053/j.seminoncol.2010.11.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Zhu Q, Huang M, Chen N, et al. Ultrasound-guided optical tomographic imaging of malignant and benign breast lesions: initial clinical results of 19 cases. Neoplasia. 2003;5(5):379–388. doi: 10.1016/s1476-5586(03)80040-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Flexman ML, Kim HK, Stoll R, Khalil MA, Fong CJ, Heilscher AH. A wireless handheld probe with spectrally constrained evolution strategies for diffuse optical imaging of tissue. Rev Sci Instrum. 2012;83:033108. doi: 10.1063/1.3694494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Labib NA, Ghobashi MM, Moneer MM, Helal MH, Abdalgaleel SA. Evaluation of BreastLight as a tool for early detection of breast lesions among females attending National Cancer Institute, Cairo University. Asian Pac J Cancer Prev. 2013;18(8):4647–4650. doi: 10.7314/apjcp.2013.14.8.4647. [DOI] [PubMed] [Google Scholar]
- 117.Rodriguez S, Kaliada H, Gabrielle C, Jung Y-J, Godavarty A. In-vivo breast imaging using an ultra-portable hand-held near-infrared optical scanner (NIROS); OSA J Biomed Opt; April 26–30, 2014; Miami, FL. p. BM3A.66. [Google Scholar]
- 118.Palmer MR, Shibata Y, Kruskal JB, Lenkinski RE. In Vivo Imaging of Small Animals with Optical Tomography and Near-Infrared Fluorescent Probes; Proceedings of SPIEBiomedical Nanotechnology Architectures and Applications; June 19, 2002; San Jose, CA. pp. 166–169. [Google Scholar]
- 119.Wieringa FP, Mastik F, Ten Cate FJ, Neumann HM, van der Steen FW. Remote non-invasive stereoscopic imaging of blood vessels: first in-vivo results of a new multispectral contrast enhancement technology. Ann Biomed Eng. 2006;34(12):1870–1878. doi: 10.1007/s10439-006-9198-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Han X, Lui H, McLean DI, Zeng H. A technique for near-infrared autofluorescence imaging of skin: preliminary results; Proceedings of SPIE Photonic Therapeutics and Diagnostics II; February 22, 2006; San Jose, CA. pp. 60780S–60780S-3. [Google Scholar]
- 121.Matsushita T, Miyati T, Nakayama K, et al. Development of qualitative near infrared vascular imaging system with tuned aperture computed tomography; Proceedings of SPIE Medical Imaging 2007: Physics of Medical Imaging; March 16, 2007; San Diego, CA. p. 65103G. [DOI] [PubMed] [Google Scholar]
- 122.Han X, Lui H. Near-infrared autofluorescence imaging of cutaneous melanins and human skin in vivo. J Biomed Opt. 2009;14(2):024017. doi: 10.1117/1.3103310. [DOI] [PubMed] [Google Scholar]
- 123.Abookasis D. Imaging cortical absorption, scattering, and hemodynamic response during ischemic stroke using spatially modulated near-infrared illumination. J Biomed Opt. 2009;14(2):1–19. doi: 10.1117/1.3116709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Bouzida N, Bendada AH, Maldague XP. Near-infrared image formation and processing for the extraction of hand veins. J Mod Opt. 2010;57(18):1731–1737. [Google Scholar]
- 125.Mizuno Y, Katayama T, Nakamachi E. Development of an accurate 3D blood vessel searching system using NIR light; Proceedings of SPIE; Advanced Biomedical and Clinical Diagnostic Systems VIII; February 19, 2010; San Francisco, CA. p. 755506. [Google Scholar]
- 126.Lee BBT, Matsui A, Hutteman M. Intraoperative near-infrared fluorescence imaging in perforator flap reconstruction: current research and early clinical experience. J Reconstr Microsurg. 2010;26(1):59–65. doi: 10.1055/s-0029-1244805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Chen P, Chang M, Chiu F, Li C, Law ABL. Quantitative measurements of blood vessel of diabetic extremity based on near-infrared image technique; IFMBE Proceedings; August 1–6, 2010; Singapore. pp. 1311–1314. [Google Scholar]
- 128.Jakovels D, Spigulis J, Saknite I. Multi-spectral mapping of in-vivo skin hemoglobin and melanin; Proceedings of SPIE; Biophotonics: Photonic Solutions for Better Health Care II; May 18, 2010; Brussels, Belgium. p. 77152Z. [Google Scholar]
- 129.Shao X, Zheng W, Huang Z. Polarized near-infrared autofluorescence imaging combined with near-infrared diffuse reflectance imaging for improving colonic cancer detection. Opt Express. 2010;18(23):24293–24300. doi: 10.1364/OE.18.024293. [DOI] [PubMed] [Google Scholar]
- 130.Shimawaki S, Sakai N. Change in blood vessel images of the human finger using near-infrared radiation while compressing the upper arm; IFMBE Proceedings; August 1–6, 2010; Singapore. pp. 1262–1265. [Google Scholar]
- 131.Matsushita T, Miyati T, Nakayama K, et al. Qualitative near-infrared vascular imaging system with tuned aperture computed tomography. J Biomed Opt. 2011;16(7):076004. doi: 10.1117/1.3595424. [DOI] [PubMed] [Google Scholar]
- 132.Lin ZJ, Niu H, Liu Y, Su J, Liu H. CCD-camera-based diffuse optical tomography to study ischemic stroke in preclinical rat models; Proceedings of SPIE; Optical Tomography and Spectroscopy; February 17, 2011; San Francisco. pp. 78960R–78960R-8. [Google Scholar]
- 133.Liu Y, Bauer AQ, Akers W, et al. Compact intraoperative imaging device for sentinel lymph node mapping; Proceedings of SPIE; Reporters, Markers, Dyes, Nanoparticles, and Molecular Probes for Biomedical Applications III; February 11, 2011; San Francisco, CA. pp. 79100D–79100D-7. [Google Scholar]
- 134.Mieog JS, Troyan SL, Hutteman M, et al. Toward optimization of imaging system and lymphatic tracer for near-infrared fluorescent sentinel lymph node mapping in breast cancer. Ann Surg Oncol. 2011;18(9):2483–2491. doi: 10.1245/s10434-011-1566-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Mieog JS, Hutteman M, van der Vorst JR, et al. Image-guided tumor resection using real-time near-infrared fluorescence in a syngeneic rat model of primary breast cancer. Breast Cancer Res Treat. 2011;128(3):679–689. doi: 10.1007/s10549-010-1130-6. [DOI] [PubMed] [Google Scholar]
- 136.Kuzmina I, Diebele I. Multi-spectral imaging analysis of pigmented and vascular skin lesions: results of a clinical trial; Proceedings of SPIE; Photonic Therapeutics and Diagnostics VII; February 17, 2011; San Francisco, CA. pp. 788312–788312. [Google Scholar]
- 137.Osaki R, Ding M, Hyodo H, Soga K, Takemura H, Mizoguchi H. 3D bioimaging sensor of breast cancer cell using rare-earth-doped ceramic nanophosphors and near-infrared; Proceedings of IEEE Sensors; October 28–31, 2011; Limerick, Ireland. pp. 1784–1787. [Google Scholar]
- 138.Chance B, Nioka S, Zhang J, et al. Breast cancer detection based on incremental biochemical and physiological properties of breast cancers: a six-year, two-site study. Acad Radiol. 2005;12(8):925–933. doi: 10.1016/j.acra.2005.04.016. [DOI] [PubMed] [Google Scholar]